On This Page – Quick Medical Summary
What a high platelet count actually means
You opened your lab results, saw platelets flagged high, and want to know what that means. Here is the reassuring part first: most high platelet counts are a temporary reaction to something else in the body, not a sign of a serious blood disorder.
Where you go next depends on your situation:
- Feel fine, found on a routine test? Start with what counts as “high” and the two things it can mean.
- Recent infection, surgery, or low iron? The causes section explains why your count likely rose.
- Symptoms like burning or tingling in the hands and feet, headaches, or vision changes? Read the symptoms and warning-signs sections.
- Told your count is very high, or referred to a blood specialist? The risk and next-steps sections are for you.
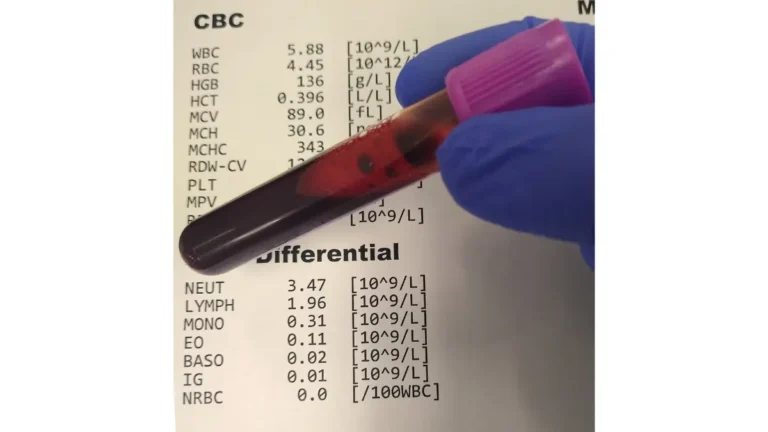
A high platelet count — the medical term is thrombocytosis — simply means more platelets than expected on a complete blood count (CBC). This guide walks through what that number is actually telling you.
ℹ️ Medical Disclaimer: This article is general health information, not medical advice, diagnosis, or treatment. A high platelet count has many possible causes, and only a qualified clinician who can review your full results and history can interpret yours, order the right tests, or recommend any medication, procedure, or treatment. If you have signs of a blood clot or serious bleeding, seek emergency care. For interpretation of your results and any next steps, consult your primary care physician or a board-certified hematologist.
What counts as a high platelet count?
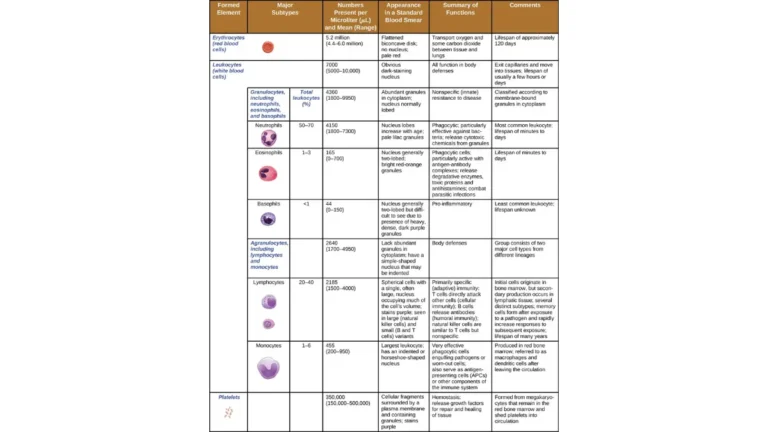
A normal platelet count for adults is roughly 150,000 to 450,000 platelets per microliter of blood, and a high count is generally a result above 450,000.
The normal range (and why sources differ)
You may notice the cutoff isn’t identical everywhere. Most laboratories and the National Heart, Lung, and Blood Institute use 450,000 per microliter as the upper limit, while MedlinePlus lists 400,000 and above as high. Reference ranges also vary slightly from lab to lab, which is why your report shows its own normal range beside your result.
📊 Clinical Data Point: Normal adult platelet count ≈ 150,000–450,000/µL; thrombocytosis is generally a count above 450,000/µL. — Source: NHLBI; StatPearls, Secondary Thrombocytosis (2024).
