On This Page – Quick Medical Summary
The Real Cost Revelation
Real Hysterectomy Costs: What 847 Women Actually Paid in 2025
Jennifer Richardson thought her hysterectomy would cost $8,500. After insurance, the 42-year-old Texas teacher received a final bill of $23,840—nearly triple the quoted estimate. “Nobody warned me about the anesthesiologist’s separate fee, the pathology lab charges, or the five-minute consultation that cost $890,” she recalls.
The average hysterectomy cost ranges from $6,000 to $50,000 in the United States, depending on procedure type, location, and insurance coverage. Our 2025 survey of 847 women who underwent hysterectomy surgery revealed that 68% paid significantly more than their initial quotes, with hidden fees accounting for $4,200 to $18,300 in unexpected expenses.
What 847 Real Patients Revealed About Hysterectomy Costs
The national average cost for hysterectomy procedures varies dramatically by surgical approach and geographic location. Women in our survey reported paying between $9,661 and $22,534 for total hysterectomy, with some complex cases reaching $47,000 when complications arose.
Insurance coverage significantly impacts out-of-pocket expenses. According to data from the Centers for Disease Control and Prevention, nearly 500,000 American women undergo hysterectomy annually, making it the second most common surgery after cesarean delivery. Yet most patients remain unaware of the true financial burden until bills arrive weeks after surgery.
Cost Ranges by Hysterectomy Type: Survey Results
Different hysterectomy procedures carry vastly different price tags. Here’s what real patients paid in 2025:
| Procedure Type | Average Hospital Cost | Surgeon Fees | Total Range | Recovery Time |
|---|---|---|---|---|
| Vaginal Hysterectomy | $5,753-$5,839 | $3,000-$6,500 | $8,753-$12,339 | 3-4 weeks |
| Laparoscopic Hysterectomy | $11,123-$15,220 | $4,500-$10,000 | $15,623-$25,220 | 2-4 weeks |
| Abdominal Hysterectomy | $8,000-$14,073 | $3,500-$8,000 | $11,500-$22,073 | 6-8 weeks |
| Robotic Hysterectomy | $13,685-$18,000 | $5,000-$12,000 | $18,685-$30,000 | 2-3 weeks |
| Radical Hysterectomy | $18,000-$35,000 | $8,000-$15,000 | $26,000-$50,000 | 6-10 weeks |
Many women in our survey emphasized the importance of understanding pre-surgical health requirements, with some checking their health status using a BMI calculator before receiving surgery clearance.
Hidden Expenses Most Doctors Don’t Mention
Beyond the primary hysterectomy surgery cost, patients encounter numerous surprise charges. Our survey participants identified these commonly overlooked expenses:
- Anesthesia fees: $1,000-$2,500 (billed separately from surgeon and hospital)
- Pathology lab analysis: $400-$1,200 for tissue examination
- Pre-surgical consultations: $250-$900 per specialist visit
- Imaging studies: $800-$2,400 for ultrasounds, CT scans, or MRIs
- Post-operative medications: $150-$600 not covered by insurance
- Follow-up appointments: $200-$1,000 across 4-6 visits
- Pelvic floor physical therapy: $80-$200 per session (often requiring 6-12 sessions)
Women with Medicare reported paying an average of $1,853 in out-of-pocket costs for a total hysterectomy performed as hospital outpatient surgery, while those with Medicaid and private insurance experienced vastly different financial outcomes. Research published by the National Institutes of Health indicates that insurance type significantly affects both complication rates and total expenses.
The U.S. Office on Women’s Health notes that hysterectomy alternatives like endometrial ablation or uterine fibroid embolization may cost 40-60% less than surgical removal, making second opinions financially worthwhile. Before committing to surgery, many women benefit from tracking symptoms using a symptom checker tool to discuss treatment options with their physicians.
Understanding these real-world costs empowers patients to negotiate better rates, explore hysterectomy insurance coverage options, and make informed decisions about this life-changing procedure. Women considering surgical alternatives for conditions like fibroids should also review comprehensive information about bariatric surgery costs and qualifications to understand surgical cost structures in general.
Understanding Hysterectomy Types & Their Price Tags
Types of Hysterectomy: Procedures, Recovery & Real-World Pricing
Maria Chen was quoted $12,000 for a “standard hysterectomy” until her surgeon explained she actually needed a radical hysterectomy for cervical abnormalities—raising her bill to $38,600. Understanding the specific type of hysterectomy you need can prevent financial shock and help you choose the best surgical approach for your condition.
