On This Page – Quick Medical Summary
What Is Laminectomy? Cost & Success Rates in 2026
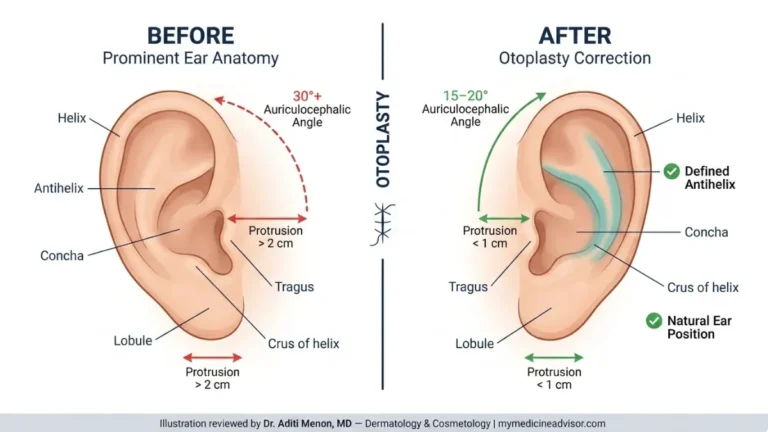
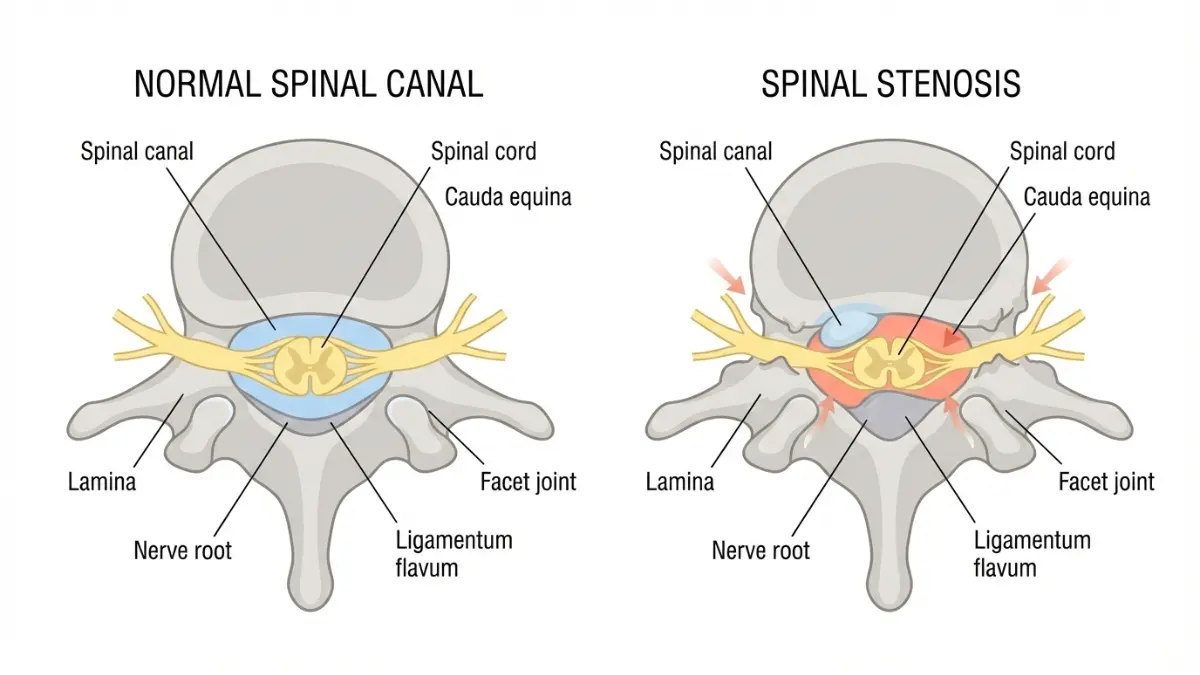
Laminectomy is a surgical procedure that removes part of the vertebral bone (lamina) to relieve pressure on spinal nerves, with costs ranging from $50,000 to $90,000 in 2026 and success rates reaching 90% for properly selected patients with spinal stenosis.
Sarah Martinez, 58, couldn’t walk more than 50 feet without severe leg pain shooting down both legs. After 14 months of failed physical therapy and epidural injections, her neurosurgeon recommended lumbar laminectomy. Twelve weeks post-surgery, Sarah walked three miles pain-free—a transformation experienced by nine out of ten patients who undergo this spinal decompression procedure.
Understanding Laminectomy Surgery
Laminectomy, also called decompression surgery, is one of the most common spinal procedures performed on adults over 65 years old. The surgery involves removing the lamina—the back portion of the vertebra covering your spinal canal—to create more space for compressed nerves.
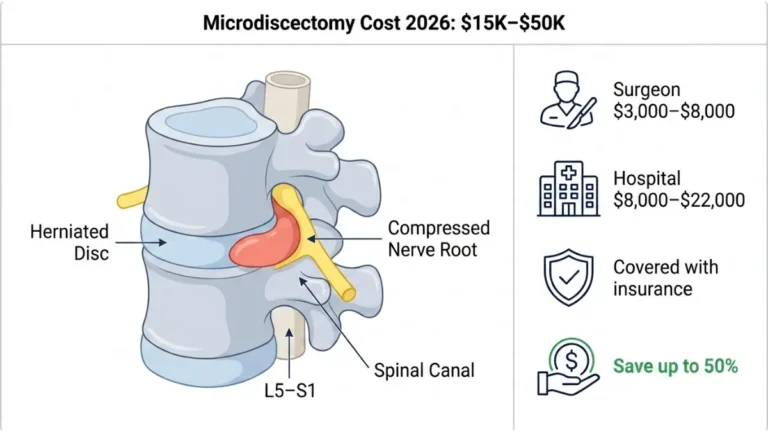
During the procedure, surgeons may also remove bone spurs, thickened ligaments, or herniated disc material causing nerve compression. This spinal stenosis treatment typically addresses conditions that conservative treatments like medications, injections, and physical therapy have failed to improve after 12 weeks.
The surgery targets three primary areas:
- Central canal stenosis – narrowing of the main spinal canal
- Lateral recess stenosis – compression where nerves branch off the spinal cord
- Foraminal stenosis – narrowing of nerve exit pathways between vertebrae
Most patients spend 1-3 hours in surgery under general anesthesia. Minimally invasive laminectomy techniques use smaller incisions (1-2 inches) compared to traditional open surgery (4-6 inches), resulting in faster recovery times and reduced surgical complications.
