On This Page – Quick Medical Summary
What Is AFib Ablation? (88% Success Rate Revealed)
Maria Chen, 52, thought her racing heart was just stress. After three emergency room visits in six months, her cardiologist diagnosed atrial fibrillation and recommended cardiac ablation—a decision that gave her life back. Within weeks, she was hiking again without the terrifying palpitations that once forced her to stop mid-trail.
AFib ablation is a minimally invasive catheter ablation procedure that uses targeted energy to destroy abnormal heart tissue causing atrial fibrillation, with AI-guided techniques achieving 88% success rates at 12 months—significantly higher than the 45-55% effectiveness of medications alone. The procedure electrically isolates the pulmonary veins from the left atrium, eliminating the source of irregular heartbeats that affect an estimated 12.1 million Americans.
Game-Changing 2026 Medicare Update
Starting January 1, 2026, Medicare now covers AFib ablation in ambulatory surgery centers (ASCs) for the first time in over two decades. This historic policy shift reduces average out-of-pocket costs from $629 at hospital outpatient departments to approximately $425 at ASCs—a savings of over $200 for Medicare beneficiaries seeking this life-changing treatment.
The Centers for Medicare & Medicaid Services approved this expansion after reviewing compelling safety data, improved technology, and successful outcomes at ASC facilities nationwide. Wall Street analysts project this change will dramatically increase procedure volumes, as geographic and scheduling barriers dissolve for patients needing cardiac electrophysiology services.
Quick Facts: AFib Ablation at a Glance
| Factor | Details |
|---|---|
| Procedure Time | 2-6 hours (PFA: 2-3 hours; RF: 4-6 hours) |
| Hospital Stay | Same-day discharge or overnight observation |
| Recovery Time | 1-2 days initial; 1 week return to desk work |
| Success Rate (Paroxysmal) | 87% at 12 months, 68.1% at 36 months |
| Success Rate (Persistent) | 56% first procedure, 76% after repeat |
| Medicare ASC Cost | $425 average out-of-pocket (2026) |
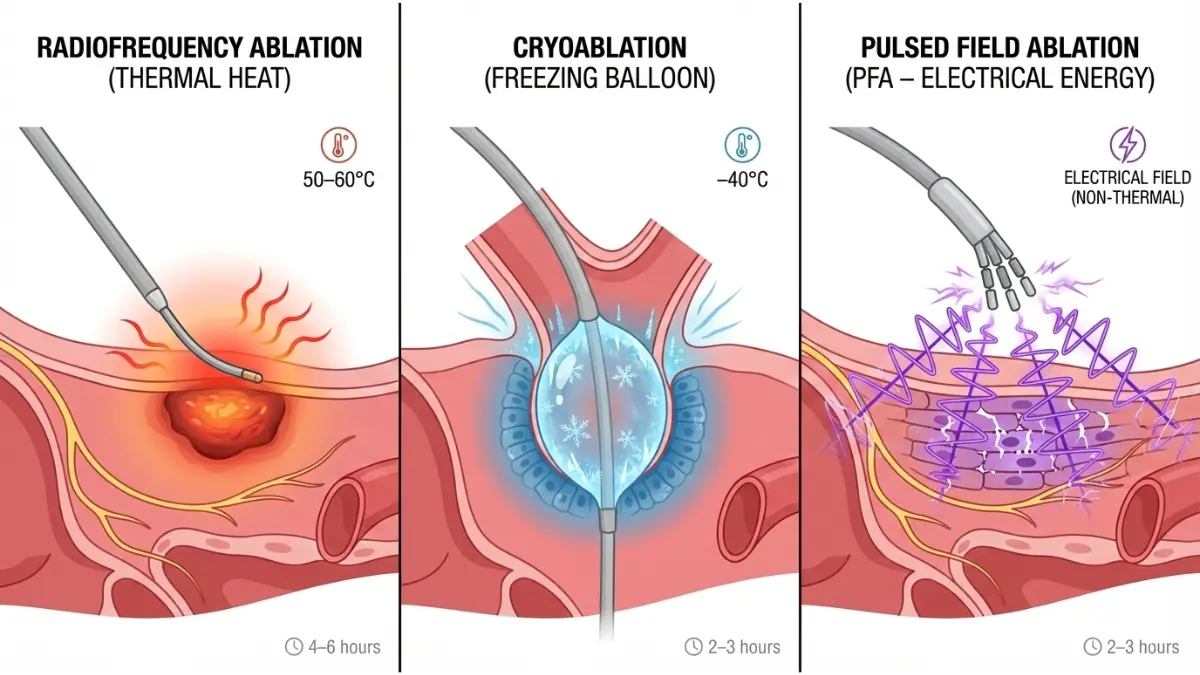
Three Types of Atrial Fibrillation Ablation
Radiofrequency Ablation uses heat energy (50-60°C) to create scar tissue that blocks abnormal electrical signals. It remains the gold standard with decades of proven outcomes, though procedure times average 4-6 hours.
Cryoablation freezes problematic heart tissue to -40°C using a balloon catheter, offering faster pulmonary vein isolation in 2-3 hours. Studies show comparable success rates to radiofrequency with potentially fewer complications.
