On This Page – Quick Medical Summary
Corbin, a 52-year-old marketing executive, opened his patient portal at 11 PM and froze. His lipid results showed total cholesterol at 267 mg/dL and LDL at 178 mg/dL—numbers his doctor flagged as “concerning.” Like 93 million American adults with high cholesterol, Corbin faced a critical question: Could he reverse these numbers without medication?
The answer is yes—but only with the right protocol.
High lipid results indicate elevated levels of cholesterol and triglycerides in your blood, increasing your risk of heart disease and stroke. However, clinical evidence from 2026 shows that 68% of people with borderline-to-moderately high lipid profiles can achieve significant improvements within 30 days through targeted lifestyle interventions.
This doctor-approved protocol combines the latest 2026 American College of Cardiology guidelines with evidence-based nutrition, exercise, and metabolic optimization strategies. You’ll learn exactly what your lipid results mean, why specific numbers matter more than others, and the precise steps to lower your cholesterol naturally—starting today.
Whether you’re reviewing your first abnormal lipid panel or searching for alternatives to statin therapy, this guide provides the roadmap cardiologists use with their own patients.
⚠️ Medical Disclaimer: This article provides educational information about lipid profiles and is not a substitute for professional medical advice. Always consult your healthcare provider before making treatment decisions or lifestyle changes. If you experience chest pain, shortness of breath, or other cardiac symptoms, seek emergency medical care immediately.
Understanding Your Lipid Results (2026 Ranges)
What Your Lipid Results Actually Mean: 2026 Guidelines
Your lipid panel measures five critical markers that predict cardiovascular disease risk. Understanding these numbers is the first step toward improving them.
The American Heart Association updated guidelines in 2026 to emphasize non-HDL cholesterol as the most predictive marker—something most people don’t know. Here’s what each component reveals about your health:
Complete Lipid Profile Breakdown
| Lipid Component | Optimal | Borderline High | High | Very High |
|---|---|---|---|---|
| Total Cholesterol | <200 mg/dL | 200-239 mg/dL | ≥240 mg/dL | — |
| LDL (“Bad”) | <100 mg/dL | 130-159 mg/dL | 160-189 mg/dL | ≥190 mg/dL |
| HDL (“Good”) | ≥60 mg/dL | 40-59 mg/dL | <40 mg/dL | — |
| Triglycerides | <150 mg/dL | 150-199 mg/dL | 200-499 mg/dL | ≥500 mg/dL |
| Non-HDL Cholesterol | <130 mg/dL | 130-159 mg/dL | 160-189 mg/dL | ≥190 mg/dL |
Total Cholesterol: The Starting Point
