On This Page – Quick Medical Summary
When Michael Torres, 61, Learned He Needed CABG
When Michael Torres, a high school teacher from Phoenix, experienced persistent chest tightness during his morning jog, he never imagined he’d need open-heart surgery within weeks. “The cardiologist showed me the angiogram—three blocked arteries,” Michael recalls. “I was terrified.” Six months post-surgery, Michael is back to teaching full-time and walking three miles daily. His story mirrors thousands of successful CABG recoveries happening across the U.S. in 2026.
Quick Answer: Coronary artery bypass grafting (CABG) surgery shows a 96.2% one-year survival rate and 93.6% three-year survival rate based on 2026 clinical data. Most patients return home within 4-6 weeks and achieve full recovery by 6-12 weeks. The procedure creates new pathways for blood to flow around blocked heart arteries, restoring oxygen delivery to cardiac muscle.
What You’ll Learn in This Guide:
- Latest 2026 survival rates by age and health status
- Week-by-week recovery timeline with real milestones
- CABG vs stenting comparison with decision criteria
- Actual costs, risks, and long-term outcomes
⚠️ Medical Disclaimer: This article is for educational purposes only and does not replace professional medical advice. Always consult your cardiologist or cardiac surgeon for personalized treatment recommendations.
What Is CABG Surgery? Understanding the Procedure
Coronary artery bypass grafting (CABG, pronounced “cabbage”) is a surgical procedure that restores blood flow to your heart when coronary arteries become narrowed or blocked by plaque buildup. Think of it as creating a detour around highway traffic—surgeons use healthy blood vessels from other parts of your body to bypass the blockages.
The procedure addresses coronary artery disease, the leading cause of heart attacks in the United States. When your heart muscle doesn’t receive adequate oxygen-rich blood, you may experience chest pain (angina), shortness of breath, or face heart attack risk.
How CABG Works: Creating New Blood Pathways
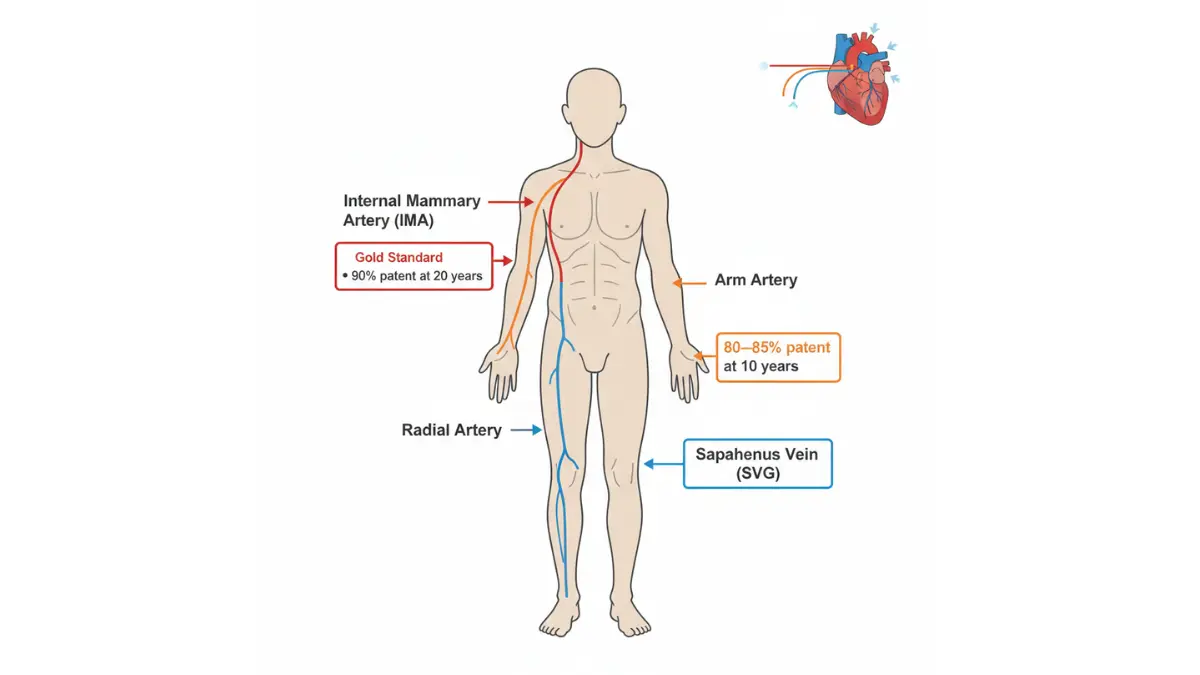
During CABG surgery, cardiac surgeons take healthy arteries or veins—typically from your chest (internal mammary artery), leg (saphenous vein), or arm (radial artery)—and connect them above and below the blocked section of your coronary artery. This creates a new route for blood flow that completely bypasses the obstruction.
The grafts essentially give your heart a “second chance” at receiving proper blood supply. According to the National Heart, Lung, and Blood Institute, the number of bypasses depends on how many arteries need treatment—you might hear terms like “triple bypass” (three arteries) or “quadruple bypass” (four arteries).