2026 Cost Breakdown by Procedure Type
| Laminectomy Type | Average Cost Range | Hospital Stay | Recovery Time |
|---|---|---|---|
| Single-level lumbar laminectomy | $50,000 – $65,000 | 0-1 days | 4-6 weeks |
| Multi-level lumbar laminectomy | $75,000 – $90,000 | 1-2 days | 6-8 weeks |
| Cervical laminectomy | $55,000 – $70,000 | 1-2 days | 6-8 weeks |
| Minimally invasive laminectomy | $50,000 – $62,000 | 0-1 days | 3-5 weeks |
| Laminectomy with fusion | $80,000 – $120,000 | 2-4 days | 4-6 months |
The total spine surgery cost includes surgeon fees (30%), hospital facility charges (50%), anesthesia (10%), and post-operative care including physical therapy (10%). Geographic location significantly impacts pricing, with procedures in the Northeast costing 40% more than those performed in the Midwest.
Medicare covers approximately 80% of approved laminectomy costs after meeting Part B deductibles, while private insurance typically covers 70-90% depending on your plan. Outpatient surgical centers charge $15,000-$25,000 less than hospital-based procedures for single-level cases.
Success Rate Statistics (2026 Data)
Clinical studies demonstrate that laminectomy surgery success rates reach impressive benchmarks when patients are properly selected. The procedure delivers significant pain relief and functional improvement for the vast majority of spinal stenosis patients.
Short-term outcomes (6-12 weeks):
- 88.1% of patients report successful pain relief at 6 weeks
- 90% achieve improved walking distance and reduced leg pain
- 85% reduce or eliminate daily pain medication use
- 75% return to normal daily activities without restrictions
Long-term outcomes (1-5 years):
- 86.7% maintain pain relief improvements at 6 months
- 70.8% sustain functional benefits at 5-year follow-up
- 82% of patients rate their outcome as “much improved” or “somewhat improved”
- 18% require revision surgery within 5 years due to recurrent stenosis
Success rates vary by the specific condition treated. Patients with isolated central canal stenosis achieve 88% success rates, while those with combined stenosis and herniated disc conditions see 78% success rates. The presence of lateral recess stenosis alone shows 64% success outcomes.
Understanding these laminectomy success rate factors helps you set realistic expectations. Use symptom tracking tools to monitor your condition before and after surgery, ensuring you’re documenting the severity of leg pain, walking limitations, and quality of life impacts.
Patient age, overall health status, smoking history, and obesity significantly influence outcomes. Individuals with a body mass index above 35 experience 30% higher complication rates and slower healing compared to patients at healthier weights.
Commercial Bridge: Considering laminectomy for your spinal stenosis? Understanding the $50,000-$90,000 investment and 90% success rate helps you make informed decisions about this back pain surgery. Schedule consultations with board-certified spine surgeons who perform at least 50 procedures annually to discuss your candidacy for decompression surgery versus conservative treatments.
Laminectomy Cost Analysis: Insurance, Payment & Financing Options
Average Laminectomy Cost in US (2026)
Hospital-based laminectomy procedures cost between $75,000 and $90,000 in 2026, while outpatient surgical centers charge $50,000 to $65,000 for single-level decompression surgery. The substantial price difference reflects facility overhead costs, with hospital operating rooms charging premium rates compared to ambulatory surgical centers.
Geographic location dramatically impacts spine surgery cost. Northeast facilities charge an average of $82,000 for single-level lumbar laminectomy, while Midwest surgical centers average $58,000 for identical procedures—a 41% cost difference based solely on ZIP code.
Cost breakdown by expense category:
- Surgeon professional fees: $18,000 – $27,000 (30% of total)
- Hospital facility charges: $30,000 – $45,000 (50% of total)
- Anesthesia services: $6,000 – $9,000 (10% of total)
- Post-operative care: $6,000 – $9,000 (10% of total)
Medicare’s national average reimbursement for CPT code 63047 (single-level laminectomy) totals $7,727 in hospital outpatient settings, with Medicare paying $6,182 and patients responsible for $1,545 after meeting deductibles. Private insurance negotiations typically result in payments ranging from $40,000 to $65,000 for the same procedure.
Factors Affecting Laminectomy Surgery Cost
Multiple variables influence the final bill for spinal stenosis surgery beyond the base surgical fee. Understanding these cost drivers helps patients anticipate their total financial commitment before scheduling the procedure.
Procedure complexity factors:
- Single-level vs multi-level: Each additional vertebral segment adds $12,000 – $18,000
- Traditional vs minimally invasive laminectomy: MIS approaches cost $3,000 – $8,000 more due to specialized equipment
- Laminectomy without fusion vs with fusion: Adding spinal fusion increases costs by $25,000 – $35,000
- Cervical vs lumbar location: Neck procedures average $5,000 – $8,000 higher than lower back
Regional cost variations (single-level lumbar laminectomy):
- Northeast: $78,000 – $92,000
- West Coast: $72,000 – $88,000
- Southeast: $62,000 – $75,000
- Midwest: $55,000 – $68,000
- Rural areas: $48,000 – $62,000
Comorbidities significantly impact pricing. Patients with diabetes, cardiovascular disease, or obesity require additional monitoring and longer hospital stays, increasing total costs by 15-30%. Assessing your overall health metrics before surgery helps predict potential complications and associated expenses.
Insurance Coverage for Spinal Stenosis Surgery
Private insurance companies cover 70-90% of medically necessary laminectomy costs after deductibles and coinsurance obligations. Medicare Part B covers outpatient laminectomy procedures at 80% of approved amounts, with beneficiaries paying 20% coinsurance plus any unmet deductibles.
Typical insurance coverage breakdown:
- Medicare coverage: 80% after $240 annual deductible (2026 rate)
- Commercial PPO plans: 70-80% after $2,500 – $5,000 deductible
- Commercial HMO plans: 85-95% after $1,500 – $3,000 deductible
- High-deductible health plans: 60-70% after $5,000 – $8,000 deductible
Out-of-pocket maximums protect patients from catastrophic expenses. Once you reach your plan’s annual limit ($9,450 for individuals or $18,900 for families in 2026), insurance covers 100% of remaining qualified expenses.
Pre-authorization requirements:
Insurance companies mandate prior approval for spinal decompression cost coverage. Submit documentation including:
- MRI or CT imaging confirming spinal stenosis diagnosis
- Conservative treatment records (physical therapy, injections, medications for 12+ weeks)
- Surgeon’s medical necessity letter with CPT codes 63047 (single level) or 63048 (additional levels)
- Neurological examination findings documenting functional impairments
Denials occur in 12-18% of initial submissions. Appeal immediately with additional clinical documentation emphasizing failed conservative treatments and progressive neurological symptoms affecting daily function.