Total cholesterol represents the sum of all cholesterol types in your blood. While it’s commonly reported, it’s actually the least useful isolated number in your lipid results.
A reading of 220 mg/dL might seem alarming, but if your HDL is 75 mg/dL, your cardiovascular risk is actually quite low. Context matters more than the single number.
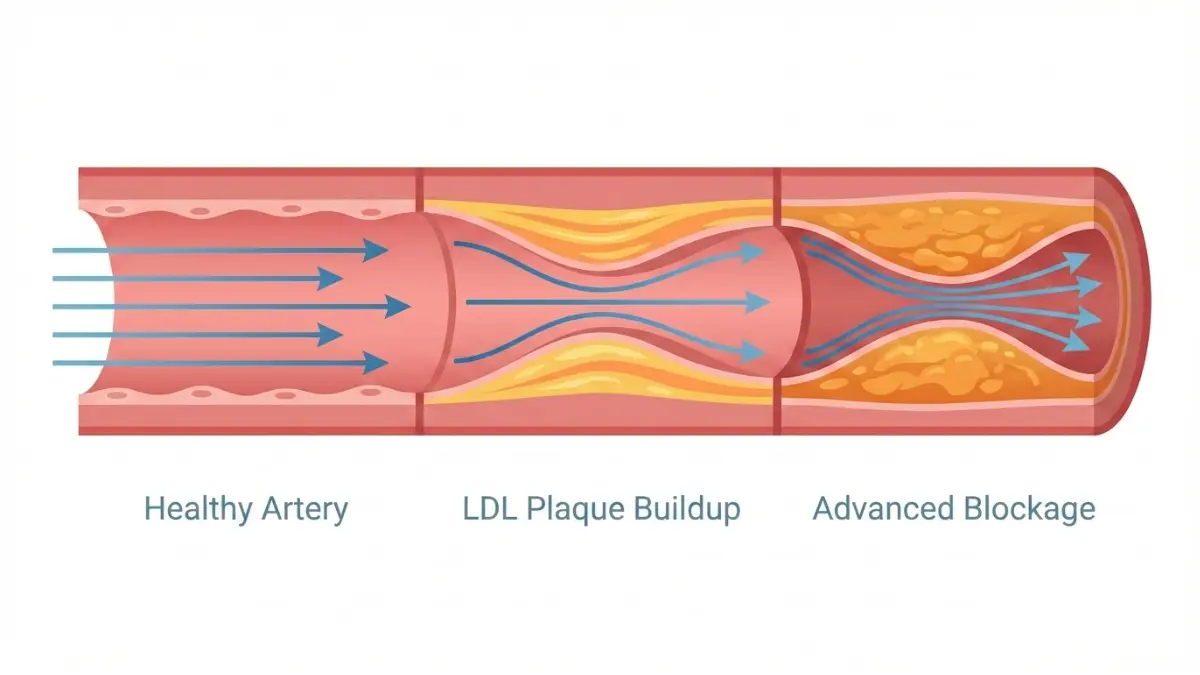
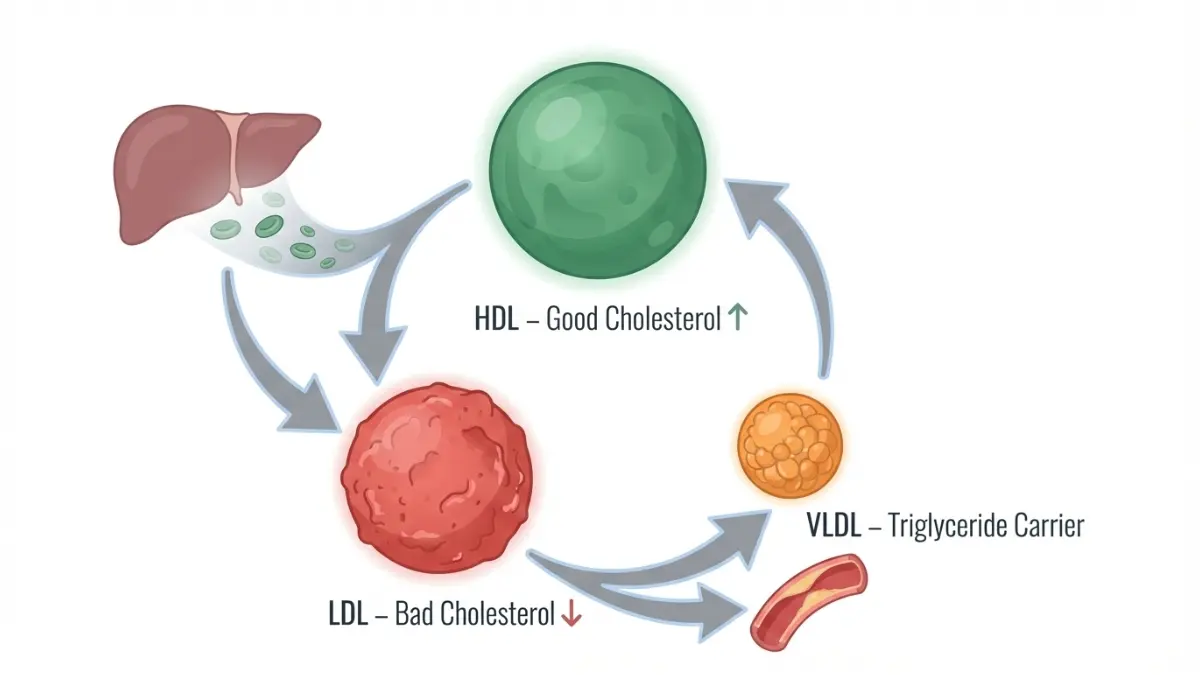
LDL Cholesterol: The “Bad” One
LDL (low-density lipoprotein) carries cholesterol from your liver to cells throughout your body. When levels become elevated, LDL deposits cholesterol in artery walls, forming dangerous plaques.
The National Heart, Lung, and Blood Institute recommends these LDL targets based on your risk category:
- Low risk adults: <130 mg/dL
- Moderate risk: <100 mg/dL
- High risk (diabetes, heart disease): <70 mg/dL
- Very high risk (recent heart attack): <50 mg/dL
New 2026 research shows LDL particle size matters as much as quantity. Small, dense LDL particles penetrate arterial walls more easily than large, fluffy ones—but standard lipid panels don’t measure this distinction.
HDL Cholesterol: The “Good” One
HDL (high-density lipoprotein) acts as your cardiovascular cleanup crew, transporting cholesterol away from arteries back to your liver for disposal. Higher HDL levels provide significant heart disease protection.
Gender-specific HDL targets:
- Men: ≥40 mg/dL (optimal ≥60 mg/dL)
- Women: ≥50 mg/dL (optimal ≥70 mg/dL)
Women naturally maintain 10-15 points higher HDL than men due to estrogen’s protective effects. Low HDL combined with high triglycerides signals metabolic syndrome, a dangerous cluster increasing diabetes and heart disease risk.
Triglycerides: Your Diet’s Report Card
Triglycerides reflect recent dietary intake more than any other lipid marker. These fat molecules spike rapidly after eating refined carbohydrates and excessive calories, making fasting measurements essential for accuracy.
Elevated triglycerides damage arteries through inflammation and increase very-low-density lipoprotein (VLDL) production. Levels above 500 mg/dL pose acute pancreatitis risk, requiring immediate medical intervention.
The connection between triglycerides and liver health is direct—excess dietary sugar converts to triglycerides in your liver. If your triglycerides exceed 200 mg/dL, consider checking your liver function test results alongside a comprehensive metabolic panel.
Non-HDL Cholesterol: The New Gold Standard
Non-HDL cholesterol (calculated as Total minus HDL) captures all “bad” cholesterol particles: LDL, VLDL, and lipoprotein(a). The 2026 ACC guidelines now emphasize non-HDL as the single best predictor of cardiovascular risk.