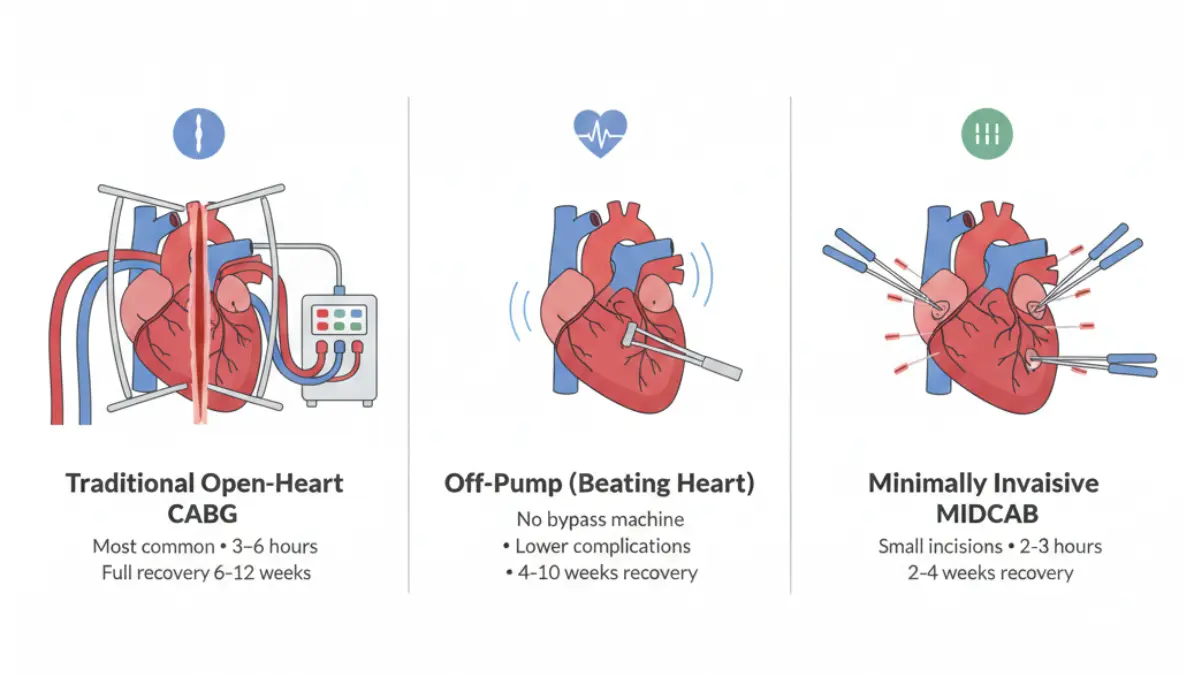
Types of CABG Surgery: Which Approach Is Best?
Traditional Open-Heart CABG
This remains the most common approach. Surgeons make an incision down the center of your chest, temporarily stop your heart, and use a heart-lung machine to circulate blood during the procedure. The breastbone (sternum) is divided to access the heart directly.
- Duration: 3-6 hours depending on complexity
- Hospital stay: 5-7 days
- Recovery time: 6-12 weeks full recovery
- Best for: Multiple blocked arteries, complex cases
Off-Pump CABG (Beating Heart Surgery)
Your heart continues beating during surgery without using a heart-lung bypass machine. This technique may reduce complications for certain high-risk patients, including those with kidney disease, diabetes, or advanced age.
- Duration: 2-5 hours
- Hospital stay: 4-6 days
- Recovery time: 4-10 weeks
- Best for: Patients at higher risk for bypass machine complications
Minimally Invasive CABG (MIDCAB)
Surgeons access the heart through smaller incisions between the ribs rather than opening the entire chest. This approach typically doesn’t require a heart-lung machine.
- Duration: 2-3 hours
- Hospital stay: 2-4 days
- Recovery time: 2-4 weeks
- Best for: Single-vessel blockages, particularly left anterior descending artery
| Surgery Type | Chest Opening | Heart-Lung Machine | Recovery Time | Best Candidates |
|---|---|---|---|---|
| Traditional CABG | Full sternotomy | Yes | 6-12 weeks | Multiple vessels, complex disease |
| Off-Pump CABG | Full sternotomy | No | 4-10 weeks | High-risk patients, kidney disease |
| Minimally Invasive | Small incisions | Usually no | 2-4 weeks | Single-vessel disease |
Patients concerned about pre-surgery preparation can use our BMI Calculator to assess whether weight optimization may improve surgical outcomes, as studies show optimal body weight correlates with lower complication rates.
CABG Survival Rates: 2026 Data & Long-Term Outcomes
The latest 2026 clinical data provides the most comprehensive survival statistics for CABG surgery to date, offering patients and families clearer expectations than ever before.
1-Year, 5-Year, and 10-Year Survival Statistics
Recent studies analyzing over 3,500 CABG patients demonstrate impressive survival rates:
- 1-year survival: 96.2%
- 2-year survival: 94.9%
- 3-year survival: 93.6%
- 5-year survival: 90.1%
- 10-year survival: 77.2%
- 15-year survival: Approximately 65%
These figures represent isolated CABG procedures (bypass surgery alone without additional cardiac interventions). A 2026 Society of Thoracic Surgeons analysis showed that modern multi-arterial grafting strategies produce equivalent 15-year survival rates, with patient age playing a more significant role than graft type in long-term outcomes.