Payment Plans & Medical Financing
Hospital payment programs allow eligible patients to spread laminectomy recovery costs over 12-36 months without interest charges. Most facilities offer these arrangements for balances between $2,000 and $25,000, requiring no credit check and featuring automatic monthly withdrawals.
Medical credit card options:
- CareCredit: 0% APR for 24 months on purchases over $2,500 (15.9% after promotional period)
- Prosper Healthcare Lending: Loans from $1,000 – $100,000 at 6.99% – 28.99% APR
- Alphaeon Credit: 0% APR for 18 months on amounts over $2,000
Health Savings Accounts and Flexible Spending Accounts cover qualified medical expenses including surgery, anesthesia, hospital stays, and physical therapy. These pre-tax dollars reduce your effective laminectomy cost by 25-35% depending on your tax bracket.
International surgery cost comparison:
Medical tourism destinations offer substantial savings but require careful evaluation of surgeon credentials and facility accreditation:
- India: $8,000 – $15,000 (85% savings)
- Mexico: $12,000 – $22,000 (70% savings)
- Thailand: $18,000 – $28,000 (60% savings)
- United States: $50,000 – $90,000 (baseline)
Travel expenses, accommodation costs, and follow-up care challenges partially offset international savings. Consider complications requiring emergency reoperation—returning to the original surgeon becomes logistically difficult and financially devastating.
Hidden Costs of Laminectomy Recovery
Physical therapy represents the largest post-operative expense beyond the surgical bill itself. Standard protocols require 2-3 sessions weekly for 8-12 weeks, totaling 24-36 visits at $125 – $200 per session depending on facility type and insurance coverage.
Post-discharge expenses (4-6 month recovery):
- Physical therapy: $3,000 – $7,200 (24-36 sessions)
- Prescription medications: $800 – $2,400 (pain management, muscle relaxants, anti-inflammatories)
- Medical equipment: $200 – $600 (back brace, shower chair, grabber tool, elevated toilet seat)
- Lost wages: $8,000 – $24,000 (6-12 weeks partial/full disability)
- Home health aide: $2,400 – $7,200 (first 2-4 weeks if living alone)
- Transportation to appointments: $300 – $800 (unable to drive 2-4 weeks)
What This Means For You: The true cost of back pain surgery extends significantly beyond the operating room bill. Budget an additional $15,000 – $40,000 for recovery-related expenses and lost income when evaluating laminectomy procedure affordability.
Disability insurance covers 60-70% of gross income during recovery periods. Short-term disability kicks in after 7-14 day waiting periods and continues for 12-26 weeks depending on policy terms. Review your coverage before surgery to understand benefit amounts and duration limits.
Commercial Bridge: Calculate your total laminectomy insurance coverage and out-of-pocket expenses before scheduling surgery. Contact your insurance provider with CPT codes 63047 and 63048 to get pre-authorization and precise cost estimates. Compare facility pricing between hospital outpatient departments and ambulatory surgical centers to potentially save $15,000 – $25,000 on identical procedures.
Similar to other major surgical procedures, understanding upfront costs prevents financial surprises during recovery when focusing on healing should be your only priority.
Laminectomy Procedure: Surgical Techniques & What to Expect
Step-by-Step Laminectomy Procedure
The laminectomy procedure begins with general anesthesia administration, ensuring complete unconsciousness and pain control during the 1-3 hour surgery. Anesthesiologists monitor vital signs continuously while the surgical team positions you face-down on a specialized operating table with padding to protect pressure points.
Pre-operative preparation (24-48 hours before):
- Fasting for 8-12 hours before surgery
- Discontinuing blood thinners (aspirin, warfarin, Plavix) 5-7 days prior
- Showering with antiseptic soap (chlorhexidine) the night before
- Removing jewelry, contact lenses, and nail polish
- Arranging transportation home (cannot drive post-anesthesia)
During the surgical procedure:
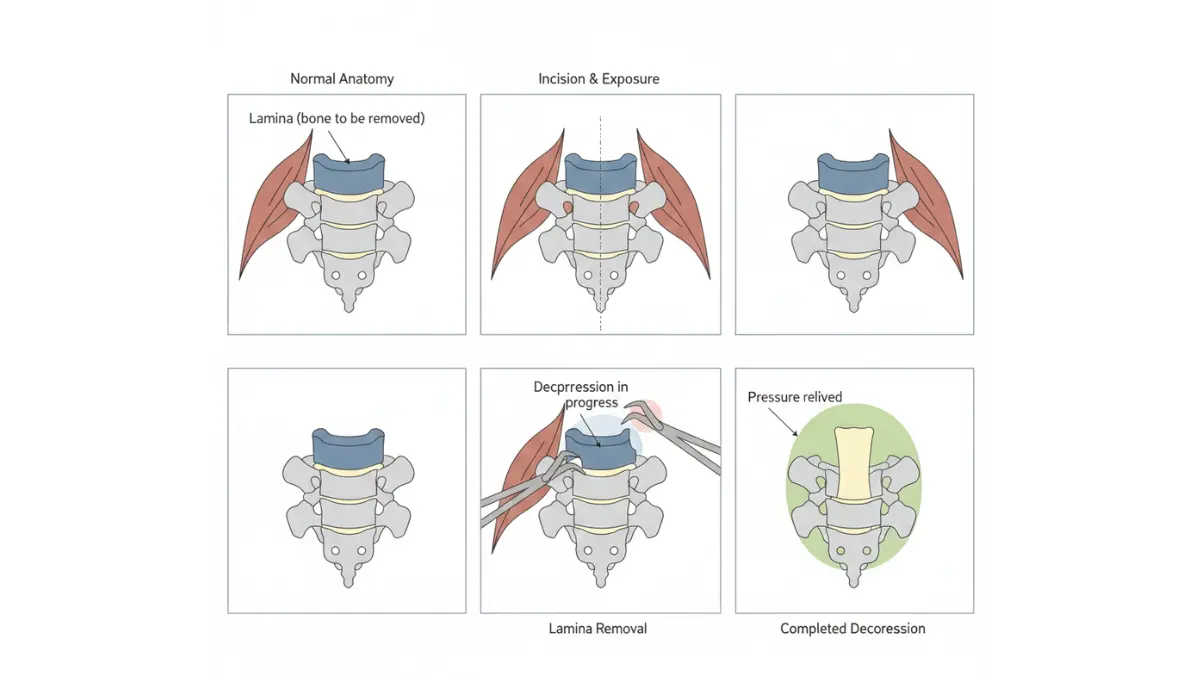
The surgeon makes a midline incision over the affected vertebrae, typically 2-4 inches for open procedures or 1-2 inches for minimally invasive techniques. Muscle tissue is carefully separated using specialized retractors, exposing the bony lamina—the posterior arch of your vertebra covering the spinal canal.