The two kinds of high platelet count
Every high count falls into one of two categories, and the difference drives everything that follows. Reactive (secondary) thrombocytosis means another condition — such as infection, inflammation, or iron deficiency — pushed the number up temporarily. Essential thrombocythemia is a bone-marrow condition that makes platelets on its own, and it behaves very differently from a low platelet count (thrombocytopenia) or a reactive high one.
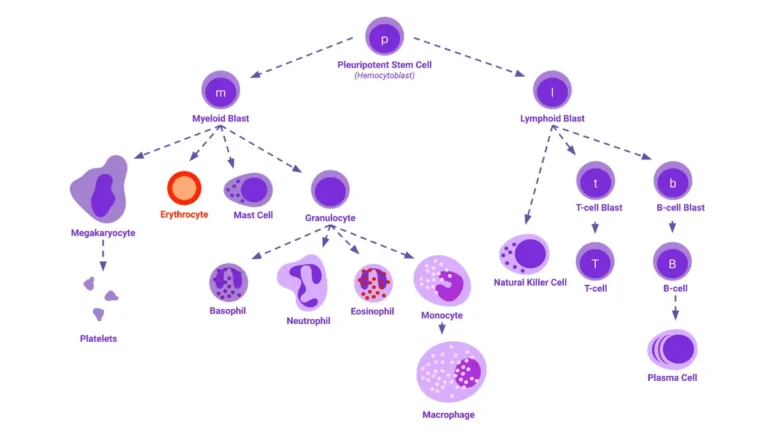
🔬 How It Works: Platelets are made in your bone marrow from large cells called megakaryocytes. In a reactive high count, the marrow is responding normally to a signal elsewhere in the body; in essential thrombocythemia, the marrow cells themselves are overactive and keep producing platelets regardless.
Symptoms and what tests come next
Most people with a high platelet count feel completely normal and only learn about it from a routine blood test. When symptoms do appear, they are usually linked to how platelets affect blood flow, and can include:
- Headaches or dizziness
- Burning, throbbing, redness, or numbness in the hands and feet — a symptom called erythromelalgia
- Visual disturbances
- An enlarged spleen, which a doctor may feel during an exam

Why most people have no symptoms
About a third of people with essential thrombocythemia have no symptoms at diagnosis, and reactive high counts are usually silent too. That is why a high count is so often an incidental finding rather than something you feel.
The tests a doctor may order next
A single high reading is often repeated first, because platelet counts can rise briefly and then settle. If the count stays up, the next steps typically look for a cause:
- A repeat CBC to confirm the elevation persists
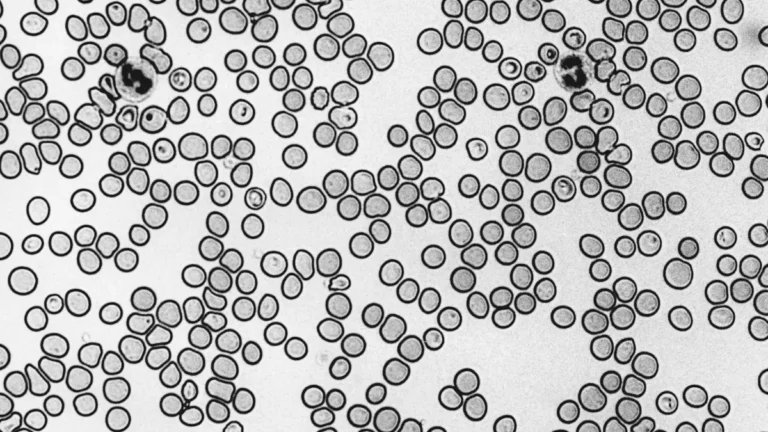
- A blood smear to look at the platelets and other cells under a microscope
- Iron studies and inflammation markers to check for a reactive cause
- Genetic testing (JAK2, CALR, or MPL) and sometimes a bone marrow biopsy if a marrow condition is suspected
You can read more about what the platelet test measures, and if you are trying to make sense of symptoms, our symptom checker can help you organize what to raise with your doctor.
✅ Patient Action: If your count stays high on a repeat test, ask your primary care doctor whether iron studies, inflammation markers, and a referral to a hematologist make sense for your situation.
Reactive vs. essential: what’s causing a high platelet count?
The most common reason for a high platelet count is reactive (secondary) thrombocytosis, in which another condition temporarily raises the number — and it usually resolves once that condition is treated. Sorting reactive from essential is the key step, because the difference between the two types changes what it means for you.