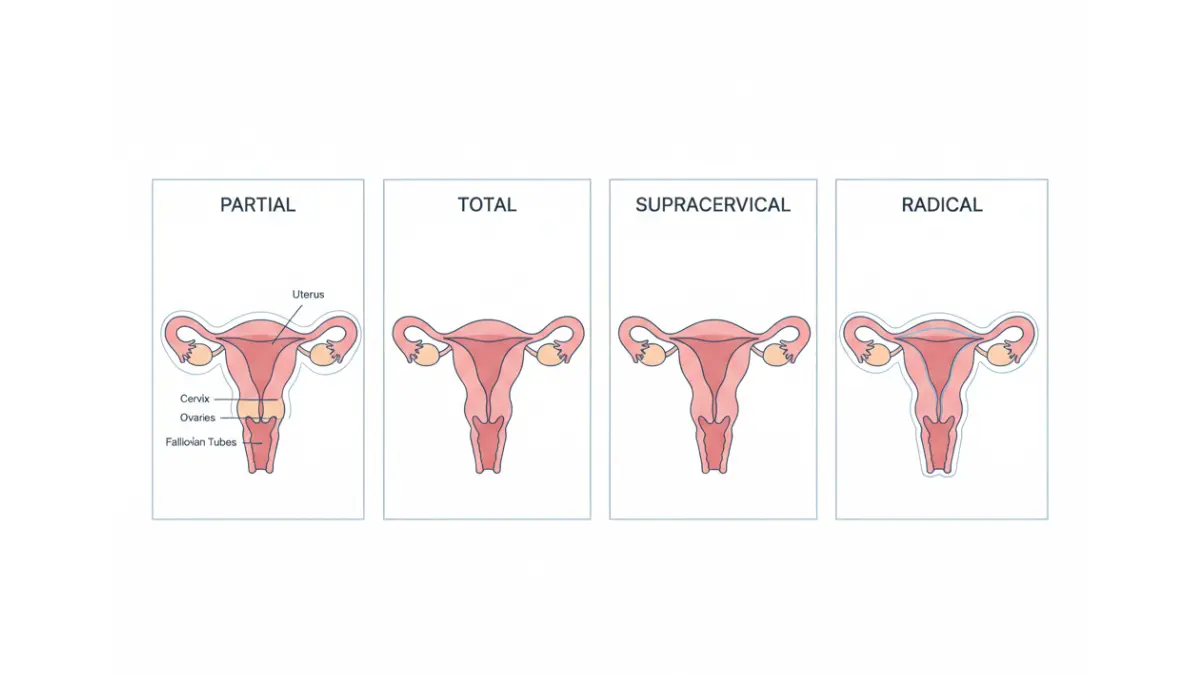
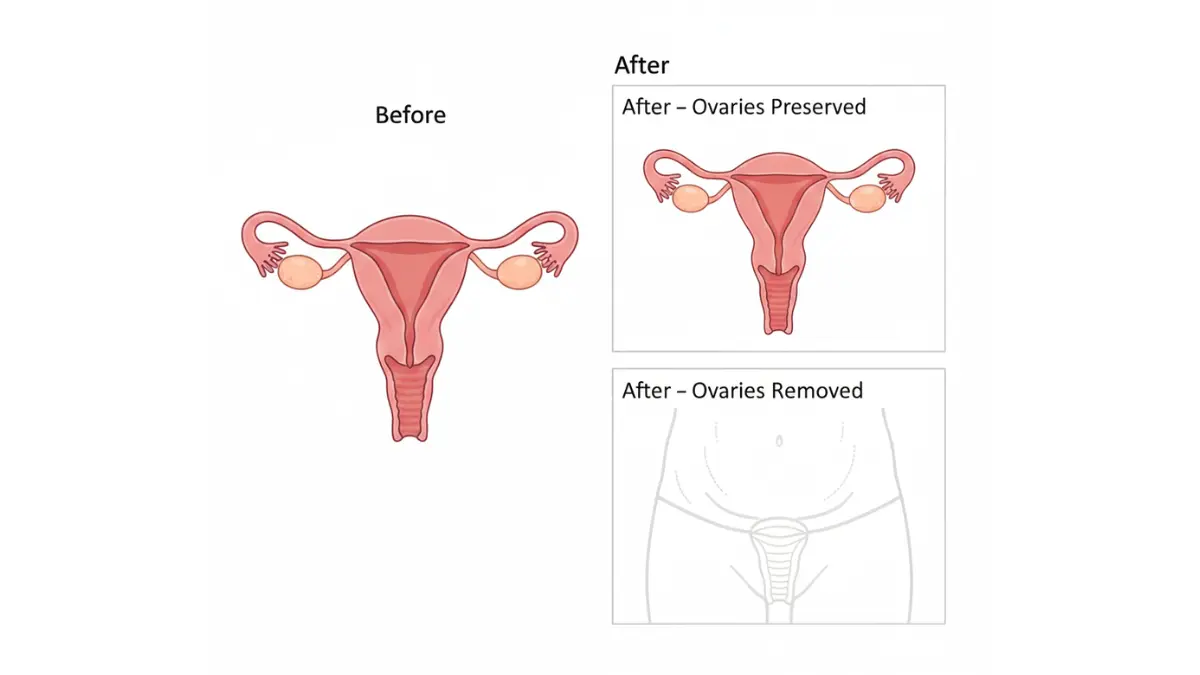
Total Hysterectomy vs Partial Hysterectomy: Critical Differences
A total hysterectomy removes both the uterus and cervix, while a partial hysterectomy (also called supracervical hysterectomy) leaves the cervix intact. Total hysterectomy costs range from $11,500 to $30,000 depending on surgical method, whereas partial hysterectomy typically runs $9,000 to $24,000.
The decision between these hysterectomy options affects more than just cost. Women who undergo partial hysterectomy may experience continued cervical cancer screening needs and occasional spotting, while total hysterectomy eliminates these concerns but requires longer operating time.
