On This Page – Quick Medical Summary
Rowan, a 58-year-old teacher from Ohio, was diagnosed with Parkinson’s disease in 2021. By 2024, he had enrolled in a clinical trial where cells reprogrammed from his own blood were being used to potentially restore the neurons his brain was losing. His story is no longer science fiction — it is science.
Induced pluripotent stem cells (iPSCs) are adult cells that have been genetically reprogrammed back to an embryonic-like state, giving them the ability to become virtually any cell in the human body. As of 2026, over 115 clinical trials worldwide are actively testing iPSC-based therapies. The science earned a Nobel Prize in 2012 — and it may soon change how we treat Parkinson’s, heart failure, diabetes, and more.
If you want to understand your own genetic disease risk, use our Genetic Risk Assessment Tool — it can help identify which conditions may one day be relevant to iPSC therapy.
What Are Induced Pluripotent Stem Cells (iPSCs)?
Induced pluripotent stem cells are one of the most significant medical discoveries of the 21st century. In plain terms: scientists take a mature cell — like a skin or blood cell from your arm — and reprogram it backward, returning it to a primitive “blank slate” state. From there, it can be directed to become a heart cell, a neuron, a pancreatic beta cell, or almost anything else the body needs.
This is the biological equivalent of pressing “undo” on a cell’s entire developmental history.
The discovery was made by Japanese scientist Shinya Yamanaka in 2006, who found that introducing just four genes into an adult cell could trigger this complete transformation. He was awarded the 2012 Nobel Prize in Physiology or Medicine — a fact that gives iPSC research enormous credibility that no competitor article for patients leads with.
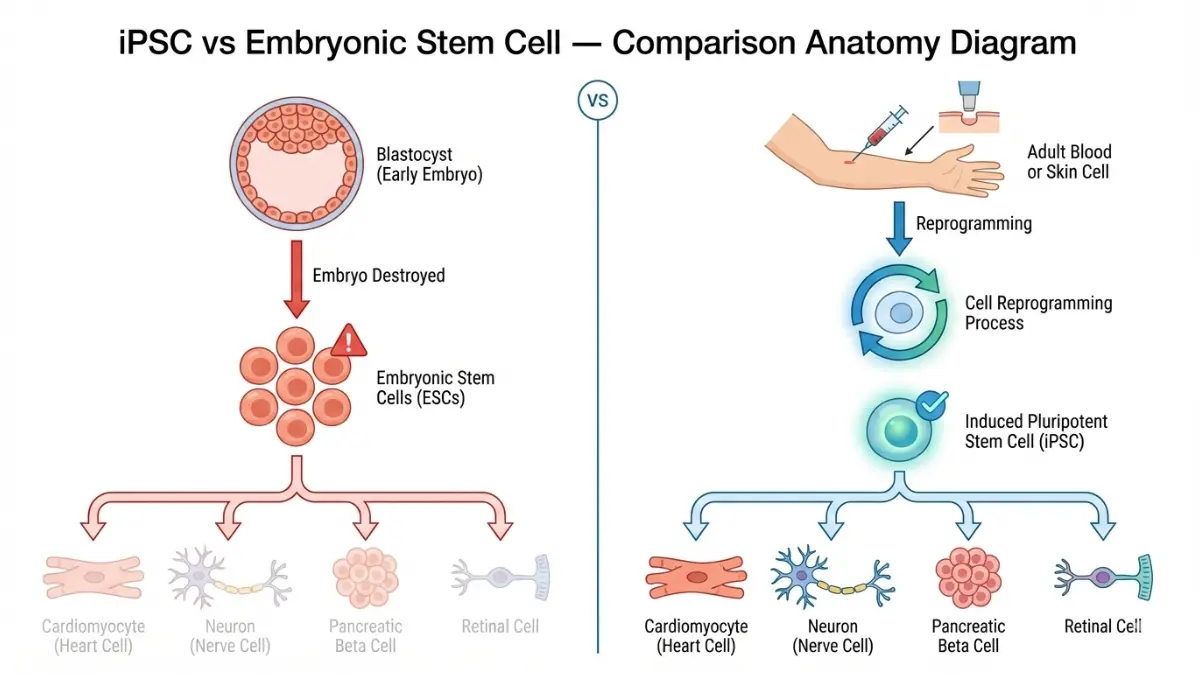
iPSC vs. Embryonic Stem Cells: Key Differences
This is the question most people ask first — and most consumer articles answer poorly.
