On This Page – Quick Medical Summary
If you or someone you love has a Whipple procedure scheduled, the hardest part right now is often the unknown — what the days and weeks after surgery will actually feel like. This guide walks through recovery honestly: the hospital stay, the timeline at home, the digestive changes, and the warning signs that matter.
How you use it depends on where you are:
- Facing a scheduled surgery? Start with why recovery takes time and the step-by-step timeline, then read why the hospital you choose changes your odds.
- Recovering at home now? Skip ahead to complications, eating and digestion, and warning signs.
- Caring for someone? The timeline, complications, and red-flag sections give you the practical map.
Recovery from a Whipple is demanding but well-charted. Knowing the phases ahead — and what is normal versus what needs a call — makes the road easier to walk. For the larger picture of diagnosis and treatment, see our complete guide to pancreatic cancer.
ℹ️ Medical Disclaimer: This article is general education, not medical advice. It does not diagnose any condition or recommend any treatment, medication, or procedure, and it does not replace guidance about your care or insurance. Whipple recovery varies by individual, surgery type, and overall health. Always follow the specific instructions of your own surgical team, consult a board-certified surgical oncologist or hepatobiliary surgeon before making decisions, and seek emergency care for any severe or sudden symptom.
Why Whipple recovery takes the time it does
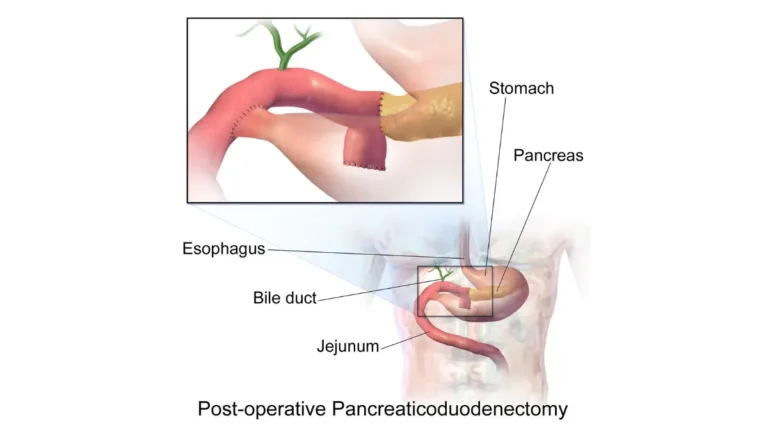