Using high-speed burrs and surgical instruments under microscopic visualization, the surgeon removes the lamina bone piece by piece. This decompression creates immediate space for compressed nerve roots and spinal cord tissue.
Additional structures may be addressed during decompression surgery:
- Ligamentum flavum: Thickened ligament removed to enlarge spinal canal
- Bone spurs (osteophytes): Bony growths shaved down with precision tools
- Herniated disc fragments: Protruding disc material excised if compressing nerves
- Facet joints: Partial trimming to access lateral recess stenosis
Real-time nerve monitoring technology tracks electrical signals throughout the procedure, alerting surgeons immediately if neural structures experience stress. This safety protocol reduces nerve injury risk to less than 1% in experienced hands.
Types of Laminectomy Surgery
Traditional open lumbar laminectomy remains the gold standard for multi-level spinal stenosis and complex cases requiring extensive decompression. The surgeon works through a 3-5 inch incision with direct visualization of all spinal structures, allowing complete removal of compressive elements.
Minimally invasive laminectomy uses tubular retractors or endoscopes inserted through 1-2 inch incisions. Specialized instruments pass through narrow tubes, removing bone and tissue while protecting surrounding muscles from unnecessary trauma. Recovery time decreases by 40-50% compared to open procedures due to reduced soft tissue injury.
Cervical laminectomy addresses neck spinal stenosis through posterior (back of neck) approaches. The surgeon removes cervical lamina from C3-C7 vertebrae, decompressing the spinal cord without disturbing anterior structures like the esophagus and carotid arteries.
Laminectomy with discectomy combines lamina removal with herniated disc material extraction. This approach treats patients suffering from both spinal stenosis and disc herniation surgery needs simultaneously, eliminating multiple surgical interventions.
Laminectomy vs Fusion Comparison
| Factor | Laminectomy Alone | Laminectomy + Fusion |
|---|---|---|
| Surgery duration | 1-2 hours | 3-5 hours |
| Hospital stay | 0-1 days | 2-4 days |
| Recovery time | 4-6 weeks | 4-6 months |
| Return to work | 2-4 weeks | 3-6 months |
| Average cost | $50,000 – $65,000 | $80,000 – $120,000 |
| Reoperation rate | 34% within 5 years | 14% within 5 years |
| Spinal mobility | Preserved | Limited/eliminated |
| Best candidates | Stenosis without instability | Stenosis + spondylolisthesis |
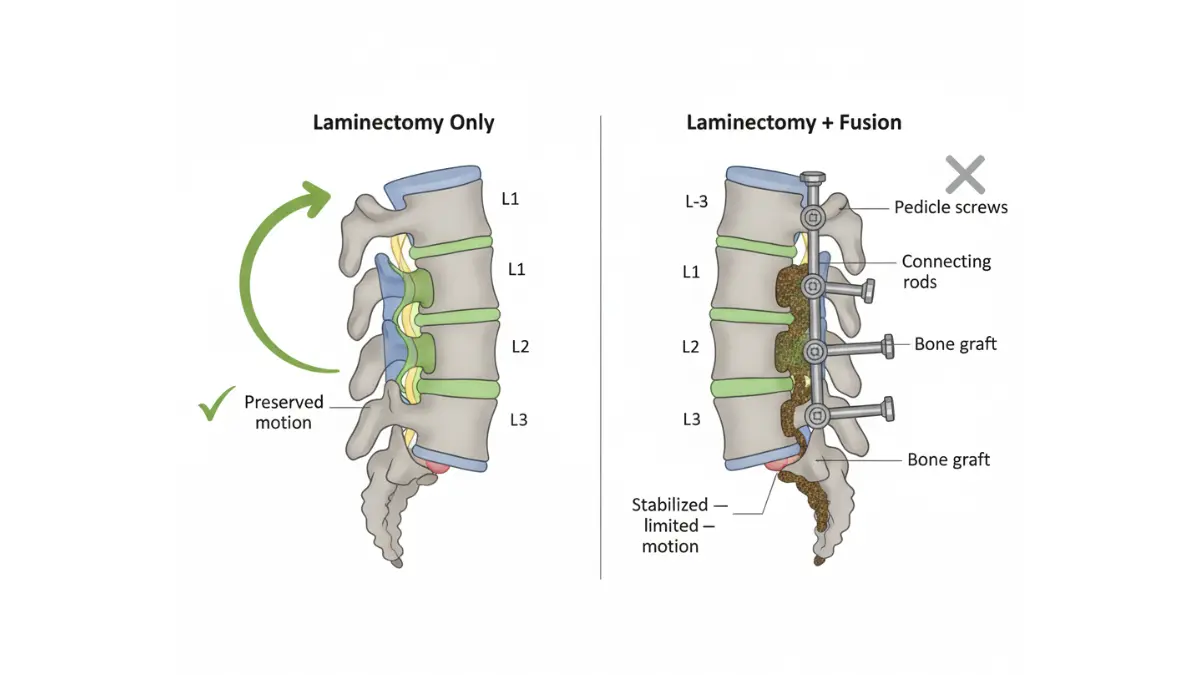
Research comparing these approaches demonstrates that fusion adds meaningful improvement in physical health-related quality of life for patients with degenerative spondylolisthesis—a condition where one vertebra slips forward on another. However, laminectomy without fusion suffices for isolated stenosis cases without spinal instability.
Blood loss averages 150-300ml for standalone decompression but increases to 400-800ml when fusion hardware is added. The extended operative time and additional instrumentation explain the significant cost differential between procedures.
Minimally Invasive Laminectomy Benefits
Minimally invasive techniques revolutionized spine surgery by achieving identical decompression through smaller incisions. Tubular retractors create working channels measuring 14-18mm in diameter, allowing instrument access while muscle tissue remains intact around the tube.
Advantages over traditional open surgery:
- 50% faster recovery: Return to normal activities in 3-5 weeks vs 6-8 weeks
- 60% less blood loss: Average 100ml vs 250ml intraoperative bleeding
- Outpatient eligibility: 65% of patients go home same day vs overnight stays
- Smaller scars: 1-2 inch incisions vs 4-6 inch traditional openings
- Reduced infection risk: 0.5% vs 2% surgical site infection rates
- Less muscle damage: Dilating rather than cutting paravertebral muscles
Endoscopic approaches take minimization further, using cameras and specialized instruments through ports as small as 7mm. Surgeons visualize the operative field on high-definition monitors, performing precise bone removal under magnified views.
Not every patient qualifies for minimally invasive laminectomy. Candidates must have single-level or two-level stenosis without significant spondylolisthesis or prior surgery at the affected level. Complex multi-level disease or revision cases often require traditional open approaches for adequate visualization and decompression.