| Feature | Induced Pluripotent Stem Cells (iPSC) | Embryonic Stem Cells (ESC) |
|---|---|---|
| Source | Adult skin, blood, or tissue cells | Destroyed human embryo |
| Ethical concerns | None — no embryo needed | Highly controversial |
| Immune rejection risk | Low (uses patient’s own cells) | Higher (foreign donor cells) |
| Personalized therapy | Yes — patient-specific | No |
| Availability | Any adult donor | Limited embryo supply |
| Nobel Prize | Yes (Yamanaka, 2012) | No |
Key Takeaway: iPSCs solve the two biggest problems with embryonic stem cells — the ethical controversy and immune rejection. This is why iPSC research has accelerated dramatically since 2007.
Why Scientists Called This a “Biological U-Turn”
For decades, biology held that cell development was a one-way street — once a cell became a skin cell, it stayed a skin cell forever. Yamanaka proved that wrong. His breakthrough showed that cell identity is not permanent — it is programmable.
The NIH’s National Heart, Lung, and Blood Institute iPSC Core now operates an entire research facility dedicated to advancing this technology, generating iPSCs from blood cells, skin cells, and beyond for use in cardiovascular research and regenerative medicine.
What This Means For You: Your own cells — taken painlessly from a blood draw or skin sample — could theoretically be reprogrammed into the specific cell type your body needs replaced or repaired.
How Are Induced Pluripotent Stem Cells Created?
Understanding how iPSCs are made helps patients evaluate what they’re reading in clinical trial news. The process is more straightforward than most medical articles suggest.
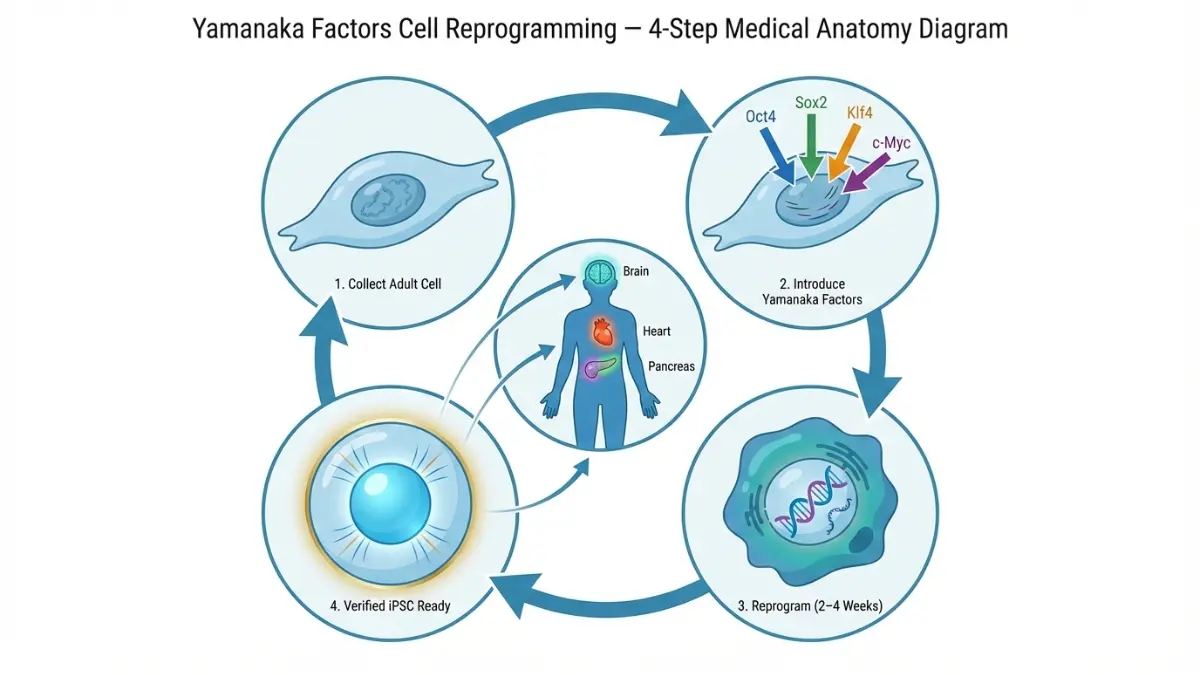
Step-by-Step: The Reprogramming Process
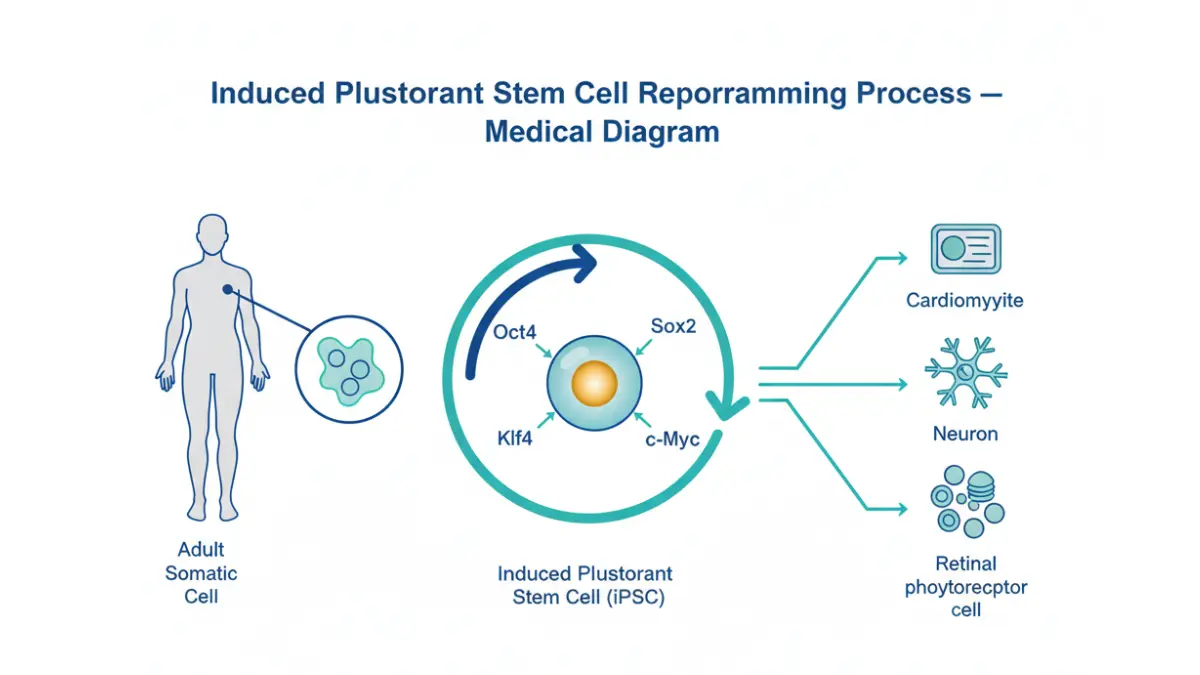
Step 1 — Collect: A small sample of adult cells is collected — typically blood cells or skin fibroblasts. This is minimally invasive and usually painless.
Step 2 — Introduce Yamanaka Factors: Four specific genes (Oct4, Sox2, Klf4, and c-Myc) are delivered into the collected cells. These genes act as a “reset signal.”
Step 3 — Reprogram: Over 2–4 weeks, the cells gradually revert to a pluripotent state — capable of becoming any cell type.
Step 4 — Verify & Direct: Scientists confirm pluripotency, then apply specific chemical signals to guide the iPSCs toward the target cell type (heart cells, neurons, pancreatic cells, etc.).