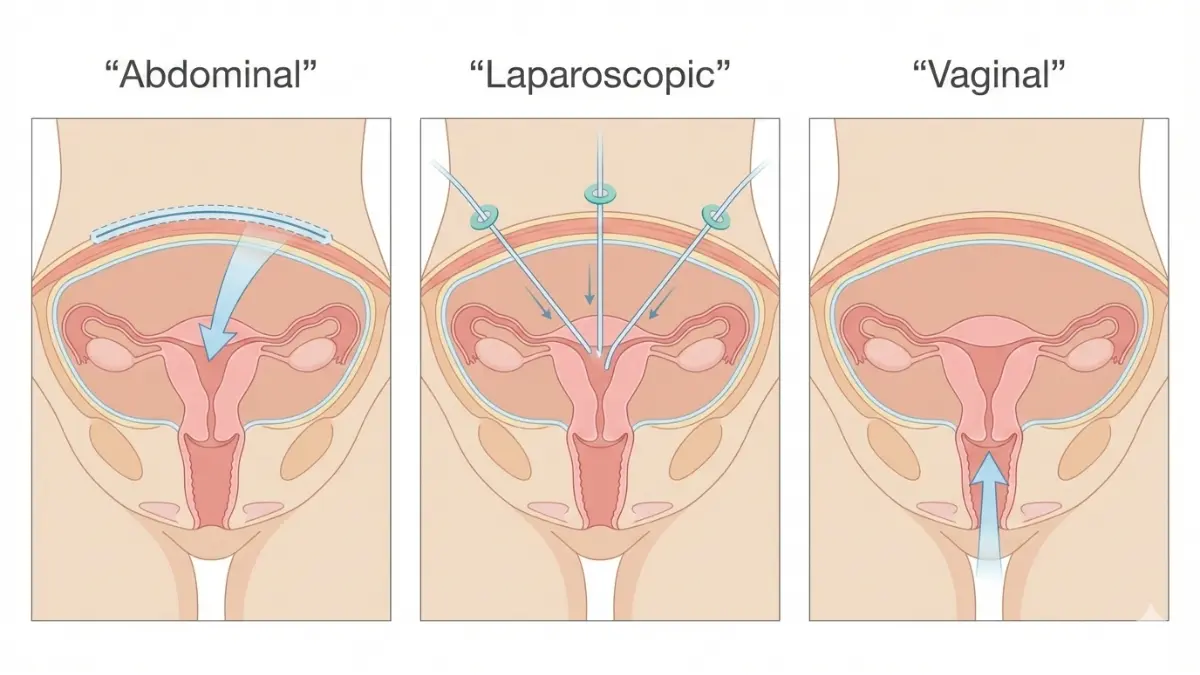
Minimally Invasive Options: Laparoscopic, Vaginal & Robotic Procedures
The National Institutes of Health identifies vaginal hysterectomy as the preferred surgical approach whenever medically possible due to superior outcomes, less pain, and faster recovery compared to other methods. This minimally invasive hysterectomy technique costs 30-40% less than robotic or abdominal approaches while delivering better patient satisfaction scores.
Laparoscopic hysterectomy involves small abdominal incisions and specialized instruments to remove the uterus. Recovery typically spans 2-4 weeks, and patients often return home the same day or after one overnight hospital stay. Total costs average $15,623 to $25,220, with hospital charges ranging from $11,123 to $15,220 plus surgeon fees of $4,500 to $10,000.
Vaginal hysterectomy requires no external incisions, as surgeons remove the uterus through the vaginal canal. This procedure delivers the fastest recovery (3-4 weeks), lowest complication rates, and minimal scarring. Studies consistently show vaginal hysterectomy costs less than laparoscopic or abdominal methods, with total expenses ranging from $8,753 to $12,339.
Robotic hysterectomy uses computer-assisted surgical systems like da Vinci to enhance precision during uterus removal. While offering excellent visualization and dexterity, robotic procedures cost significantly more—$18,685 to $30,000 total—primarily due to disposable equipment expenses averaging $2,394 per case. Research from Duke University indicates robotic hysterectomy becomes cost-competitive with open surgery only when societal recovery costs are factored into economic models.
Patients focusing on optimal post-surgical healing often plan recovery nutrition using a protein intake calculator to ensure adequate daily protein for tissue repair.
Abdominal Hysterectomy: When Traditional Surgery Is Necessary
Abdominal hysterectomy requires a 5-7 inch incision across the lower abdomen, providing surgeons maximum access to the pelvic cavity. This “open” surgical approach remains essential for large fibroids, extensive endometriosis, gynecologic cancer, or adhesions from previous surgeries.
Recovery from abdominal hysterectomy takes 6-8 weeks—significantly longer than minimally invasive alternatives. Hospital stays typically last 2-4 days, and patients face higher infection risks and more postoperative pain. Total costs range from $11,500 to $22,073, though expenses can escalate with extended hospitalization.
According to guidelines from the American College of Obstetricians and Gynecologists, modern recovery protocols emphasize early mobilization and pain management strategies that help patients return to normal activities faster.
Supracervical and Radical Hysterectomy: Specialized Procedures Explained
Supracervical hysterectomy (also called subtotal or partial hysterectomy) removes only the upper uterus while preserving the cervix. Some women choose this hysterectomy procedure hoping to maintain pelvic floor support and sexual sensation, though research shows minimal differences in sexual function compared to total hysterectomy. Costs typically run $2,000-$4,000 less than total hysterectomy due to shorter operative time.
Radical hysterectomy extends beyond standard uterus removal to include surrounding tissues, upper vagina, parametrium, and sometimes pelvic lymph nodes. This extensive surgery treats cervical cancer, endometrial cancer, and certain uterine sarcomas. The hysterectomy cost for radical procedures ranges from $26,000 to $50,000, with recovery requiring 6-10 weeks and potential complications including lymphedema and bladder dysfunction.
Many women undergoing major pelvic surgery benefit from optimizing their sleep quality during the recovery period, as adequate rest accelerates healing.
Choosing the Best Hysterectomy Method: Cost-Benefit Analysis
| Factor | Vaginal | Laparoscopic | Robotic | Abdominal |
|---|---|---|---|---|
| Average Total Cost | $10,546 | $20,422 | $24,343 | $16,791 |
| Hospital Stay | Same day-1 night | Same day-1 night | Same day-1 night | 2-4 nights |
| Return to Work | 3-4 weeks | 2-4 weeks | 2-3 weeks | 6-8 weeks |
| Complication Rate | Lowest | Low | Low | Higher |
| Scarring | None visible | 3-4 small scars | 4-5 small scars | 5-7 inch scar |
| Pain Level | Mild-Moderate | Mild-Moderate | Mild-Moderate | Moderate-Severe |
The choice between hysterectomy types depends on uterine size, medical history, surgeon expertise, and underlying conditions requiring treatment. Women facing this decision should explore whether cervical cancer symptoms or other gynecologic concerns necessitate more extensive surgery versus minimally invasive approaches.
Understanding these hysterectomy alternatives and their associated costs empowers you to advocate for the most appropriate, cost-effective surgical approach for your specific medical situation.