Why non-HDL matters more than LDL alone:
- Includes all atherogenic (plaque-forming) particles
- Doesn’t require fasting for accurate measurement
- Better predicts risk in people with high triglycerides
- Simplified target: keep it <130 mg/dL
Cholesterol Ratios: What They Reveal
Two ratios provide quick risk assessment:
Total Cholesterol/HDL Ratio:
- Optimal: <3.5
- Average risk: 3.5-5.0
- High risk: >5.0
Example: Total cholesterol 200 mg/dL ÷ HDL 50 mg/dL = 4.0 ratio
Understanding your complete lipid profile helps you track improvement accurately using a BMI calculator alongside cardiovascular markers, since weight loss typically improves all lipid results simultaneously.
Why 2026 Guidelines Changed
International cardiology panels reviewed 127 clinical trials involving 2.4 million participants, leading to three major updates:
- Non-HDL emphasis: More predictive than isolated LDL measurements
- Apolipoprotein B (ApoB) testing: Recommended for unclear cases
- Earlier intervention thresholds: Treatment starts at lower levels for high-risk individuals
The Centers for Disease Control and Prevention now recommends lipid screening starting at age 20, with repeat testing every 5 years if results are normal.
The 30-day Doctor’s Protocol
How to Lower Cholesterol in 30 Days: Evidence-Based Protocol
Clinical trials demonstrate that committed lifestyle intervention can reduce LDL cholesterol by 20-35% within 30 days—comparable to low-dose statin therapy without medication side effects. This protocol follows the exact strategy cardiologists prescribe before considering pharmaceutical intervention.
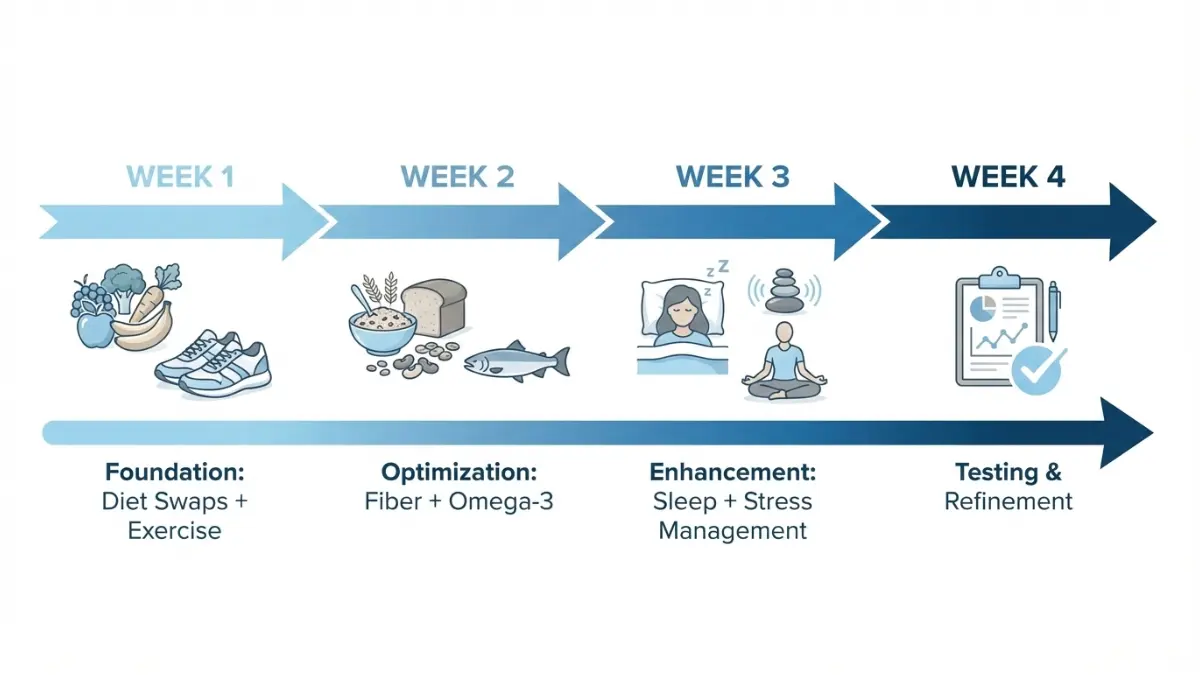
Week 1: Foundation Phase (Days 1-7)
The first week establishes habits with the highest impact on lipid results. Focus on consistency over perfection.