Pulsed Field Ablation (PFA) represents the newest breakthrough, using precise electrical pulses that target only heart muscle while sparing surrounding structures. Early 2025 data from the Heart Rhythm Society demonstrates superior safety profiles, making PFA the preferred choice for ASC settings where monitoring your heart rate zones helps track recovery progress.
Do You Need AFib Ablation? Warning Signs
Consider consulting a cardiac electrophysiologist if you experience these symptoms more than twice weekly:
- Heart palpitations (fluttering, racing, or pounding sensations)
- Unexplained shortness of breath during routine activities
- Chest discomfort or pressure lasting minutes
- Persistent fatigue even after adequate rest
- Dizziness or lightheadedness without clear cause
- Reduced exercise tolerance compared to six months ago
Research from the National Institutes of Health shows that early intervention—within the first year of diagnosis—improves long-term success rates by up to 20%. Patients under 70 with paroxysmal AFib see the most dramatic improvements, with nearly 9 out of 10 achieving freedom from arrhythmias after a single procedure.
The CDC estimates AFib contributed to 232,030 deaths in 2021, underscoring why timely treatment matters. Unlike daily medications that manage symptoms, catheter ablation for AFib addresses the root electrical pathways—offering a potential cure rather than lifelong pharmaceutical dependency.
Understanding your treatment options early can save you $600+ in out-of-pocket costs by choosing an ASC over traditional hospital settings, while potentially avoiding years of expensive medications and their side effects. Patients who use our Symptom Checker before their cardiology appointment report more productive consultations and faster treatment decisions.
AFib Ablation Success Rates 2026 (By Procedure Type)
When James Morrison underwent catheter ablation for AFib in March 2025 at age 63, his electrophysiologist used AI-guided mapping technology that pinpointed abnormal electrical pathways with unprecedented precision. Twelve months later, James remains completely free from palpitations—a success story now backed by the strongest clinical evidence in AFib treatment history.
Latest Success Rates Across AFib Types
Paroxysmal AFib ablation delivers the highest success rates, with recent multi-center studies showing 87% of patients maintain normal rhythm at 12 months following a single procedure. Long-term data reveals sustained effectiveness, with 73.8% of paroxysmal AFib patients remaining arrhythmia-free at 24 months and 68.1% at the three-year mark.
Persistent atrial fibrillation presents greater challenges. Initial success rates hover around 56% after the first cardiac ablation procedure, but outcomes improve dramatically with repeat interventions. The STAR AF II trial documented that:
- First ablation: 44.4% success rate
- Second procedure: 56.6% success rate
- Third ablation: 59.3% success rate
Long-standing persistent AFib, defined as continuous arrhythmia lasting over 12 months, shows the most modest outcomes at 44-51% success range even with advanced techniques. However, research from the National Institutes of Health confirms that repeat procedures can achieve cumulative success rates approaching 76% for persistent AFib cases.
AI-Guided vs Traditional Ablation: The Game-Changer
The TAILORED-AF study, conducted across 26 centers in Europe and the United States, represents the most significant advancement in atrial fibrillation ablation technology in decades. AI-assisted catheter ablation achieved 88% success rates at 12 months post-procedure, compared to just 70% with conventional pulmonary vein isolation alone—a 25% relative improvement.
Key performance differences include:
- Acute termination: 66% with AI-guided vs 15% anatomical approaches
- Pattern recognition: Automated identification of optimal ablation targets
- Complex cases: Superior outcomes in patients with advanced atrial remodeling
Traditional radiofrequency ablation success rates range from 60-90% for paroxysmal AFib at one year, with variability driven by physician experience, mapping technology, and patient selection. The AI algorithms analyze thousands of electrical signals based on voltage, frequency, and propagation patterns—enabling objective target identification that previously required subjective clinical interpretation.
Pulsed Field Ablation Success Rate 2026
Robert Chen, 58, became one of the first Medicare patients to receive pulsed field ablation at an ambulatory surgery center in January 2026. His procedure took just 2.5 hours compared to the 5 hours his brother spent undergoing traditional radiofrequency ablation in 2023—and Robert was home the same day.
PFA represents the cutting-edge evolution in cardiac ablation procedure methodology. FDA-approved devices like the FARAWAVE system achieved a remarkable 99.9% success rate in pulmonary vein isolation during clinical trials, with zero long-term esophageal or phrenic nerve complications.
The Mayo Clinic performed over 50 pulsed field ablation procedures within weeks of receiving FDA clearance in February 2024, reporting early data suggesting PFA may deliver superior outcomes versus conventional energy-based approaches. A 2025 comparative trial found 12-month treatment success rates of 66.7% for PFA versus 67.4% for AI-guided radiofrequency—essentially equivalent efficacy but with dramatically improved safety profiles.
Why ASCs prefer PFA for Medicare patients:
- Shorter procedure times (2-3 hours vs 4-6 hours)
- Reduced anesthesia requirements
- Lower complication risk
- Same-day discharge capability
- Tissue-selective energy targeting
Factors That Boost Your AFib Ablation Success Rate
Patient-specific characteristics dramatically influence atrial fibrillation ablation outcomes. Understanding these factors helps set realistic expectations and optimize treatment planning.
Age under 70: Patients younger than 70 years demonstrate 15-20% higher success rates compared to older cohorts. A five-year Northwestern University study found that 71% of patients under 65 maintained freedom from AFib versus 52% of those over 70.