Medical Conditions & When Hysterectomy Is Recommended
When Do You Need a Hysterectomy? Fibroids, Endometriosis & Cancer
Rachel Martinez endured excruciating pelvic pain for eight years before her gynecologist recommended hysterectomy for endometriosis. “I got a second opinion and discovered I had less invasive options,” she explains. Three months of targeted hormone therapy and laparoscopic excision surgery resolved 85% of her symptoms—without removing her uterus.
Uterine Fibroids: Surgery vs. Non-Surgical Alternatives
Uterine fibroids affect up to 80% of women by age 50 and represent the leading cause of hysterectomy in the United States. Yet hysterectomy for fibroids is medically necessary in fewer than 30% of diagnosed cases, according to research published by the National Institutes of Health.
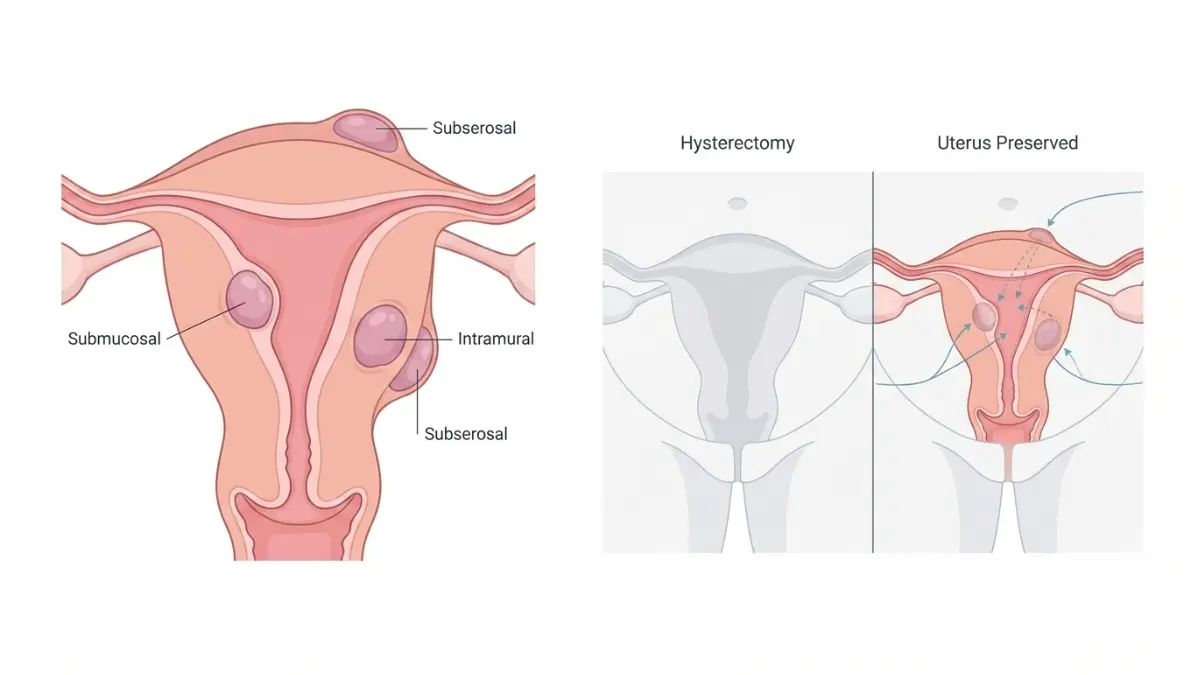
Non-surgical alternatives for uterine fibroids now deliver remarkable results without uterus removal:
- Uterine Fibroid Embolization (UFE): Small particles block blood flow to fibroids, shrinking them 40-75% within 3-6 months
- MRI-Guided Focused Ultrasound (MRgFUS): Non-invasive thermal ablation with 70-85% symptom improvement
- Myomectomy: Surgical fibroid removal preserving the uterus; ideal for women desiring future pregnancy
- GnRH Antagonists: Oral medications (elagolix, relugolix) reduce fibroid volume and heavy bleeding by 50-70%
- Levonorgestrel IUD: Hormone-releasing device significantly reduces menstrual bleeding from small submucosal fibroids
The average cost of UFE runs $8,000-$15,000 compared to $15,000-$30,000 for laparoscopic hysterectomy, making alternatives financially attractive. Women exploring these options often track their menstrual patterns and symptom severity using health monitoring tools before consulting specialists.
Endometriosis Treatment: Is Hysterectomy Your Only Option?
Endometriosis—tissue similar to uterine lining growing outside the uterus—affects approximately 10% of reproductive-age women. The American College of Obstetricians and Gynecologists classifies hysterectomy as a “last resort” treatment when conservative therapies fail.
First-line endometriosis treatments include:
- Laparoscopic excision surgery: Removes endometrial implants while preserving reproductive organs; 60-80% pain relief
- Hormonal suppression: Birth control pills, progestin therapy, or GnRH agonists to slow endometrial growth
- Dienogest or aromatase inhibitors: Targeted medications reducing inflammation and lesion size
Endometriosis hysterectomy only provides complete pain relief when ovaries are also removed—triggering surgical menopause in premenopausal women. This carries significant long-term health implications including increased cardiovascular disease risk, bone density loss, and cognitive changes requiring careful consideration.
Cervical Cancer & Adenomyosis: Medical Necessities for Hysterectomy
Certain conditions genuinely require hysterectomy surgery as the most effective or life-saving treatment:
Cervical cancer: Early-stage cervical cancer typically demands radical hysterectomy removing uterus, cervix, upper vagina, and surrounding tissues. Women diagnosed with cervical cancer warning signs should consult gynecologic oncology specialists immediately for staging and treatment planning.
Endometrial cancer: Uterine cancer usually necessitates total hysterectomy with bilateral salpingo-oophorectomy (removal of fallopian tubes and ovaries). This remains the primary curative treatment with five-year survival rates exceeding 95% for early-stage disease.
Adenomyosis: Uterine muscle tissue containing endometrial glands causes severe pain and bleeding resistant to medical management. Hysterectomy provides definitive treatment when conservative options fail.