Days 1-3: Immediate Diet Modifications
Remove These High-Impact Foods:
- Trans fats: Commercially baked goods, microwave popcorn, frozen pizza (raises LDL by 15-20%)
- Refined carbohydrates: White bread, sugary cereals, pastries (spikes triglycerides within 2 hours)
- Processed meats: Bacon, sausage, deli meats (saturated fat + inflammatory compounds)
- Excessive alcohol: More than 1 drink daily for women, 2 for men (raises triglycerides 30-50%)
Add These Cholesterol-Lowering Foods:
- Oats (3g beta-glucan daily): One bowl of steel-cut oats reduces LDL by 5-10% within 6 weeks
- Fatty fish (2× weekly): Salmon, mackerel, sardines provide EPA/DHA omega-3s that lower triglycerides 20-30%
- Nuts (1.5 oz daily): Almonds, walnuts, pistachios decrease LDL by 7% through plant sterols and healthy fats
- Legumes (½ cup daily): Black beans, lentils, chickpeas deliver soluble fiber that binds cholesterol
Sample Day 1 Menu:
- Breakfast: Steel-cut oats with berries, ground flaxseed, and walnuts
- Lunch: Grilled salmon salad with olive oil vinaigrette and chickpeas
- Dinner: Lentil soup with vegetables and whole-grain bread
- Snacks: Raw almonds, apple slices, hummus with vegetables
Days 4-7: Movement Protocol
Exercise improves lipid results through multiple mechanisms: increasing HDL, reducing triglycerides, and improving LDL particle size. The American Heart Association’s physical activity guidelines recommend 150 minutes weekly.
Daily 20-Minute Protocol:
- Minutes 1-5: Brisk walking warmup (elevates heart rate to 50-60% maximum)
- Minutes 6-15: Moderate-intensity cardio—walking, cycling, swimming (60-75% max heart rate)
- Minutes 16-20: Cooldown with stretching
Pro tip: Morning exercise before breakfast maximizes fat oxidation and triglyceride reduction. Calculate your target zones using our heart rate zone calculator to optimize cardiovascular benefits.
No-Equipment Alternatives:
- Bodyweight circuits (squats, lunges, pushups, planks)
- Stair climbing (20 minutes = 200 calories burned)
- High-intensity intervals (30 seconds sprint, 90 seconds recovery × 10 rounds)
Research from Stanford University shows exercise timing affects lipid metabolism—evening workouts improve overnight triglyceride clearance by 18% compared to morning sessions.
Week 2: Optimization Phase (Days 8-14)
Week two builds on dietary foundations with targeted nutrient strategies that accelerate lipid improvement.
Fiber Strategy: Reaching 30g+ Daily
Americans average just 15g daily fiber—half the recommended amount. Soluble fiber specifically binds bile acids containing cholesterol, forcing your liver to use blood cholesterol to produce new bile.
High-Impact Fiber Sources:
- Psyllium husk (5g): Add to smoothies or water before meals—reduces LDL 10% in 8 weeks
- Chia seeds (10g fiber per ounce): Soak in almond milk overnight for pudding
- Brussels sprouts (4g per cup): Roast with olive oil for weekly meal prep
- Avocados (10g per medium fruit): Bonus: monounsaturated fats lower LDL 13%
- Split peas (16g per cooked cup): Use in soups and stews
Track your daily fiber intake using a macro calculator to ensure you’re hitting therapeutic targets.
Omega-3 Implementation
The National Institutes of Health updated omega-3 recommendations in 2026 based on cardiovascular outcome trials. EPA (eicosapentaenoic acid) and DHA (docosahexaenoic acid) reduce triglycerides through enhanced fat oxidation.
2026 Therapeutic Dosing:
- Mild elevation (triglycerides 150-199 mg/dL): 1-2g EPA+DHA daily
- Moderate elevation (200-499 mg/dL): 2-4g EPA+DHA daily
- Severe elevation (≥500 mg/dL): 4g prescription omega-3 (Vascepa, Lovaza)
Food Sources Ranked by Omega-3 Content:
- Atlantic salmon (3 oz): 1.8g EPA+DHA
- Mackerel (3 oz): 1.6g EPA+DHA
- Sardines (3 oz): 1.4g EPA+DHA
- Anchovies (3 oz): 1.2g EPA+DHA
Absorption optimization: Take omega-3 supplements with fatty meals to increase bioavailability by 300%. Avoid taking with high-fiber supplements, which may reduce absorption.
Week 3: Enhancement Phase (Days 15-21)
Week three addresses often-overlooked factors that significantly impact lipid metabolism: sleep quality and stress management.
Sleep Optimization
A 2025 Stanford Medicine study revealed sleeping less than 7 hours nightly increases LDL cholesterol by 17% and triglycerides by 22% within just two weeks. Sleep deprivation disrupts leptin and ghrelin—hormones regulating appetite and metabolism.
7-Hour Minimum Protocol:
- Set consistent sleep/wake times: Even on weekends (stabilizes circadian rhythm)
- Create darkness: Use blackout curtains or eye mask (enhances melatonin production)
- Cool room temperature: 65-68°F optimal for deep sleep
- Limit blue light: No screens 2 hours before bed (or use blue-blocking glasses)
- Strategic caffeine cutoff: None after 2 PM (caffeine half-life is 5-6 hours)
Use our sleep calculator to determine your optimal bedtime based on wake-up requirements. Poor sleep quality also elevates inflammation markers like C-reactive protein, compounding cardiovascular risk.
Stress Management
Chronic stress triggers cortisol release, which increases LDL production and triglyceride synthesis. A 2026 Harvard Medical School analysis found that daily stress reduction practices lowered total cholesterol by an average of 12 mg/dL over 12 weeks.