What Happens During Decompression Surgery
The core objective of all decompression surgery techniques focuses on relieving pressure from neural structures while maintaining spinal stability. Surgeons follow systematic steps regardless of whether open or minimally invasive approaches are utilized.
Lamina removal technique:
High-speed pneumatic drills thin the lamina bone to eggshell consistency. Surgeons then use specialized instruments called Kerrison rongeurs—angled punches that nibble away remaining bone fragments without touching underlying dura (spinal cord covering). This incremental approach prevents sudden movements that could injure neural tissue.
Ligamentum flavum resection:
After lamina removal exposes the yellow ligament (ligamentum flavum), surgeons carefully separate it from the dura using fine dissectors. This thickened ligament often contributes significantly to canal narrowing, so complete removal is essential for adequate decompression.
Facet joint preservation:
Preserving at least 50% of facet joint structures maintains spinal stability and reduces future fusion needs. Surgeons carefully balance aggressive decompression with stability preservation, removing only the medial (inner) portion of facets when accessing lateral recess stenosis.
Spinal cord pressure relief verification:
Before closing incisions, surgeons verify complete decompression by gently probing around nerve roots with blunt instruments. Adequate space allows instruments to pass freely beside nerves without resistance—confirming successful pressure relief that translates to symptom improvement.
Commercial Bridge: Discuss minimally invasive laminectomy options with your spine surgeon to potentially reduce recovery time and surgical complications. Board-certified neurosurgeons and orthopedic spine specialists performing 50+ annual procedures demonstrate superior outcomes compared to low-volume surgeons.
Laminectomy Recovery Time: Week-by-Week Timeline & Success Factors
Laminectomy Surgery Recovery Timeline
The laminectomy recovery time varies significantly based on surgical approach, patient age, and the number of spinal levels decompressed. Most patients experience three distinct recovery phases marked by progressive improvements in mobility, pain reduction, and functional capacity.
Week 1-2: Immediate Post-Operative Phase
Hospital discharge occurs within 0-2 days for uncomplicated single-level procedures, with most minimally invasive laminectomy patients leaving the same day. Pain management focuses on scheduled medications rather than waiting for severe discomfort—taking opioids, muscle relaxants, and anti-inflammatories as prescribed prevents pain escalation.
Walking begins within 4-6 hours post-surgery, with nursing staff assisting your first steps. Short walks of 5-10 minutes every 2-3 hours reduce blood clot risk and promote healing circulation. Avoid sitting for longer than 30-45 minutes during this crucial period.
Week 3-6: Early Recovery Phase
Physical therapy typically begins 4-6 weeks post-operatively for standard laminectomy cases, focusing on proper body mechanics and core stabilization. Sessions occur 2-3 times weekly for 6-8 weeks, totaling 12-24 supervised visits.
Most patients resume driving at 2-3 weeks if not taking narcotic pain medications and can comfortably perform emergency braking maneuvers. Desk work return happens at 2-4 weeks for sedentary jobs, while physical labor positions require 8-12 weeks minimum.
Week 7-12: Active Rehabilitation Phase
Exercise intensity increases significantly during this phase. Walking goals expand to 30 minutes twice daily, with gradual progression to treadmill workouts and recumbent cycling. Resistance training begins using light weights, resistance bands, and pulley systems while maintaining neutral spine positioning.
Core strengthening targets transverse abdominis and lumbar multifidus muscles—the deep stabilizers protecting your spine from future injury. Proper nutrition supports tissue healing, with protein requirements increasing to 1.2-1.5 grams per kilogram of body weight during active recovery.
Month 4-6: Return to Full Activity
Patients with fusion procedures require 4-6 months for complete bone healing, while standalone decompression allows return to normal activities by 3-4 months. Sports participation and recreational activities resume gradually under physical therapist guidance, progressing from low-impact to high-impact movements.
Laminectomy Healing Time Factors
Individual recovery timelines vary dramatically based on patient-specific factors that either accelerate or delay the healing process. Understanding these variables helps set realistic expectations for your laminectomy surgery recovery journey.
Age impact on recovery:
- Under 50 years: 4-6 weeks to normal activities
- 50-65 years: 6-8 weeks to normal activities
- Over 65 years: 8-12 weeks to normal activities
- Over 75 years: 12-16 weeks to normal activities
Older patients experience slower tissue regeneration and often have multiple comorbidities complicating recovery. However, chronological age matters less than biological health status—a fit 70-year-old often heals faster than a sedentary 55-year-old with diabetes and obesity.
Health conditions affecting laminectomy healing time:
- Diabetes: 30-40% longer healing, increased infection risk
- Smoking: 50% slower bone and soft tissue healing
- Obesity (BMI > 35): 25-35% increased complication rates
- Cardiovascular disease: Extended hospital stays, slower mobilization
- Osteoporosis: Higher refracture risk, modified activity restrictions
Smoking cessation before surgery dramatically improves outcomes. Patients who quit 4-8 weeks pre-operatively demonstrate healing rates comparable to non-smokers.
Surgical complexity factors:
- Single-level: 4-6 week recovery baseline
- Two-level: Add 1-2 weeks to recovery timeline
- Three+ levels: Add 2-4 weeks to recovery timeline
- Minimally invasive approach: 40% faster return to activities
- Revision surgery: 50-75% longer recovery than primary procedures
Post Laminectomy Recovery Best Practices
Successful recovery requires active patient participation beyond simply attending physical therapy sessions. Daily habits and activity modifications during the initial 12 weeks determine long-term surgical outcomes and prevent complications.