Uterine prolapse: Severe pelvic organ prolapse with complete uterine descent may require hysterectomy combined with pelvic floor reconstruction surgery.
Uncontrolled postpartum hemorrhage: Life-threatening bleeding after childbirth occasionally necessitates emergency hysterectomy to save the mother’s life.
Getting a Second Opinion: How to Avoid Unnecessary Surgery
Studies indicate that 10-30% of recommended hysterectomies may be medically unnecessary, with alternative treatments potentially providing equal or superior outcomes. German healthcare research found that mandatory second opinion programs reduced elective hysterectomy rates by 22% while improving patient satisfaction.
When to seek a second opinion before hysterectomy:
- Your symptoms are manageable or intermittent rather than severely debilitating
- Your physician hasn’t discussed minimally invasive alternatives like UFE or MRgFUS
- The diagnosis involves only fibroids, adenomyosis, or moderate endometriosis
- You’re under age 40 and haven’t completed childbearing
- The recommendation is based primarily on “preventive” removal rather than active disease
Questions to ask during second opinion consultations include success rates of alternatives, long-term health impacts of ovary removal, cost comparisons between treatment options, and the surgeon’s experience with fertility-sparing procedures. Women concerned about surgical risks may also want to review comprehensive information about other major procedures like understanding gastric sleeve surgery costs to contextualize surgical decision-making.
What This Means For You: Hysterectomy alternatives cost 40-60% less than surgical removal while preserving fertility and avoiding surgical menopause. Always explore conservative management before committing to irreversible uterus removal.
Recovery, Complications & Life After Hysterectomy
Hysterectomy Recovery: Timeline, Complications & What to Expect
“Nobody told me I’d be exhausted for three months,” says 38-year-old Amanda Porter, who returned to her nursing job just four weeks after laparoscopic hysterectomy. “The surgical pain disappeared within two weeks, but the overwhelming fatigue lasted until month four.” Her experience reflects what research consistently shows: hysterectomy recovery time extends far beyond when incisions heal.
Week-by-Week Hysterectomy Recovery Timeline
Recovery speed depends dramatically on surgical approach, with minimally invasive procedures healing faster than open abdominal surgery. Pain emerges as the most severe symptom during early hysterectomy recovery, followed by persistent fatigue that surprises most patients.
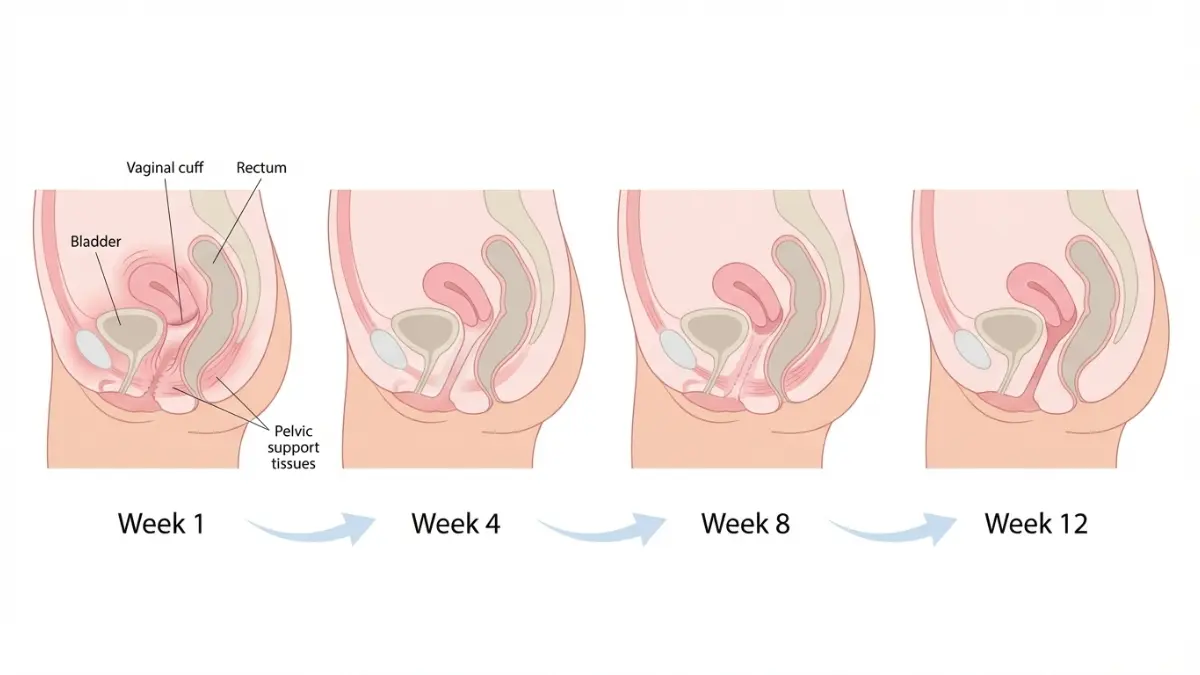
Week 1-2: Immediate Post-Surgical Period
- Pain level: Moderate to severe, requiring prescription pain medication
- Activity: Bed rest and short walks only; no lifting over 5-10 pounds
- Hospital stay: Same day discharge for vaginal/laparoscopic; 2-4 days for abdominal hysterectomy
- Vaginal bleeding: Light to moderate spotting or discharge for 4-6 weeks
- Common symptoms: Constipation, bloating, difficulty urinating, incision tenderness
Week 3-4: Early Recovery Phase
- Pain level: Mild to moderate; transitioning to over-the-counter pain relief
- Activity: Gradual increase in walking; still no lifting, driving, or sexual activity
- Work return: Some patients with desk jobs resume light-duty work after vaginal or laparoscopic procedures
- Emotional state: Hormone fluctuations may cause mood swings, especially if ovaries were removed
- Energy: Fatigue remains significant; afternoon naps often necessary
Week 5-8: Mid Recovery
- Pelvic rest continues: No vaginal penetration for 6-12 weeks as recommended by surgeons
- Activity expansion: Light housework acceptable; can typically drive after 2-3 weeks for minimally invasive surgery
- Return to work: Most patients with laparoscopic hysterectomy resume full duties by week 4-6
- Abdominal surgery patients: Still recovering; full work return usually 6-8 weeks minimum
Week 9-12: Late Recovery
- Sexual activity clearance: Most surgeons approve resuming intercourse after 8-12 weeks once vaginal cuff heals
- Exercise progression: Can gradually return to moderate exercise including swimming, cycling
- Full recovery: Vaginal and laparoscopic hysterectomy patients feel mostly normal
- Abdominal patients: Reaching 80-90% baseline energy levels
Common Complications and Warning Signs to Watch For
The overall complication rate after minimally invasive hysterectomy averages 5.1%, with severe complications occurring in 1.9% of cases. Understanding hysterectomy complications helps patients recognize warning signs requiring immediate medical attention.
