On This Page – Quick Medical Summary
What your flagged glucose number means
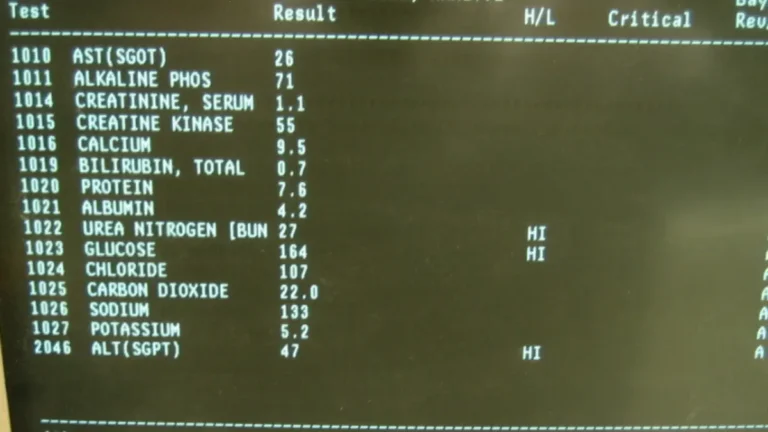
If your comprehensive metabolic panel came back with glucose flagged in red, the number almost always sits in one of two ranges — 100 to 125 mg/dL, or 126 mg/dL and above. They mean very different things.
One variable decides which yardstick applies: whether you fasted.
Start here:
- Fasted 8+ hours → the fasting thresholds below apply to your number.
- Ate, drank, or aren’t sure → read the next section first.
- Glucose 200 mg/dL or higher, or you have excessive thirst, frequent urination, or unexplained weight loss → skip to the red-flag section now.
- Glucose under 70 mg/dL → the low-glucose rows below apply to you.
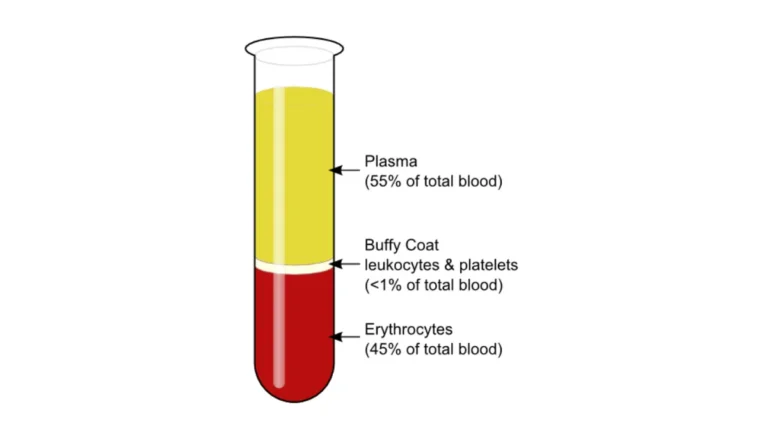
A single fasting plasma glucose on a CMP does not diagnose diabetes. It is a screening signal — the first of two results.
ℹ️ Medical Disclaimer: This is general health education, not a diagnosis, treatment plan, or medication recommendation, and it creates no clinician–patient relationship. Interpreting your result, diagnosing prediabetes or diabetes, any decision to start, stop, or change a medication, and any coverage question belong to a licensed clinician with your full record — start with your primary care physician.
What the glucose line on a CMP is actually measuring
Your CMP measured 14 substances in one tube of blood. Glucose is one of them.
Glucose is one of 14 markers on the panel
The panel covers five areas: blood sugar, kidney markers, liver markers, proteins, and electrolytes plus calcium. MedlinePlus, the NIH’s patient library, describes the comprehensive metabolic panel as a routine screen of your metabolism.
Glucose is a snapshot — the sugar circulating at the moment the needle went in. The same healthy person reads 88 mg/dL before breakfast and 140 mg/dL an hour after it.
Why the fasting question changes the answer
Fasting has a precise clinical definition: no caloric intake for at least 8 hours. Water is fine.
That matters because the diagnostic thresholds you have seen online — 100, 126 — were built for fasting samples only. Applied to a non-fasting draw, they will frighten you with a number that means something else.
CMPs are frequently drawn without fasting: at physicals, before surgery, in the emergency department. Our guide to whether you need to fast for a CMP explains how to find out.
Your glucose number: normal, prediabetes, or diabetes range
On a fasting sample, glucose below 100 mg/dL is normal, 100 to 125 mg/dL is prediabetes, and 126 mg/dL or above falls in the diabetes range. These cut points come from the American Diabetes Association.
If you fasted for at least 8 hours
| Fasting glucose (mg/dL) | What it’s called | Key clinical detail |
|---|---|---|
| Below 100 | Normal | Below the impaired-fasting-glucose threshold. |
| 100–125 | Prediabetes | The ADA’s definition of impaired fasting glucose. |
| 126 or above | Diabetes range | Meets the threshold; still requires confirmation. |
| Below 70 (54 or above) | Level 1 hypoglycemia | An alert value, not automatically urgent. |
| Below 54 | Level 2 hypoglycemia | Where symptoms typically appear. |
Source: American Diabetes Association, Standards of Care in Diabetes—2026, Section 2. Our blood sugar converter translates these to mmol/L.