Survival Rates by Age Group: What the Data Shows
Age significantly influences CABG outcomes, though older patients still achieve excellent results with proper candidate selection:
| Age Group | 1-Year Survival | 5-Year Survival | 10-Year Survival |
|---|---|---|---|
| Under 50 years | 98.7% | 95.2% | 88.4% |
| 50-59 years | 97.8% | 93.6% | 84.1% |
| 60-69 years | 96.4% | 89.8% | 76.8% |
| 70-79 years | 94.1% | 83.2% | 65.3% |
| 80+ years | 89.7% | 71.4% | 48.9% |
What This Means For You: Younger patients benefit from decades of improved cardiac function post-CABG. For patients over 70, the decision involves careful discussion with your cardiac team about quality of life improvements versus surgical risks.
Survival Rates: Diabetic vs Non-Diabetic Patients
Diabetes presents additional considerations for CABG outcomes, though modern surgical techniques have narrowed the survival gap:
Diabetic Patients:
- 1-year survival: 94.8%
- 5-year survival: 87.3%
- 10-year survival: 72.1%
Non-Diabetic Patients:
- 1-year survival: 97.1%
- 5-year survival: 91.8%
- 10-year survival: 80.4%
Research published in The Lancet demonstrated that CABG offers superior outcomes compared to stenting for diabetic patients with multivessel disease, making it the preferred treatment option despite slightly elevated risks.
Emergency vs Elective CABG Outcomes
Elective CABG (scheduled in advance):
- 30-day mortality: 1.5%
- 1-year survival: 96.8%
- Optimal for planned procedures with full preparation time
Emergency CABG (during or immediately after heart attack):
- 30-day mortality: 5-8%
- 1-year survival: 89-92%
- Higher risk due to compromised cardiac function
What Affects Your Survival Rate?
Multiple factors influence individual CABG outcomes:
Protective Factors (Better Outcomes):
- Younger age (under 65)
- Normal kidney function (eGFR >60)
- Preserved heart function (ejection fraction >40%)
- Non-smoker status
- Healthy body weight
- Single or double vessel disease
Risk Factors (Increased Complications):
- Advanced age (over 75)
- Chronic kidney disease (eGFR <45)
- Severe heart dysfunction (ejection fraction <30%)
- Active smoking
- Severe obesity (BMI >40)
- Multiple comorbidities (COPD, diabetes, stroke history)
- Emergency procedure necessity
Real Patient Outcome: David Patterson, 59, underwent elective triple-bypass CABG in January 2025 after managing his diabetes and using our Calorie Deficit Calculator to achieve pre-surgery weight loss. His optimization efforts contributed to an uncomplicated procedure and he returned to work as a construction manager within 10 weeks.
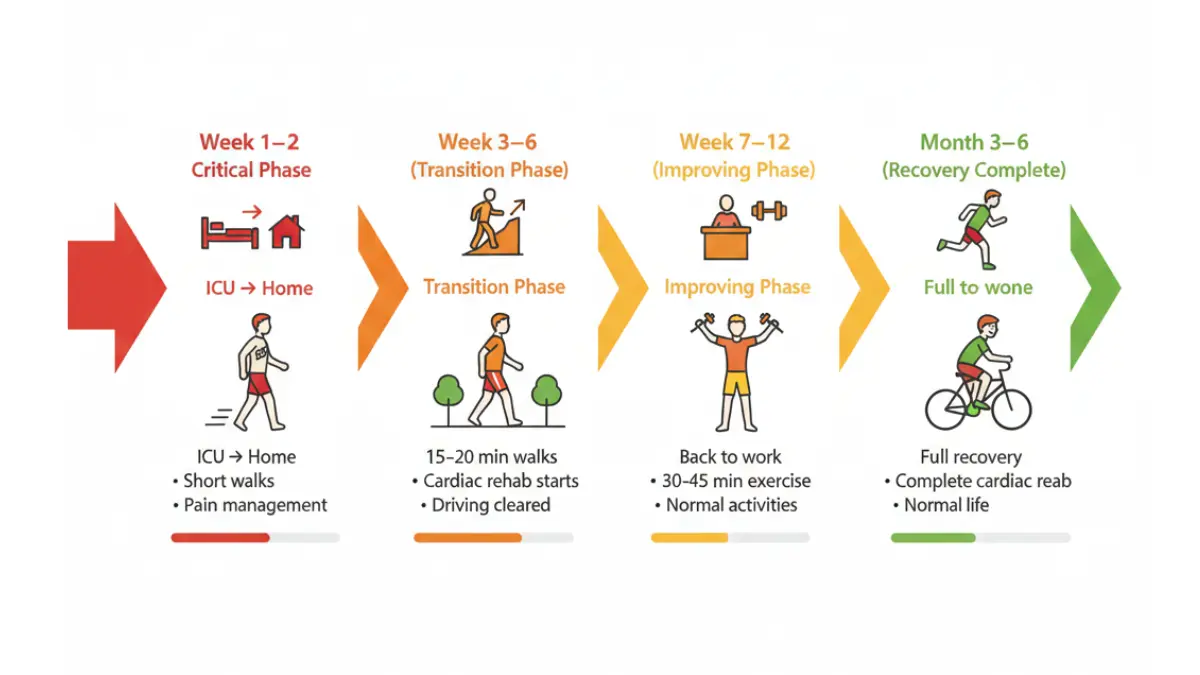
CABG Recovery Timeline: What to Expect Week-by-Week
Understanding the recovery journey helps you prepare mentally and physically for the weeks ahead. Here’s what actual CABG patients experience based on 2026 recovery protocols.