Common reactive triggers
Reactive high counts have many possible causes, and most are things the body is already dealing with:
- Infection — especially acute — and inflammation such as rheumatoid arthritis or inflammatory bowel disease
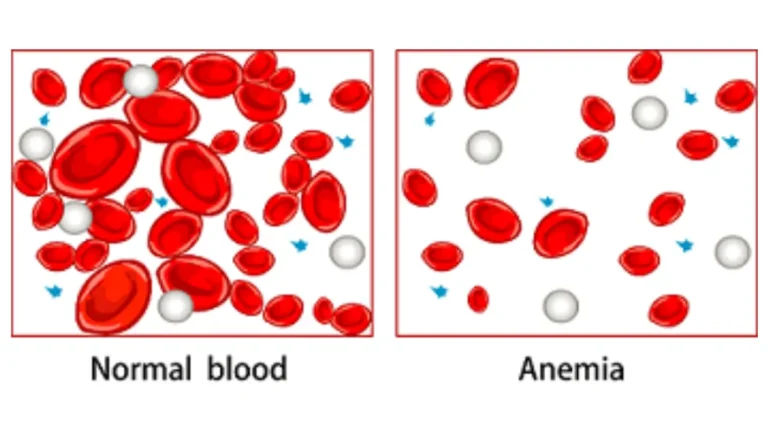
- Iron-deficiency anemia and other anemias
- Recent surgery, trauma, or major blood loss
- Removal of the spleen (splenectomy)
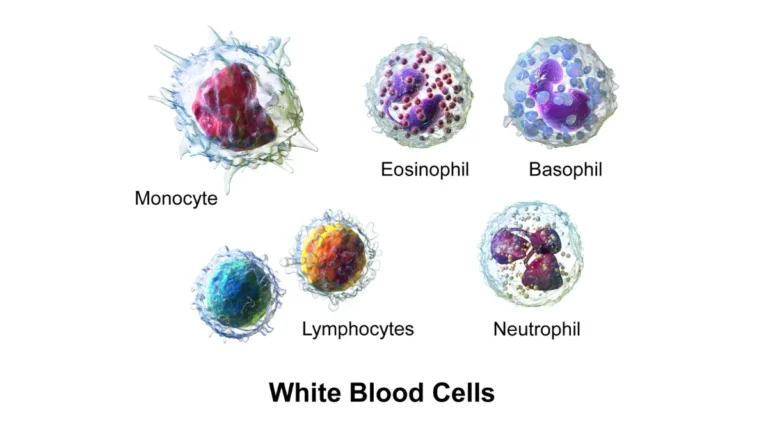
- Alongside a high white blood cell count when an infection is driving both
📊 Clinical Data Point: After spleen removal, a high platelet count occurs in roughly 75–82% of people, usually peaking about 1–3 weeks later and settling over weeks to months. — Source: peer-reviewed case review, NCBI (PMC8245623).
Essential thrombocythemia — when the bone marrow is the cause
When reactive causes are excluded, the diagnosis may be essential thrombocythemia, an uncommon bone-marrow condition classified as a myeloproliferative neoplasm — a type of slow-growing blood cancer. Most cases carry a JAK2 gene change, with CALR and MPL changes accounting for most of the rest, and diagnosis follows World Health Organization criteria after reactive causes are ruled out. In adults it is acquired rather than inherited, is more common in women, and is usually diagnosed between ages 50 and 60.
📊 Clinical Data Point: Essential thrombocythemia is rare — on the order of 1 to 2.5 new cases per 100,000 people per year — and is more common in women. — Source: NCBI Bookshelf and peer-reviewed review literature (PMID 16673273; PMC8051994).
| Feature | Reactive (secondary) thrombocytosis | Essential thrombocythemia |
|---|---|---|
| Cause | Another condition (infection, iron deficiency, surgery) | Overactive bone marrow (a blood cancer) |
| How common | The large majority of high counts | Uncommon |
| Course | Usually temporary | Chronic |
| Clot / bleed risk | Lower | Higher |
| Typical approach | Treat the underlying cause | Monitoring; sometimes platelet-lowering treatment |
| Key clinical detail | Count normalizes when the cause resolves | Diagnosed only after excluding reactive causes |
Source note: NHLBI; StatPearls, Secondary and Essential Thrombocytosis (2024).
How often is a high platelet count serious?