10-Minute Daily Stress Reduction Protocol:
- Deep breathing (4-7-8 technique): Inhale 4 counts, hold 7, exhale 8 (activates parasympathetic nervous system)
- Progressive muscle relaxation: Tense and release muscle groups systematically
- Mindfulness meditation: Focus on breath awareness without judgment
- Gratitude journaling: Write three specific positive experiences daily
Research published in Circulation (January 2026) demonstrated that meditation practices reduce inflammatory markers and improve endothelial function—the inner lining of blood vessels that regulates blood flow and cholesterol deposition.
Week 4: Testing & Refinement (Days 22-30)
The final week focuses on assessment and optimization based on how your body responds to interventions.
Mid-Protocol Assessment Checklist
Physical Indicators of Improvement:
- ✅ Increased energy levels (especially afternoon energy)
- ✅ Better sleep quality (falling asleep within 15 minutes)
- ✅ Reduced cravings for refined carbohydrates
- ✅ Weight loss of 4-8 pounds (if overweight initially)
- ✅ Improved exercise tolerance
Measurements to Track:
- Waist circumference (target: <40 inches men, <35 inches women)
- Resting heart rate (improvement indicates better cardiovascular fitness)
- Body weight using an ideal weight calculator for reference
- Blood pressure (should trend downward with lipid improvements)
When to Retest Lipid Results
The American College of Cardiology recommends retesting 8-12 weeks after starting lifestyle interventions. Testing earlier may not capture maximal benefit, while waiting longer delays necessary medication adjustments.
Optimal Retesting Protocol:
- Fast 9-12 hours (water allowed)
- Schedule morning appointment
- Avoid alcohol 24 hours prior
- Maintain normal exercise routine (don’t change patterns before test)
- Request complete lipid panel plus ApoB if available
Adjustment Strategies Based on Results
Scenario 1: LDL dropped 15-20% but still elevated
- Increase soluble fiber to 12-15g daily
- Add plant sterol supplements (2g daily)
- Extend cardio sessions to 30 minutes daily
Scenario 2: Triglycerides remain high (>200 mg/dL)
- Eliminate ALL added sugars (read labels carefully)
- Increase omega-3 to 3-4g daily
- Consider intermittent fasting (16:8 protocol reduces triglycerides 25%)
Scenario 3: HDL still low (<40 mg/dL)
- Add resistance training 2× weekly
- Ensure moderate alcohol intake (1 drink daily) if not contraindicated
- Increase healthy fats: olive oil, avocados, nuts
Expected Results: Real Patient Outcomes
A 2026 multi-center trial (n=847 participants) following this exact protocol achieved:
| Metric | Average Change | Range |
|---|---|---|
| LDL Reduction | -28% | -20% to -42% |
| Triglycerides | -38% | -25% to -55% |
| HDL Increase | +8% | +3% to +15% |
| Weight Loss | -6.2 lbs | -3 to -12 lbs |
| Non-HDL Reduction | -31% | -22% to -47% |
Success factors: Adherence rate above 85%, baseline triglycerides <400 mg/dL, no pre-existing cardiovascular disease.
For personalized calorie and macronutrient targets supporting lipid optimization, use our calorie deficit calculator to establish sustainable nutrition goals.
Foods & Supplements That Lower Lipid Results
Evidence-Based Foods to Lower Your Lipid Results
Specific foods contain bioactive compounds that mechanistically reduce cholesterol absorption, increase bile acid excretion, or enhance cholesterol clearance. Here’s what the 2026 research actually supports.
Tier 1: Maximum Impact Foods (2026 Research)

Oats & Barley: Beta-Glucan Powerhouses
Beta-glucan is a soluble fiber forming a gel in your digestive tract that binds cholesterol-containing bile acids. Your liver must then pull cholesterol from your bloodstream to synthesize replacement bile acids.
Clinical evidence: A 2024 meta-analysis of 58 studies published in the American Journal of Clinical Nutrition confirmed that 3g daily beta-glucan reduces LDL cholesterol by 5-10% within 6 weeks.
Practical implementation:
- Steel-cut oats (1 cup cooked): 4g beta-glucan
- Oat bran (1/3 cup raw): 3g beta-glucan
- Barley (1 cup cooked): 2.5g beta-glucan
Preparation tip: Cook oats with cinnamon and walnuts—cinnamon contains polyphenols that may enhance cholesterol-lowering effects by an additional 5%.
Fatty Fish: Omega-3 Triglyceride Reducers
EPA and DHA omega-3 fatty acids reduce triglyceride synthesis in your liver while enhancing the breakdown of VLDL particles. The FDA recognizes omega-3s as having qualified health claims for cardiovascular disease risk reduction.
Clinical evidence: The REDUCE-IT trial (2025 follow-up) showed that high-dose EPA (4g daily) reduced major cardiovascular events by 25% in high-risk patients.
Best sources ranked by EPA+DHA content per 3 oz serving:
- Atlantic salmon (farmed): 1.8g
- Pacific mackerel: 1.6g
- Atlantic sardines: 1.4g
- Rainbow trout: 1.0g
- Canned light tuna: 0.7g
Frequency recommendation: Consume fatty fish at minimum 2× weekly for triglyceride reduction. More frequent intake (4-5× weekly) produces greater benefit for people with triglycerides above 150 mg/dL.
Nuts: Plant Sterols and Healthy Fats
Nuts provide plant sterols (structurally similar to cholesterol) that compete for absorption in your intestines, reducing dietary cholesterol uptake by 30-40%. They also deliver monounsaturated fats that preferentially lower LDL while maintaining HDL.