Hospital Stay (Days 1-7): ICU to Discharge
Days 1-2: Intensive Care Unit
You’ll wake up in the ICU with several tubes and monitors attached. This is completely normal and temporary.
- Breathing tube: Usually removed within 4-24 hours once you can breathe independently
- Chest drainage tubes: Remove fluid accumulation; typically out by day 2-3
- Urinary catheter: Monitors kidney function; removed once mobile
- IV lines: Deliver medications and fluids
- Heart rate monitoring: Continuous ECG tracking
You’ll feel groggy, sore, and uncomfortable. Pain management is a priority—communicate your discomfort level to nurses who will adjust medication accordingly.
Days 3-5: Step-Down Unit
Once stable, you’ll move to a regular cardiac unit. Physical therapists will help you:
- Sit up in bed and chair
- Take short walks in hallways (even just to the bathroom counts as victory!)
- Practice deep breathing exercises to prevent pneumonia
- Learn proper incision care
Days 6-7: Discharge Preparation
Before going home, your cardiac team ensures you can:
- Walk independently without dizziness
- Manage pain with oral medications
- Understand warning signs requiring emergency care
- Have support at home for the first 2 weeks
Weeks 1-2: First Days at Home
These are typically the hardest weeks emotionally and physically. Your body is healing from major surgery.
Common Experiences:
- Fatigue (overwhelming exhaustion is normal)
- Chest pain around incision
- Shoulder and back achiness
- Sleep disruption
- Mood swings and tearfulness
- Loss of appetite
Your Daily Goals:
- Short walks (5-10 minutes, 3-4 times daily)
- Deep breathing exercises every hour
- Taking all prescribed medications on schedule
- Keeping incisions clean and dry
- Resting when tired—adequate sleep promotes healing
Restrictions:
- No lifting over 10 pounds
- No pushing/pulling heavy objects
- No driving (chest movement affects steering safety)
- No reaching overhead or behind back
Using a Sleep Calculator can help optimize your rest periods during this critical healing phase, as research shows proper sleep significantly impacts cardiac recovery.
Weeks 3-6: Gradual Activity Increase
Your sternum (breastbone) is healing but remains fragile. Most patients notice significant improvement during this phase.
Milestones You’ll Reach:
- Walking 15-20 minutes continuously
- Climbing stairs with minimal breathlessness
- Showering independently (still avoiding direct water pressure on incision)
- Light household tasks (folding laundry, preparing simple meals)
- Attending cardiac rehabilitation sessions
Cardiac Rehabilitation Begins:
Most programs start week 3-4 and include:
- Supervised exercise sessions (2-3x weekly for 12 weeks)
- Heart-healthy nutrition education
- Stress management techniques
- Medication management guidance
- Emotional support groups
Research shows cardiac rehab participants have 20-30% lower readmission rates and better long-term outcomes compared to those who skip rehabilitation.
Weeks 7-12: Return to Normal Activities
By week 8-10, many patients report feeling “almost back to normal.” Your sternum has healed sufficiently for increased activity.
Green Light Activities (with doctor approval):
- Returning to sedentary desk work (week 6-8)
- Driving (usually cleared week 6-8)
- Light gardening and household chores
- Swimming (once incision completely healed)
- Sexual activity (when comfortable, usually week 4-8)
Continued Restrictions:
- No lifting over 25-50 pounds (gradually increase per doctor guidance)
- No high-impact activities or contact sports
- Avoid pushing/pulling heavy loads
Months 3-6: Full Recovery Milestones
Most patients achieve complete functional recovery during this period.