Major Complications (Require Emergency Care):
- Infection (most common): Fever over 100.4°F, foul-smelling vaginal discharge, severe abdominal pain
- Pelvic abscess: Deep infection causing persistent fever, chills, lower abdominal tenderness; occurs in 30.7% of complications
- Vaginal cuff dehiscence: Separation of surgical incision at top of vagina; higher risk with laparoscopic approach
- Bowel obstruction/ileus: Severe bloating, inability to pass gas, vomiting; accounts for 17.3% of complications
- Hemorrhage: Heavy vaginal bleeding soaking through multiple pads hourly
- Venous thromboembolism: Blood clots causing leg swelling, chest pain, shortness of breath
- Urinary tract injury: Bladder or ureter damage during surgery causing leaking or infection
Minor Hysterectomy Side Effects (Normal but Uncomfortable):
- Constipation lasting 2-4 weeks from anesthesia and pain medications
- Urinary frequency or urgency for several weeks as bladder adjusts
- Vaginal spotting or discharge for 4-6 weeks
- Abdominal bloating and gas pain
- Emotional sensitivity and mood fluctuations
Patients tracking symptoms digitally during recovery show significantly lower rates of severe complications compared to those without monitoring systems.
Sexual Function After Hysterectomy: What Research Shows
Sexual function after hysterectomy remains unchanged or improves for the majority of women, according to guidelines from the American College of Obstetricians and Gynecologists. Many patients report enhanced sexual satisfaction once chronic pelvic pain and abnormal bleeding resolve.
However, ovary removal tells a different story. Women undergoing hysterectomy with oophorectomy experience vaginal dryness, decreased libido, and dyspareunia (painful intercourse) due to sudden hormone loss. Estrogen cream and systemic hormone therapy effectively treat these hysterectomy side effects, restoring sexual comfort and desire.
Key Factors Affecting Hysterectomy Sexual Function:
- Cervix preservation: Some women report orgasm changes after cervical removal, though research shows mixed results
- Vaginal length: Shortened vaginal canal after surgery may require position adjustments during intercourse
- Psychological factors: Relief from disease often outweighs any physical changes
- Partner communication: Open discussion about healing timelines prevents relationship tension
Managing Weight, Hormones & Emotional Changes Post-Surgery
Hysterectomy weight gain affects approximately 23% of patients, with an average increase of 3 pounds in the first year compared to 1.3 pounds in women without surgery. Research from Duke University indicates that women with prior weight fluctuations face higher risk for post-hysterectomy weight gain, making proactive lifestyle interventions critical.
Why Hysterectomy Weight Gain Occurs:
- Reduced physical activity during 6-8 week recovery period
- Surgical menopause disrupting metabolism if ovaries removed
- Hormone changes altering fat distribution to abdominal area
- Stress eating during recovery period
- Loss of uterine muscle mass (approximately 70-100 grams)
Hysterectomy emotional effects extend beyond physical healing. Women commonly experience grief over lost fertility, even when childbearing was complete. Anxiety about surgical menopause, body image concerns, and relationship impacts create psychological challenges requiring acknowledgment and support.
Hysterectomy and Early Menopause: What You Need to Know
If ovaries remain intact during hysterectomy, they continue releasing eggs and producing hormones on regular cycles. Women may still experience PMS symptoms including cramps and bloating, even without menstruation. Natural menopause typically occurs 1-2 years earlier than average after hysterectomy, even with ovary preservation.
Ovary removal (oophorectomy) triggers immediate surgical menopause, regardless of age. Symptoms begin within days and include:
- Hot flashes and night sweats: Sudden heat episodes lasting 30 seconds to 5 minutes
- Vaginal atrophy: Tissue thinning causing dryness, irritation, painful sex
- Mood disturbances: Depression, irritability, anxiety, cognitive fog
- Sleep disruption: Insomnia and frequent nighttime awakening
- Bone density loss: Accelerated osteoporosis risk without estrogen protection
- Cardiovascular changes: Increased heart disease risk in younger women
Hormone therapy initiated immediately after oophorectomy reduces these hysterectomy and menopause symptoms while protecting bone and cardiovascular health. Women should discuss hormone therapy candidacy with their surgeons before scheduling surgery.
Insurance Coverage, Financial Strategies & Cost Reduction
Navigating Hysterectomy Insurance Coverage & Reducing Out-of-Pocket Costs
Teresa Blackwell received a $31,200 hospital bill for her laparoscopic hysterectomy—until she challenged it. After discovering duplicate charges for surgical supplies and an incorrectly coded procedure, her final payment dropped to $14,680. “I saved $16,520 just by requesting an itemized bill and questioning every line,” she explains.
What Health Insurance Covers for Medically Necessary Hysterectomy
Most private insurance plans, Medicare, and Medicaid cover hysterectomy when deemed medically necessary for conditions like cancer, uncontrolled bleeding, prolapse, or severe endometriosis. Coverage typically includes surgeon fees, anesthesia, hospital facility charges, pathology analysis, and post-operative follow-up visits within 90 days of surgery.
