On This Page – Quick Medical Summary
Seeing one line on your CBC differential flagged high or low — while the rest of the report looks fine — is unsettling, especially when the result appears in your patient portal before your doctor has called. A single value slightly outside the reference range is common, and on its own it rarely signals anything serious. What a flagged line actually means depends on which white blood cell it is.
Use this guide to go straight to your result. If your neutrophils are high or low, start there; for a flagged lymphocyte line, read the lymphocyte section; for monocytes, eosinophils, or basophils, use the section covering all three; and if you came here about the neutrophil-to-lymphocyte ratio, skip ahead to that part. Each explains what a shift in that cell commonly reflects — and, just as important, when it is worth a call.
This article focuses on the white blood cell breakdown specifically. For how the test works as a whole, see what your complete blood count can and can’t tell you.
ℹ️ Medical Disclaimer: This article is general health education, not a diagnosis or medical advice. A CBC differential is interpreted by a qualified clinician alongside your full blood count, symptoms, and medical history — one flagged value cannot diagnose a condition by itself. Do not start, stop, or change any treatment based on this page. If you have severe or sudden symptoms such as a high fever, uncontrolled bleeding, or difficulty breathing, seek emergency care. For questions about your results, consult your primary care clinician or a board-certified hematologist.
What a CBC differential measures — and why absolute counts matter
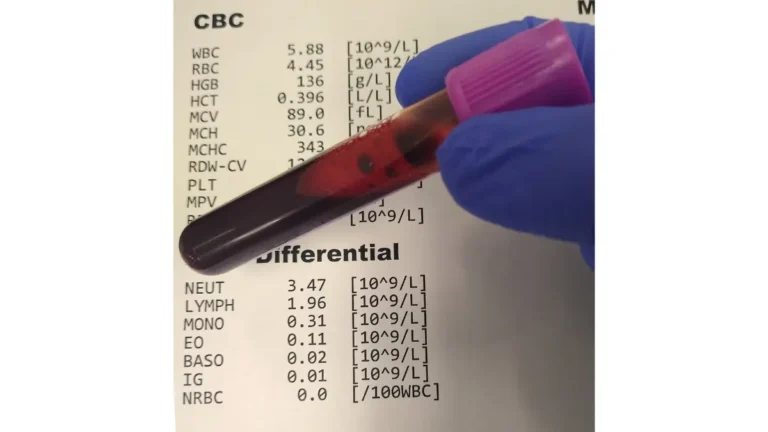
A CBC differential breaks your total white blood cell count into its five types and reports each one as both a percentage and an absolute number. According to the National Library of Medicine, each type has a distinct job in defending the body. Knowing what each cell does makes a flagged line far easier to understand.
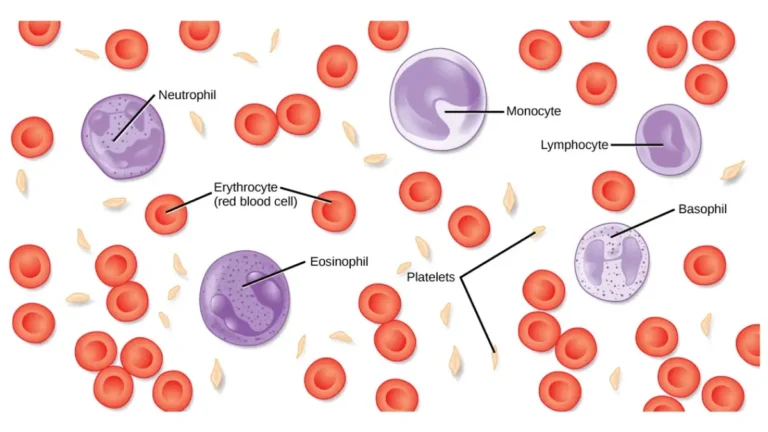
The five white blood cell types
- Neutrophils — your main defense against bacteria and other germs.
