On This Page – Quick Medical Summary
If you are holding your child’s complete blood count results and a number is flagged, start here. Most parents don’t realize that a child’s normal ranges are not the same as an adult’s, and they shift as a child grows. That single fact explains why a value that looks alarming against an adult range printed in a patient portal, or against a figure you found online, is often completely normal for your child’s age.
This guide is for three situations. If your baby or toddler’s hemoglobin looks low, the section on why counts change explains the normal infant dip. If a specific number is flagged, the by-age chart and the “what it can mean” section are for you. And if you’re preparing for a pediatrician visit, the sections on reading the report and knowing when to call will help you arrive ready. Throughout, the ranges here are approximate — the age-adjusted range printed on your child’s own report is what actually applies, and you can see what a complete blood count measures in our full guide.
ℹ️ Medical Disclaimer: This article is general health information, not a diagnosis, treatment recommendation, or medical advice. Blood test results can only be interpreted in the context of your child’s age, symptoms, history, and physical exam. Reference ranges vary by laboratory. Do not start, stop, or change any care based on this page — bring any abnormal result to your child’s pediatrician, and seek same-day or emergency care if your child appears acutely unwell.
Why normal blood counts change as children grow
A child’s blood counts move with age because their body is actively rebuilding its blood supply during the first years of life. The most common source of parent worry — a lower-than-expected hemoglobin in a baby — is usually a normal, expected phase, not a disease.
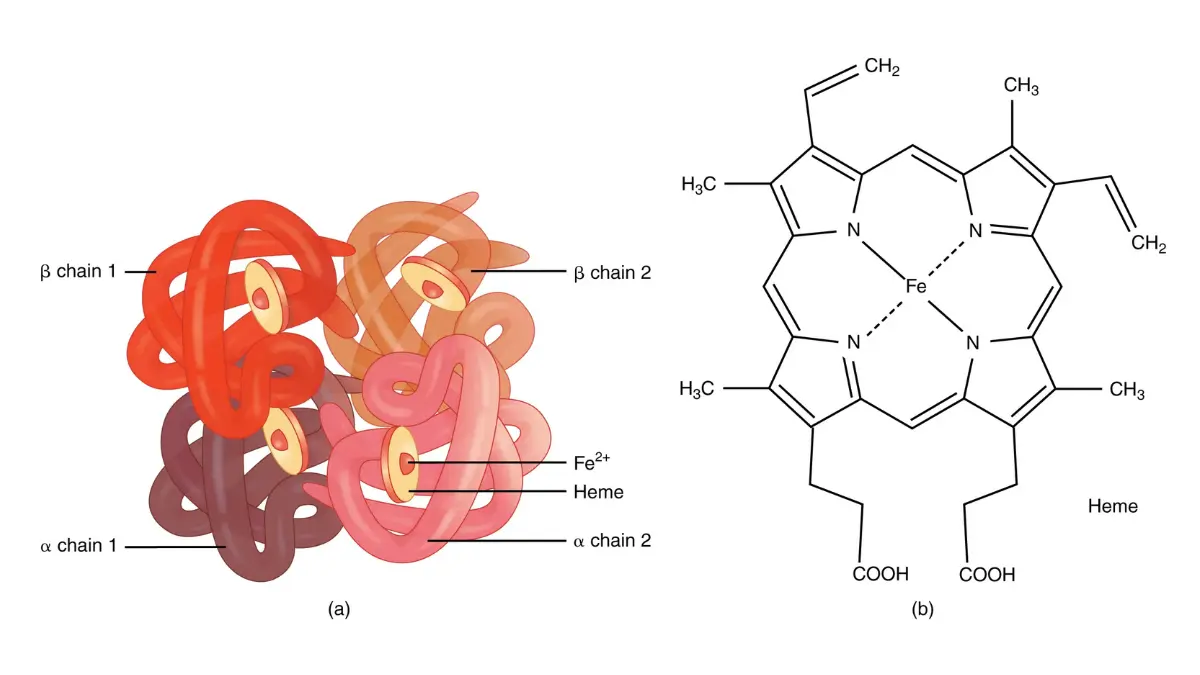
The switch from fetal to adult hemoglobin
Babies are born with mostly fetal hemoglobin, which carried oxygen efficiently in the womb. After birth, the body gradually replaces it with adult hemoglobin over roughly the first six months. You can read more about what hemoglobin and hematocrit measure if those terms are new.
The normal dip: physiologic anemia of infancy
Hemoglobin is highest at birth, then falls to a low point around 2 to 3 months of age before recovering. This dip is normal and self-correcting, and doctors call it physiologic anemia of infancy.