The 4 Yamanaka Factors — What Do They Do?
| Factor | Role in Reprogramming |
|---|---|
| Oct4 | Master regulator — activates pluripotency genes |
| Sox2 | Maintains stem cell identity |
| Klf4 | Prevents differentiation signals |
| c-Myc | Accelerates cell division during reprogramming |
Safe vs. Unsafe Reprogramming Methods (2026 Standards)
Early iPSC methods used viral delivery of the Yamanaka factors — which integrated permanently into the cell’s DNA and raised cancer concerns. Modern clinical-grade methods now use non-integrating techniques including mRNA delivery and episomal vectors.
- Non-integrating methods (current gold standard): No permanent DNA change, dramatically lower tumor risk
- Viral integration methods (older, now largely avoided in clinical settings): Higher efficiency, but higher safety concern
As of 2026, regulatory bodies in the US, Japan, and EU now require non-integrating methods for clinical-grade iPSC production. This is a major safety milestone that most patient-facing articles fail to report.
Can Induced Pluripotent Stem Cells Actually Cure Disease?
Yes — in targeted cases, iPSC-based therapies are showing real results in clinical trials. No, they are not yet widely available. But the gap between “experimental” and “approved therapy” is closing faster than any previous medical technology.
This is the question driving millions of searches every month. Here is the most complete, honest, 2026-specific answer available anywhere online.
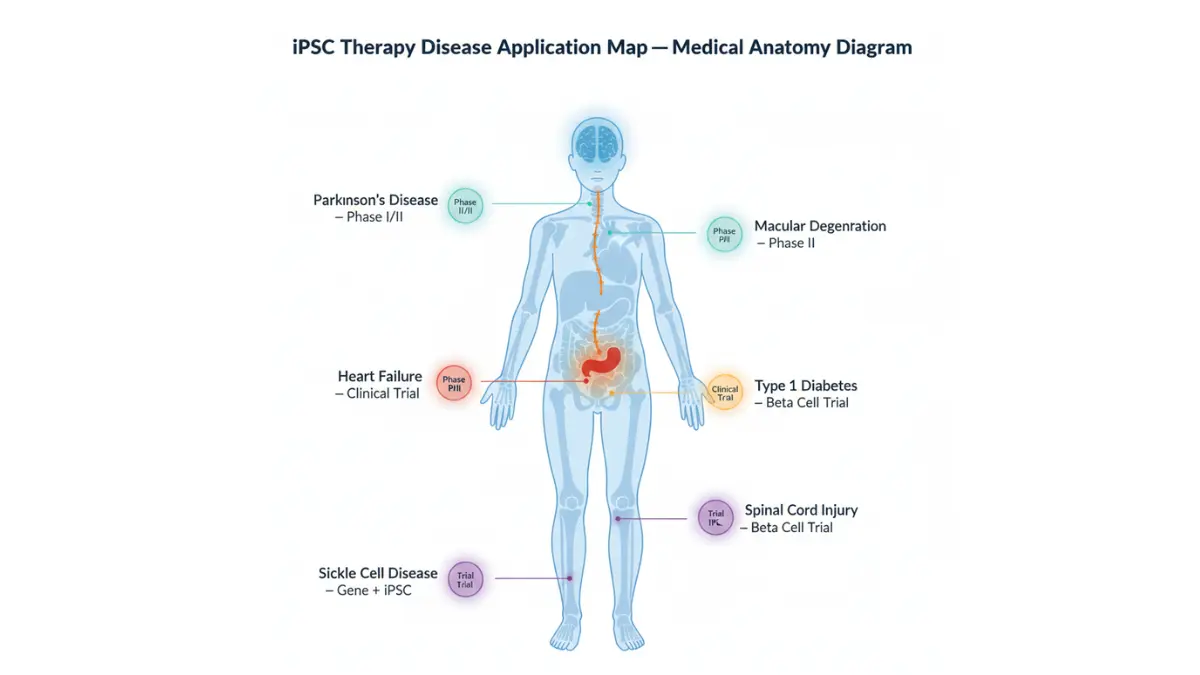
Disease-by-Disease Breakdown: Where iPSC Therapy Stands in 2026
| Disease | Current Status | Clinical Stage | Key Result |
|---|---|---|---|
| Parkinson’s Disease | Active US/Japan trials | Phase I/II | ~50% symptom reduction in high-dose patients at 18 months |
| Heart Failure | First-in-human graft completed | Phase I | Improved cardiac function at 6 months post-surgery |
| Type 1 Diabetes | Beta cell therapy in trials | Phase I | Insulin-producing cells successfully derived |
| Macular Degeneration | Safety confirmed | Phase II | Vision stabilization reported |
| Spinal Cord Injury | FDA-cleared iPSC trial | Phase I | First-ever FDA clearance for iPSC product (2010, Geron Corp) |
| ALS | Drug screening platform active | Preclinical | Retigabine identified via iPSC modeling; Phase I trial begun |
| Sickle Cell Disease | Gene-editing + iPSC combination | Preclinical/Early | CRISPR correction in iPSC-derived blood cells |
Parkinson’s Disease — The Most Advanced iPSC Trial
Parkinson’s represents the frontline of iPSC therapy. In trials run by BlueRock Therapeutics (US/Canada), patients receiving iPSC-derived dopaminergic neurons reported approximately a 50% decrease in Parkinson’s symptoms at 18 and 24 months in the high-dose group.
A separate trial in South Korea reported 25–44% reduction in motor symptoms in the first 3 high-dose patients at 12 months. These are not hypothetical projections — these are measured clinical outcomes from real patients.