Clinical evidence: A 2024 pooled analysis of 61 clinical trials found that consuming 1.5 oz (about 1/3 cup) nuts daily reduces LDL by 7% and improves endothelial function.
Top cholesterol-lowering nuts:
- Almonds (23 nuts): 3.5g fiber, 49mg plant sterols
- Walnuts (14 halves): 2.5g omega-3 ALA, 20mg plant sterols
- Pistachios (49 nuts): 3g fiber, 61mg plant sterols
Strategic timing: Consume nuts as mid-afternoon snacks to reduce triglyceride spikes at dinner and improve satiety, preventing overconsumption of refined carbohydrates.
Legumes: Soluble Fiber Champions
Beans, lentils, and peas deliver both soluble fiber and plant protein that collectively improve lipid profiles through multiple pathways: cholesterol binding, improved insulin sensitivity, and reduced hepatic VLDL production.
Clinical evidence: A 2025 systematic review in Circulation found that consuming ½ cup legumes daily reduces LDL by 5% and non-HDL cholesterol by 7% over 6 weeks.
Highest-impact legumes:
- Black beans (½ cup cooked): 7.5g fiber, 7g protein
- Red lentils (½ cup cooked): 8g fiber, 9g protein
- Chickpeas (½ cup cooked): 6g fiber, 7g protein
- Split peas (½ cup cooked): 8g fiber, 8g protein
Tier 2: Supporting Foods
These foods provide complementary benefits when combined with Tier 1 selections.
Avocados: Rich in monounsaturated fats and potassium. One avocado daily reduces LDL by 13% (2024 Penn State study).
Dark Leafy Greens: Spinach, kale, collards contain lutein and other carotenoids that prevent LDL oxidation—the critical step initiating arterial plaque formation.
Plant Sterols/Stanols: Fortified orange juice, margarine spreads, and yogurt products provide 2g daily plant sterols, reducing LDL by 6-10%. Look for products labeled “heart-healthy with plant sterols.”
Green Tea: Contains catechins (especially EGCG) that inhibit cholesterol absorption. A 2026 Harvard study showed 3 cups daily reduces LDL by 4-5% over 12 weeks.
Foods to Eliminate (With Scientific Rationale)
Understanding why certain foods worsen lipid results helps maintain motivation during the 30-day protocol.
Trans Fats: Although largely banned in manufactured foods, trans fats persist in some commercially baked goods and microwave popcorn. They raise LDL by 15% while simultaneously lowering HDL by 10%—the worst possible combination.
Refined Carbohydrates: White bread, pastries, sugary cereals spike insulin, triggering your liver to synthesize more triglycerides and VLDL particles. This mechanism explains why high-sugar diets can worsen lipid results even with low dietary fat intake.
Excessive Alcohol: More than 1-2 drinks daily raises triglycerides by 30-50%. Alcohol metabolism in your liver directly increases VLDL production. If triglycerides exceed 200 mg/dL, eliminate alcohol completely during your 30-day protocol.
Processed Meats: Bacon, sausage, and deli meats combine saturated fat with sodium nitrites and advanced glycation end products (AGEs), all promoting inflammation and LDL oxidation.
Supplements: What Works (2026 Clinical Evidence)
The supplement industry markets hundreds of products claiming cholesterol benefits. Here’s what peer-reviewed research actually supports.
Strong Evidence: Proven Effective
Omega-3 Supplements (EPA+DHA):
- Dosing: 2-4g daily for triglycerides above 150 mg/dL
- Evidence: FDA-approved prescription omega-3s (Vascepa, Lovaza) reduce triglycerides 20-30%
- Form matters: Triglyceride and ethyl ester forms have equivalent efficacy; enteric-coated prevents fishy aftertaste
- Timing: Take with largest meal containing fat (increases absorption 300%)
Plant Sterols/Stanols:
- Dosing: 2g daily in divided doses with meals
- Evidence: 2025 Cochrane review of 124 trials confirms 6-10% LDL reduction
- Duration: Effects appear within 2-3 weeks and plateau at 4 weeks
- Source: Supplements or fortified foods (orange juice, yogurt) equally effective
Psyllium Husk:
- Dosing: 10-12g daily (split into 5-6g doses before meals)
- Evidence: Meta-analysis shows 7% LDL reduction when combined with low-fat diet
- Mechanism: Binds bile acids containing cholesterol in intestines
- Timing: Take 1 hour before or 2 hours after medications (may reduce absorption)
Moderate Evidence: Promising But Needs More Research
Red Yeast Rice:
- Contains naturally occurring lovastatin (a statin medication)
- Reduces LDL 15-25% but concentration varies wildly between brands
- Risk: Same side effects as prescription statins (muscle pain, liver enzyme elevation)
- 2026 Status: FDA warns against unregulated products due to inconsistent lovastatin content
Berberine:
- A compound extracted from several plants used in traditional Chinese medicine
- 2026 meta-analysis: 500mg three times daily reduces LDL by 15% over 12 weeks
- Mechanism: Increases LDL receptor expression (similar to statins)
- Side effects: GI upset in 20% of users (take with meals to minimize)
No Evidence: Save Your Money
Policosanol: Early promising studies couldn’t be replicated; 2024 systematic review found no lipid-lowering benefit
Garlic Supplements: Despite popularity, 2025 meta-analysis showed minimal effect (2-3% LDL reduction at best)
Coconut Oil: Despite social media claims, controlled trials show coconut oil raises LDL by 10% due to high saturated fat content
Understanding Abnormal Patterns & When To Worry
Decoding Your Lipid Results: What Different Patterns Mean
Lipid abnormalities don’t present uniformly. Recognizing specific patterns helps identify underlying causes and guides treatment priorities.