🔬 How It Works: Once a newborn starts breathing, tissue oxygen rises sharply. That signals the body to slow red blood cell production, and because newborn red cells also live a shorter time than adult cells (about 90 days versus 120), hemoglobin naturally drifts down over the first two to three months before production ramps back up. — Merck Manual Professional Edition, Perinatal Anemia.
📊 Clinical Data Point: In healthy full-term infants, the physiologic hemoglobin low point is typically about 9 to 11 g/dL, reached at roughly 2 to 3 months, then rising again. — Merck Manual Professional Edition (Perinatal Anemia).
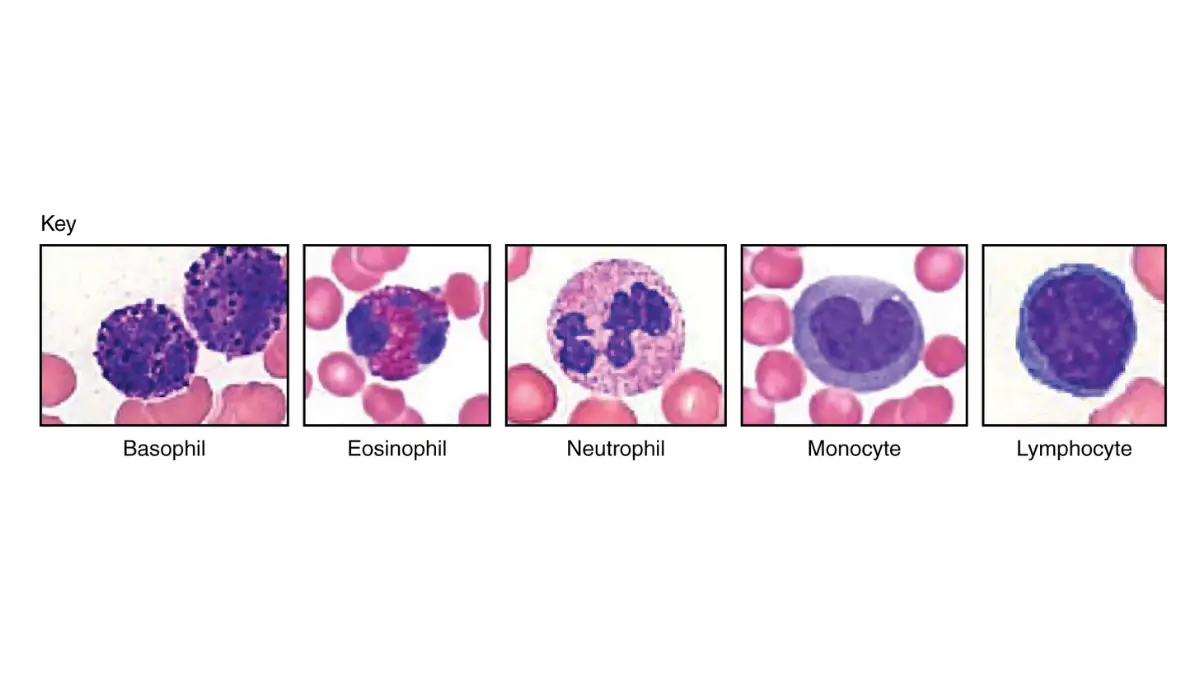
Why white counts start high and settle later
White blood cell counts are also highest at birth and fall over the first months and years. In early childhood, lymphocytes normally outnumber other white cells — the reverse of the adult pattern — before the balance shifts back toward adult proportions during the school years.
Normal CBC ranges for children by age
Normal CBC ranges in children are age-specific and lab-dependent, so use the chart below as a general reference only. The values are approximate and compiled from published pediatric laboratory reference tables and cohort studies; the range printed beside your child’s own result is the one that applies.
| Age group | Hemoglobin (g/dL) | Hematocrit (%) | White blood cells (×10⁹/L) | Platelets (×10⁹/L) |
|---|---|---|---|---|
| Newborn (0–1 month) | ~14–24 | ~44–64 | ~9–30 | ~150–450 |
| Infant (1–12 months) | ~9.5–14* | ~28–42 | ~6–17.5 | ~150–450 |
| Toddler (1–2 years) | ~10.5–13.5 | ~33–39 | ~6–17 | ~150–450 |
| Preschool (3–5 years) | ~11.5–13.5 | ~34–40 | ~5–15 | ~150–450 |
| School-age (6–12 years) | ~11.5–15.5 | ~35–45 | ~5–14.5 | ~150–450 |
| Adolescent girls (13–17) | ~12–16 | ~36–46 | ~4.5–13 | ~150–450 |
| Adolescent boys (13–17) | ~13–17 | ~37–49 | ~4.5–13 | ~150–450 |
* The lower infant figure reflects the normal 2–3 month hemoglobin dip described above, not necessarily a problem. Approximate ranges; they vary by laboratory and analyzer. Sources: published pediatric laboratory reference intervals (LabCorp; American Board of Pathology; Children’s Minnesota; ACCP PedSAP), neonatal cohort data (Pediatrics/PMC), and the Merck Manual. Always compare against the age-adjusted range on your child’s report.