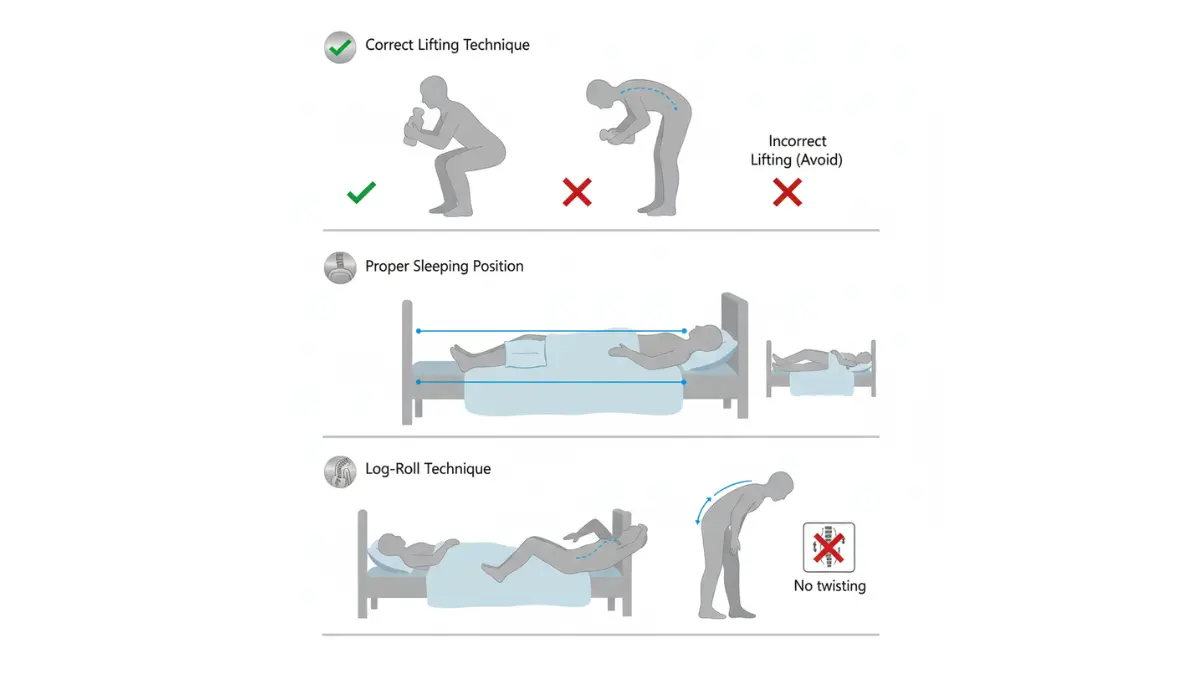
Activity restrictions (First 6-12 weeks):
- NO bending at waist: Use log-rolling technique in bed, squat with knees to pick items up
- NO lifting over 10 pounds: Includes groceries, laundry baskets, children, pets
- NO twisting motions: Turn entire body rather than rotating spine
- NO high-impact activities: Running, jumping, contact sports remain prohibited
- NO prolonged sitting: Stand and walk every 30-45 minutes
Pain management strategies:
Medication schedules follow a stepwise approach. Begin with maximum prescribed doses for the first 5-7 days, then gradually taper as pain improves. Ice packs applied 20 minutes every 2-3 hours reduce inflammation and discomfort during week 1-2.
Heat therapy replaces ice after week 2, when inflammatory phase concludes. Moist heat penetrates deeper than dry heat, making heating pads with moisture settings more effective for muscle relaxation.
Sleep position recommendations:
Side-lying with pillow between knees maintains neutral spine alignment and reduces nerve root tension. Back sleeping requires a pillow under knees to decrease lumbar lordosis. Stomach sleeping remains prohibited for 8-12 weeks as it hyperextends the surgical site.
Wound care and infection prevention:
Keep surgical incisions dry for 48-72 hours post-discharge. After initial healing, gentle soap and water cleansing during showers prevents infection. Watch for warning signs including increased redness, warmth, swelling, drainage, or fever above 101°F (38.3°C).
Laminectomy Physical Therapy Program
Structured rehabilitation protocols following evidence-based guidelines optimize outcomes while preventing reinjury. Three distinct phases build upon each other, progressively challenging your spine’s stability and strength.
Phase 1 (Week 2-4): Gentle Mobilization
- Walking program: Start 5-10 minutes three times daily, increase by 5 minutes weekly
- Ankle pumps and gentle knee bends while lying down
- Deep breathing exercises to prevent pneumonia
- Postural education for sitting, standing, and sleeping positions
- Proper body mechanics training for daily activities
- Goal: Independent movement without assistive devices
Phase 2 (Week 5-8): Active Strengthening
- Transverse abdominis activation: Hold 5 seconds × 10 repetitions, three times daily
- Lumbar multifidus contractions targeting deep spinal stabilizers
- Bilateral leg stretches: hamstrings, hip flexors, gastrocnemius 3 × 30 seconds
- Wall squats maintaining neutral spine: 2 sets × 10-15 repetitions
- Supine abdominal crunches (not full sit-ups)
- Stationary bike: 10-15 minutes at low resistance
- Goal: Pain-free completion of daily activities
Phase 3 (Week 9-12): Advanced Conditioning
- Progressive resistance training with bands and light weights (under 15 pounds)
- Multi-plane stabilization exercises challenging balance
- Proprioceptive training on unstable surfaces
- Aerobic conditioning: 30-45 minutes walking or cycling
- Sport-specific movement patterns if relevant
- Goal: Return to recreational activities and physical hobbies
Cost considerations:
Outpatient physical therapy averages $100-150 per session without insurance. Most plans cover 20-30 visits annually with $20-50 copays. Complete post-laminectomy physical therapy programs totaling $2,400-3,600 represent a worthwhile investment preventing future spine problems costing far more.
When to Resume Daily Activities
Gradual activity progression prevents setbacks while allowing adequate healing time. Rushing back to full activities increases reoperation risk and can damage decompressed nerve roots still recovering from years of compression.
Driving: 1-2 weeks after discontinuing narcotic medications, once you can comfortably turn your head/torso and perform emergency brake maneuvers without hesitation.
Desk work: 2-4 weeks for sedentary office jobs with ergonomic workstation setup allowing frequent position changes every 30 minutes.
Light household chores: 3-4 weeks for tasks like washing dishes, folding laundry (no lifting baskets), preparing meals.
Physical labor jobs: 8-12 weeks minimum for construction, nursing, warehouse work requiring lifting, bending, and prolonged standing.
Sexual activity: 4-6 weeks following surgeon approval, using positions avoiding spinal flexion, extension, or twisting movements.
Exercise and sports: 3-4 months for impact activities like running, tennis, skiing; 4-6 months for contact sports or activities with fall risk.
Signs of Successful Recovery
Tracking improvement milestones confirms your laminectomy surgery recovery progresses normally. Document weekly changes to discuss with your surgeon and physical therapist during follow-up appointments.
Pain reduction benchmarks:
- Week 2: 25% reduction in leg pain intensity
- Week 4: 50% reduction in radiating symptoms
- Week 8: 75% improvement in neurogenic pain
- Week 12: 80-90% resolution of pre-operative leg symptoms
Functional improvement markers:
- Walking distance: Double baseline distance by week 4, triple by week 8
- Medication needs: 50% reduction in opioid use by week 2, off narcotics by week 4-6
- Sleep quality: Sleeping 6+ hours without waking from pain by week 3-4
- Daily activity tolerance: Completing full self-care tasks independently by week 3
John’s 8-Week Recovery Journey:
John, 62, underwent single-level L4-L5 laminectomy after 18 months of progressively worsening leg pain limiting his walking to 100 yards. Week 1 post-surgery brought immediate 60% relief in leg symptoms despite incision discomfort. By week 4, he walked one mile pain-free—ten times his pre-operative distance. Week 8 marked his return to part-time work and hiking three miles on flat trails. At 12 weeks, John completed a five-mile hike with his wife, something impossible before surgery.