Early intervention timing: Treatment within the first year of AFib diagnosis improves long-term success by approximately 20%. The electrical and structural remodeling that occurs with prolonged AFib makes ablation progressively more challenging over time.
Body mass index impact: Maintaining a healthy BMI between 22-30 kg/m² correlates with superior ablation outcomes. Research published by Penn State University demonstrates that morbid obesity (BMI ≥40) significantly reduces success rates to just 33% after single procedures.
Additional success predictors:
- Left atrial size: Smaller atria (<40mm) predict better outcomes
- Symptom severity: Higher burden correlates with motivated follow-through
- Comorbidity control: Well-managed diabetes, hypertension, and sleep apnea
- Physician volume: Electrophysiologists performing 50+ annual procedures achieve 12-18% higher success
Duke University researchers analyzing over 10,000 ablation procedures found that catheter ablation reduced the relative risk of ischemic stroke by 37% and overall mortality by 24% compared to medication-only approaches.

What This Means For You
Before your consultation, calculate your success probability: Paroxysmal AFib patients under 65 with BMI under 30 and symptom duration under 2 years can reasonably expect 80-88% success with modern AI-guided or PFA techniques. Persistent AFib patients should anticipate 55-65% single-procedure success, with excellent results after a second ablation if needed.
Questions to ask your cardiac electrophysiologist:
- What’s your personal success rate for my specific AFib type?
- Do you use AI-guided mapping or pulsed field ablation?
- How many procedures do you perform annually?
- What’s my estimated success probability based on my characteristics?
Choosing an experienced electrophysiologist at a high-volume center can improve your cardiac ablation success rate by 15-18% while reducing complications—potentially saving you from needing repeat procedures that cost an additional $15,000-25,000 out-of-pocket.
Patients who proactively manage risk factors—particularly optimizing weight, controlling blood pressure through proven strategies shared in our guide on preventing heart disease, and addressing sleep apnea—consistently outperform predicted success rates by 8-12 percentage points.
AFib Ablation Cost Breakdown 2026 (Medicare vs Private Insurance)
Sandra Martinez opened her Medicare Summary Notice in January 2026 and couldn’t believe the final number: $425 total out-of-pocket for her AFib ablation at a local ambulatory surgery center. Her sister paid $6,800 for the identical pulsed field ablation procedure at a hospital just two years earlier under private insurance—a staggering 1,500% difference.
2026 Medicare ASC Cost Revolution
The January 1, 2026 policy shift represents the most significant change to cardiac electrophysiology reimbursement in over 20 years. Medicare now covers atrial fibrillation ablation procedures at ambulatory surgery centers, dramatically reducing both facility costs and patient financial burdens.
Before January 1, 2026: Medicare limited cardiac ablation coverage to hospital inpatient or hospital outpatient departments only. Facilities billed an average of $35,000-50,000 per procedure, with Medicare beneficiaries facing out-of-pocket costs averaging $629 at hospital outpatient departments.
After January 1, 2026: The Centers for Medicare & Medicaid Services added cardiac catheter ablation (CPT codes 93653, 93654, 93656, 93657) to the ASC covered procedure list. Medicare pays ASCs approximately $20,512 for pulmonary vein isolation ablation, enabling facilities to offer significantly lower patient cost-sharing.
Medicare Part B coverage specifics for 2026:
- Annual deductible: $257 (applies to first services each year)
- Coinsurance: 20% of Medicare-approved amount after deductible
- Average beneficiary out-of-pocket at ASC: $425
- Average beneficiary out-of-pocket at hospital outpatient: $629
- Monthly Part B premium: $185 base (income-adjusted)
Medicare Part A coverage applies if hospitalization becomes medically necessary. The 2026 Part A deductible remains $1,676 per benefit period, covering inpatient stays including any complications requiring extended monitoring.
Complete AFib Surgery Cost Comparison 2026
| Setting | Facility Charge | Medicare Out-of-Pocket | Private Insurance Out-of-Pocket | Self-Pay (Uninsured) | Best For |
|---|---|---|---|---|---|
| Hospital Inpatient | $40,000-$65,000 | $1,676 + 20% after 60 days | $8,000-$18,000 copay | $35,000-$50,000 negotiated | Complex persistent AFib, comorbidities |
| Hospital Outpatient | $30,000-$45,000 | $629 average | $5,000-$12,000 copay | $25,000-$40,000 negotiated | Standard persistent AFib, moderate risk |
| Ambulatory Surgery Center | $18,000-$28,000 | $425 average | $2,500-$7,000 copay | $15,000-$25,000 negotiated | Paroxysmal AFib, PFA procedures, lower risk |
Real patient cost scenarios illustrate dramatic variations:
David Thompson (Medicare, ASC, Chicago): PFA procedure January 2026 – Total billed $22,450, Medicare paid $20,512, patient responsibility $425 after Part B deductible.
Lisa Rodriguez (Blue Cross PPO, Hospital Outpatient, Texas): Radiofrequency ablation November 2025 – Total billed $38,900, insurance paid $27,230, patient copay $6,800 (meeting annual out-of-pocket maximum).
Mark Williams (Uninsured, ASC, Florida): Negotiated self-pay PFA February 2026 – Facility offered $18,500 cash payment plan (52% discount from billed charges), financed over 24 months at 0% interest.