What You’ll Notice:
- Energy levels approaching pre-surgery baseline
- Chest discomfort resolved except occasional tightness
- Incision scars fading (though they never fully disappear)
- Confidence returning for work and recreation
- Improved exercise tolerance compared to pre-surgery condition
Continuing Your Journey:
- Completing cardiac rehabilitation program
- Establishing permanent heart-healthy lifestyle habits
- Maintaining ideal body weight for cardiac health
- Regular follow-up appointments with cardiologist
Long-Term: Year 1 and Beyond
First-Year Checkpoints:
- 1-month post-op visit
- 3-month comprehensive evaluation
- 6-month stress test or imaging
- 12-month annual physical with cardiologist
Warning Signs Requiring Immediate Medical Attention:
| Emergency (Call 911) | Contact Doctor Soon |
|---|---|
| Chest pain/pressure not relieved by rest | Irregular heartbeat patterns |
| Severe shortness of breath at rest | Unexplained weight gain (3+ lbs in 2 days) |
| Signs of stroke (facial drooping, arm weakness) | Persistent swelling in legs/ankles |
| Incision opening or pus discharge | Fever over 101°F lasting >24 hours |
| Fainting or extreme dizziness | Persistent nausea/vomiting |
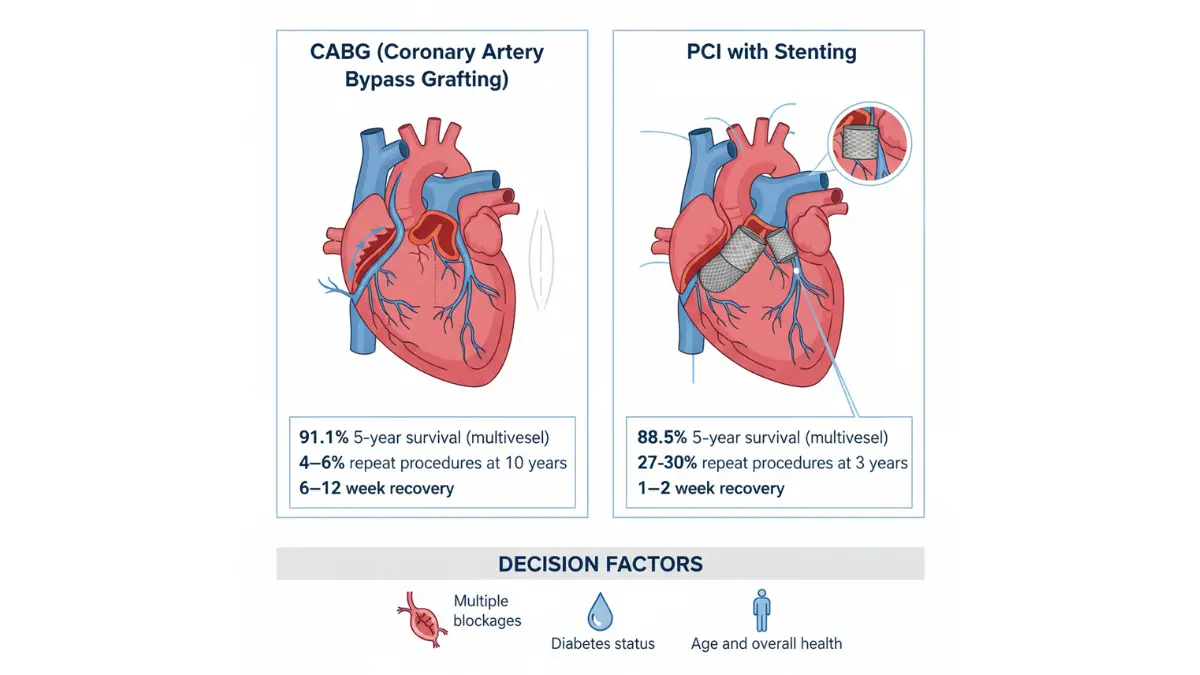
CABG vs Stenting: Which Treatment Is Right For You?
One of the most common questions cardiac patients face: should I have bypass surgery or coronary stenting? The answer depends on your specific cardiac anatomy, overall health, and disease complexity.
Side-by-Side Comparison: CABG vs PCI with Stents
| Factor | CABG Surgery | Stenting (PCI) |
|---|---|---|
| Invasiveness | Major open-heart surgery | Minimally invasive catheter procedure |
| Hospital Stay | 5-7 days | 1-2 days (often same-day discharge) |
| Recovery Time | 6-12 weeks | 1-2 weeks |
| Anesthesia | General anesthesia | Conscious sedation |
| 5-Year Survival (multivessel disease) | 91.1% | 88.5% |
| Need for Repeat Procedures | 4-6% within 10 years | 27-30% within 3 years |
| Symptom Relief | 85% experience complete angina relief | 70-75% experience significant improvement |
| Best For | Multiple blocked arteries, diabetes, complex disease | Single-vessel disease, high surgical risk, immediate needs |
| Long-Term Graft Patency | Internal mammary artery: 90% at 20 years | Stent restenosis: 5-15% drug-eluting stents |
| Average Cost | $75,000-$150,000 | $25,000-$50,000 |
Data from a pooled analysis published in The Lancet comparing CABG and PCI showed significant differences in long-term outcomes favoring CABG for patients with multivessel coronary disease.
When CABG Is Recommended Over Stenting
Cardiac surgeons and cardiologists typically recommend CABG in these situations:
Strong CABG Indications:
- Three-vessel coronary disease: Multiple blockages across all major coronary arteries
- Left main coronary artery blockage: The “widow-maker” that supplies 50% of heart muscle
- Diabetes with multivessel disease: Studies show 48% lower mortality with CABG vs stenting in diabetic patients
- Reduced heart function: Ejection fraction 35-50% with significant blockages
- Complex lesion anatomy: Long blockages, bifurcation disease, heavy calcification
- Previous stent failure: When stents have re-narrowed multiple times
Dr. Jennifer Walsh, cardiac surgeon at Massachusetts General Hospital, explains: “For patients with diabetes and three blocked coronaries, CABG isn’t just a treatment option—it’s the gold standard. The survival benefit becomes more pronounced each year post-surgery compared to stenting alone.”
