Maria, a 34-year-old teacher from Atlanta, sat in her car staring at her patient portal. The words “ANA: Positive” and “Anti-dsDNA: 156 IU/mL” blurred through her tears. Her doctor’s nurse had called to schedule a “follow-up discussion,” but Google was already telling her she might have systemic lupus erythematosus. Three sleepless nights later, she walked into her rheumatologist’s office desperate for answers about what these numbers actually meant for her future.
On This Page – Quick Medical Summary
Direct Answer: What Is the Anti-dsDNA Test?
The anti-dsDNA test is a specialized lupus blood test that measures antibodies against double stranded DNA in your bloodstream. Doctors order this autoimmune antibodies test after you receive an ANA test positive result to confirm lupus diagnosis and monitor disease activity, particularly lupus nephritis. Unlike the broader ANA test, anti-dsDNA is highly specific to systemic lupus erythematosus, appearing in 65-85% of lupus patients.
Quick Takeaways: Understanding Your Test
- What it measures: Your immune system’s production of antibodies that attack your own DNA
- Why it matters: Helps confirm lupus diagnosis when combined with symptoms and other lupus diagnostic tests
- When you need it: Typically ordered after positive ANA results or to monitor known lupus flare up activity
- Connection to organs: High anti-dsDNA levels strongly correlate with lupus kidney disease and other organ involvement
If you’ve just received confusing lupus test results explained in medical jargon, you’re navigating one of healthcare’s most emotionally challenging moments. Approximately 1.5 million Americans live with lupus, and many faced the same uncertainty you’re experiencing when they first saw “anti-dsDNA positive” on their lab work. This test doesn’t define your entire health picture—it’s one crucial piece of diagnostic information that, when combined with your symptoms, physical examination, and additional lupus antibodies testing, helps your medical team create the clearest treatment roadmap.
The anti-dsDNA test specifically targets autoantibodies that attack the genetic material inside your cells, a hallmark of systemic lupus erythematosus test panels. Unlike general inflammation markers, these double stranded DNA antibody measurements provide targeted insight into lupus autoimmune test activity and potential kidney involvement. Understanding what your specific anti-dsDNA test results mean—whether negative, borderline, or significantly elevated—empowers you to ask the right questions and advocate effectively during your next rheumatology appointment.
Understanding Anti-dsDNA Test – The Complete Guide
What Is the Anti-dsDNA Test and Why It’s Ordered
The anti-dsDNA test detects specific autoimmune antibodies that target the double-helix structure of your genetic material, functioning as a critical marker in systemic lupus erythematosus diagnosis and monitoring. Unlike the broader ANA test that screens for multiple autoantibodies, this lupus blood test specifically identifies antibodies against double stranded DNA, making it highly specific for lupus diagnosis. Rheumatologists typically order anti-dsDNA testing after receiving an ANA test positive result, especially when patients exhibit classic lupus symptoms like joint pain, facial rashes, or unexplained fatigue.

Your doctor requests this lupus autoimmune test in several critical scenarios: confirming suspected systemic lupus erythematosus when clinical symptoms align with positive ANA results, monitoring disease activity in established lupus patients, detecting potential lupus nephritis before kidney damage becomes severe, and assessing treatment effectiveness during lupus flare up episodes. The anti-dsDNA test serves dual purposes—diagnostic confirmation and ongoing disease surveillance—which makes it one of the most valuable lupus diagnostic tests in rheumatology. Understanding your body’s overall health markers alongside specialized autoimmune antibodies testing provides a comprehensive picture of disease management.
How the Anti-dsDNA Blood Test Works
The anti-dsDNA test measures lupus antibodies through three primary laboratory methods, each with distinct sensitivity and specificity characteristics that affect lupus test results explained to patients. When you provide a blood sample—typically drawn from a vein in your arm—laboratory technicians process the serum to detect and quantify anti-dsDNA antibodies using one of these established methodologies. The testing process takes 2-5 business days depending on your facility’s equipment and protocol, though urgent cases may receive expedited processing.
Anti-dsDNA Testing Method Comparison
The ELISA method remains the most common anti-dsDNA test approach in clinical laboratories due to its automation capabilities and ability to process multiple samples simultaneously. However, ELISA can occasionally produce false-positive results in patients with hepatitis or certain drug-induced conditions, requiring clinical correlation. The Farr assay, utilizing radioactive isotopes to measure antibody-antigen binding, demonstrates exceptional specificity for high-avidity anti-dsDNA antibodies that correlate strongly with active lupus kidney test abnormalities.