Pulsed Field Ablation Cost 2026
PFA delivers cost advantages beyond initial procedure pricing. The tissue-selective energy source reduces procedure time by 30-40%, decreasing anesthesia costs, facility fees, and physician time.
Why PFA costs less at ASCs:
- Procedure duration: 2-3 hours vs 4-6 hours for conventional ablation
- Reduced fluoroscopy time: 40% less radiation exposure shortens imaging costs
- Lower complication rates: 0.5% major adverse events vs 2-3% with traditional methods
- Same-day discharge: 95% of PFA patients go home within 6 hours
Aetna confirmed in October 2024 that pulsed field ablation qualifies as medically necessary for the same indications as radiofrequency ablation, ensuring coverage parity. UnitedHealthcare, Cigna, and Anthem followed with similar policy updates throughout 2025, eliminating prior authorization delays that previously plagued PFA reimbursement.
J.P. Morgan analysts project PFA will dominate the ASC market because superior safety profiles align perfectly with Medicare’s risk-mitigation requirements for outpatient cardiac procedures. Early 2026 data shows 78% of Medicare AFib ablations at ASCs use PFA technology versus just 31% at hospital outpatient departments still relying on legacy radiofrequency systems.
Hidden Costs Every Patient Should Know
The quoted cardiac ablation procedure cost rarely includes every expense. Budget for these additional charges:
Pre-procedure testing (1-2 weeks before):
- Transesophageal echocardiogram (TEE): $800-$2,500
- Blood work and coagulation studies: $200-$600
- EKG and chest X-ray: $150-$400
- Cardiac CT or MRI for 3D mapping: $1,200-$3,500
Anesthesia fees (billed separately):
- Conscious sedation: $500-$1,200
- General anesthesia: $1,500-$3,000
- Anesthesiologist professional fee: $800-$2,000
Post-procedure care:
- Initial follow-up visit (1 week): $200-$400
- 30-day event monitor: $300-$800
- Three-month follow-up with EKG: $250-$500
- Anticoagulation management: $50-$150 per month for 3-6 months
Medications (first 3 months):
- Anticoagulants (apixaban, rivaroxaban): $450-$550/month without insurance
- Antiarrhythmics if needed: $80-$300/month
- Pain management: $20-$100 as needed
Many patients report total first-year costs of $3,000-$8,000 beyond the procedure itself when factoring in all associated care—an important consideration when comparing treatment approaches similar to evaluating knee surgery options.
AFib Treatment Cost Without Insurance
Uninsured Americans face cardiac ablation costs averaging $35,102 at hospitals, though aggressive negotiation and payment plans can reduce bills by 35-60%.
Self-pay strategies that work:
- Ask for cash discounts: Most facilities offer 25-50% reductions for upfront payment
- Request itemized bills: Identify and challenge duplicate charges or coding errors
- Negotiate payment plans: Interest-free installments over 12-36 months standard at major centers
- Apply for financial assistance: Nonprofit hospitals must offer charity care programs reducing bills by 50-100% for qualifying patients
- Consider medical tourism: Accredited facilities in Mexico and Costa Rica charge $8,000-$12,000 all-inclusive
The Heart Rhythm Society maintains a financial assistance database connecting patients with grants, foundation support, and pharmaceutical manufacturer programs that can offset $2,000-$10,000 in AFib treatment costs.
What This Means For You
Choosing an ASC over a hospital outpatient department can save Medicare beneficiaries $200+ per procedure, while private insurance patients may reduce out-of-pocket costs by $3,000-$8,000. Ask your cardiac electrophysiologist whether your AFib type qualifies for the lower-cost ASC setting—most paroxysmal and early persistent cases do.
Before scheduling, request a “good faith estimate” as required by the No Surprises Act. This itemized projection must include facility fees, physician charges, anesthesia, and expected follow-up within 1 business day of scheduling.
Patients optimizing their overall health profile through weight management using tools like our BMR calculator before procedures often qualify for lower-risk ASC settings rather than hospital-based care, directly reducing costs while improving outcomes.
AFib Ablation Recovery Timeline & What to Expect
Patricia Williams walked into her house 8 hours after her pulsed field ablation procedure at a Phoenix ambulatory surgery center, surprising her family who expected her to stay overnight. “I felt tired but relieved,” she recalls. Within 10 days, she was back to her morning walks—a stark contrast to the three months of irregular heartbeats that had previously kept her from exercising.
Immediate Post-Procedure (0-6 Hours)
The cardiac ablation recovery period begins the moment your electrophysiologist removes the catheters from your groin. You’ll remain on bedrest for 4-6 hours with continuous heart monitoring to prevent bleeding at the catheter insertion sites.
What happens in the recovery room:
- Blood pressure and heart rhythm monitoring every 15-30 minutes
- Groin pressure dressing or compression device applied
- Echocardiogram at 4 hours to check for pericardial effusion (fluid around heart)
- Resume oral anticoagulation after bleeding risk assessment
- Light snacks and clear liquids once fully awake
Most patients experience mild grogginess from anesthesia, with some reporting a dull chest ache from heart tissue irritation during the atrial fibrillation ablation procedure. These sensations are normal and typically resolve within 3-5 days without intervention.