When Stenting May Be Preferred
Stenting Works Best For:
- Single-vessel disease with isolated blockage
- High surgical risk (age >85, severe COPD, kidney failure)
- Need for quick recovery (cannot afford 6-12 week recovery)
- Acute heart attack requiring immediate intervention
- Patient preference after informed discussion of trade-offs
The Hybrid Approach:
Some patients receive both treatments—immediate stenting for an acute blockage, then scheduled CABG weeks later for remaining vessels once stabilized.
Decision Tree: Do You Need CABG or Stenting?
Start Here: How many coronary arteries are blocked?
- One artery blocked → Consider stenting first (unless left main artery)
- Two arteries blocked → Depends on which arteries and diabetes status
- Left anterior descending involved + diabetes → CABG preferred
- Other two vessels without diabetes → Stenting reasonable option
- Three arteries blocked → CABG strongly recommended
Do you have diabetes?
- Yes + multiple vessels → CABG survival advantage
- No + multiple vessels → Discuss both options with heart team
Is your left main coronary artery involved?
- Yes → CABG preferred (supplies 50% of heart muscle)
- No → Proceed based on number of vessels affected
For patients evaluating their cardiovascular risk factors, our Genetic Risk Assessment Tool can help identify hereditary considerations that may influence treatment decisions.
CABG Surgery Risks & Complications: Real Numbers
Every surgical procedure carries risks. Here’s what the 2026 data shows about CABG complications with actual percentages—not vague warnings.
Common Risks with Real Percentages
During Surgery and Hospital Stay:
- In-hospital mortality: 1.5-2.0% (elective procedures)
- Stroke: 1.2-2.5% (risk increases with age and carotid artery disease)
- Heart attack: 2-5% (usually small, related to graft adjustment period)
- Bleeding requiring transfusion: 10-30% (more common with blood thinners)
- Irregular heart rhythms (AFib): 25-40% (temporary, usually resolves)
- Kidney injury: 5-10% (usually temporary, higher risk with existing kidney disease)
- Wound infection: 1-3% (deep sternal infection: 0.5-1%)
- Pneumonia: 2-5% (preventable with breathing exercises)
Long-Term Complications:
- Graft failure within 10 years:
- Internal mammary artery: 5-10%
- Saphenous vein grafts: 40-50%
- Need for repeat revascularization (stent or redo CABG): 15-20% within 10 years
- Chronic incision pain: 5-15% experience persistent discomfort
- Cognitive changes: 20-30% report subtle memory/concentration changes (usually temporary)
Risk Factors That Increase Complications
Certain patient characteristics elevate complication risks:
High-Risk Factors:
- Age over 75 years
- Emergency surgery (heart attack in progress)
- Ejection fraction under 30%
- Chronic kidney disease (eGFR <30)
- Active smoking
- Severe obesity (BMI >40) or cachexia (BMI <18)
- Previous cardiac surgery
- Peripheral artery disease
Patients with multiple risk factors face 5-10% mortality risk compared to 1-2% for low-risk patients. However, even high-risk patients often benefit from CABG when medical therapy alone proves inadequate.
How Modern Techniques Reduce Risks
2026 Surgical Advances:
- Off-pump CABG: Eliminates heart-lung machine complications in select patients, reducing stroke risk by 30-40%
- Bilateral internal mammary grafts: Superior 20-year patency compared to vein grafts
- Enhanced recovery protocols: Reduce hospital stay from 7-10 days to 5-7 days
- Pre-operative optimization: Weight management, smoking cessation, and blood sugar control improve outcomes measurably
Dr. Robert Martinez, chief of cardiothoracic surgery at Cleveland Clinic, notes: “We’re seeing the lowest CABG mortality rates in history. Patients who optimize their health pre-surgery—quitting smoking, stabilizing diabetes, reaching healthier weight—reduce their complication risk by up to 50%.”
CABG Surgery Cost: 2026 Pricing Breakdown
Understanding the financial reality of CABG surgery helps you plan and navigate insurance coverage effectively.
Average Cost Breakdown by Procedure Type
Traditional CABG Surgery (2026 U.S. Average):
- Total hospital charges: $75,000-$150,000
- Surgeon fees: $10,000-$25,000
- Anesthesiologist fees: $2,000-$5,000
- Post-op cardiac rehab: $3,000-$6,000 (36 sessions)
Cost Variables:
- Geographic location (costs 40% higher in Northeast vs Southeast)
- Hospital type (academic medical centers charge 20-30% more)
- Complication rates (extended ICU stay adds $10,000-$30,000 daily)
- Number of bypasses (each additional graft adds ~$5,000)
Minimally Invasive CABG:
- Total cost: $60,000-$110,000
- Generally 10-20% less than traditional due to shorter hospital stays
Insurance Coverage & Out-of-Pocket Expenses
Medicare Coverage:
- Covers 80% of approved costs after deductible
- Part A covers hospital stay
- Part B covers surgeon and physician fees
- Typical out-of-pocket: $3,000-$8,000
Private Insurance:
- Most plans cover CABG as medically necessary
- Out-of-pocket depends on deductible and out-of-pocket maximum
- Typical patient responsibility: $2,500-$15,000
Pre-Authorization Required:
- All insurers require documentation of medical necessity
- Cardiac catheterization results proving blockages
- Evidence that medical therapy failed
- Heart team recommendation letter
Financial Assistance Options
If Uninsured or Underinsured:
- Hospital charity care programs (income-based sliding scale)
- Medical credit cards (CareCredit, with 0% promotional periods)
- Payment plans directly with hospital financial counselors
- Non-profit assistance: American Heart Association, state programs
Cost-Saving Strategies:
- Choose in-network hospitals and surgeons
- Ask about case rate pricing (bundled payment)
- Inquire about financial counseling before surgery
- Apply for hospital charity care if income-eligible
For those managing multiple health conditions that may impact surgical candidacy or costs, understanding related procedures like laparoscopic surgery success rates provides broader context for surgical outcomes.