Crithidia luciliae immunofluorescence testing employs a unique organism—a parasitic flagellate—whose kinetoplast contains pure double stranded DNA without contaminating single-stranded DNA. This biological specificity makes CLIFT results highly reliable when positive, though its lower sensitivity means approximately 35-60% of lupus patients may test negative despite having active disease. Modern laboratories increasingly combine methods, using ELISA for screening and CLIFT or Farr assay for confirmation when anti-dsDNA levels approach diagnostic thresholds.
What This Means For You
If your rheumatologist ordered anti-dsDNA testing after your ANA test positive result, expect your medical team to interpret results within the context of your complete clinical picture—not as an isolated finding. The test method your laboratory uses significantly impacts reference ranges and interpretation, so always request the specific numerical value and testing methodology rather than accepting vague “positive” or “negative” reports. Monitoring your kidney health markers becomes particularly important if anti-dsDNA levels are elevated, as this antibody strongly predicts lupus nephritis development.
Before your lupus blood test appointment, consider these preparation steps: avoid fasting unless specifically instructed (most anti-dsDNA tests don’t require it), bring a current medication list including over-the-counter supplements, document any recent infections or illnesses that might influence results, and prepare questions about which testing method your laboratory employs. Understanding that no single lupus diagnostic test confirms or excludes the diagnosis empowers you to view anti-dsDNA results as one component of a comprehensive autoimmune evaluation rather than a definitive answer.
Decoding Your Anti-dsDNA Test Results
Anti-dsDNA Normal Range and What Numbers Mean
Anti-dsDNA test results are reported in International Units per milliliter (IU/mL) or titers, with reference ranges varying significantly based on the laboratory method and equipment your facility uses. Most laboratories establish their own cutoff values, but general clinical thresholds help rheumatologists interpret whether your lupus blood test indicates active disease requiring intervention. Understanding these numerical benchmarks empowers you to have informed conversations with your healthcare team about your systemic lupus erythematosus test progression and track health metrics alongside your lab work.
Anti-dsDNA Test Result Interpretation
| Result Category | Typical IU/mL Range | Clinical Significance | Recommended Action |
|---|---|---|---|
| Negative/Normal | <10-30 IU/mL | No detectable anti-dsDNA antibodies; does NOT rule out lupus | Monitor symptoms; may need additional lupus antibodies testing |
| Borderline/Equivocal | 30-75 IU/mL | Uncertain significance; possible early disease or cross-reactivity | Repeat test in 8-12 weeks; correlate with clinical symptoms |
| Positive/Moderate | 75-200 IU/mL | Confirms active lupus diagnosis when combined with symptoms and ANA test positive | Begin or adjust treatment; monitor for lupus nephritis |
| High/Strongly Positive | >200 IU/mL | Indicates active disease with high risk of kidney involvement | Urgent rheumatology follow-up; kidney function assessment |
Laboratory reference ranges differ because anti-dsDNA test methodologies—ELISA, Farr assay, and CLIFT—measure antibodies with varying sensitivity thresholds. Your report should specify which method was used and the laboratory’s established normal range, as comparing results from different facilities without this context can create unnecessary confusion about lupus test results explained during appointments. Some laboratories report titers (such as 1:10, 1:40, 1:160) instead of IU/mL values, particularly when using immunofluorescence methods.
The concept of “normal” deserves careful clarification: approximately 0.5-3% of healthy individuals without lupus may test weakly positive for anti-dsDNA antibodies, though these levels rarely exceed 30 IU/mL. Conversely, 15-35% of confirmed systemic lupus erythematosus patients consistently test negative for anti-dsDNA throughout their disease course, demonstrating that this single lupus blood work marker cannot definitively confirm or exclude diagnosis. Your rheumatologist interprets anti-dsDNA levels alongside complement proteins (C3, C4), complete blood counts, urinalysis, and clinical presentation to form comprehensive diagnostic conclusions.
Anti-dsDNA Positive: What It Really Means
Receiving an anti-dsDNA positive result typically indicates your immune system is producing autoimmune antibodies that attack your body’s DNA, a hallmark finding in 65-85% of people diagnosed with systemic lupus erythematosus. However, this lupus test positive outcome requires careful interpretation within your complete medical context rather than functioning as a standalone diagnostic criterion. The 2019 EULAR/ACR classification criteria for lupus diagnosis assign anti-dsDNA antibodies significant weight (6 points) but still require clinical symptoms and additional laboratory findings to reach the diagnostic threshold.