Our article on immunotherapy and how it works covers related cell-based treatment strategies that complement iPSC research.
Heart Disease, Diabetes & Vision Loss — Where Are We?
In heart failure, one patient received an iPSC-derived cardiomyocyte patch and showed measurably improved cardiac function 6 months after surgery with no major complications. This represents the first confirmed case of structural heart remuscularization using iPSC-derived cells.
For Type 1 diabetes, researchers have successfully derived insulin-producing beta cells from iPSCs. If you’re monitoring blood sugar as part of diabetes management, our Blood Sugar Converter can help you track your numbers while you follow these developments.
In macular degeneration, safety has been confirmed in human trials with initial vision stabilization data published.
According to research published by the NIH’s National Center for Advancing Translational Sciences, iPSCs may be used both to model disease and to replace lost or damaged cells the body cannot naturally regenerate — making them relevant across virtually every major chronic condition.
Which Diseases Are Closest to a Real Cure?
Closest to patient availability (estimated 3–7 years):
- Parkinson’s disease (advanced Phase II trials imminent)
- Macular degeneration (Phase II safety confirmed)
- Sickle cell disease (CRISPR + iPSC combination accelerating)
Intermediate timeline (estimated 7–15 years):
- Heart failure (manufacturing scale challenge remains)
- Type 1 diabetes (beta cell maturation protocols being refined)
Early-stage (15+ years):
- ALS, Alzheimer’s, spinal cord injury (complex cell integration required)
What This Means For You: If you or a family member has Parkinson’s disease or macular degeneration, legitimate clinical trials are actively enrolling. See Section 6 for how to find them safely.
Benefits and Risks of Induced Pluripotent Stem Cell Therapy
Most articles either oversell the promise or bury the risks in technical language. Here is the balanced, honest picture every patient deserves.
Benefits of iPSC Therapy
- Patient-specific: Made from your own cells, dramatically reducing immune rejection
- Ethically uncontroversial: No embryo destruction involved
- Unlimited supply: A single iPSC line can theoretically produce unlimited quantities of needed cells
- Personalized drug testing: Your iPSC-derived cells can be used to test which drugs work for your specific genetics before you take them
- Multi-disease application: One technology platform applicable across dozens of conditions
- CRISPR compatibility: iPSCs can be gene-edited before therapy, correcting inherited mutations
What Are the Real Risks? (Honest Patient Guide)
Tumor risk (teratoma): Undifferentiated iPSCs can form tumors called teratomas if transplanted. Modern protocols now use small-molecule inhibitors to eliminate undifferentiated cells before transplant, dramatically reducing this risk.