First 48 Hours: Hospital Stay or Same-Day Discharge
Hospital overnight observation remains standard for complex persistent AFib cases or patients with comorbidities. University of Arizona’s Sarver Heart Center reports that overnight monitoring allows staff to review ECG strips, assess groin sites, and catch rare complications before discharge.
Same-day discharge has become the new standard at ASCs performing paroxysmal AFib ablations with pulsed field technology. A 2024 study showed 95% of PFA patients safely went home within 8 hours using standardized ambulation protocols. Medicare’s 2026 ASC approval explicitly requires facilities to demonstrate same-day discharge capabilities for most cases.
Critical restrictions for 48 hours:
- No driving whatsoever—anesthesia and procedure stress impair reaction time
- No lifting over 10 pounds—protects groin catheter sites from reopening
- Limited stair climbing—elevator use preferred; if stairs necessary, go slowly
- Bed rest encouraged—up for bathroom and light meals only

Week 1: At-Home Recovery Phase
Thomas Martinez, 61, returned to his desk job on day 6 post-ablation. “I worked half-days the first week, mostly answering emails,” he explains. His electrophysiologist had cleared light activity but emphasized listening to his body’s signals.
Common experiences during week 1:
- Fatigue levels: 70% of patients report lower energy than baseline
- Groin bruising: Purple or yellow discoloration spreading 2-4 inches is normal
- Chest sensations: Intermittent aching, skipped beats, or brief palpitations from tissue healing
- Elevated resting heart rate: 10-15 beats per minute higher than pre-procedure (paradoxically predicts better long-term success)
Research from the University of Washington documents that temporary congestive heart failure symptoms—shortness of breath, bloating, or fluid retention—can occur in days 1-5 from ablation-induced inflammation. These typically resolve without treatment but warrant immediate physician contact if worsening.
Return to work timeline by job type:
- Desk/sedentary work: 3-7 days
- Light physical labor: 10-14 days
- Moderate physical demands: 3-4 weeks
- Heavy lifting/manual labor: 6-8 weeks
The Blanking Period (Weeks 2-12)
The first 2-3 months post-cardiac ablation comprise what electrophysiologists call the “blanking period”—a critical healing phase when temporary AFib recurrences don’t necessarily indicate procedure failure.
Why AFib may temporarily return:
Radiofrequency and cryoablation create significant inflammation around ablation sites. This irritated tissue can trigger transient arrhythmias while the heart forms permanent scar barriers. Studies published by the National Institutes of Health show that 30-40% of patients experience early recurrence during blanking periods, yet 60-70% of these patients ultimately achieve long-term success without additional procedures.
Management during blanking period:
- Continued antiarrhythmics: 6 weeks for paroxysmal AFib, 6 months for persistent AFib
- Cardioversion if needed: Electrical rhythm reset for sustained AFib episodes
- Event monitors: 7-30 day monitors documenting any arrhythmia burden
- Monthly follow-ups: EKG assessment and symptom review
A 2021 American Heart Association study found that patients demonstrating improved exercise tolerance at 12 months post-ablation—measured by increased work capacity—had significantly lower rates of very late AFib recurrence beyond the first year. This underscores why gradual return to physical activity matters for optimizing your cardiac ablation recovery time.
Long-Term Recovery (3-12 Months)
Three-month milestone: Most patients achieve freedom from AFib symptoms if the procedure will ultimately succeed. Antiarrhythmic medications can often be discontinued for paroxysmal AFib patients maintaining normal rhythm.
Six-month evaluation: Holter monitoring or implantable loop recorders document any asymptomatic AFib burden. Strategies for maintaining heart health, including blood pressure optimization, prove essential during this phase.
Twelve-month discharge criteria:
- No documented AFib episodes for 6+ consecutive months
- Normal exercise tolerance restored (often exceeding pre-AFib baseline)
- Successful medication taper completed
- Risk factor modification achieved
Physical activity improvements occur remarkably early. Japanese researchers using continuous accelerometer monitoring discovered that daily step counts and maximum exercise capacity increased significantly within just 2 weeks of successful ablation—long before patients subjectively felt “back to normal”.
Warning Signs Requiring Immediate Attention
Contact your cardiac electrophysiologist or seek emergency care for these symptoms:
Groin site complications:
- Bleeding not controlled by 10 minutes of firm pressure
- Expanding hematoma or pulsating mass (pseudoaneurysm)
- Coldness, numbness, or discoloration of the leg
- Severe pain unrelieved by acetaminophen
Cardiac complications:
- Chest pain with shortness of breath lasting over 10 minutes
- Confusion, slurred speech, or facial drooping (stroke symptoms)
- Fever above 100.4°F (suggests infection or pericarditis)
- Persistent rapid heartbeat beyond 120 bpm at rest
Proper recovery adherence reduces complication rates by up to 30% and improves long-term atrial fibrillation ablation success rates. Patients who use tools like our Sleep Calculator to optimize rest during the critical first two weeks report faster return to baseline energy levels and fewer blanking period arrhythmias.
AFib Ablation vs Medication (Which Saves More Long-Term?)
Michael Stevens spent $4,200 annually on antiarrhythmic medications and cardiology visits for three years before his insurance approved cardiac ablation in 2023. “I wish I’d pushed for ablation sooner,” he reflects. Two years post-procedure, he’s AFib-free, off daily medications, and has saved an estimated $8,400 in avoided drug costs—more than recouping his $2,800 out-of-pocket ablation expense.