What Anti-dsDNA Positive Does NOT Automatically Mean:
- You will definitely develop lupus nephritis symptoms (though risk increases with higher levels)
- Your disease is currently active or severe (clinical correlation essential)
- You need aggressive immunosuppression immediately (treatment depends on organ involvement)
- Other autoimmune conditions are ruled out (overlap syndromes exist)
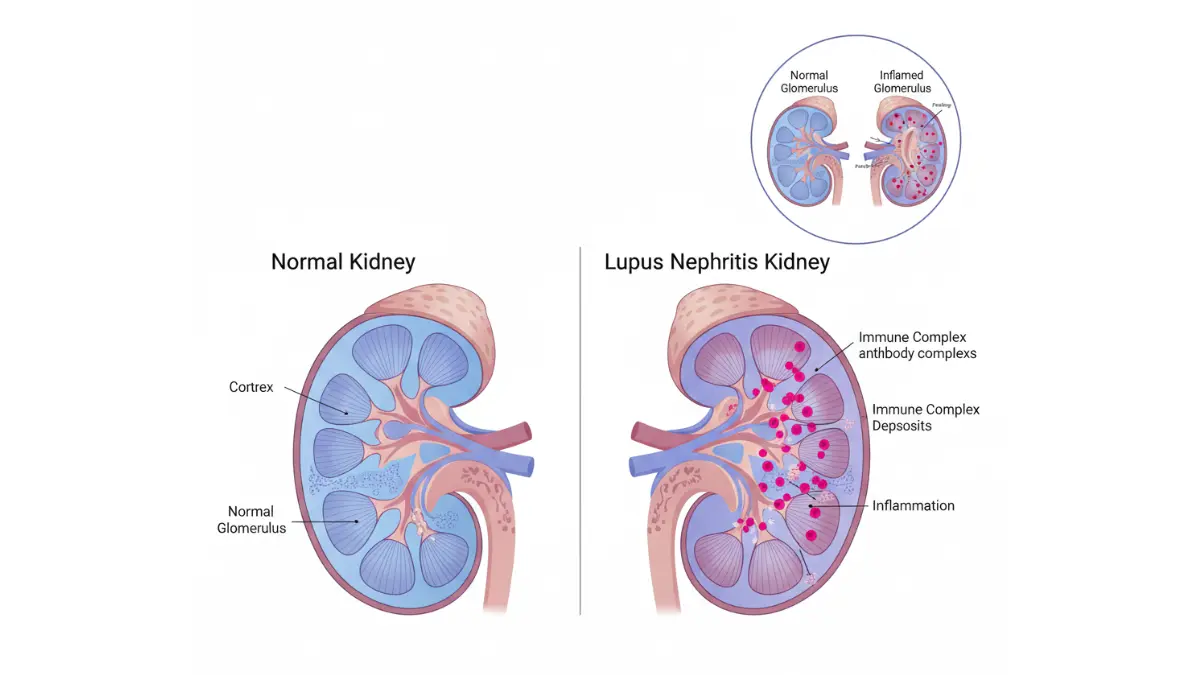
The presence of anti-dsDNA antibodies correlates strongly with lupus kidney disease risk, as these specific autoantibodies can form immune complexes that deposit in kidney glomeruli, triggering inflammation and progressive damage. Studies demonstrate that lupus patients with persistently high anti-dsDNA levels face 60-80% higher likelihood of developing lupus nephritis compared to those with negative or low-positive results. Maintaining awareness of your kidney health indicators becomes crucial when anti-dsDNA testing shows elevated values.
Patient Perspective: Understanding the Emotional Impact
“When I saw ‘anti-dsDNA positive’ on my patient portal at 2 AM, I immediately thought I was dying,” shares Jennifer, a 29-year-old lupus patient from Boston. “My rheumatologist explained that while the test confirmed my lupus diagnosis, my level of 68 IU/mL was relatively low, my kidneys were functioning perfectly, and many people live full, active lives with proper management. That context—not just the word ‘positive’—made all the difference in managing my anxiety and focusing on actionable next steps.”
This emotional reaction reflects the common experience among patients receiving autoimmune antibodies test results without immediate medical interpretation. The gap between seeing laboratory values and understanding their clinical significance creates unnecessary distress, emphasizing why immediate rheumatology consultation matters when lupus diagnostic tests return positive.