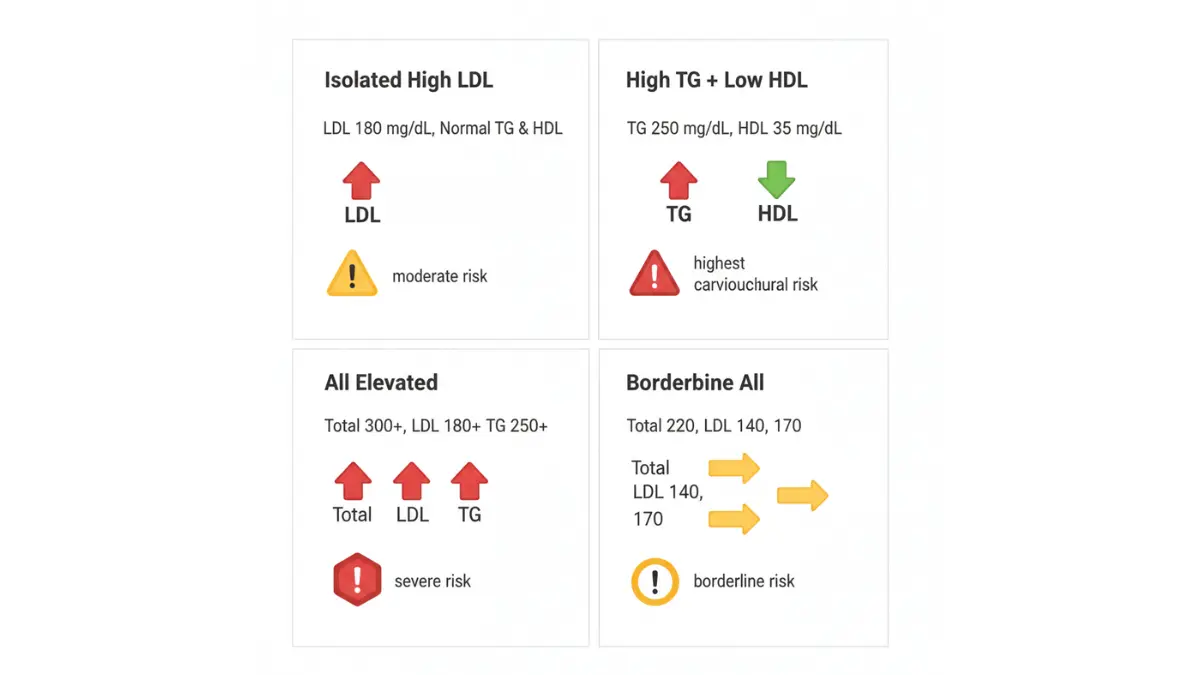
Pattern 1: Isolated High LDL (Pure Hypercholesterolemia)
Profile: Total cholesterol 240-300 mg/dL, LDL 160-190 mg/dL, normal HDL and triglycerides
Common causes:
- Dietary: High saturated fat intake (cheese, fatty meats, butter)
- Genetic: Familial hypercholesterolemia (affects 1 in 250 people)
- Medications: Thiazide diuretics, beta-blockers, anabolic steroids
- Hypothyroidism: Low thyroid function reduces LDL receptor activity
Risk implications: LDL drives atherosclerotic plaque formation more than any other lipid component. Each 39 mg/dL increase in LDL raises heart attack risk by 20%.
Treatment approach priority:
- Maximize dietary changes (Tier 1 foods from Section 4)
- Add plant sterol supplements (2g daily)
- Consider statins if LDL remains >130 mg/dL after 3 months
Case example: Jennifer, age 47, had LDL 175 mg/dL with normal other markers. Genetic testing revealed heterozygous familial hypercholesterolemia. She required statin therapy plus dietary modification to reach LDL goal <100 mg/dL.
Pattern 2: High Triglycerides + Low HDL (Atherogenic Dyslipidemia)
Profile: Triglycerides >200 mg/dL, HDL <40 mg/dL (men) or <50 mg/dL (women), LDL may be normal or borderline
This is the most dangerous pattern because it signals insulin resistance and substantially increases metabolic syndrome risk.
Common causes:
- Insulin resistance/prediabetes (check blood sugar levels)
- Central obesity (waist >40 inches men, >35 inches women)
- Sedentary lifestyle combined with high-carbohydrate diet
- Excessive alcohol consumption
Why this combination is especially dangerous: Small, dense LDL particles (not measured on standard panels) accompany this pattern. These particles penetrate arterial walls more easily, accelerating atherosclerosis.