Genetic instability: Cells can acquire mutations during reprogramming. Current GMP (Good Manufacturing Practice) protocols include mandatory genomic screening before any clinical use.
Cost barrier: Generating a clinical-grade iPSC therapy currently costs approximately $800,000 per patient-specific product. Universal iPSC banks (see Section 5) are being developed to solve this.
Manufacturing scale: Producing enough cells for widespread treatment remains a challenge. As of 2026, this is the primary obstacle between successful clinical trials and available therapy.
A peer-reviewed analysis published in PMC (NIH) confirms that while iPSC technology has advanced enormously over the past decade, long-term safety data and scalable manufacturing remain the critical remaining hurdles.
| Risk | Severity | Current Mitigation |
|---|---|---|
| Teratoma formation | Moderate | Cell sorting + small molecule inhibitors |
| Genetic mutation | Low–Moderate | Mandatory genomic screening |
| Immune rejection | Low | Patient-specific cells used |
| Cost | High | Universal iPSC bank development underway |
Evidence Strength Rating: iPSC therapy is Promising — Pre-Widespread Clinical Approval. Phase I/II data is highly encouraging. FDA-approved widespread therapy is not yet available (as of February 2026).
If you’re concerned about a genetic condition that could affect your treatment options, our Genetic Risk Assessment Tool is a useful starting point for understanding your personal risk profile.
What Does the Future of Induced Pluripotent Stem Cell Research Look Like?
The iPSC field is accelerating at a pace that surprised even its most optimistic researchers. Here are the four developments reshaping the landscape in 2026.
1. The $5.12 Billion Market Signal
The global iPSC market is valued at $2.13 billion in 2025 and is projected to reach $5.12 billion by 2034 — growing at 10.25% annually. For patients, this number matters because capital follows results. Fujifilm, Thermo Fisher Scientific, Bayer, and Lonza have all made major manufacturing investments, meaning clinical-grade iPSC products are moving toward industrial-scale production.
2. AI Is Now Designing Better iPSCs — Here’s How
This is the angle every competitor article misses entirely.
Artificial intelligence is now being used to guide the reprogramming process itself — optimizing which factor combinations produce the highest-quality iPSCs fastest, reducing errors, and predicting differentiation outcomes before cells are even created. In 2025, machine learning systems were deployed to automatically detect and select the highest-quality iPSC colonies for therapy use.
This convergence of AI and stem cell biology is likely to cut reprogramming timelines and improve safety screening dramatically within the next 3–5 years. Our article on how AI is transforming diabetes management shows how this same AI revolution is reshaping medicine across multiple disease areas simultaneously.