Anti-dsDNA High Levels and Disease Activity
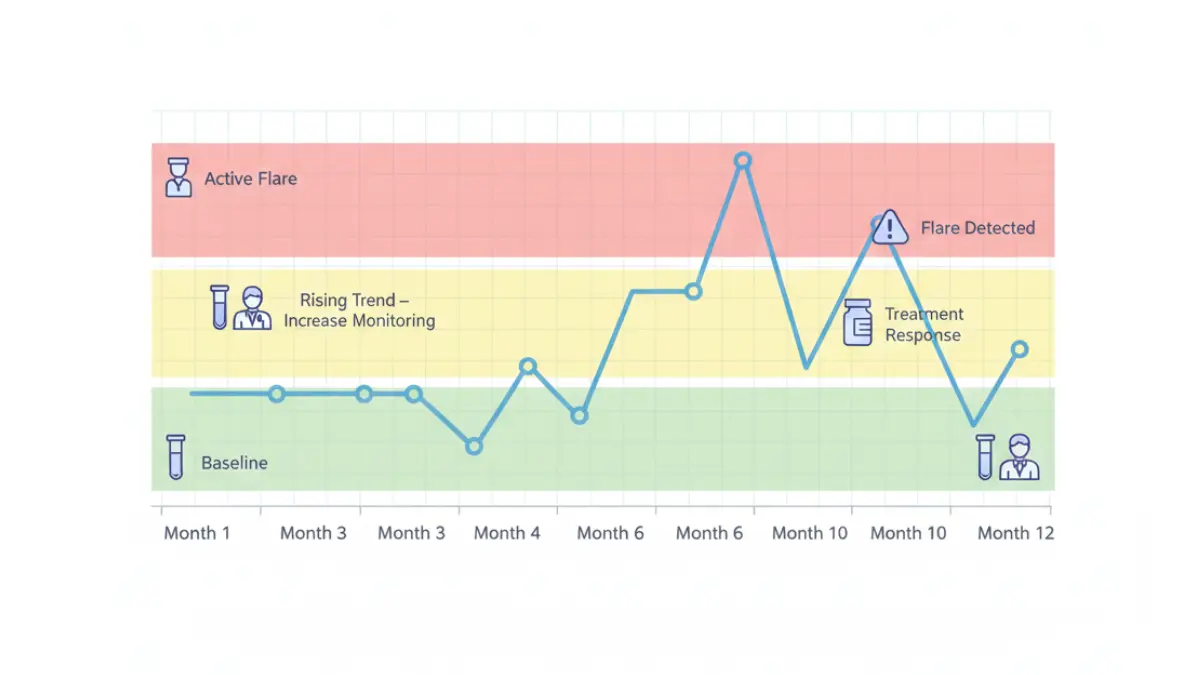
Significantly elevated anti-dsDNA levels (typically >200 IU/mL) signal active lupus flare up in approximately 50-70% of cases, though the relationship varies among individuals. Serial monitoring of anti-dsDNA levels over time provides more valuable information than single measurements, as rising trends often precede clinical flares by weeks or months, enabling proactive treatment adjustments. Your rheumatologist may increase testing frequency from every 6 months to monthly intervals when anti-dsDNA high results suggest brewing disease activity.
The correlation between anti-dsDNA levels and lupus nephritis represents one of the strongest biomarker relationships in rheumatology, with research showing that anti-dsDNA IgE antibodies may predict kidney involvement even before traditional markers become abnormal. Patients with anti-dsDNA levels exceeding 150 IU/mL should undergo regular urinalysis and kidney function testing (serum creatinine, estimated GFR) even without obvious lupus nephritis symptoms like swelling or decreased urination. Monitoring these interconnected markers alongside overall wellness indicators helps detect complications early when interventions prove most effective.
Evidence Strength Pyramid for Anti-dsDNA Clinical Correlations:
High Certainty Evidence (Multiple Studies, Consistent Results):
- Anti-dsDNA positivity correlates with lupus nephritis development and progression
- Rising anti-dsDNA levels precede disease flares in 50-70% of patients
- High-avidity anti-dsDNA antibodies indicate more severe disease activity
Moderate Certainty Evidence (Some Studies, Occasional Conflicting Data):
- Anti-dsDNA levels predict specific organ involvement beyond kidneys
- Declining anti-dsDNA with treatment suggests therapeutic response
- Anti-dsDNA antibodies may increase cardiovascular disease risk in lupus patients
Lower Certainty Evidence (Limited Studies, Needs More Research):
- Anti-dsDNA levels directly correlate with central nervous system lupus
- Specific anti-dsDNA titers predict disease outcomes years in advance
False Positives and Negatives
Understanding the limitations of anti-dsDNA testing prevents both overdiagnosis and missed diagnoses in lupus blood work interpretation. False-positive results—positive anti-dsDNA without lupus—occur in approximately 1-5% of healthy individuals, patients with chronic hepatitis B or C, people taking certain medications (procainamide, hydralazine, quinidine), and individuals with other autoimmune conditions like Sjögren’s syndrome or rheumatoid arthritis. These cross-reactions typically produce low-level positivity (30-50 IU/mL) rather than the markedly elevated values seen in active systemic lupus erythematosus test scenarios.