Commercial Bridge: Track your recovery milestones and use rest optimization tools to ensure adequate healing time during the critical first 12 weeks. Maintain regular communication with your surgical team—reporting concerns early prevents minor issues from becoming major complications requiring additional intervention.
Laminectomy Success Rate, Complications & Long-Term Outcomes
Laminectomy Surgery Success Rate Data (2026)
The laminectomy surgery success rate reaches 90% for appropriately selected patients with lumbar spinal stenosis, making it one of the most effective treatments for nerve compression conditions. Success is defined as significant pain reduction, improved walking capacity, and enhanced quality of life measures sustained for at least 12 months post-operatively.
Short-term success rates demonstrate immediate and substantial improvements. At 6 weeks post-surgery, 88.1% of patients report successful pain relief and functional restoration. This impressive early outcome validates the procedure’s effectiveness for addressing compressed nerve roots.
Long-term outcome data (1-11 year follow-up):
Studies tracking patients for extended periods reveal that 70.8% maintain improvement at 5+ years after surgery. The gradual decline from 88% at 6 weeks to 71% at 5 years reflects natural spinal aging processes rather than surgical failure. Two-thirds of patients sustain long-term benefits, representing excellent durability for a decompression procedure.
Patient satisfaction rates provide additional success metrics beyond clinical measurements. Seventy-five percent of laminectomy patients rate their outcomes as “much improved” or “somewhat improved” at 2-year follow-up. These subjective assessments often matter more to patients than objective clinical findings—the ability to walk without leg pain transforms daily life regardless of imaging results.
Success Rates by Condition Treated
| Spinal Condition | 6-Week Success | 1-Year Success | 5-Year Success | Reoperation Rate |
|---|---|---|---|---|
| Central canal stenosis | 88.1% | 86.7% | 70.8% | 18% |
| Stenosis + herniated disc | 78.0% | 77.2% | 66.6% | 22% |
| Lateral recess stenosis | 64.0% | 65.2% | 63.6% | 35% |
| Cervical stenosis | 85.0% | 80.0% | 68.0% | 16% |
| Multi-level stenosis | 75.0% | 72.0% | 58.0% | 28% |
Isolated central canal stenosis achieves the highest success rates, with 88% of patients experiencing significant symptom relief at 6 weeks. Combined conditions involving both stenosis and herniated disc material demonstrate moderately lower success at 78%, though still representing excellent outcomes for most patients.
Lateral recess stenosis presents the most challenging scenario, with only 64% success rates even at early follow-up. This anatomical variant compresses nerve roots at their exit points—a location more difficult to decompress completely without destabilizing the spine.
Laminectomy Benefits: Real Functional Improvements
The transformation laminectomy provides extends far beyond numerical success percentages. Patients experience concrete quality of life improvements measurable through daily activity restoration and reduced disability.
Pain reduction achievements:
Leg pain (radiculopathy) improves dramatically in 80-90% of patients within the first month post-surgery. This represents the primary benefit driving surgical decisions—resolving the shooting, burning, or electrical sensations radiating down limbs.
Back pain shows more modest improvement, with only 50-60% experiencing substantial relief. This discrepancy occurs because laminectomy directly addresses nerve compression but doesn’t resolve degenerative disc disease or facet arthritis causing axial back pain.
Walking distance improvements:
Pre-operative walking limitations average 50-150 yards before leg pain forces rest stops. Post-laminectomy, 85% of patients achieve walking distances exceeding 400 yards—often reaching unlimited distances without neurogenic claudication symptoms.
Medication reduction:
Seventy-eight percent of patients decrease or eliminate daily pain medications within 3 months. Opioid dependency particularly decreases, with 65% stopping narcotic use entirely after successful decompression surgery.
What This Means For You: If you can barely walk one block due to leg pain and numbness, successful laminectomy typically restores the ability to walk 20+ blocks comfortably. This functional improvement allows grocery shopping, recreational walking, and travel activities impossible before surgery.
Laminectomy Complications & Risk Management
Despite high success rates, laminectomy carries inherent surgical risks requiring transparent discussion before proceeding. Understanding potential complications allows informed consent and helps patients recognize warning signs requiring immediate medical attention.
Infection risk: 1-3%
Surgical site infections occur in approximately 1.25% of laminectomy cases, lower than spinal fusion procedures. Prophylactic antibiotics administered within 60 minutes before skin incision reduce this risk by 40%. Watch for fever above 101°F, increasing wound redness, drainage, or warmth beyond day 3 post-surgery.
Deep infections involving bone (osteomyelitis) or epidural space require prolonged IV antibiotics and often reoperation for debridement. Superficial skin infections typically respond to oral antibiotics without surgical intervention.
Nerve injury: <1%
Permanent nerve damage occurs rarely despite surgeons working millimeters from spinal cord and nerve roots. Intraoperative neuromonitoring technology tracks nerve function continuously, alerting teams immediately to electrical changes suggesting neural stress. Transient numbness or weakness lasting days to weeks occurs in 3-5% of patients but typically resolves completely.
Cerebrospinal fluid leak: 2-4%
Accidental dural tears happen during tissue dissection, particularly in revision cases with scar tissue. Most surgeons repair tears immediately with sutures and sealants. Small unrecognized leaks manifest as postural headaches—throbbing pain when upright that resolves when lying flat. Treatment involves bed rest, hydration, and occasionally epidural blood patches.
Blood clots (DVT/PE): 1-2%
Deep vein thrombosis develops when immobility allows blood to pool in leg veins. Early mobilization—walking within hours post-surgery—represents the best prevention. Sequential compression devices worn during hospitalization and for 2 weeks home provide additional protection. Patients taking birth control pills or with clotting disorders face elevated risk.
Recurrent stenosis: 18% reoperation rate
Adjacent segment disease requiring reoperation affects 10% of laminectomy patients within 4 years. Degeneration progresses at spinal levels above or below the original surgery site, eventually causing new nerve compression symptoms. This reflects ongoing spinal aging rather than surgical failure.
Laminectomy Risks vs Benefits Decision Analysis
Weighing surgical intervention against continued conservative management requires individualized assessment. Generic population statistics provide starting points, but your specific circumstances determine the appropriateness of proceeding.