If you didn’t fast — or aren’t sure
Most sites skip this. On a random sample, the ADA defines exactly one diagnostic threshold: 200 mg/dL or above, with classic symptoms.
There is no prediabetes band for a random draw. A non-fasting glucose of 130 cannot be called prediabetes — that category does not exist for a random sample. A fasting glucose or an A1C is needed before anyone can classify it.
If your glucose came back low
Under 70 mg/dL is an alert value; under 54 mg/dL is clinically significant. Both are covered in the red-flag section below. For context, see what a normal blood sugar result looks like.
🩺 Physician Note: Absent unequivocal hyperglycemia, ADA guidance requires two abnormal results to diagnose — two different tests at the same time, or the same test repeated. One CMP glucose, however high, is the first of two.
How common is an elevated glucose result?
More common than most people expect, and the national figures were revised upward this year.
What the newest national numbers show
📊 Clinical Data Point: 115.2 million US adults have prediabetes — more than 2 in 5. An estimated 40.1 million people have diabetes, about 1 in 8. Of adults with diabetes, 27.6% — roughly 11.0 million — do not know it. Source: CDC, National Diabetes Statistics Report, updated January 21, 2026.
Those figures replaced the older estimates of 97.6 million and 38.4 million, still quoted across much of the health web.
Why most people never find out
Prediabetes and early type 2 diabetes are usually silent — no pain, no symptom, nothing to prompt a test. Which is why more than 1 in 4 adults with diabetes never know.
That reframes your result. A flagged glucose is early information, arriving before symptoms. To compare your own profile, try our genetic risk assessment tool.
Why glucose can read high — or low — without diabetes
Several ordinary things push glucose off baseline. Ruling them out is part of what the follow-up test does.
You didn’t fast, and nobody told you to
The most common explanation. A glucose of 118 mg/dL two hours after a sandwich is a different finding from 118 mg/dL after an overnight fast.
Stress, illness, and medications
Acute stress and acute illness raise blood sugar, because the body releases hormones that drive the liver to produce more glucose.
Medications do the same. A 2024 review in Diabetes Therapy, indexed on PubMed, links glucocorticoids such as prednisone, antipsychotics, statins, beta blockers, diuretics, some anti-infectives, cancer therapies, and immunosuppressants to changes in glucose metabolism.
⚠️ Clinical Warning: Never stop, reduce, or skip a prescribed medication because of a lab result. Steroids, blood-pressure drugs, and antipsychotics treat conditions where stopping abruptly carries its own serious risk. Bring the result to the clinician who prescribed it.
When the number itself is off
This one is almost never explained to patients, and it runs opposite to what you would expect.
🔬 How It Works: Blood cells keep consuming glucose after the tube leaves your arm. In an unseparated sample at room temperature, glucose falls roughly 5–7% per hour — about 5 to 10 mg/dL in the first hour alone. The result reads lower than your true value. Fluoride tubes slow this; they do not stop it immediately.
A delayed sample makes a borderline result look better than it is, not worse. Falsely low glucose is a documented cause of missed prediabetes diagnoses — which is why glucose is read alongside the rest of the panel, including the kidney markers on the same report.
What happens next: how one number becomes a diagnosis
No — a CMP cannot diagnose diabetes, and was never designed to. It is a screen. ADA guidance requires two abnormal results: two different tests at the same time, or the same test repeated.
Why one result is never enough
The one exception is unequivocal hyperglycemia — a random glucose of 200 mg/dL or above with classic symptoms. There, no confirmation is required.
The three tests that confirm
- A1C — a 2–3 month average, no fasting needed. Below 5.7% normal, 5.7–6.4% prediabetes, 6.5%+ the diabetes range. See what an A1C of 5.7% to 6.4% means.
- Repeat fasting glucose — retests the same moment under controlled conditions.
- Oral glucose tolerance test — the only one detecting impaired glucose tolerance, which a CMP structurally cannot see.
What to ask at your appointment
✅ Patient Action: Ask your primary care physician: (1) Was my glucose draw fasting? (2) Do you want to confirm with an A1C or a repeat fasting glucose? (3) Do any of my medications affect blood sugar? (4) If this is prediabetes, am I eligible for a National Diabetes Prevention Program?
📊 Clinical Data Point: A structured lifestyle change program cut the risk of developing type 2 diabetes by 58% versus placebo — 71% in adults aged 60 and older, roughly double metformin’s 31%. Target: 5–7% body-weight loss plus 150 weekly minutes of moderate activity. Source: CDC, National Diabetes Prevention Program.
Screening criteria activate at a BMI of 25, or 23 in Asian Americans — our BMI calculator will tell you yours.
When a glucose result shouldn’t wait
Most flagged glucose results can wait for a scheduled appointment. A few cannot.