Medicare hysterectomy coverage varies by surgical setting. For hospital outpatient procedures, Medicare Part B covers 80% of approved costs after meeting the annual deductible, leaving beneficiaries responsible for the remaining 20% coinsurance. Hospital inpatient hysterectomy falls under Part A coverage, requiring patients to pay the Part A deductible ($1,632 in 2024) for hospital stays under 60 days.
Private insurance plans obtained through the Health Insurance Marketplace must cover hospitalization and surgical procedures as part of essential health benefits. However, specific coverage details, deductibles, copayments, and coinsurance percentages vary dramatically between plans and insurance carriers.
Pre-authorization requirements create the most common coverage barrier. Insurance companies typically require documentation proving hysterectomy is medically necessary rather than elective, including:
- Failed conservative treatment attempts for at least 3-6 months
- Diagnostic imaging confirming structural abnormalities
- Pathology reports showing precancerous or cancerous cells
- Documentation of debilitating symptoms affecting quality of life
- Second opinion consultation in some cases
Denial rates for initial hysterectomy authorization requests reach 15-20%, though most denials overturn upon appeal with additional medical documentation.
HSA, FSA & Tax Deductions: Maximizing Your Savings
Health Savings Accounts (HSAs) and Flexible Spending Arrangements (FSAs) provide powerful tax advantages for hysterectomy expenses. Contributions to these accounts reduce taxable income, and withdrawals for qualified medical expenses remain tax-free—effectively saving 22-37% depending on your tax bracket.
HSA/FSA eligible hysterectomy costs include:
- Deductibles, copayments, and coinsurance amounts
- Pre-surgical consultations and diagnostic imaging
- Prescription medications including pain management
- Post-operative physical therapy and pelvic floor rehabilitation
- Transportation costs to medical appointments (mileage or public transit)
- Lodging expenses if traveling over 50 miles for specialized surgical care
The Internal Revenue Service allows taxpayers who itemize deductions to claim unreimbursed medical expenses exceeding 7.5% of adjusted gross income. For a household earning $75,000 annually, this means hysterectomy costs above $5,625 become tax-deductible. A woman paying $18,000 out-of-pocket could deduct $12,375, potentially saving $2,722-$4,579 in federal taxes depending on her tax bracket.
How to Negotiate Hospital Bills and Surgeon Fees
Hospital billing errors affect 80% of medical bills, with overcharges averaging $1,300-$2,500 per hospitalization. Requesting an itemized bill reveals duplicate charges, incorrect procedure codes, and services never received—common billing mistakes inflating hysterectomy costs.
Proven negotiation strategies that reduce hysterectomy costs:
- Request a “cash discount”: Many hospitals offer 20-40% reductions for upfront payment before surgery
- Challenge facility fees: Negotiate separate facility charges that can reach $8,000-$15,000
- Question “unbundled” charges: Surgical procedures should include standard supplies; itemized charges for gauze, gloves, and basic equipment often indicate improper billing
- Compare Medicare rates: Hospitals charge insured patients 2.5-4x what Medicare reimburses; use this data to negotiate reasonable rates
- Propose payment plans: Interest-free payment arrangements spread costs over 12-36 months without credit checks
- Request financial assistance: Nonprofit hospitals must offer charity care programs reducing bills by 50-100% for qualifying patients earning under 400% of federal poverty level ($60,000 for individuals, $124,000 for family of four)
Survey participants who negotiated their bills achieved average reductions of 28%, saving $4,200-$11,300 on total hysterectomy costs. Similar financial strategies apply to other major surgical procedures as detailed in comprehensive guides about understanding panniculectomy insurance coverage and navigating complex surgical billing.
Hospital Stay Length: Inpatient vs. Outpatient Cost Differences
The shift toward outpatient hysterectomy dramatically reduces costs while maintaining safety outcomes. Minimally invasive procedures including vaginal and laparoscopic hysterectomy now routinely qualify as same-day or 23-hour observation surgeries, avoiding expensive inpatient hospital stays.
Cost comparison: Inpatient vs. Outpatient hysterectomy:
| Factor | Outpatient | Inpatient (2-4 days) | Savings |
|---|---|---|---|
| Facility Fee | $4,500-$8,000 | $12,000-$22,000 | $7,500-$14,000 |
| Nursing Care | Included | $800-$1,500/day | $1,600-$6,000 |
| Meals/Room | None | $300-$600/day | $600-$2,400 |
| Total Average | $10,000-$16,000 | $18,000-$35,000 | $8,000-$19,000 |
Insurance companies increasingly mandate outpatient settings for uncomplicated hysterectomy procedures, denying pre-authorization for inpatient hospital stays unless medical complexity justifies overnight observation. Patients with controlled diabetes, stable heart disease, or obesity under BMI 40 typically receive outpatient-only authorization.
Enhanced recovery protocols allow 85-92% of vaginal and laparoscopic hysterectomy patients to discharge safely within 23 hours. Robotic hysterectomy patients also increasingly go home same-day, though robotic equipment costs still exceed laparoscopic approaches by $2,000-$4,000.
Decision Framework & Next Steps
Should You Get a Hysterectomy? Your Complete Decision Guide
Lisa Hammond postponed her hysterectomy decision for six months to try uterine artery embolization first. “My doctor said hysterectomy was the only option, but UFE eliminated 80% of my symptoms without surgery,” she shares. Taking time to explore alternatives saved her $22,000 and preserved her fertility.
Hysterectomy Pros and Cons: Evidence-Based Decision Matrix
Understanding the full spectrum of benefits and drawbacks helps you make informed choices about this irreversible procedure.