False-negative results present an even more significant clinical challenge: 15-35% of people with confirmed lupus consistently test negative for anti-dsDNA antibodies throughout their disease course. This phenomenon explains why rheumatologists never rely solely on anti-dsDNA for lupus diagnosis and why you can absolutely have active, serious lupus despite negative double stranded DNA antibody results. Patients with seronegative lupus—negative for both anti-dsDNA and anti-Sm antibodies—require diagnosis based on clinical criteria, complement levels, and other laboratory markers.
What This Means For You: Interpreting Your Specific Results
Your anti-dsDNA result represents one data point in a comprehensive evaluation, not a definitive diagnosis or prognosis. If your test is positive with high levels, this confirms lupus diagnosis when combined with symptoms and warrants kidney monitoring, but does NOT guarantee you will develop kidney damage lupus—proper treatment significantly reduces this risk. If your anti-dsDNA is negative despite strong clinical suspicion for lupus, your rheumatologist should pursue additional testing including anti-Sm antibodies, anti-Ro/La antibodies, and complement levels through comprehensive autoimmune panels. Borderline results require repeat testing in 8-12 weeks with careful symptom monitoring rather than immediate treatment decisions.
Anti-dsDNA and Lupus Diagnosis – The Full Picture
How Anti-dsDNA Fits Into Lupus Diagnosis
The anti-dsDNA test functions as a critical diagnostic component within a comprehensive multi-test approach, working alongside clinical symptoms, physical examination findings, and additional laboratory markers to confirm systemic lupus erythematosus. The 2019 EULAR/ACR classification criteria for lupus diagnosis assign anti-dsDNA antibodies significant diagnostic weight—6 points in a system requiring 10 total points plus a mandatory positive ANA result—but explicitly recognize that no single lupus blood test definitively confirms the condition. Rheumatologists evaluate anti-dsDNA results within a framework that includes complement levels (C3, C4), complete blood counts showing cytopenias, urinalysis for proteinuria or cellular casts, and clinical manifestations across multiple organ systems.
The diagnostic process typically follows this sequence: initial ANA test positive screening (required entry criterion), followed by targeted autoimmune antibodies testing including anti-dsDNA, anti-Smith, anti-Ro/SSA, and anti-La/SSB antibodies. When anti-dsDNA appears alongside low complement levels and clinical features like malar rash, photosensitivity, oral ulcers, or serositis, the diagnostic certainty for systemic lupus erythematosus increases substantially. Approximately 65-85% of lupus patients demonstrate anti-dsDNA positivity at some point during their disease course, though levels may fluctuate significantly during periods of remission versus active lupus flare up.
International consensus panels emphasize that lupus diagnosis remains fundamentally clinical, with laboratory tests serving to support rather than replace careful medical evaluation. Dr. Michelle Petri from Johns Hopkins University’s Lupus Center notes that experienced rheumatologists consider the temporal relationship between symptoms and antibody development, family history of autoimmune conditions, medication exposures that might trigger drug-induced lupus, and response to initial therapeutic interventions when interpreting anti-dsDNA test results. This holistic approach prevents both overdiagnosis in patients with isolated positive lupus antibodies but no clinical disease, and underdiagnosis in those with seronegative lupus who meet clinical criteria despite negative double stranded DNA antibody testing.
Anti-dsDNA for Lupus Nephritis and Kidney Monitoring
Anti-dsDNA antibodies represent the single most valuable lupus kidney test biomarker, with persistently elevated or rising levels strongly predicting lupus nephritis development even before clinical symptoms emerge. Kidney involvement affects 40-60% of lupus patients during their disease course, making early detection through strategic anti-dsDNA monitoring absolutely critical for preventing irreversible kidney damage lupus complications. Research published in BMJ Open demonstrates that anti-dsDNA IgE antibodies may serve as non-invasive predictors of lupus nephritis, potentially identifying at-risk patients months before traditional markers like proteinuria or elevated creatinine become detectable.