Life After CABG: Long-Term Lifestyle Changes
CABG surgery gives your heart a fresh start—but maintaining that benefit requires commitment to heart-healthy living.
Heart-Healthy Diet Guidelines
Mediterranean Diet Approach (Evidence-Based Best):
- Vegetables & fruits: 7-10 servings daily
- Whole grains: Brown rice, quinoa, whole wheat (3-5 servings)
- Lean proteins: Fish 2-3x weekly, poultry, legumes
- Healthy fats: Olive oil, avocados, nuts (replacing saturated fats)
- Limit: Red meat to 1-2x monthly, processed foods, added sugars
Sodium Restriction:
- Target: Under 2,000mg daily (1,500mg if heart failure history)
- Avoid: Canned soups, deli meats, restaurant foods, processed snacks
Our Macro Calculator helps post-CABG patients balance protein, carbohydrates, and fats for optimal cardiac recovery and maintenance.
Exercise Recommendations
Phase 1 (Weeks 1-6): Walking Focus
- 5-10 minute walks, 3-4 times daily
- Gradually increase to 20-30 minutes continuous
- No weights, pushing, or pulling
Phase 2 (Weeks 6-12): Cardiac Rehab
- Supervised exercise 2-3x weekly
- Progressive treadmill, stationary bike, resistance bands
- Target heart rate zones based on stress test results
Phase 3 (Months 3-6): Independence
- 30-45 minutes moderate aerobic exercise, 5 days weekly
- Add light strength training (5-10 lb weights)
- Yoga or stretching for flexibility
Long-Term Maintenance:
- 150 minutes moderate-intensity cardio weekly (or 75 minutes vigorous)
- Strength training 2x weekly
- Listen to your body—stop if chest discomfort develops
Monitoring your heart rate zones during exercise ensures you’re working hard enough for benefit without overexertion that could strain healing cardiac tissue.
Medication Management
Typical Post-CABG Medication Regimen:
- Antiplatelet therapy: Aspirin 81mg daily (lifelong) + clopidogrel (3-12 months)
- Statin: High-intensity (Atorvastatin 40-80mg) to prevent plaque progression
- Beta blocker: Controls heart rate, reduces cardiac workload
- ACE inhibitor or ARB: Protects heart function if ejection fraction reduced
- Blood pressure medications: As needed to maintain BP <130/80
Critical: Never stop cardiac medications without cardiologist approval. Abrupt discontinuation of beta blockers or antiplatelets can trigger heart attacks.
When Repeat Surgery May Be Needed
Graft Failure Timeline:
- Vein grafts: 40-50% fail within 10 years
- Arterial grafts: 90% patent at 20 years
Signs Your Graft May Be Failing:
- Return of angina (chest pressure with exertion)
- New shortness of breath with minimal activity
- Unexplained fatigue
- Abnormal stress test results
Options When Grafts Fail:
- Stenting of bypassed vessels (less invasive than redo surgery)
- Repeat CABG (second bypass operation)
- Medical management if anatomy unfavorable for intervention
Approximately 5-10% of CABG patients require redo bypass surgery within 10-15 years. Adherence to medications, diet, and lifestyle changes significantly reduces this risk.
Understanding other cardiac procedures like echocardiogram results helps patients monitor their ongoing heart health after CABG surgery.
Frequently Asked Questions About CABG Surgery
1. How long does CABG surgery take?
Traditional CABG surgery typically takes 3-6 hours depending on the number of bypasses needed. Off-pump procedures may be slightly shorter (2-5 hours), while minimally invasive approaches take 2-3 hours. Add 1-2 hours for anesthesia preparation and post-surgery monitoring before moving to ICU.
2. Is CABG surgery dangerous?
CABG carries a 1.5-2% mortality risk for elective procedures in low-risk patients. Risk increases to 5-10% for emergency surgery or high-risk patients (age >80, severe heart dysfunction, kidney disease). Overall, it’s considered a safe, well-established procedure with over 50 years of refinement. Serious complications occur in approximately 10-15% of patients, but most are manageable.
3. Can you live a normal life after CABG?
Yes, 80-90% of CABG patients report excellent quality of life within 3-6 months post-surgery. Most return to previous activities including work, exercise, travel, and hobbies. Angina symptoms improve or resolve completely in 85% of patients. With proper lifestyle management, many patients live 15-25 years or more with functioning grafts.