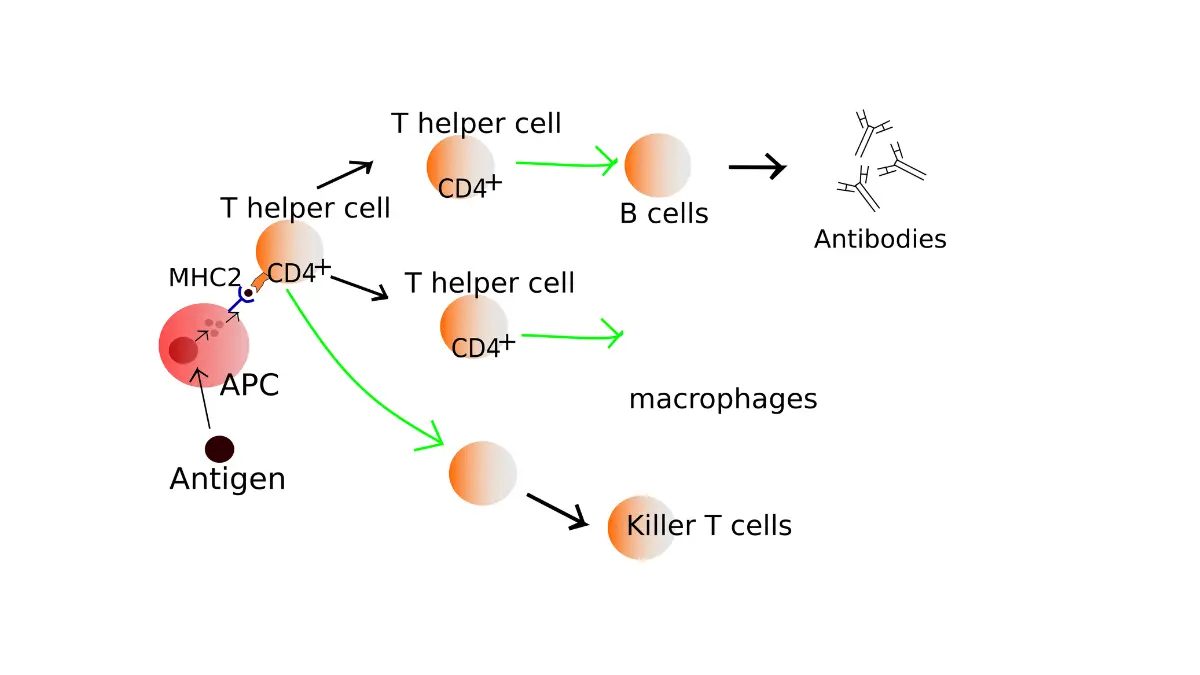
- Lymphocytes — B cells and T cells that fight viruses and target infected or cancerous cells.
- Monocytes — clear germs and dead cells and help coordinate the immune response.
- Eosinophils — act against parasites and play a role in allergies and inflammation.
- Basophils — release chemicals during allergic reactions and asthma.
As a general reference, neutrophils make up about 40–60% of white cells, lymphocytes 20–40%, monocytes 2–8%, eosinophils 1–4%, and basophils 0.5–1%. These proportions come from MedlinePlus, and the exact numbers vary between labs, so compare your result only to the range printed on your own report. The numeric ranges for the rest of the panel are in the full CBC reference-range chart.
Percentage versus absolute count
Here is the point most reports don’t explain: a flagged percentage often means the proportions shifted, not that you truly have too many or too few of a cell. Your result is reported as both a percentage and an absolute count, and clinicians generally weigh the absolute count — the actual number of cells per microliter — because a percentage on its own can mislead.
🔬 How It Works: When your total white blood cell count rises, one cell type’s percentage can climb even though the number of those cells barely changed — the slices shift when the whole pie grows. That is why two people can both show “60% neutrophils” yet have very different absolute counts, and why the absolute number is usually the more useful figure.
You can read what each white blood cell type does in more detail from the National Library of Medicine’s overview of the blood differential.
What high or low neutrophils mean (neutrophilia and neutropenia)
Neutrophils are the body’s first responders to bacterial infection, so they are the line that shifts most often. A high count is called neutrophilia, and a low count is called neutropenia.
📊 Clinical Data Point: Neutrophils normally make up about 40–60% of white blood cells, or roughly 1,500–8,000 per microliter — Source: MedlinePlus (National Library of Medicine) and StatPearls (NCBI), verified against both.

High neutrophils (neutrophilia)
A high neutrophil count most often reflects an acute bacterial infection, inflammation, physical stress on the body, or tissue injury such as after a heart attack — and, less commonly, a bone-marrow condition like chronic leukemia. Any infection or acute stress tends to raise white blood cells overall. Sometimes the report also notes a “left shift,” meaning more young (band) neutrophils have entered the blood, which can accompany an active infection.
Low neutrophils (neutropenia)
A low neutrophil count reduces the body’s front-line defense against bacteria, which is why counts are monitored closely during chemotherapy. Other causes include certain viral infections, some medicines, and problems with the bone marrow. Because a low count can matter clinically, its significance is best judged by your clinician rather than from a number alone.
⚠️ Clinical Warning: A markedly low neutrophil count can raise the risk of serious infection, and this is not something to assess or manage on your own. If you take chemotherapy or another medication known to lower neutrophils and you develop a fever, contact your care team promptly — this can be urgent.