Kidney Monitoring Action Steps When Anti-dsDNA Is Elevated:
- Schedule comprehensive renal panel including serum creatinine, blood urea nitrogen (BUN), and estimated glomerular filtration rate (eGFR) within 2 weeks
- Obtain complete urinalysis checking for proteinuria, hematuria, and cellular casts that indicate active lupus nephritis symptoms
- Monitor blood pressure at home twice daily, as hypertension often accompanies kidney involvement
- Request 24-hour urine protein collection or spot urine protein-to-creatinine ratio if initial urinalysis shows abnormalities
- Consider kidney biopsy consultation if anti-dsDNA levels exceed 200 IU/mL with any urinary abnormalities
- Maintain optimal hydration using tools like our water intake calculator to support kidney function during monitoring periods
The recommended monitoring frequency for lupus kidney disease surveillance depends on anti-dsDNA levels and clinical stability: patients with consistently negative or low-positive results (under 50 IU/mL) typically require testing every 6-12 months, while those with moderate elevation (50-150 IU/mL) need quarterly assessments, and individuals with high levels (over 150 IU/mL) often undergo monthly monitoring during treatment adjustments. This risk-stratified approach ensures appropriate resource utilization while maintaining vigilance for complications requiring urgent intervention.
When Anti-dsDNA Test Is NOT Enough
Relying exclusively on anti-dsDNA results creates significant diagnostic blind spots, as 15-35% of confirmed lupus patients never develop these antibodies despite active, sometimes severe disease. Complement levels—specifically C3 and C4 proteins—provide essential complementary information, with low complement frequently indicating active disease and immune complex consumption even when anti-dsDNA remains negative or borderline. Additional lupus diagnostic tests including anti-Smith antibodies (highly specific but present in only 25-30% of patients), anti-Ro/SSA antibodies (associated with photosensitivity and neonatal lupus risk), and anti-phospholipid antibodies (indicating thrombotic complications) complete the comprehensive serological evaluation.
Clinical correlation remains absolutely essential—no combination of lupus blood work definitively confirms or excludes diagnosis without careful consideration of symptoms, physical examination findings, and response to treatment over time. Patients may exhibit classic lupus manifestations including debilitating arthritis, severe photosensitive rashes, life-threatening serositis, or neurological complications despite persistently negative anti-dsDNA testing. The National Institute of Arthritis and Musculoskeletal and Skin Diseases emphasizes that lupus diagnosis requires integration of laboratory data with clinical judgment rather than algorithmic interpretation of individual test results.
What This Means For You: Taking Control of Your Diagnosis Journey
If your anti-dsDNA test is positive, request simultaneous complement testing (C3, C4) and complete urinalysis to assess disease activity and kidney involvement before your rheumatology appointment. Document your symptoms using our symptom checker tool to ensure comprehensive discussion of all concerning manifestations during consultation. If anti-dsDNA is negative but clinical suspicion for lupus remains high, advocate for expanded antibody panels including anti-Smith, anti-Ro, anti-La, and anti-RNP antibodies rather than accepting premature reassurance. Understanding that lupus diagnosis represents a clinical process spanning weeks to months—not a single test interpretation—helps manage expectations while ensuring thorough evaluation through systematic health monitoring approaches.
Monitoring, Treatment & Lifestyle Implications
How Often to Test Anti-dsDNA Levels
The frequency of anti-dsDNA testing varies dramatically based on your disease status, treatment response, and kidney involvement risk, making personalized monitoring schedules essential for optimal lupus blood work management. Newly diagnosed patients require more frequent testing to establish baseline patterns and assess initial treatment effectiveness, while those with stable disease on maintenance therapy can safely extend intervals between lupus lab results monitoring. Your rheumatologist adjusts testing frequency based on anti-dsDNA trends over time rather than rigid protocols, recognizing that individual patients demonstrate unique patterns of antibody fluctuation.
Recommended Anti-dsDNA Monitoring Schedule
Patients should request urgent anti-dsDNA retesting when experiencing new or worsening symptoms including unexplained fever lasting more than 3 days, sudden joint swelling affecting multiple areas, new skin rashes or worsening photosensitivity, chest pain with breathing (possible serositis), decreased urine output or foamy urine (lupus nephritis symptoms), or persistent severe fatigue despite adequate sleep. These clinical changes may signal lupus flare up before anti-dsDNA levels rise, though serial measurements help distinguish true disease activity from temporary symptom fluctuations.
What Your Results Mean for Treatment
Rising anti-dsDNA levels—particularly increases of 50% or more from baseline—often prompt rheumatologists to intensify immunosuppressive therapy even before clinical symptoms worsen. Treatment decisions integrate anti-dsDNA trends with complement consumption (declining C3/C4), organ-specific manifestations, and overall disease activity scores rather than responding to isolated laboratory values. Patients with persistently high anti-dsDNA test results exceeding 200 IU/mL combined with proteinuria typically require aggressive lupus nephritis treatment including high-dose corticosteroids, mycophenolate mofetil, or cyclophosphamide to prevent irreversible kidney damage lupus complications.