A pancreaticoduodenectomy — the formal name for the Whipple — is one of the most involved operations in abdominal surgery, which is why healing is measured in weeks and months rather than days. Understanding what the surgeon does makes the recovery timeline make sense.
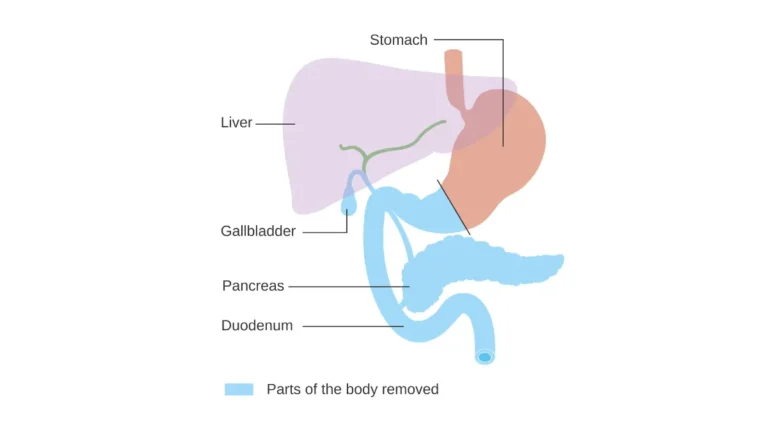
What the surgeon removes and reconnects
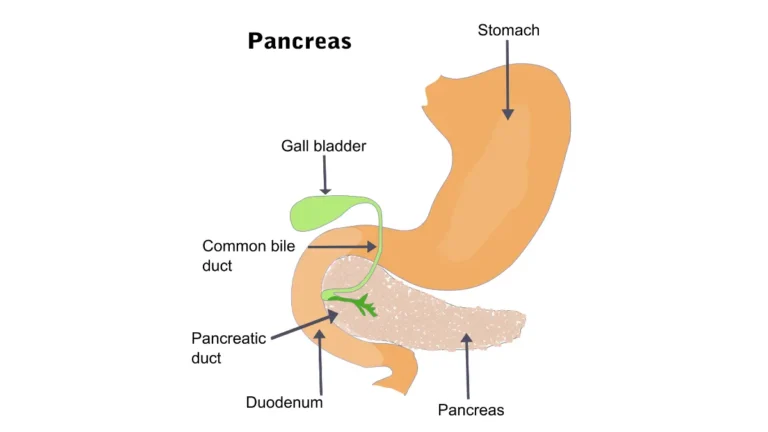
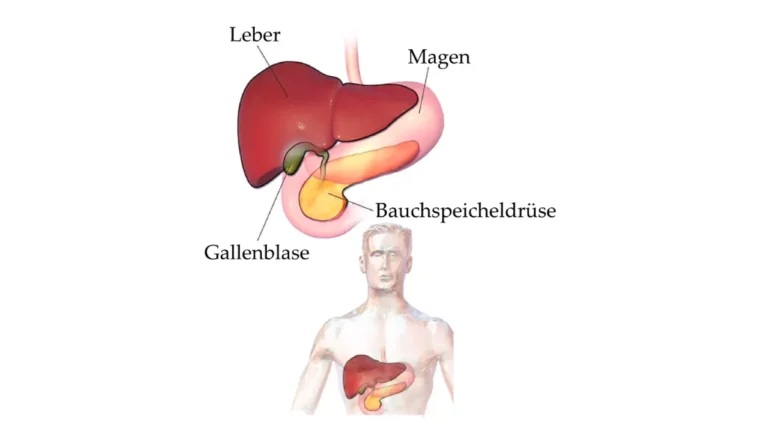
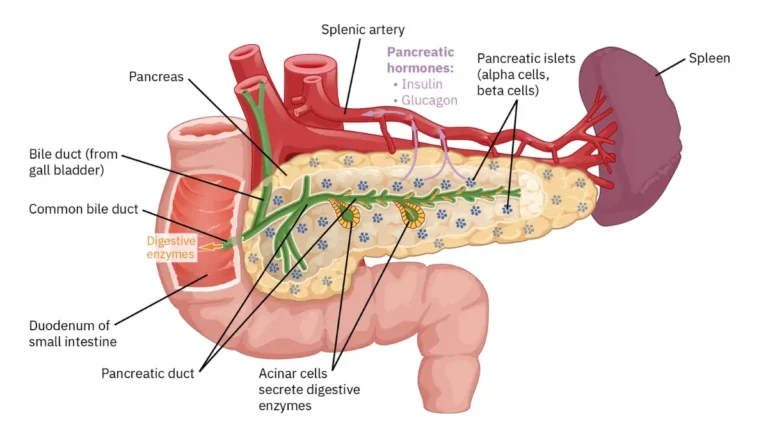
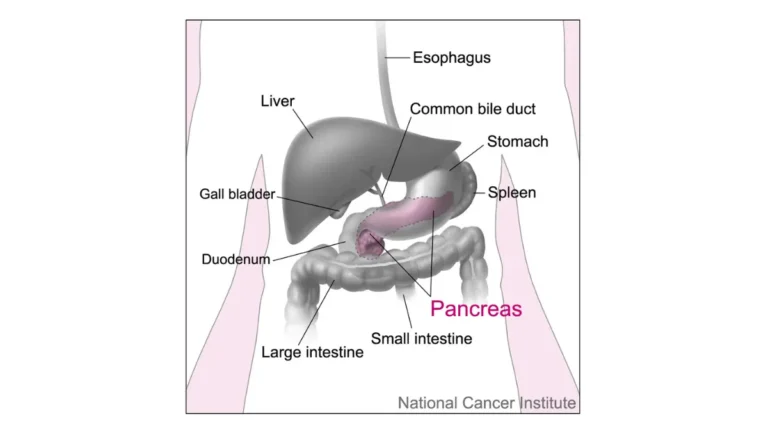
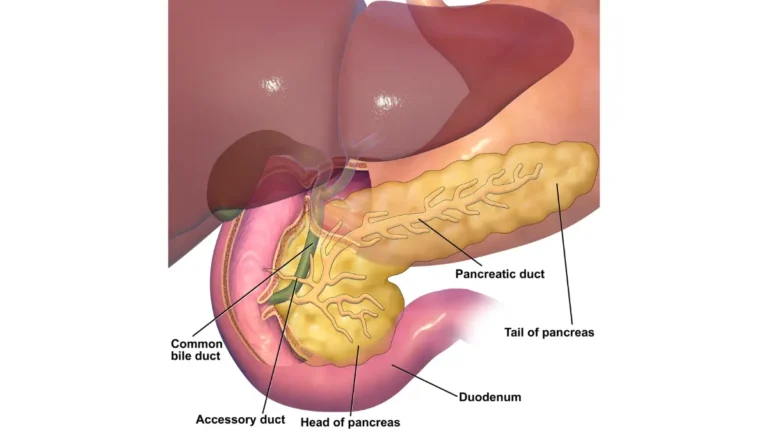
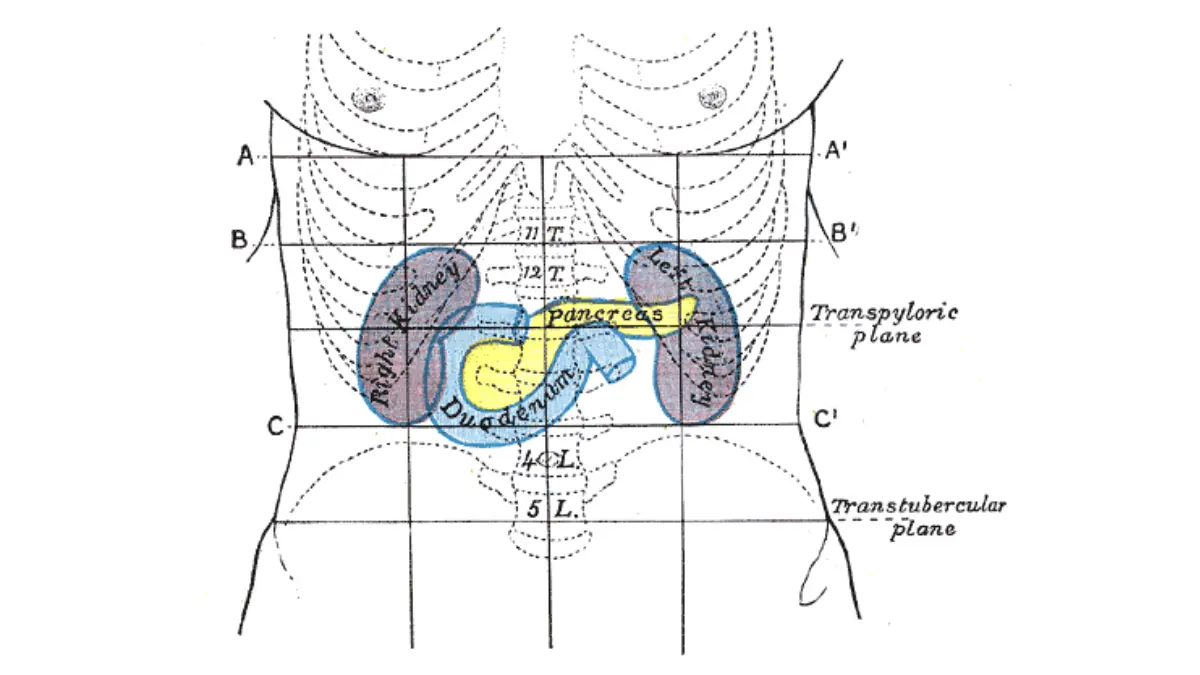
During the operation, the surgeon removes the head of the pancreas, the gallbladder, the duodenum (the first part of the small intestine), part of the bile duct, and sometimes a portion of the stomach. The remaining pancreas, bile duct, and stomach are then reconnected to the small intestine. This is why a Whipple is often described as both removing and rebuilding part of the digestive tract.