✅ Patient Action: Ask your clinician whether your absolute neutrophil count is low enough to affect your infection risk, and whether you need any specific precautions. You can review the causes behind a high or low count of each cell type at MedlinePlus’s blood differential reference.
What high or low lymphocytes mean (lymphocytosis and lymphopenia)
Where neutrophils rise mainly with bacterial infections, lymphocytes tend to react to viruses. A high count is called lymphocytosis; a low count is called lymphopenia.
High lymphocytes (lymphocytosis)
A high lymphocyte level can point to an acute viral infection such as chickenpox, herpes, or hepatitis. It can also reflect certain bacterial infections like tuberculosis or whooping cough, or a blood cancer such as lymphocytic leukemia or lymphoma. A mild, temporary rise after a recent virus is common and often means little on its own.
Low lymphocytes (lymphopenia)
A low lymphocyte count can accompany autoimmune disorders such as lupus or rheumatoid arthritis. Infections including HIV, tuberculosis, hepatitis, and the flu can lower it too, as can steroid use. Lymphocytes are the B cells and T cells that fight viruses and help identify infected or cancerous cells, so their numbers move with immune activity.
A persistently high or low lymphocyte count is read alongside your symptoms. The plainer terms behind these results — including neutrophilia and lymphocytosis — are explained in the National Library of Medicine’s guide to the white blood count.
What high monocytes, eosinophils, and basophils mean
The three least common lines — monocytes, eosinophils, and basophils — each point in different directions when they rise.
Monocytes (monocytosis)
Monocytes clear germs and dead cells and support the immune response. A high monocyte count can result from a chronic infection such as tuberculosis, ongoing inflammation, or, less often, certain leukemias.
Eosinophils (eosinophilia)
Eosinophils act against parasites and are involved in allergies and inflammation. A high eosinophil count most often reflects allergic conditions such as asthma or eczema, a reaction to a medication, a parasitic infection, or an inflammatory disorder like celiac disease or inflammatory bowel disease.
Basophils (basophilia)
Basophils release chemicals during allergic reactions and asthma. A high basophil count can point to a severe allergic reaction and, less commonly, to certain blood cancers such as chronic myeloid leukemia.
These three are present in small numbers to begin with — monocytes at about 2–8%, eosinophils 1–4%, and basophils 0.5–1% — so a small shift is often not alarming, while a persistent elevation is worth reviewing with your clinician.
The neutrophil-to-lymphocyte ratio (NLR): what it is and what it isn’t
The neutrophil-to-lymphocyte ratio divides your neutrophil count by your lymphocyte count, and it has drawn attention as a simple marker of body-wide inflammation. It is worth understanding honestly, because it is easy to over-read.
What NLR reflects
Researchers have studied the ratio as an indicator of systemic inflammation, and it has shown prognostic value in work on cardiovascular disease, infections, inflammatory conditions, and several cancers. In broad terms, the ratio tends to rise when neutrophils climb and lymphocytes dip, as they can during stress, infection, or inflammation.
📊 Clinical Data Point: In a peer-reviewed study of healthy adults, the neutrophil-to-lymphocyte ratio ranged from about 0.78 to 3.53 — Source: BMC Research Notes (via NCBI), the study that measured NLR values in a healthy population.
Why there’s no single “normal” cutoff
Here is the honest limit: the same researchers who measured that healthy range noted that no clinical cutoff has been established from healthy-population reference values. The ratio is used mainly as a research and prognostic tool, not as a stand-alone diagnosis, and a single reading should not be over-interpreted. You can compare it with other markers of inflammation like CRP, which your clinician may weigh alongside it.
🔬 How It Works: Neutrophils are part of the fast, general (innate) immune response, while lymphocytes drive the slower, targeted (adaptive) response. The ratio between them is thought to reflect the balance between those two systems — which is why it shifts with inflammation but doesn’t, by itself, tell you the cause.
✅ Patient Action: The ratio is not a diagnosis on its own — ask your clinician whether it adds anything meaningful to your specific picture. The full healthy-population data is available in a peer-reviewed reference range for the ratio in healthy adults.
When to worry about an abnormal differential — and when not to
Most single, mild shifts on a differential settle on their own — the real skill is knowing which ones deserve a call. An abnormal differential is a starting point for your clinician, not a verdict.
Signs a differential flag is likely minor
- A single value just outside the range, with no symptoms.
- A recent cold, flu, allergy flare, or stressful stretch — any infection or acute stress can shift white cells.
- A flagged percentage when the absolute count is normal.
Reasons to call your doctor
- A count that is markedly high or low, not just borderline.
- The same abnormality showing up on repeat tests.
- Abnormal or immature cells noted on the report, which typically prompt a blood-smear review.
- New or worsening symptoms alongside the result.