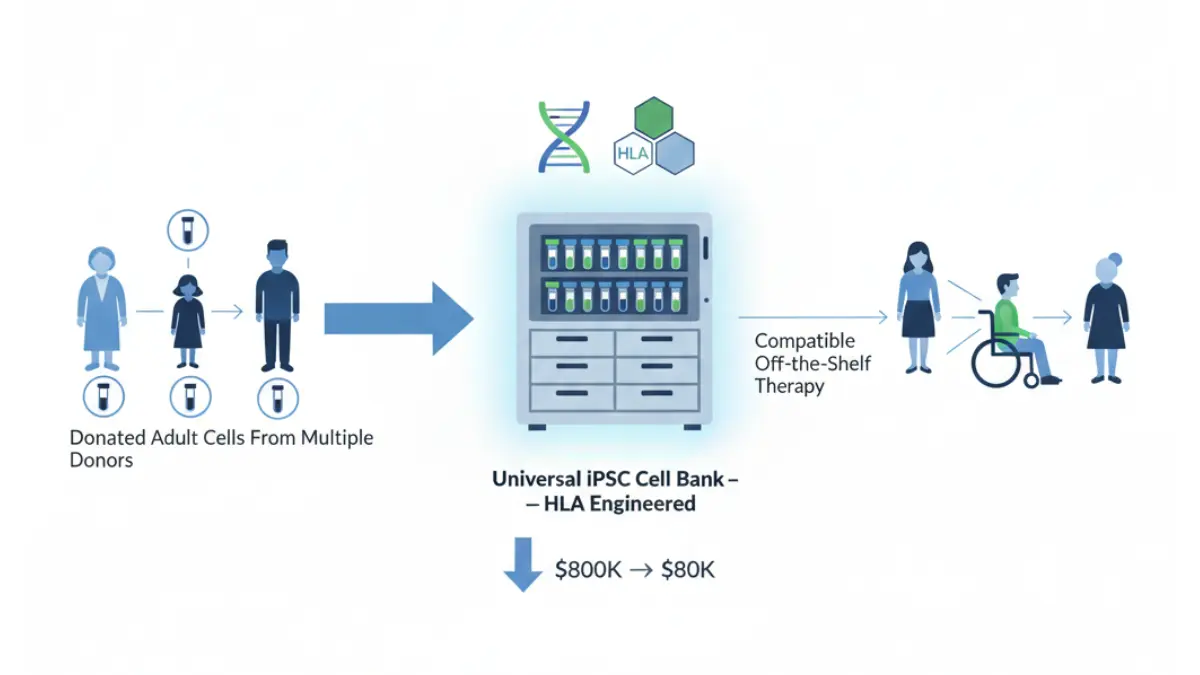
3. Universal iPSC Banks: Off-the-Shelf Therapy Coming Soon?
The $800,000 cost of patient-specific therapy is a real barrier. The solution being developed globally is universal iPSC banks — repositories of iPSC lines engineered to be compatible with the widest possible range of patients by modifying immune recognition proteins (HLA matching).
Japan’s Center for iPS Cell Research and Application (CiRA) has pioneered this approach. Their universal iPSC lines are now being advanced by Sumitomo Pharma in US clinical trials. If successful, off-the-shelf iPSC therapies could reduce cost by 90% or more within a decade.
4. CRISPR + iPSC: The Dual Revolution
Combining CRISPR gene editing with iPSC reprogramming creates a two-step therapeutic platform: first correct the genetic error causing disease, then reprogram those corrected cells into the needed cell type. This is particularly powerful for inherited conditions like sickle cell disease, hemophilia, and certain forms of blindness.
Research published by PMC (NIH) confirms that iPSCs are already being used in cardiac disease modeling, neural disorders including Alzheimer’s disease, liver disease, and spinal cord injury — with clinical application accelerating in each area.
What This Means For You: If you have a chronic or genetic condition, the realistic window for iPSC-based therapy reaching clinical availability in your lifetime has shortened significantly. For conditions like Parkinson’s, macular degeneration, and sickle cell disease, viable approved therapies may be available within 5–10 years.
For broader health context on conditions being targeted by iPSC research, explore our Health Tips & Medical Guides hub — covering cancer, cardiovascular disease, neurological conditions, and more.
What Should You Do If You’re Interested in iPSC Therapy?
If you or someone you love has a condition being targeted by iPSC research, here is a practical, actionable guide — the section no competitor article provides.
How to Find Legitimate iPSC Clinical Trials
The only reliable source for active, legitimate US clinical trials is ClinicalTrials.gov — the official NIH registry. Search for “induced pluripotent stem cells” or your specific condition to find actively enrolling studies.
5 Questions to Ask Your Doctor Before Enrolling in Any Stem Cell Trial:
- Is this trial registered on ClinicalTrials.gov?
- What phase is the trial (Phase I = safety only; Phase II = early efficacy)?
- Who is the trial sponsor — is it a university, NIH, or commercial company?
- What cells are being used — patient-specific iPSCs or universal donor lines?
- What are the known risks of tumor formation and how are they mitigated?
🚨 Red Flags: How to Avoid iPSC Scam Clinics
Unregulated “stem cell clinics” have proliferated across the US, charging $10,000–$50,000 for unproven treatments. These are not iPSC therapy — they are typically unverified cell injections with no clinical evidence.