Factors favoring surgical intervention:
- Progressive neurological deficits (worsening weakness, foot drop)
- Failed conservative treatment for 12+ weeks (physical therapy, injections, medications)
- Moderate-to-severe stenosis on MRI correlating with symptoms
- Functional disability preventing work, hobbies, or daily activities
- Age under 75 with minimal comorbidities
Factors favoring continued conservative treatment:
- Mild symptoms tolerable with activity modification
- Significant medical comorbidities increasing surgical risk (recent heart attack, uncontrolled diabetes)
- Age over 80 with limited functional demands
- Stenosis severity not matching symptom intensity
- Patient preference to avoid surgery after informed discussion
Quality-Adjusted Life Years analysis:
Medical economic studies calculate that laminectomy provides 2.8 additional quality-adjusted life years compared to continued non-surgical management for moderate-to-severe stenosis. This translates to nearly three extra years of pain-free, fully functional living—substantial benefit justifying the $50,000-$90,000 investment.
Commercial Bridge: Understanding laminectomy benefits and risks requires honest evaluation of your functional limitations and treatment goals. Discuss your specific success probability with board-certified spine surgeons who can assess your imaging, symptoms, and health status to provide personalized outcome predictions.
Laminectomy FAQs & Next Steps: Your Treatment Decision Guide
Frequently Asked Questions About Laminectomy
1. How much does laminectomy cost with insurance in 2026?
Out-of-pocket expenses range from $5,000 to $15,000 after insurance coverage, depending on your deductible, coinsurance percentage, and out-of-pocket maximum. High-deductible health plans require meeting $5,000-$8,000 deductibles before coverage begins, while traditional PPO plans start coverage after $2,500-$4,000 deductibles.
2. What is laminectomy recovery time for elderly patients?
Patients over 65 typically require 8-12 weeks for full recovery compared to 4-6 weeks for younger individuals. Advanced age doesn’t preclude excellent outcomes—biological health status matters more than chronological age when predicting laminectomy healing time.
3. Is laminectomy worth it for spinal stenosis?
The 90% success rate and 2.8 additional quality-adjusted life years gained make laminectomy highly worthwhile for moderate-to-severe stenosis after failed conservative treatment. Patients regain walking ability, reduce medication dependence, and restore quality of life activities impossible before surgery.
4. Laminectomy vs fusion: which costs more?
Spinal fusion adds $25,000-$35,000 to the base laminectomy cost due to instrumentation, bone graft materials, and extended operative time. Total fusion procedures range from $80,000-$120,000 compared to $50,000-$65,000 for standalone decompression.
5. When is minimally invasive laminectomy an option?
Single-level or two-level stenosis without spondylolisthesis or spinal instability qualifies for minimally invasive approaches. Patients experience 40% faster recovery and same-day discharge in 65% of cases.
6. What is lumbar stenosis treatment success without surgery?
Conservative management improves symptoms in only 30-40% of patients with moderate-to-severe stenosis, compared to 90% surgical success rates. Physical therapy, epidural injections, and medications provide temporary relief but don’t address the underlying nerve compression.
7. Can laminectomy pain relief be permanent?
Seventy-one percent maintain improvement at 5+ years, though 18% require revision surgery for adjacent segment stenosis. The procedure provides long-lasting benefits for most patients, with reoperation risk lower than many assume.
8. Does Medicare cover decompression surgery?
Medicare Part B covers medically necessary laminectomy at 80% of approved amounts after meeting the annual deductible. Beneficiaries pay 20% coinsurance, with supplemental policies often covering the remaining balance.
Am I a Candidate for Laminectomy?
Self-Assessment Checklist:
- Leg pain worse than back pain lasting 12+ weeks
- Walking limited to less than 2-3 blocks before pain forces stopping
- Bending forward temporarily relieves symptoms (shopping cart sign)
- Failed conservative treatments: physical therapy, injections, medications
- MRI confirms moderate-to-severe spinal stenosis matching symptoms
- No severe medical conditions precluding anesthesia
- Age under 80 with reasonable functional demands
Red flag symptoms requiring urgent evaluation:
- Progressive leg weakness or foot drop developing over days
- New bowel or bladder incontinence (cauda equina syndrome)
- Severe pain unrelieved by any position or medication
- Numbness in groin/inner thigh (saddle anesthesia)
Conservative treatment trial requirements:
Most insurance companies mandate 12 weeks of documented conservative care before approving surgery. Optimizing your overall health during this period improves surgical outcomes if conservative measures fail.
How to Choose a Laminectomy Surgeon
Surgeon selection dramatically impacts outcomes, with high-volume specialists demonstrating superior results and lower complication rates. Board certification represents the minimum qualification—additional factors separate excellent from average surgeons.
Critical surgeon qualifications:
- Board certification in neurosurgery or orthopedic surgery with spine fellowship
- Minimum 50 laminectomy procedures annually
- Privileges at accredited hospitals with dedicated spine services
- Transparent outcome data including complication and reoperation rates
- Expertise in both open and minimally invasive techniques
Surgeon volume correlates directly with patient outcomes—those performing 100+ spine surgeries annually demonstrate 30% lower complication rates than low-volume surgeons. Don’t hesitate to ask about procedure volume during consultations.
Hospital quality indicators:
- Level 1 or 2 trauma center designation
- Joint Commission accreditation for spine programs
- 24/7 neurosurgical coverage for emergency complications
- Dedicated spine physical therapy programs
- Infection rates below national benchmarks (under 2%)
Questions to Ask Your Surgeon
Pre-operative discussion essentials:
- How many laminectomy procedures do you perform annually?
- What is your personal complication rate for this surgery?
- What percentage of your patients achieve pain relief?
- Am I a candidate for minimally invasive techniques?
- Will I need fusion in addition to decompression?
- What alternative treatments exist for my condition?
- What happens if I delay surgery 3-6 months?
- How long is your typical recovery timeline?
- What percentage of patients return to work full-time?
- What are the signs of complications requiring immediate attention?
Second opinion importance:
Thirty percent of patients change treatment plans after obtaining second opinions. Complex cases involving multi-level stenosis, spondylolisthesis, or prior failed surgery particularly benefit from multiple expert evaluations.
Commercial Bridge: Document your symptoms using our comprehensive tracking tools before your consultation to ensure accurate symptom reporting. Prepare a list of all medications, previous treatments attempted, and specific functional limitations to maximize appointment productivity.
Explore additional health resources and evidence-based guides covering surgical procedures, recovery optimization, and wellness strategies tailored to spine health management.
MEDICAL DISCLAIMER: This article provides educational information about laminectomy surgery and should not replace personalized medical advice from qualified healthcare providers. Always consult board-certified spine surgeons for individualized treatment recommendations based on your specific medical history, imaging findings, and functional limitations. Surgical decisions require comprehensive evaluation including physical examination, diagnostic imaging review, and discussion of risks, benefits, and alternatives specific to your condition.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.