You can read more about how surgery fits into the larger pancreatic cancer treatment plan and about whether a tumor can be surgically removed in our related guides.
🔬 How It Works: Each reconnection between two organs is called an anastomosis. These new surgical joins need weeks to heal, and because a Whipple creates several of them, the body needs a long, gradual recovery before digestion works smoothly again.
How long the operation itself takes
The surgery typically takes about 5 to 7 hours. That length, combined with the multiple reconnections, is why early recovery is slow and why fatigue can linger. For the authoritative clinical overview, see the National Cancer Institute’s summary of pancreatic cancer surgery.
The Whipple recovery timeline, step by step
Whipple procedure recovery happens in three phases: a hospital stay of about 7 to 14 days, several weeks of limited activity at home, and full recovery in roughly 2 months — sometimes up to 6 months or longer. Knowing each phase helps you plan support and pace yourself.
In the hospital: the first 7 to 14 days
Most people stay in the hospital about 8 to 10 days after open surgery, though stays of 7 to 14 days are common. Minimally invasive (robotic or laparoscopic) surgery can mean a shorter stay of roughly 4 to 6 days.
You will likely be encouraged to sit up and take short walks the day after surgery, which helps prevent blood clots and pneumonia. Tubes and drains placed during surgery are removed as you heal, and eating restarts gradually — from liquids to soft foods.
The first weeks at home
Fatigue, a reduced appetite, and a tender incision are expected in the early weeks. Most people slowly increase walking and light activity while resting often.
Getting back to normal: 2 to 6 months
Many people return to light normal activities around a month after surgery and recover more fully by about 2 months — though it can take up to 6 months, and some say it takes the better part of a year to feel like themselves again. Complications can extend this timeline.
📊 Clinical Data Point: After a Whipple, the hospital stay is typically 8–10 days, and most people recover completely within about 2 months (occasionally up to 6 months). — Sources: Pancreatic Cancer Action Network; Aurora Health Care.
Common complications and what’s normal afterward
Most complications after a Whipple are anticipated by the surgical team and managed during the hospital stay — but knowing the common ones helps you tell ordinary recovery from a problem that needs attention. Postoperative complications occur in roughly 30% to 60% of patients overall. The two most common are:
- Delayed gastric emptying — the stomach empties more slowly than usual, causing nausea or fullness; it affects roughly 1 in 6 people (about 17%).
- Pancreatic fistula — leakage from the new pancreatic connection; reported in around 9% of patients in some series, and higher in others.
Other risks include bile leak (around 4%), bleeding (around 2%), and surgical site infection. Most are handled in the hospital, though a few extend recovery considerably.
🔬 How It Works: A pancreatic fistula happens when pancreatic fluid leaks from a surgical join before it fully heals. The surgical team watches the drains placed during surgery to catch this early — one reason drains stay in for a while.
✅ Patient Action: Before surgery, ask your surgeon: “What is this center’s pancreatic fistula and overall complication rate, and how are leaks managed if one happens?”
Eating and digestion after a Whipple
Eating changes after a Whipple, often for the long term, because the surgery alters how the body digests food. Most people do best with small, frequent, protein-focused meals, and many need enzyme support to digest fat properly.
Why digestion changes
With part of the pancreas removed, the gland may not make enough digestive enzymes, leading to fat malabsorption and steatorrhea (loose, oily, foul-smelling stools). Whipple patients are more likely than people who have other pancreatic surgeries to have insufficient enzyme production. You can read more about managing weight loss with pancreatic cancer in our related guide.