Symptoms that change the timeline
⚠️ Clinical Warning: A glucose of 200 mg/dL or higher together with excessive thirst, frequent urination, or unexplained weight loss is not a wait-and-see result. The ADA treats that combination as unequivocal hyperglycemia — a diagnosis requiring no second test. Contact a clinician the same day. With confusion, rapid breathing, or vomiting, seek emergency care.
High glucose alongside a low bicarbonate (CO₂) warrants urgent attention, not routine follow-up — our guide to the electrolyte results on a CMP explains why those lines are read together.
When a low number is the emergency
A glucose below 54 mg/dL is clinically significant. In someone not taking diabetes medication, a genuinely low value needs evaluation, not reassurance.
The sample-handling artifact above is real. But it is an explanation your clinician confirms — not a reason to dismiss a low number, especially if you had symptoms at the draw.
✅ Patient Action: If your glucose is below 70 mg/dL and you are not on diabetes medication, call your primary care physician this week and ask: “Should this be repeated, and could it be a sample-handling artifact?”
Common questions about a high glucose result on a CMP
1. What does high glucose on a CMP mean?
On a fasting sample, 100–125 mg/dL is prediabetes and 126 mg/dL or above falls in the diabetes range under ADA criteria. On a non-fasting sample, only 200 mg/dL or higher with classic symptoms is diagnostic. A single value never confirms a diagnosis. Ask your primary care physician which follow-up test they want.
2. Is a glucose level of 105 on a CMP bad?
If you fasted at least 8 hours, 105 mg/dL sits inside the 100–125 mg/dL prediabetes band — above normal, but well below the diabetes threshold of 126 mg/dL. If you did not fast, 105 mg/dL cannot be classified at all, because no prediabetes category exists for a random sample.
3. Can a CMP diagnose diabetes?
No. A CMP is a screening test, not a diagnostic one. ADA guidance requires two abnormal results — either two different tests collected at the same time, or the same test repeated later. The one exception is a random glucose of 200 mg/dL or above with classic symptoms. Your physician orders the confirming test.
4. Do you have to fast for a CMP glucose test?
Fasting means no caloric intake for at least 8 hours; water is allowed. But CMPs are frequently drawn without fasting — at annual physicals, before surgery, or in the emergency department. If nobody told you to fast, you probably did not, and the fasting thresholds do not apply to your number.
5. What glucose level is dangerous?
A glucose of 200 mg/dL or higher combined with excessive thirst, frequent urination, or unexplained weight loss warrants same-day contact with a clinician. A glucose below 54 mg/dL is clinically significant hypoglycemia. Confusion, rapid breathing, or vomiting alongside a high glucose warrants emergency care rather than a phone call.
6. Can stress or illness raise blood glucose?
Yes. Acute stress and acute illness both raise blood sugar, because the body releases hormones that drive the liver to produce more glucose. A sample drawn during an infection, an injury, or a hospital stay may not reflect your baseline — one reason a single abnormal value is confirmed rather than acted on.
7. Can medications cause a high glucose result?
Yes. A 2024 review indexed on PubMed links glucocorticoids such as prednisone, antipsychotics, statins, beta blockers, diuretics, certain anti-infectives, cancer therapies, and immunosuppressants to changes in glucose metabolism. Never stop a prescribed medication over a lab result — bring it to the clinician who prescribed the drug.
8. What if my CMP glucose is 126 or higher?
On a fasting sample, 126 mg/dL is the ADA’s diabetes threshold — but it still requires confirmation, either with a second test collected at the same time or a repeat later. It is not yet a diagnosis. Contact your primary care physician this week and ask which confirming test they want to run.
9. What does a low glucose result on a CMP mean?
A glucose below 70 mg/dL is a Level 1 alert value; below 54 mg/dL is Level 2, clinically significant. In someone not taking diabetes medication, either warrants evaluation. It can also be an artifact of delayed sample processing. Ask your primary care physician whether the result should be repeated.
10. How often should glucose be rechecked?
ADA guidance sets screening at age 35 for all adults, and at any age for adults with overweight or obesity plus at least one additional risk factor. If the result is normal, repeating at minimum three-year intervals is reasonable — sooner if symptoms appear or your risk profile changes.
11. Can a high glucose result on a CMP be wrong?
It can mislead in both directions. A non-fasting draw reads higher and cannot be judged against fasting thresholds. Delayed sample processing reads lower — glucose falls roughly 5–7% per hour in an unseparated tube at room temperature, which can mask a borderline result rather than create a false alarm.
What to do with your result
Three things, in order.
Find out whether your draw was fasting. It decides which thresholds apply — and most people do not know.
Book the confirming test. One glucose value is a signal, not a verdict — the ADA requires two abnormal results before anyone calls it diabetes.
And if you have the red-flag symptoms above, do not wait for the appointment you already have.
A flagged glucose is early information. More than 1 in 4 adults with diabetes never get that warning. If other lines were flagged too, read the rest of your panel.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.