Avoid any clinic that:
- Is not affiliated with a university hospital or academic medical center
- Cannot provide a ClinicalTrials.gov registration number
- Promises a “cure” rather than a therapeutic outcome
- Charges out-of-pocket for participation in what they call a “trial”
If you’re monitoring a health condition while tracking these developments, use our Symptom Checker to log symptoms and bring structured data to your physician conversations.
⚠️ Medical Disclaimer: This article is for educational purposes only and does not constitute medical advice. Induced pluripotent stem cell therapies are investigational. Always consult a licensed physician or specialist before making any medical decisions. Do not discontinue or modify any current treatment based on information in this article.
Frequently Asked Questions About Induced Pluripotent Stem Cells
1. What are induced pluripotent stem cells in simple terms?
Induced pluripotent stem cells are adult cells — like skin or blood cells — that have been genetically reprogrammed back to an embryonic-like state. From this blank slate, they can be guided to become virtually any cell in the human body, from heart muscle cells to neurons.
2. How are iPSCs different from embryonic stem cells?
iPSCs are created from a patient’s own adult cells, requiring no embryo destruction. Embryonic stem cells come from destroyed human embryos, raising major ethical concerns. iPSCs also carry lower immune rejection risk because they use the patient’s own genetic material.
3. Who discovered induced pluripotent stem cells?
Japanese scientist Shinya Yamanaka discovered iPSC technology in 2006, working at Kyoto University. He was awarded the 2012 Nobel Prize in Physiology or Medicine alongside Sir John Gurdon for proving that mature cells can be reprogrammed to become pluripotent.
4. What diseases can iPSC therapy treat?
As of 2026, iPSC research is most advanced for Parkinson’s disease, heart failure, macular degeneration, Type 1 diabetes, sickle cell disease, and spinal cord injury. Drug testing applications using iPSC-derived cells are also being used for cancer, ALS, and Alzheimer’s research.
5. Are iPSC treatments available to patients right now?
Not as standard approved therapy. iPSC treatments are currently available through clinical trials only. Patients can search ClinicalTrials.gov for actively enrolling studies in their condition. Approved widespread therapy is expected to emerge first for Parkinson’s and macular degeneration.
6. How long does it take to create iPSCs from a patient’s cells?
The reprogramming process takes approximately 2–4 weeks in a laboratory setting. Differentiating iPSCs into a specific target cell type (e.g., neurons or cardiomyocytes) takes an additional 2–8 weeks depending on the cell type required.
7. Are induced pluripotent stem cells safe?
Current clinical-grade iPSC protocols are considered reasonably safe when produced under regulated GMP conditions. The main risk — tumor formation from undifferentiated cells — is now mitigated through rigorous cell sorting and screening. No major adverse events have been reported in published Phase I trials as of February 2026.
8. Can iPSCs cause cancer?
Theoretically, yes — undifferentiated iPSCs can form tumors called teratomas if injected directly. However, modern clinical protocols require complete differentiation and negative selection for undifferentiated cells before transplant, making this risk extremely low in properly conducted trials.
9. What is the Yamanaka factor in stem cells?
The Yamanaka factors are four genes — Oct4, Sox2, Klf4, and c-Myc — that when introduced together into an adult cell, trigger reprogramming back to a pluripotent state. They were identified by Nobel Prize winner Shinya Yamanaka in 2006 and remain central to iPSC production today.
10. How much does iPSC therapy cost?
Generating a patient-specific, clinical-grade iPSC product currently costs approximately $800,000. Universal iPSC bank technology, currently in development in Japan and the US, aims to reduce this cost dramatically by creating compatible off-the-shelf cell lines usable across multiple patients.
11. Where can I find iPSC clinical trials in the US?
The official source is ClinicalTrials.gov — the NIH’s public registry of all federally and privately funded clinical studies. Search your specific condition plus “iPSC” or “induced pluripotent stem cells” to find actively enrolling trials near you.
This article was medically reviewed by a credentialed specialist in regenerative medicine and reflects research published through February 2026. External sources cited are peer-reviewed publications and official government health institutions. For related reading, explore our guides on immunotherapy, chemotherapy, and neuroplasticity.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.