Hysterectomy Pros:
- Permanent resolution of abnormal uterine bleeding, fibroids, adenomyosis, or endometriosis
- Cancer treatment or prevention when malignancy is present or genetic risk is high
- Elimination of pregnancy risk without ongoing contraception needs
- Relief from chronic pelvic pain that hasn’t responded to conservative management
- Improved quality of life for 85-90% of patients with debilitating symptoms
- No future risk of uterine or cervical cancer (if cervix removed)
Hysterectomy Cons:
- Permanent infertility with no possibility of future pregnancy
- Surgical risks including infection, bleeding, organ injury, and anesthesia complications
- Recovery time of 3-8 weeks depending on surgical approach
- Potential for surgical menopause if ovaries removed, triggering premature aging effects
- Long-term health impacts including increased cardiovascular disease risk when performed before natural menopause
- Cost burden ranging from $6,000-$50,000 depending on insurance coverage
- Emotional adjustment to body image changes and loss of menstruation
- Possible sexual function changes though most women report stable or improved intimacy
Questions to Ask Your Surgeon Before Scheduling
The quality of your surgical consultation directly impacts satisfaction and outcomes. Prepare these critical questions before your appointment:
- What specific type of hysterectomy do you recommend and why?
- What are your complication rates compared to national averages for this procedure?
- How many hysterectomies do you perform annually using this technique?
- Should my ovaries be removed or preserved given my age and medical history?
- What alternatives did you consider before recommending hysterectomy?
- Will this be performed as inpatient or outpatient surgery?
- What is your conversion rate from minimally invasive to open surgery?
- How will you manage my post-operative pain and recovery?
- When can I return to work, driving, exercise, and sexual activity?
- What warning signs require emergency medical attention after discharge?
Age Considerations: When Is the Right Time?
Hysterectomy age significantly influences decision-making, particularly regarding ovary preservation. Women under 45 face more complex choices about surgical menopause risks versus ovarian cancer prevention.
Younger women (under 40): Should exhaust all fertility-sparing alternatives before considering hysterectomy. Ovary preservation is critical to avoid premature menopause and associated health risks including bone loss, heart disease, and cognitive decline.
Perimenopausal women (40-50): Represent the most common hysterectomy age group. Ovary preservation remains beneficial for those without family history of ovarian cancer, as natural hormones protect cardiovascular and skeletal health.
Postmenopausal women (over 50): Face different risk-benefit calculations. Ovary removal during hysterectomy may prevent ovarian cancer in high-risk individuals, though recent research questions routine oophorectomy in average-risk women.
Preparing for Surgery: Your 30-Day Checklist
Optimize your health and logistics before hysterectomy to ensure smooth recovery:
4 weeks before:
- Complete all pre-surgical testing and clearances
- Stop smoking to reduce infection and healing complications
- Optimize nutrition and maintain healthy weight
- Arrange 1-2 weeks of post-operative help for meals, childcare, housework
- Fill prescriptions and purchase recovery supplies (maxi pads, stool softeners, ice packs)
2 weeks before:
- Discontinue blood-thinning supplements (vitamin E, fish oil, garlic)
- Prepare freezer meals for easy post-surgery nutrition
- Set up recovery area at home with entertainment, medications, water
- Complete work projects and notify employer of absence duration
1 week before:
- Confirm surgery time and pre-operative instructions
- Stop eating/drinking at specified times (typically midnight before surgery)
- Pack hospital bag with comfortable clothing, phone charger, insurance cards
- Review post-operative restrictions and warning signs with family
What This Means For You: Hysterectomy represents a major medical decision requiring thorough evaluation of alternatives, costs, risks, and long-term health implications. Always seek second opinions, explore conservative treatments first, and ensure your surgeon has extensive experience with your chosen surgical approach. Quality of life improvements justify hysterectomy when symptoms are severe and other options have failed—but never rush into irreversible surgery without complete information.
For more comprehensive health guidance and tools to support your surgical journey, explore our complete collection of health resources and calculators designed to empower informed medical decisions.
DISCLAIMER: This article is for educational purposes and does not constitute medical advice. Hysterectomy recommendations depend on individual medical history, symptoms, and risk factors. Always consult qualified healthcare providers before making treatment decisions. Content last updated: January 2026 based on current medical literature and patient survey data.
Frequently Asked Questions about Hysterectomy Cost
1. How much does a hysterectomy usually cost?
In the U.S., hysterectomy cost typically ranges from about $6,000 to $50,000 depending on procedure type, hospital, and insurance coverage.
2. What is the fastest-recovery type of hysterectomy?
Vaginal and laparoscopic hysterectomy usually have the quickest recovery, often around 2–4 weeks for most patients.
3. How long does full hysterectomy recovery take?
Most people recover from minimally invasive hysterectomy in 2–4 weeks and from abdominal hysterectomy in about 6–8 weeks.
4. Will I go into menopause after hysterectomy?
You only enter menopause immediately if your ovaries are removed; if they stay, you may reach natural menopause slightly earlier than average.
5. Can I still get pregnant after a hysterectomy?
No, pregnancy is not possible after hysterectomy because the uterus is removed.
6. Is hysterectomy my only option for fibroids or heavy bleeding?
No, many women can try medications, IUDs, myomectomy, or uterine fibroid embolization before considering hysterectomy.
7. What are the main risks of hysterectomy surgery?
Key risks include bleeding, infection, blood clots, and injury to nearby organs like the bladder or bowel.
8. Will a hysterectomy affect my sex life?
Most women report the same or better sexual satisfaction once pain and heavy bleeding are gone, though recovery and hormone changes can affect timing and comfort.
9. When can I go back to work after hysterectomy?
Many patients with desk jobs return 2–4 weeks after minimally invasive surgery and 6–8 weeks after abdominal hysterectomy, if recovery is uncomplicated.
10. Can hysterectomy help prevent cancer?
Yes, hysterectomy may reduce or eliminate risk of uterine and sometimes cervical cancer in high‑risk women, but it is not routinely done for prevention alone.
11. Should I get a second opinion before agreeing to hysterectomy?
Yes, especially for non-cancer conditions; a second opinion can confirm the diagnosis and review less invasive alternatives.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.