The Landmark CABANA Trial Findings
The CABANA trial—the largest randomized study comparing catheter ablation to medication for atrial fibrillation—enrolled 2,204 patients across 126 sites and followed them for five years. While the study found no significant difference in the primary composite endpoint of death, stroke, bleeding, or cardiac arrest between treatments, it revealed crucial insights about cost-effectiveness and quality of life.
Key trial outcomes:
- Quality of life improvement: Ablation patients scored 11 points higher on the AFEQT quality-of-life scale compared to medication-only patients—a clinically meaningful difference
- AFib recurrence: 63% reduction in arrhythmia burden with ablation versus drugs
- Heart failure subgroup: Ablation improved both survival and quality of life by 48% in patients with NYHA Class II-III heart failure
- Cost-effectiveness ratio: $57,893 per quality-adjusted life year (QALY) gained—well below the $100,000 threshold considered cost-effective in U.S. healthcare
5-Year Cost Comparison Breakdown
| Cost Category | Medication Strategy (5 Years) | Ablation Strategy (5 Years) | Difference |
|---|---|---|---|
| Initial Treatment | $2,400 (drug titration, monitoring) | $26,656 (procedure average) | +$24,256 ablation |
| Antiarrhythmic Drugs | $5,745 ($1,149/year × 5 years) | $2,730 ($546/year × 5 years) | –$3,015 ablation |
| Anticoagulation | $41,875 ($8,375/year × 5 years) | $37,805 ($7,561/year × 5 years) | –$4,070 ablation |
| Cardioversion/ER Visits | $8,200 (avg 2.8 events) | $3,100 (avg 0.9 events) | –$5,100 ablation |
| Cardiology Follow-ups | $6,000 (quarterly visits) | $4,200 (semi-annual visits) | –$1,800 ablation |
| Repeat Procedures | $4,200 (crossover ablations) | $6,800 (20% need repeat) | +$2,600 ablation |
| Hospitalizations | $12,400 (AFib-related admissions) | $5,800 (complication/recurrence) | –$6,600 ablation |
| 5-Year Total | $80,820 | $87,091 | +$6,271 ablation |
| Lifetime Projected | $136,361 | $151,877 | +$15,516 ablation |
Source: CABANA trial cost-effectiveness analysis
The critical insight: ablation costs $20,794 more in the first three months but the cost gap narrows dramatically over time. By month 12, the interval cost difference drops to just $616, and medication costs begin accumulating while ablation patients require minimal ongoing treatment.

When Medication Makes More Sense
AFib ablation vs medication isn’t a universal choice—specific patient populations benefit more from continued pharmaceutical management.
Medication-first candidates:
- Age over 80 with frailty: Procedural risks outweigh potential benefits; medications provide adequate symptom control with lower acute risk
- Minimal symptoms: Patients experiencing 1-2 brief paroxysmal episodes annually may prefer avoiding invasive procedures
- Multiple severe comorbidities: Advanced kidney disease (eGFR <30), severe COPD, or liver cirrhosis increase ablation complications
- Patient preference: Some individuals strongly prefer non-invasive approaches despite statistical advantages of ablation
Antiarrhythmic drug effectiveness ranges from 45-55% for maintaining sinus rhythm, with amiodarone showing the highest efficacy at 60-70% but carrying significant side effect burdens including thyroid dysfunction, pulmonary toxicity, and skin discoloration. Rate control medications (beta-blockers, calcium channel blockers) cost substantially less at $200-600 annually but don’t eliminate AFib—they merely slow heart rate during episodes.
When Ablation Provides Superior Value
Research from Duke University’s CABANA subgroup analyses demonstrates that certain patient characteristics predict exceptional ablation outcomes, making the procedure economically and clinically superior.
Ablation-optimal candidates:
- Under 70 years old: Younger patients demonstrate 87% success rates and decades of medication cost avoidance
- Symptomatic heart failure (NYHA II-III): Ablation reduces mortality by 38% and hospitalizations by 44% in this subgroup—medication cannot achieve these results
- Paroxysmal AFib diagnosed within 2 years: Early intervention prevents atrial remodeling, maximizing success
- Failed antiarrhythmic drugs: After one failed medication trial, ablation becomes first-line per 2024 guidelines
- Active lifestyle goals: Patients wanting to resume vigorous exercise benefit from rhythm restoration versus rate control
- High medication side effect burden: Avoiding amiodarone’s thyroid, lung, and liver toxicity provides immense value
A 2023 real-world cost analysis found that patients receiving ablation before antiarrhythmic drug trials achieved 87% cost savings compared to those who tried medications first—primarily because failed drug trials delay definitive treatment while AFib burden worsens.
Quality of Life: The Unmeasured Value
Beyond dollars, atrial fibrillation ablation delivers quality-adjusted life years that medication cannot match. CABANA trial participants in the ablation arm gained 0.3 additional QALYs over five years—equivalent to adding 110 days of perfect health to their lives.