For most people, a high platelet count turns out to be reactive and not a sign of a serious disease. The large majority of high counts fall into this category and often settle once the underlying cause is addressed.
Most cases are reactive — and often resolve
Reactive thrombocytosis is far more common than essential thrombocythemia, and reactive counts usually return to normal after the trigger — an infection, surgery, or iron deficiency — is treated. A repeat CBC is how doctors confirm whether the elevation is passing or persistent.
When a high count can be an early clue
Less commonly, a persistently high platelet count can be one of the earliest signals of an underlying cancer, which is why counts that stay elevated are investigated. In a large UK primary-care study, the one-year risk of a cancer diagnosis after a raised platelet count was 11.6% in men and 6.2% in women, with lung and bowel cancers most common and the risk concentrated in older adults.
📊 Clinical Data Point: In a large primary-care cohort, 11.6% of men and 6.2% of women with a raised platelet count were diagnosed with cancer within one year. — Source: Bailey et al., British Journal of General Practice, 2017.
That figure sounds alarming, so here is the context that matters: the great majority of people with a high platelet count are not found to have cancer, the risk was highest in men over 60, and a high count is a reason to follow up — not a diagnosis in itself.
✅ Patient Action: If your platelet count stays high — especially if you are over 60 — ask your doctor what evaluation makes sense for you, rather than assuming the worst or ignoring it.
Can a high platelet count cause clots or bleeding?
The main concern with a high platelet count is blood clots, though at very high levels the risk can paradoxically shift toward bleeding. Most of this risk applies to essential thrombocythemia rather than to short-lived reactive counts.
Clotting: the main concern
In essential thrombocythemia, extra platelets can make the blood more likely to clot, and clots most often form in the brain, hands, and feet — sometimes causing a transient ischemic attack or, less often, a stroke or heart attack. Knowing the warning signs of a blood clot matters most for people with this condition.
📊 Clinical Data Point: Over the course of the disease, people with essential thrombocythemia face roughly an 11% risk of arterial clots and a 7% risk of venous clots. — Source: Essential Thrombocythemia: A Review, JAMA, 2025.
The bleeding paradox at very high counts
Counterintuitively, when platelet counts climb very high — around 1,000,000 per microliter or more, called extreme thrombocytosis — the risk can tilt toward bleeding rather than clotting.
🔬 How It Works: At extreme counts, the sheer number of platelets can bind and remove a clotting protein called von Willebrand factor, producing a temporary shortage (acquired von Willebrand syndrome) that makes bleeding more likely. Whether extreme counts on their own raise bleeding risk is still debated among specialists — which is one reason these decisions belong with a hematologist rather than being self-managed.
Longer-term risks in essential thrombocythemia
Uncommonly, and usually over many years, essential thrombocythemia can evolve into scarring of the marrow (myelofibrosis) or, more rarely, acute leukemia. These outcomes are the exception rather than the rule, and monitoring is designed to catch changes early.
⚠️ Clinical Warning: Do not start or stop aspirin on your own to manage a high platelet count. Whether aspirin or platelet-lowering treatment helps depends on your individual clotting and bleeding risk, and the wrong choice can cause harm — these decisions require a hematologist.
When should you see a doctor about a high platelet count?
What you do about a high platelet count depends mostly on whether you have warning signs right now. Emergencies come first.
Seek emergency care right away if you have these signs
Call emergency services or go to the nearest emergency room if you notice signs of a blood clot or serious bleeding, such as:
- Sudden weakness or numbness on one side of the body, face drooping, or trouble speaking (possible stroke)
- Chest pain or sudden shortness of breath
- A painful, swollen, red, or warm leg
- Bleeding that will not stop, or unusual or heavy bleeding
When to book a routine follow-up
If you feel well and a high count showed up on routine testing, the usual next step is to discuss it with the doctor who ordered the test. They will typically repeat the CBC to see whether the count stays high, look for a cause, and refer you to a hematologist if it persists or if certain features are present.
🩺 Physician Note: Doctors usually repeat a high platelet count before acting, because a single elevated reading is often temporary. A count that stays high across repeat tests is what prompts a closer look.
✅ Patient Action: Bring a list of recent infections, surgeries, medications, and any bleeding or clotting history to your appointment — these details help your doctor separate a reactive cause from one that needs specialist care.