Symptoms that need urgent care
- Unexplained or persistent fever.
- Unusual bruising or bleeding.
- Drenching night sweats or unexplained weight loss.
- Severe fatigue or breathlessness.
Emergency symptoms — not the number alone — are what drive urgent care. On its own, the differential cannot confirm a diagnosis; it is read together with the full CBC and your symptoms.
✅ Patient Action: Ask your primary care clinician whether your differential needs a repeat CBC, a blood-smear review, or a referral to a hematologist. If your main counts were also flagged, see what your main CBC counts may mean and, for a flagged platelet line, decode a platelet result. You can also check your symptoms to help gauge how urgent your situation may be.
Frequently asked questions
1. What does an abnormal CBC differential mean?
An abnormal CBC differential means one or more of your five white blood cell types fell outside your lab’s reference range. On its own this is common and does not confirm a disease — what it suggests depends on which cell is high or low, read alongside your symptoms and the rest of your blood count.
2. What does a high neutrophil count mean?
A high neutrophil count, called neutrophilia, most often reflects a bacterial infection, inflammation, physical stress, or tissue injury such as after a heart attack. Less commonly it points to a bone-marrow condition. Because neutrophils respond fast to infection, a temporary rise during illness is common.
3. What does a low neutrophil count (neutropenia) mean?
A low neutrophil count, or neutropenia, reduces your defense against bacterial infection and can follow chemotherapy, some viral infections, certain medicines, or bone-marrow problems. Because a low count can affect infection risk, discuss its meaning and any precautions with your clinician rather than judging it from the number alone.
4. What do high lymphocytes indicate?
High lymphocytes, or lymphocytosis, often indicate an acute viral infection such as chickenpox, herpes, or hepatitis. They can also reflect certain bacterial infections like tuberculosis or whooping cough, or a blood cancer such as lymphocytic leukemia or lymphoma. A mild rise after a recent virus is frequently temporary.
5. What does a low lymphocyte count mean?
A low lymphocyte count, called lymphopenia, can accompany autoimmune disorders such as lupus or rheumatoid arthritis, infections including HIV, tuberculosis, hepatitis, and the flu, and steroid use. Because lymphocytes track immune activity, a persistently low count is best interpreted by your clinician alongside your history.
6. What causes high eosinophils?
High eosinophils, or eosinophilia, most often result from allergic conditions such as asthma or eczema, a medication reaction, a parasitic infection, or an inflammatory disorder like celiac disease or inflammatory bowel disease. Eosinophils normally make up only 1–4% of white cells, so small shifts are often not alarming.
7. What does a high monocyte count mean?
A high monocyte count, called monocytosis, can result from a chronic infection such as tuberculosis, ongoing inflammation, or, less often, certain leukemias. Monocytes help clear germs and dead cells. Because they normally make up just 2–8% of white cells, a mild elevation is read in the context of your other results.
8. Why do percentages and absolute counts differ on a differential?
Your differential reports each cell type as both a percentage and an absolute number. When your total white blood cell count changes, a cell type’s percentage can shift even if its actual number barely moves. Clinicians generally weigh the absolute count because a percentage on its own can be misleading.
9. Is the neutrophil-to-lymphocyte ratio a reliable test?
The neutrophil-to-lymphocyte ratio is a useful research marker of inflammation, but not a stand-alone diagnostic test. A peer-reviewed study put the healthy-adult range at about 0.78 to 3.53, yet no official clinical cutoff exists. Ask your clinician whether it adds anything to your specific picture.
10. Can an abnormal differential mean leukemia?
An abnormal differential can occasionally reflect a blood cancer such as leukemia or lymphoma, but far more often it reflects infection, allergy, inflammation, stress, or medication effects. A single flagged line rarely points to cancer by itself. Abnormal or immature cells on the report are what prompt further testing with your clinician.
11. When should I worry about an abnormal differential?
Worry less about a single borderline value with no symptoms, and more about a markedly high or low count, the same abnormality on repeat tests, abnormal cells on the report, or new symptoms. Fever, unusual bleeding, night sweats, or severe fatigue warrant prompt medical attention.
The bottom line on your CBC differential
A single flagged line on your CBC differential rarely tells the whole story. Most mild shifts trace back to something ordinary — a recent infection, an allergy, stress, or simply a percentage moving while the absolute count stays normal. What matters is the pattern: whether the change is large, whether it repeats, and whether symptoms come with it.
Your clinician reads the differential together with the rest of your blood count and your history, which is what turns a set of numbers into an answer. If your main counts were flagged too, reading about those next will fill in the rest of the picture — and any marked or lasting abnormality is worth a conversation with your primary care clinician or a hematologist.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.