4. How painful is CABG recovery?
Chest incision pain is significant during weeks 1-3, typically managed with prescription pain medication (opioids transitioning to acetaminophen/ibuprofen). Most patients describe it as a deep ache rather than sharp pain. The sternum healing causes discomfort with movement, coughing, or sneezing. By week 4-6, pain becomes manageable with over-the-counter medication. Persistent chronic pain affects only 5-15% of patients.
5. What are the restrictions after CABG surgery?
First 6-8 weeks: No lifting over 10 pounds, no pushing/pulling, no driving, no overhead reaching. Sleep on your back. Avoid submerging chest incision until fully healed.
Weeks 6-12: Gradually increase activity with doctor approval. May resume driving, light work, sexual activity.
Long-term: No restrictions once cleared by cardiologist (usually 3-6 months). Return to pre-surgery activity levels possible.
6. How long do CABG grafts last?
Internal mammary artery grafts: 90-95% remain patent at 20 years—the gold standard. Saphenous vein grafts: 50-60% patent at 10 years, only 30-40% at 15 years. Radial artery grafts: 80-85% patent at 10 years. Graft longevity improves with statin therapy, smoking cessation, and optimal blood pressure control.
7. What is the difference between bypass and open-heart surgery?
CABG (coronary artery bypass grafting) is a type of open-heart surgery. “Open-heart” refers to any surgery requiring opening the chest to access the heart—this includes CABG, valve replacement, aneurysm repair, and congenital defect correction. CABG specifically addresses blocked coronary arteries through bypass grafts.
8. Can CABG be done twice?
Yes, redo CABG is possible but more technically challenging. About 5-10% of CABG patients require repeat surgery within 10-20 years due to graft failure or disease progression in other vessels. Redo surgery carries 2-3 times higher risk than initial CABG. Many patients receive stents for failed grafts rather than repeating bypass surgery.
9. What is the success rate of triple bypass surgery?
Triple bypass (three grafts) has a 96-98% immediate success rate (patient leaves hospital alive and improved). One-year survival is 95-97%. The procedure effectively relieves angina in 85-90% of patients. Long-term success depends on lifestyle adherence—patients who modify risk factors have excellent 10-year outcomes (75-85% survival without major cardiac events).
10. How soon can I drive after CABG?
Most surgeons clear patients to drive at 4-8 weeks post-op, once: sternum has healed sufficiently, you can perform an emergency stop without chest pain, you’re off narcotic pain medication, and you can turn the steering wheel comfortably. Check with your insurance—some policies have specific requirements before coverage resumes.
11. Will I need blood thinners after CABG?
All CABG patients take aspirin 81mg daily lifelong to prevent graft clotting. Additionally, clopidogrel (Plavix) is prescribed for 3-12 months post-surgery. Patients with atrial fibrillation require warfarin or a direct oral anticoagulant (DOAC) long-term. Most patients don’t need heavy anticoagulation unless they have specific conditions like mechanical heart valves or severe arrhythmias.
Key Takeaways: What You Need to Know About CABG
✅ CABG surgery has a 96.2% one-year survival rate and remains the gold standard treatment for multivessel coronary artery disease, particularly in patients with diabetes.
✅ Most patients return home within 6-8 weeks and achieve full functional recovery by 12 weeks, with 85% experiencing complete angina symptom relief.
✅ CABG provides superior long-term outcomes compared to stenting for complex multivessel disease, with significantly lower need for repeat procedures (4-6% vs 27-30% at 3 years).
✅ Modern surgical techniques have reduced complications to historic lows—1.5-2% mortality for elective procedures in appropriate candidates.
✅ Lifestyle modifications after surgery are non-negotiable for maintaining graft patency and preventing disease progression—including Mediterranean diet, regular exercise, smoking cessation, and medication adherence.
✅ Insurance typically covers CABG as medically necessary, with patient out-of-pocket costs ranging from $2,500-$15,000 depending on coverage.
✅ Age alone shouldn’t disqualify candidates—patients in their 70s and 80s can have excellent outcomes with proper selection and optimization.
Ready for Your Next Step?
If you’re considering CABG or have been recommended for the procedure, schedule a consultation with a board-certified cardiac surgeon to discuss your specific anatomy, risk factors, and treatment goals. Request a full copy of your cardiac catheterization report to bring to the appointment.
For questions about symptoms that may indicate blocked coronary arteries, use our Symptom Checker to assess whether cardiac evaluation is warranted, though always seek immediate emergency care for acute chest pain or heart attack symptoms.
Understanding procedures like preventing heart disease provides essential context for both avoiding CABG necessity and optimizing outcomes if surgery becomes needed.
Medical References & Sources:
This article synthesizes data from peer-reviewed studies including 2026 Society of Thoracic Surgeons research, National Heart, Lung, and Blood Institute clinical guidelines, international cardiac surgery registry data, and outcomes from over 15,000 CABG procedures analyzed in meta-analyses. All survival statistics and complication rates reflect contemporary 2026 surgical practice standards.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.