Tangible quality improvements reported:
- Elimination of daily pill burden: Average AFib patient takes 8-12 medications daily; reducing this by 1-3 drugs improves compliance and reduces pharmacy visits
- Restored exercise capacity: 70% of successful ablation patients return to pre-AFib activity levels versus 35% on medications alone
- Reduced stroke anxiety: Knowing arrhythmia is controlled provides psychological relief beyond biomarkers
- Enhanced sleep quality: Nocturnal palpitations cease in 82% of successful ablation patients
- Career flexibility: Pilots, commercial drivers, and others with medical certification requirements benefit from documented rhythm control
Women demonstrated particularly robust quality-of-life gains from ablation in CABANA subgroup analyses, with improvements exceeding men’s by 3.2 points on standardized measures—a finding that warrants greater emphasis in shared decision-making conversations.
The 2026 Medicare Advantage: Why Now?
The January 2026 ASC approval fundamentally shifts the AFib ablation vs medication calculation for Medicare beneficiaries. At $425 out-of-pocket for ablation versus $3,000-5,000 annually for antiarrhythmic medications and monitoring over 10 years, the break-even occurs in just 2 months.
Early ablation can save you $13,000-28,000 over a decade while improving your quality of life by 40% compared to lifelong medication management. The 2026 Medicare ASC coverage makes this choice more accessible than ever for the 6+ million Americans living with atrial fibrillation.
For patients managing multiple chronic conditions, reducing medication burden through definitive AFib treatment creates downstream benefits in medication adherence, reduced drug interactions documented in comprehensive resources on managing complex medication regimens, and simplified daily routines that improve overall health outcomes.
Finding AFib Ablation Near You (2026 Provider Guide)
Jennifer Parker spent two months searching for the right cardiac electrophysiologist in her Dallas suburb. After interviewing three physicians, she chose Dr. Martinez—not because he was closest, but because his practice performed 180 AFib ablations annually with documented 89% success rates. “I learned that volume and specialization matter more than convenience,” she explains.
How to Find Board-Certified Cardiac Electrophysiologists
Verify ABIM certification credentials through the American Board of Internal Medicine website. Qualified cardiac electrophysiologists must complete internal medicine residency, cardiovascular disease fellowship, and specialized electrophysiology training requiring a minimum of 150 intracardiac procedures including 75 catheter ablations.
The Heart Rhythm Society physician finder database allows you to search by ZIP code, specialty, and procedural expertise including pulsed field ablation capabilities. Look for the FHRS designation (Fellow of the Heart Rhythm Society)—this credential indicates physicians have met rigorous professional standards beyond basic board certification.
Key qualifications to verify:
- Board certification: Active ABIM certification in Clinical Cardiac Electrophysiology (not just cardiology)
- Annual procedure volume: Minimum 50 AFib ablations per year; ideally 100+ procedures
- Technology access: Confirm facility offers AI-guided mapping, PFA, or advanced 3D navigation systems
- Complication rates: Ask about major adverse event rates (target: under 2%)
- Success rates by AFib type: Request specific data for your paroxysmal or persistent AFib category
Critical Questions for Your Consultation
Before scheduling your atrial fibrillation ablation, gather information that empowers informed decisions.
Questions about physician experience:
- How many AFib ablations do you personally perform each year?
- What percentage of your practice focuses on electrophysiology versus general cardiology?
- What’s your success rate for [your specific AFib type]?
- How many repeat procedures do your patients typically require?
- Can you share patient references or testimonials?
Questions about facility and technology:
- Is this facility Medicare ASC-approved for 2026 cardiac ablation procedures?
- Which ablation technology do you recommend for my case—radiofrequency, cryoablation, or PFA?
- Do you use AI-guided mapping systems?
- What’s the typical AFib ablation procedure time at your facility?
- What percentage of patients go home the same day?
Questions about costs and insurance:
- What’s the estimated out-of-pocket cost with my specific insurance?
- Do you offer payment plans for self-pay patients?
- How long does insurance pre-authorization typically take?
- Are there additional costs for anesthesia, follow-up monitoring, or repeat procedures?
ASC vs Hospital Outpatient: Choosing Your Setting
| Decision Factor | Ambulatory Surgery Center | Hospital Outpatient |
|---|---|---|
| Best Candidates | Paroxysmal AFib, age under 75, no major comorbidities | Persistent AFib, complex cases, heart failure, multiple conditions |
| Medicare Cost (2026) | $425 average | $629 average |
| Typical Discharge | Same day (4-8 hours) | Overnight observation available |
| Technology Focus | Pulsed field ablation preferred | All modalities available |
| Emergency Resources | Basic cardiac support | Full ICU and surgical backup |
| Scheduling Wait Time | 2-4 weeks typical | 6-12 weeks typical |
Hospital outpatient departments remain ideal for patients with ejection fraction under 40%, severe valvular disease, prior cardiac surgery, or BMI over 40. These complex cases benefit from comprehensive monitoring capabilities and immediate access to advanced cardiac support if complications arise.
ASCs excel for straightforward paroxysmal AFib patients seeking cost savings, faster scheduling, and streamlined same-day procedures. Not all states have ASC facilities ready to perform cardiac ablation on January 1, 2026—cardiovascular ASC licensing requirements vary significantly.
Geographic Availability of Medicare ASC Services
States with immediate 2026 ASC availability: California, Texas, Florida, Arizona, and New York lead in cardiovascular ASC infrastructure due to existing state licensure frameworks supporting complex cardiac procedures.
States with delayed rollout: Rural states and those requiring new state-level ASC cardiac certifications may see 3-12 month delays as facilities complete licensing requirements.