How to eat in early recovery
Eating small amounts every few hours, focusing on protein, drinking fluids between rather than with meals, and chewing well all help. Feeling full quickly — early satiety — is very common and tends to ease with time. It can help to estimate your daily protein needs and to gauge your daily fluid needs as you rebuild your appetite.
Pancreatic enzymes (PERT)
If the remaining pancreas can’t keep up, your team may prescribe pancreatic enzyme replacement therapy (PERT), taken with meals and snacks. The American Cancer Society’s explanation of pancreatic surgery and its effects covers these digestive changes in more detail.
🔬 How It Works: PERT capsules contain the digestive enzymes your pancreas would normally release, helping your body break down fat and absorb nutrients. The right dose varies, which is why it is set and adjusted by your care team.
✅ Patient Action: Ask for a referral to a registered dietitian, and ask your team whether you need pancreatic enzymes and exactly how and when to take them.
Why the hospital you choose changes your odds
One of the most important decisions a patient can still influence is where the surgery happens — because outcomes after a Whipple depend heavily on how often the surgeon and hospital perform it. High-volume centers consistently report lower complication and death rates.
High-volume vs low-volume centers
In pooled data, Whipple procedures performed by high-volume surgeons had markedly lower death rates than those by low-volume surgeons — about 2.4% versus 6.7%. At the highest-volume centers, mortality is roughly 1% to 2%, with overall complication rates lower than at less experienced centers.
📊 Clinical Data Point: Whipple procedures done by high-volume surgeons carried about a 2.4% death rate, versus 6.7% for low-volume surgeons. — Source: a meta-analysis of surgeon volume and Whipple outcomes (PubMed).
Getting a second opinion
Asking about surgical volume is reasonable and expected. Guidelines recommend that decisions about whether a tumor can be removed be made by a multidisciplinary team at a high-volume center.
✅ Patient Action: Ask any prospective surgeon: “How many Whipple procedures do you and this hospital perform each year, and what are your complication and mortality rates?”
Warning signs: when to call your care team
Knowing which symptoms need a call — and which need emergency care — gives patients and caregivers confidence during recovery. When something feels wrong, it is always reasonable to contact your surgical team.
Call your team promptly if…
- You develop a fever or chills
- Abdominal pain is worsening rather than slowly improving
- You can’t keep food or fluids down, or vomiting persists
- The incision becomes red, swollen, warm, or starts draining
- You notice new or worsening yellowing of the skin or eyes
These can signal infection, a leak, or delayed gastric emptying that needs evaluation.
Seek emergency care if…
Severe or sudden symptoms — heavy bleeding, intense unrelenting abdominal pain, difficulty breathing, or signs of a serious reaction — warrant immediate emergency care rather than waiting for a callback.
⚠️ Clinical Warning: A fever with worsening abdominal pain after a Whipple can be an early sign of a leak or infection and should prompt a same-day call to your surgical team. These complications are most treatable when caught early.
✅ Patient Action: Keep your surgical team’s after-hours contact number visible at home, and don’t wait to call if something feels wrong — early contact is safer than waiting it out.
Whipple recovery: frequently asked questions
1. How long does it take to recover from a Whipple procedure?
Whipple procedure recovery happens in phases: about 7 to 14 days in the hospital, several weeks of limited activity at home, and fuller recovery by roughly 2 months — sometimes up to 6 months or longer. Your timeline depends on your surgery type and whether complications arise, so confirm expectations with your surgical team.
2. How long will I be in the hospital after a Whipple?
Most people stay about 8 to 10 days after open Whipple surgery, though 7 to 14 days is common. Minimally invasive (robotic or laparoscopic) surgery can mean a shorter stay of roughly 4 to 6 days. Your length of stay depends on how your recovery progresses and whether any complications develop.
3. What are the most common complications after a Whipple?
The two most common are delayed gastric emptying, where the stomach empties slowly (about 17% of patients), and pancreatic fistula, a leak from the new pancreatic connection (around 9% in some series). Overall, complications affect roughly 30% to 60% of people. Ask your center about its own complication rates.