Other values on the report
Two more numbers often appear. MCV (mean corpuscular volume, average red cell size) is normally lower in young children and rises with age toward adult levels, so it is read against an age-adjusted range — you can see what MCV means for more. The red blood cell count in children generally runs about 4.0–5.5 million/µL.
How to use this chart
Match your child’s value to their age band, then check whether it falls near the middle or only just outside the edge. For adult comparison, our standard adult reference ranges show how different the grown-up numbers are — which is exactly why an adult range mis-flags a healthy child.
What high or low CBC results can mean in children
An out-of-range value points to a range of possibilities, most of them common and manageable — but only your child’s pediatrician can say what a specific result means for your child. This section is general education, not a diagnosis.
Low hemoglobin (anemia) in children
Low hemoglobin in children is most often anemia, and the most common cause in young children is iron deficiency. Beyond the normal infant dip, it can follow low dietary iron, rapid growth, or blood loss. Our guide to low hemoglobin and anemia covers this in more depth.
📊 Clinical Data Point: Among US children ages 1–5, an estimated 3.9% have anemia and about 7.1% have iron deficiency, with both more common at ages 1–2 (roughly 13.5% iron deficiency). Current guidance defines anemia in this age group as hemoglobin below about 11 g/dL. — CDC/NHANES analysis (Gupta et al., Nutrients, 2016).
High or low white blood cell count
A high white blood cell count in a child most often reflects a common infection, and the normal upper limit is higher in young children than in adults. A low white blood cell count can follow an ordinary viral illness and is frequently temporary. The white blood cell differential — which types are up or down — often matters more than the total.
Platelet counts outside the range
Platelets help blood clot, and mild changes are common and often transient. A high platelet count in children frequently rises briefly after infection or inflammation, while a low count that appears after a viral illness is also seen and usually rechecked over time.
✅ Patient Action: Ask your child’s pediatrician: “Given my child’s age, symptoms, and this specific number, does this need a repeat test or any further evaluation?”
When a result outside the range is (and isn’t) a concern
A flagged result is not the same as a diagnosis. Three things determine whether an out-of-range number matters: how far outside the range it falls, whether your child has symptoms, and how it compares to any previous results.
Physiologic versus pathologic
Many childhood values sit just outside the “normal” band and are still perfectly healthy — the infant hemoglobin dip is the clearest example. The question a clinician asks is whether a result reflects normal development (physiologic) or an underlying issue (pathologic), and that judgment depends on the whole picture, not one number.
🩺 Physician Note: Reference ranges are built to capture the middle 95% of healthy children, which means about 1 in 20 healthy children will have a value that falls slightly outside “normal” purely by statistics. A single borderline result, in a well child, is frequently just rechecked rather than acted on. — general laboratory and clinical practice; see the NHLBI overview of anemia.
Borderline values and rechecks
A value at the edge of the range often reads differently on a repeat test. Growth spurts, a recent illness, hydration, and even how the sample was drawn can nudge results. This is why a pediatrician may simply repeat the test before doing anything else.
✅ Patient Action: Ask your child’s pediatrician: “Is this value mild enough to simply recheck, or does it need evaluation now given my child’s symptoms?”
How to read your child’s CBC report
Reading the report is mostly about comparing each value to the right column. The goal is not to interpret the numbers yourself, but to arrive at your pediatrician visit knowing which values were flagged and what to ask.
Find the age-adjusted range column
Locate the reference-range column next to each result, and confirm it is age-adjusted for a child rather than a generic adult range. If a portal only shows adult ranges, that is often why a healthy child’s value looks flagged. Our step-by-step guide to how to read a CBC report walks through each line.
Match each value and note the flags
Go line by line — hemoglobin, hematocrit, white cells, platelets — and mark which values fall outside the printed range and by how much. A value flagged “low” that sits right at the edge is different from one far outside.
Prepare questions for the pediatrician
Write down the specific flagged values and any symptoms your child has had. Bringing that short list turns a worried appointment into a focused one.
Red flags: when to call your child’s doctor about blood test results
Most out-of-range results are mild and get sorted out with a recheck. A smaller number deserve a prompt call to the pediatrician, and knowing which is the point of this section.