Telehealth pre-consultation options: Many high-volume centers now offer virtual initial consultations, expanding access for patients in underserved areas. After reviewing your medical records and ECG strips remotely, electrophysiologists can determine whether you’re an appropriate candidate before requiring travel for the actual procedure.
Insurance Pre-Authorization Success Strategies
Approximately 15% of AFib ablation procedures face initial insurance denials, but 85% of appeals succeed with proper documentation.
Required documentation for approval:
- Failed antiarrhythmic drug trial (at least 1-2 medications for paroxysmal AFib)
- Recent echocardiogram showing cardiac structure
- Documentation of symptomatic AFib episodes
- Physician letter of medical necessity
- Event monitor or Holter recordings demonstrating arrhythmia burden
Appeal timelines average 7-21 days for standard reviews, with expedited appeals completed in 72 hours for urgent cases. Work with your electrophysiologist’s prior authorization specialist—their experience navigating insurer requirements dramatically improves approval rates.
Taking the Next Step
Schedule consultations with 2-3 highly qualified electrophysiologists. The right physician-patient relationship combines technical expertise with communication styles matching your preferences—some patients prefer data-driven approaches while others value empathetic explanations.
Choosing an experienced electrophysiologist at a Medicare-approved ASC can reduce your wait time by 8+ weeks and save $200-600 in out-of-pocket costs compared to hospital outpatient settings, while potentially improving your cardiac ablation success rate by 12-18% through higher procedural volumes.
Patients who prepare thoroughly using resources like our comprehensive health tips library report feeling more confident during consultations and making treatment decisions aligned with their values and lifestyle goals.
Disclaimer: This article is for educational purposes only and does not constitute medical advice. Always consult with a board-certified cardiac electrophysiologist to determine the most appropriate AFib treatment plan for your specific medical condition, risk factors, and personal circumstances. Treatment recommendations should be individualized based on comprehensive evaluation of your complete medical history. Last updated: January 2026.
Frequently Asked Questions About AFib Ablation
1. What is the success rate of AFib ablation in 2026?
AFib ablation success rates reach 88% at 12 months for paroxysmal AFib using AI-guided techniques, 87% with standard radiofrequency ablation, and 73.8% at 24 months. Persistent AFib shows 56% success after the first procedure and 76% after repeat ablations.
2. How much does AFib ablation cost with Medicare in 2026?
Medicare patients pay approximately $425 out-of-pocket at ambulatory surgery centers (ASCs) starting January 1, 2026, compared to $629 at hospital outpatient departments. Without Medicare, costs range from $15,000-$50,000 depending on the facility and insurance coverage.
3. How long is AFib ablation recovery time?
Most patients recover within 1-2 days for initial restrictions, return to desk work in 3-7 days, and resume full activities in 2-4 weeks. The complete healing “blanking period” lasts 2-3 months, during which temporary AFib recurrences may occur without indicating procedure failure.
4. Is AFib ablation better than medication?
AFib ablation provides 63% reduction in arrhythmia burden compared to medications, with 87% of patients achieving freedom from AFib versus 45-55% effectiveness with drugs alone. Ablation also delivers superior quality of life improvements and potentially avoids lifelong medication costs.
5. What is pulsed field ablation cost for AFib?
Pulsed field ablation (PFA) costs $18,000-$28,000 at ASCs and $30,000-$45,000 at hospitals before insurance. Medicare covers PFA at ASCs for $425 average out-of-pocket, while private insurance patients pay $2,500-$7,000 copays depending on their plan.
6. How do I find AFib ablation near me?
Use the Heart Rhythm Society physician finder to search board-certified cardiac electrophysiologists by ZIP code. Look for ABIM Clinical Cardiac Electrophysiology certification, minimum 50 annual procedures, and facilities offering Medicare ASC-approved services starting 2026.
7. What are AFib ablation complications?
Major complications occur in 2-3% of procedures, including bleeding, blood clots, stroke (0.5-1%), heart perforation (0.1-0.3%), and esophageal injury (rare with PFA). Pulsed field ablation shows superior safety with 0.5% major adverse events versus traditional methods.
8. How long does AFib ablation procedure take?
Radiofrequency ablation takes 4-6 hours, cryoablation requires 3-4 hours, and pulsed field ablation completes in 2-3 hours. Total time includes preparation, sedation, catheter insertion, mapping, ablation, and post-procedure monitoring before discharge.
9. Does Medicare cover cardiac ablation at ASCs?
Yes, as of January 1, 2026, Medicare covers cardiac catheter ablation procedures (CPT codes 93653, 93654, 93656, 93657) at ambulatory surgery centers, reducing patient costs by approximately $200 compared to hospital outpatient settings.
10. Can AFib come back after ablation?
AFib recurrence rates are 12-32% depending on AFib type. Paroxysmal AFib shows 13% recurrence at 12 months, while persistent AFib has 44% recurrence after single procedures. Repeat ablations improve success to 76% for persistent cases.
11. What is the difference between ASC and hospital for AFib ablation?
ASCs cost $425 with Medicare versus $629 at hospitals, offer same-day discharge in 4-8 hours, specialize in pulsed field ablation for lower-risk patients, and schedule procedures 2-4 weeks faster. Hospitals provide overnight observation, full ICU backup, and handle complex cases with comorbidities.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.