4. Is recovery from a Whipple procedure painful?
Pain is expected in early recovery and is managed with medication; walking the day after surgery actually helps you recover. Discomfort generally eases over the following weeks as the incision and internal connections heal. Tell your surgical team if pain is worsening rather than improving, since that can signal a problem worth checking.
5. Will I have to change my diet permanently after a Whipple?
Many people make lasting changes — eating small, frequent, protein-focused meals, and often taking pancreatic enzymes to digest fat. Some foods may become harder to tolerate, and tolerance varies from person to person. A registered dietitian can tailor a plan to your digestion, so ask your team for a referral.
6. Will I become diabetic after a Whipple procedure?
Some people develop new or worsened diabetes because part of the pancreas is removed, though a standard Whipple removes only part of it. Diabetes is certain only after a total pancreatectomy, which removes the whole pancreas. Your team will monitor your blood sugar, and you can read more about new-onset diabetes linked to the pancreas. Discuss your individual risk with your care team.
7. When can I drive, work, and exercise again after a Whipple?
Many people return to light normal activities around a month after surgery, with fuller recovery by about 2 months — though it can take longer. Driving, lifting, and returning to work depend on your healing and pain control. Get your surgeon’s clearance before driving or lifting anything heavy.
8. Why does the hospital I choose matter for a Whipple?
Outcomes depend heavily on experience: Whipple procedures done by high-volume surgeons had about a 2.4% death rate, versus 6.7% for low-volume surgeons. The highest-volume centers report mortality of roughly 1% to 2%. Ask any surgeon how many Whipples they and the hospital perform each year.
9. Do I need pancreatic enzymes forever after a Whipple?
Often yes, if the remaining pancreas can’t make enough digestive enzymes — pancreatic enzyme replacement therapy is taken with meals and snacks. Some people need it long term; others need less over time. Your team decides based on your symptoms and tests, so follow their guidance on dosing and timing.
10. Is recovery faster with robotic or laparoscopic Whipple surgery?
Minimally invasive Whipple surgery can mean a shorter hospital stay (roughly 4 to 6 days) and less scarring, although the operation is just as complex as open surgery. Whether it suits you depends on your tumor and your surgeon’s expertise. Ask your surgeon which approach fits your situation and why.
11. What warning signs after a Whipple mean I should call my doctor?
Contact your surgical team promptly for fever, worsening abdominal pain, persistent vomiting, or a red, swollen, or draining incision — these can signal infection or a leak. Seek emergency care for severe or sudden symptoms like heavy bleeding or difficulty breathing. Keep your team’s contact number handy at home.
Moving forward after a Whipple
Recovery from a Whipple procedure is demanding, but it is also well-charted and survivable. Three things are worth carrying with you: recovery happens in predictable phases, most complications are anticipated and managed by your team, and where you have surgery measurably affects your odds.
You have real agency here. Prepare questions for your surgical team, consider seeking care at a high-volume center, and lean on your care team and a registered dietitian as digestion changes.
For the bigger picture of diagnosis, staging, and treatment, return to our complete guide to pancreatic cancer. The road is long, but knowing the map ahead makes each step steadier.
About this content
This medical content is prepared through a structured publishing workflow with expert writing, clinical review and editorial quality checks.

Board Certifications: Internal Medicine (2005); Medical Oncology (2008); Hematology (2009) Experience: 20 years | Location: Houston, Texas Education: BS Biology, Duke University (1999); MD, Baylor College of Medicine…

Board Certifications: Internal Medicine (2010); Clinical Pharmacology (2013) Experience: 15 years | Location: San Francisco, California Education: BS Molecular Biology, Caltech (2000); MD/PhD, UCSF School of Medicine (2007);…

Board Certifications: Preventive Medicine (2010); Public Health & General Preventive Medicine (2010) Experience: 15 years | Location: Washington, DC Education: BA Public Policy, Georgetown University (2001); MD, George…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.