⚠️ Clinical Warning: Contact your child’s pediatrician promptly if a value is markedly outside the range, or if any abnormal result comes alongside symptoms such as persistent tiredness or paleness, unusual bruising or bleeding, or a recurrent or unexplained fever. If your child appears acutely unwell — very lethargic, struggling to breathe, or with uncontrolled bleeding — seek same-day or emergency care rather than waiting for a routine appointment.
Trust the pediatrician’s interpretation
No chart, including this one, can tell you whether your child is sick. The same number can be reassuring in one child and worth investigating in another, and only a clinician who can examine your child and see the full history can make that call.
✅ Patient Action: Bring the report to your child’s pediatrician and ask: “Which of these values, if any, needs follow-up, and what would the next step be?”
Frequently asked questions about children’s CBC values
1. What is a normal CBC for a child?
Normal CBC values for a child are age-specific and vary by laboratory, so there is no single set of numbers. Newborns have the highest hemoglobin and white cell counts, which fall through infancy and settle toward adult ranges during the school years. Use the by-age chart above as a general reference, and rely on the age-adjusted range printed on your child’s own report.
2. What are normal hemoglobin levels by age?
Hemoglobin is highest at birth (roughly 14–24 g/dL), dips to about 9–11 g/dL around 2–3 months, then recovers. School-age children typically run about 11.5–15.5 g/dL, and in adolescence the ranges differ by sex. These figures are approximate and lab-dependent; ask your child’s pediatrician to interpret any specific value.
3. Why is my child’s white blood cell count high?
In children, a high white blood cell count most often reflects a common infection, and the normal upper limit is higher in young children than in adults. It can also rise temporarily with stress or inflammation. Because context matters more than the number alone, have your child’s pediatrician interpret the result together with symptoms.
4. What is a normal platelet count for a child?
A normal platelet count for a child is roughly 150–450 ×10⁹/L across most pediatric ages. Mild changes are common and often transient — platelets frequently rise briefly after an infection, and a dip after a viral illness is also seen. Any platelet result outside the range should be reviewed by your child’s pediatrician.
5. Is low hemoglobin normal in a baby?
Yes — a temporary dip is normal in healthy infants. Hemoglobin naturally falls to a low point of about 9–11 g/dL around 2–3 months of age, called physiologic anemia of infancy, before rising again. It is a normal phase, not a disease. If you’re unsure whether a baby’s value fits this pattern, ask your child’s pediatrician.
6. At what age do children reach adult blood count ranges?
Children approach adult ranges gradually, with the largest changes in the first year of life and a further shift during adolescence. Hemoglobin, in particular, diverges by sex around puberty, running higher in boys than girls. Because the transition is gradual, values are always read against age-specific — and in teens, sex-specific — reference ranges.
7. What does it mean if my child’s CBC is abnormal?
An abnormal CBC in a child is often mild, developmental, or temporary rather than a sign of serious illness. What matters is how far the value falls outside the range, whether your child has symptoms, and how it compares to previous results. About 1 in 20 healthy children fall slightly outside “normal” by statistics alone. Have your child’s pediatrician interpret it.
8. When should I worry about my child’s blood test results?
Call your child’s pediatrician promptly if a value is markedly out of range, or if an abnormal result comes with symptoms like persistent fatigue or paleness, unusual bruising or bleeding, or recurrent fever. Seek same-day or emergency care if your child appears acutely unwell. For mild, borderline results in a well child, a recheck is often all that’s needed.
9. Do boys and girls have different normal ranges?
Before puberty, boys and girls share very similar CBC ranges. From adolescence onward, hemoglobin and hematocrit run higher in boys than in girls, largely due to hormonal changes. That’s why teen results are compared against sex-specific reference ranges rather than a single childhood range.
10. Why does the lab’s range differ from what I found online?
Reference ranges are specific to each laboratory’s equipment and the population it serves, and for children they are age-adjusted. A generic adult range from a website — or the adult column in a patient portal — can make a perfectly normal child’s value look abnormal. Always compare your child’s result to the range printed on their own report.
11. What is MCV and what’s normal for a child?
MCV (mean corpuscular volume) measures the average size of red blood cells. It is normally lower in young children and rises with age toward adult levels, so it is interpreted against an age-adjusted range rather than the adult one. A value flagged against an adult MCV range may still be normal for a child; ask your child’s pediatrician what it means.
The bottom line on your child’s CBC results
The single most useful thing to remember is that a child’s normal blood counts are age-specific and lab-dependent. A number that looks alarming against an adult range, or against a figure online, is frequently normal for your child’s age — the infant hemoglobin dip is the classic example.
Compare your child’s values to the range printed on their own report, note anything that’s flagged, and let their pediatrician interpret it in the context of age, symptoms, and history. That combination — the right reference range plus a clinician who knows your child — is what turns a worrying printout into a clear answer.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.