Conversely, declining anti-dsDNA levels during treatment suggest therapeutic response, though clinical improvement should parallel laboratory normalization. Some patients achieve clinical remission with normal complement levels while maintaining low-positive anti-dsDNA results (30-75 IU/mL), which may represent their individual baseline rather than active disease requiring escalation. The Lupus Foundation of America emphasizes shared decision-making between patients and rheumatologists when interpreting borderline results, balancing medication side effects against potential disease progression risks.
International Expert Consensus on Treatment Thresholds:
Dr. David Isenberg from University College London notes that European rheumatologists often adopt more conservative approaches to isolated anti-dsDNA elevations without clinical correlation, preferring to increase monitoring frequency before adding medications. In contrast, North American guidelines frequently recommend preemptive treatment intensification when anti-dsDNA doubles from baseline, even without overt symptoms, citing long-term organ preservation benefits. Asian-Pacific consensus statements highlight regional variations in anti-dsDNA test interpretation, with laboratories in Japan and South Korea using different reference ranges requiring adjusted clinical thresholds.
What This Means For You: Treatment Discussion Points
Bring printed copies of your anti-dsDNA trends over the past 6-12 months to rheumatology appointments, as patterns matter more than single values. Ask your doctor, “What is MY baseline anti-dsDNA level during stable disease?” to establish personalized treatment triggers rather than relying on generic reference ranges. If your rheumatologist recommends medication changes based on rising anti-dsDNA levels, inquire about complement status and urinalysis results to understand the complete picture justifying therapeutic adjustments.
Lifestyle and Test Results
While lifestyle modifications cannot directly lower anti-dsDNA antibodies—these autoantibodies reflect fundamental immune dysregulation rather than modifiable behaviors—comprehensive wellness strategies significantly impact overall lupus disease activity and may indirectly influence lupus blood work trends. Chronic psychological stress activates inflammatory pathways that can trigger lupus flare up episodes, though current evidence doesn’t demonstrate direct stress-to-anti-dsDNA causation. Quality sleep emerges as particularly crucial, with studies showing that lupus patients averaging less than 6 hours nightly experience more frequent disease flares and potentially higher autoimmune antibodies levels.
Evidence-Based Lifestyle Strategies for Lupus Management:
- Sleep optimization: Aim for 7-9 hours using our sleep calculator to determine ideal bedtimes based on your schedule, as inadequate rest correlates with increased inflammation markers
- UV protection: Rigorous sun avoidance and SPF 50+ sunscreen prevents photosensitivity flares that may trigger rising anti-dsDNA levels in susceptible patients
- Anti-inflammatory nutrition: Mediterranean diet patterns emphasizing omega-3 fatty acids, colorful vegetables, and minimal processed foods support immune regulation, though specific dietary changes don’t normalize lupus diagnostic tests
- Stress management: Cognitive behavioral therapy, mindfulness meditation, and structured relaxation reduce cortisol dysregulation associated with disease activity
- Moderate exercise: Regular low-impact activity like walking, swimming, or yoga improves fatigue and mood without triggering flares in most stable patients
- Smoking cessation: Tobacco use worsens lupus outcomes and may impair treatment response, though direct effects on anti-dsDNA levels remain unclear
Maintaining stable body weight through balanced nutrition assessed via our BMI calculator helps minimize cardiovascular risks that compound lupus-related complications, though weight changes don’t directly influence double stranded DNA antibody production. Some patients report symptom improvements after eliminating specific foods (commonly alfalfa sprouts, which contain L-canavanine that may trigger lupus activity), though rigorous dietary restriction lacks strong evidence for impacting lupus lab results.
Cost, Insurance, and Access
Anti-dsDNA testing typically costs between $50-$250 per test depending on the laboratory method employed, facility type (hospital versus independent lab), and geographic region, with ELISA methods generally less expensive than Farr assay or CLIFT immunofluorescence. Most commercial insurance plans cover anti-dsDNA testing when medically necessary—meaning ordered by a physician for diagnosis or monitoring of known lupus—though prior authorization requirements increasingly delay access to specialty immunology panels. Medicare Part B covers the test at 80% of the Medicare-approved amount after deductible for beneficiaries with documented medical necessity, while Medicaid coverage varies by state with some requiring rheumatology referrals before authorizing autoimmune testing.