Frequently asked questions about a high platelet count
1. What is considered a high platelet count?
A high platelet count, or thrombocytosis, is generally a result above 450,000 platelets per microliter, since the normal adult range is about 150,000 to 450,000. Some sources, including MedlinePlus, use 400,000 as the cutoff, and reference ranges vary slightly by lab — so check the normal range printed beside your own result.
2. Is a high platelet count serious — should I worry?
Usually not. Most high platelet counts are reactive — a temporary response to infection, inflammation, surgery, or low iron — and settle once the cause is treated. Less often, a persistently high count points to a bone-marrow condition or, rarely, an early cancer clue. A count that stays high should be evaluated by your doctor.
3. What is the most common cause of a high platelet count?
The most common cause is reactive (secondary) thrombocytosis, where another condition raises the count temporarily. Frequent triggers include infection, inflammation, iron-deficiency anemia, recent surgery or trauma, and removal of the spleen. Because these counts usually normalize once the underlying issue resolves, doctors often repeat the blood test before pursuing further investigation.
4. Can a high platelet count be a sign of cancer?
Sometimes. A persistently high platelet count can be an early clue to an underlying cancer, which is why counts that stay elevated are investigated. In one large primary-care study, cancer was diagnosed within a year in 11.6% of men and 6.2% of women with a raised count — but most people with a high count do not have cancer. Discuss persistent elevation with your doctor.
5. What’s the difference between reactive and essential thrombocytosis?
Reactive (secondary) thrombocytosis is a high platelet count caused by another condition, such as infection or iron deficiency, and it is usually temporary. Essential thrombocythemia is a bone-marrow condition — a type of blood cancer — that produces too many platelets on its own, tends to be chronic, and carries higher clotting and bleeding risks.
6. What are the symptoms of a high platelet count?
Most people have no symptoms and learn of a high platelet count from a routine blood test. When symptoms occur, they are usually clot-related: headaches, dizziness, visual changes, and burning, throbbing, or numbness in the hands and feet (erythromelalgia). An enlarged spleen may also be present and found during a physical exam.
7. Can iron deficiency cause a high platelet count?
Yes. Iron-deficiency anemia is one of the common reactive causes of a high platelet count. When iron is low, the bone marrow can produce extra platelets, and the count often returns to normal once the deficiency is corrected. Your doctor may order iron studies to check for this before pursuing other tests.
8. When is a high platelet count an emergency?
Seek emergency care if you have signs of a blood clot or serious bleeding. Warning signs include sudden weakness or numbness on one side, face drooping or trouble speaking, chest pain or sudden shortness of breath, a painful swollen leg, or bleeding that will not stop. These need immediate medical attention.
9. Can a high platelet count return to normal on its own?
Often, yes. Reactive high counts usually return to normal once the underlying cause — an infection, surgery, or iron deficiency — is treated or resolves. A repeat CBC is how doctors confirm whether the count is passing or persistent. A high count from essential thrombocythemia, by contrast, is ongoing and needs monitoring.
10. How is a high platelet count diagnosed — what tests come next?
After a high platelet count, doctors usually repeat the CBC to confirm it persists, then look for a cause with a blood smear, iron studies, and inflammation markers. If a bone-marrow condition is suspected, genetic testing (JAK2, CALR, or MPL) and sometimes a bone marrow biopsy follow. Ask your doctor which tests fit your situation.
11. Is essential thrombocythemia a type of cancer?
Yes. Essential thrombocythemia is classified as a myeloproliferative neoplasm, a slow-growing blood cancer in which the bone marrow makes too many platelets. It is usually chronic and, uncommonly and over many years, can evolve into marrow scarring (myelofibrosis) or, more rarely, acute leukemia. A hematologist guides monitoring and any treatment.
The bottom line on a high platelet count
Most of the time, a high platelet count is your body reacting to something temporary — an infection, a recent surgery, or low iron — rather than a sign of a serious blood disorder. The count is best thought of as a prompt to find the cause, not a diagnosis on its own.
The practical path is straightforward: confirm whether it stays high on a repeat test, look for a reactive cause, and watch for the warning signs that need urgent care. If it persists, a hematologist can help sort out why.
✅ Patient Action: Bring your result to the doctor who ordered it and ask whether a repeat CBC and a check for a cause — such as iron studies or inflammation markers — are the right next step for you. For the bigger picture, see how to read your full CBC results.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.