Strategies for Managing Testing Costs:
- Request itemized laboratory bills to verify you’re charged for tests actually performed, not comprehensive panels you didn’t need
- Ask your rheumatologist to order only essential tests at each visit rather than reflexive comprehensive autoimmune panels
- Utilize hospital-affiliated laboratories when your insurance has negotiated favorable rates compared to independent facilities
- Explore patient assistance programs through the Lupus Foundation when facing financial barriers to recommended monitoring
- Appeal insurance denials by requesting your doctor provide detailed medical necessity documentation citing rising symptoms or previous lupus nephritis
Patients without insurance can access reduced-cost anti-dsDNA testing through federally qualified health centers, county health departments, and university medical center charity care programs, though availability varies significantly by location. Some direct-to-consumer laboratory companies offer anti-dsDNA testing for $75-$150 without insurance, but results require professional interpretation—never make treatment decisions based on self-ordered testing without rheumatology consultation.
Patient Questions, Expert Answers & Next Steps
1. Q: Can you have lupus with negative anti-dsDNA?
Yes, absolutely. Between 15-35% of people with confirmed systemic lupus erythematosus consistently test negative for anti-dsDNA antibodies throughout their disease course. These patients—termed “seronegative lupus”—receive diagnosis based on clinical symptoms, positive ANA test results, low complement levels, and other lupus antibodies like anti-Smith or anti-Ro. Your rheumatologist evaluates the complete clinical picture rather than relying on any single lupus blood test for diagnosis.
2. Q: What does a borderline anti-dsDNA result mean?
Borderline results (typically 30-75 IU/mL) represent uncertain clinical significance requiring follow-up testing in 8-12 weeks alongside careful symptom monitoring. These equivocal anti-dsDNA test results may indicate early lupus diagnosis, laboratory variation, or cross-reactivity with other conditions. Never make treatment decisions based solely on borderline lupus lab results without comprehensive rheumatology evaluation and repeat testing.
3. Q: Does anti-dsDNA predict lupus nephritis symptoms?
High anti-dsDNA levels (especially above 150-200 IU/mL) strongly correlate with lupus kidney disease development, with studies showing 60-80% increased risk compared to patients with negative or low-positive results. Rising anti-dsDNA levels combined with declining complement often precede kidney damage lupus complications by weeks to months, enabling proactive intervention. Regular urinalysis monitoring alongside kidney health tracking helps detect lupus nephritis early when treatment proves most effective.
When to Call Your Doctor Immediately
Contact your rheumatologist or seek urgent medical evaluation if you experience these warning signs suggesting active lupus flare up or kidney involvement:
- New or worsening kidney symptoms: Significant leg/facial swelling, foamy or dark-colored urine, decreased urine output, or sudden unexplained weight gain
- Rapid symptom progression: High fever above 101°F lasting more than 48 hours, severe chest pain worsening with breathing, or sudden severe headache with confusion
- Known anti-dsDNA elevation: If previous lupus blood work showed rising double stranded DNA antibody levels and you develop new symptoms
- Neurological changes: New seizures, severe cognitive difficulties, vision changes, or stroke-like symptoms requiring emergency evaluation
Don’t wait for your scheduled follow-up appointment when experiencing these concerning manifestations—early intervention prevents irreversible complications and improves long-term outcomes in systemic lupus erythematosus management.
Your Action Plan
Follow these evidence-based steps to optimize your lupus diagnostic tests interpretation and care coordination:
- Request comprehensive lupus panels including anti-dsDNA, complement levels (C3, C4), complete blood count, and urinalysis rather than isolated testing
- Obtain specific numerical values for all lupus test results explained, not just “positive” or “negative” designations, to track trends over time
- Document baseline anti-dsDNA levels during stable disease to establish personalized treatment thresholds with your rheumatologist
- Schedule rheumatology follow-up within 2 weeks if anti-dsDNA test results exceed 150 IU/mL or show significant increases from previous values
- Monitor symptoms systematically using our symptom checker tool to provide detailed information during medical appointments
- Maintain treatment adherence even when feeling well, as autoimmune antibodies may remain elevated despite symptom improvement
- Review test methodology with your laboratory to understand whether results used ELISA, Farr assay, or CLIFT methods affecting interpretation
Understanding your anti-dsDNA test empowers informed discussions with your healthcare team while maintaining realistic expectations about what these lupus blood work values can and cannot tell you about your prognosis. For comprehensive lupus management resources, visit the National Institute of Arthritis and Musculoskeletal and Skin Diseases for patient education materials.
Medical Disclaimer
This article provides educational information about anti-dsDNA testing and lupus lab results for informational purposes only and does not constitute medical advice, diagnosis, or treatment recommendations. Always consult your rheumatologist or qualified healthcare provider to interpret your specific anti-dsDNA test results within the context of your complete medical history, symptoms, and additional diagnostic findings. Never start, stop, or modify lupus treatments based solely on information from this or any online resource without direct physician guidance. Individual results vary significantly, and personalized medical evaluation remains essential for appropriate lupus diagnosis and management decisions.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.