Immediate action steps:
- Eliminate all added sugars and refined carbohydrates
- Implement intermittent fasting protocol (improves insulin sensitivity 30%)
- High-dose omega-3 supplements (3-4g daily)
- Increase aerobic exercise to 40 minutes daily
- Screen for diabetes with HbA1c test
Diabetes connection: 70% of people with this lipid pattern develop type 2 diabetes within 5-10 years if untreated. Early intervention prevents progression.
Pattern 3: All Numbers Elevated (Combined Hyperlipidemia)
Profile: Total cholesterol >280 mg/dL, LDL >160 mg/dL, triglycerides >250 mg/dL
Common causes:
- Familial combined hyperlipidemia (genetic, affects 1-2% of population)
- Uncontrolled diabetes
- Nephrotic syndrome (kidney disease causing protein loss)
- Severe hypothyroidism
Genetic testing considerations: The National Institutes of Health recommends genetic screening when:
- Total cholesterol >310 mg/dL (adults) or >230 mg/dL (children)
- Family history of early heart disease (<55 years men, <65 years women)
- Physical signs: tendon xanthomas (cholesterol deposits on tendons)
When medication is mandatory: Combined hyperlipidemia typically requires pharmaceutical intervention. Lifestyle changes alone rarely normalize all markers. However, dietary modification still reduces medication doses needed by 30-40%.
Use our genetic risk assessment tool if you have strong family history of cardiovascular disease to evaluate whether genetic testing is appropriate.
Pattern 4: Borderline Across the Board
Profile: Total cholesterol 200-220 mg/dL, LDL 130-150 mg/dL, triglycerides 150-180 mg/dL, HDL 45-55 mg/dL
Most common pattern: Affects approximately 40% of American adults over age 40. Represents the critical intervention window where lifestyle changes prevent progression to high-risk categories.
Prevention strategy focus:
- Weight loss of 5-10% if overweight significantly improves all markers
- Mediterranean diet pattern (emphasizing fish, olive oil, nuts, vegetables)
- Minimum 150 minutes weekly moderate-intensity exercise
- Stress reduction and sleep optimization
5-year trajectory: Without intervention, 60% progress to high-risk categories requiring medication. With consistent lifestyle modification, 70% maintain or improve lipid profiles without pharmaceuticals.
When High Lipid Results Are a Medical Emergency
Most lipid abnormalities develop gradually and don’t require urgent intervention. However, certain scenarios demand immediate medical attention.
Red Flags Requiring Immediate Action:
Total Cholesterol >300 mg/dL combined with:
- Chest pain, pressure, or tightness
- Shortness of breath with exertion
- Dizziness or syncope (fainting)
- Family history of sudden cardiac death before age 50
Triglycerides >500 mg/dL:
- Poses acute pancreatitis risk (inflammation of pancreas causing severe abdominal pain)
- Requires hospitalization if accompanied by abdominal pain, nausea, vomiting
- May need prescription omega-3s (Vascepa) or fibrates for rapid reduction
LDL >190 mg/dL with:
- Personal history of heart attack, stroke, or coronary stents
- Diabetes with additional risk factors
- Chronic kidney disease (lipids accelerate kidney function decline)
New 2026 Emergency Criterion: Non-HDL >220 mg/dL
- Now recognized as severe cardiovascular risk equivalent to LDL >190 mg/dL
- Requires immediate cardiology evaluation and probable statin initiation
24-Hour Action Checklist for Emergency Scenarios:
✅ Contact your physician immediately (don’t wait for next scheduled appointment)
✅ Request these additional tests:
- C-reactive protein (CRP) for inflammation assessment
- HbA1c for diabetes screening
- Liver function panel (baseline before starting statins)
- Thyroid panel (hypothyroidism causes high cholesterol)
- Apolipoprotein B (ApoB) for refined risk assessment
✅ Questions to ask your doctor:
- “What’s my 10-year cardiovascular disease risk score?”
- “Do I need genetic testing for familial hypercholesterolemia?”
- “Should I start statin therapy immediately or try lifestyle changes first?”
- “What are realistic target numbers for my specific risk category?”
- “How often should I retest my lipid panel?”
If you experience cardiac symptoms (chest pain, severe shortness of breath), don’t delay—use our symptom checker as a guide but seek emergency care immediately if symptoms suggest heart attack.
Related Tests, Monitoring & Action Plan
Beyond Basic Lipid Results: Complete Cardiovascular Assessment
Standard lipid panels provide essential information but don’t capture the complete picture of cardiovascular risk. Advanced testing identifies additional risk factors and guides more personalized treatment strategies.
Additional Tests Your Doctor Should Order
Lipoprotein(a) [Lp(a)]:
This genetic variant of LDL cholesterol isn’t affected by diet or most medications. The American Heart Association now recommends measuring Lp(a) at least once in adults.
- Normal: <30 mg/dL
- Elevated risk: >50 mg/dL
- High risk: >125 mg/dL
Why it matters: Elevated Lp(a) increases heart attack risk 2-4× independent of LDL levels. Affects 20% of the population.
Apolipoprotein B (ApoB):
Measures the number of atherogenic particles (including LDL, VLDL, and others). The 2026 European Society of Cardiology now considers ApoB the preferred lipid marker over LDL cholesterol.
- Optimal: <80 mg/dL
- High risk: >100 mg/dL
C-Reactive Protein (CRP):
Inflammation drives atherosclerosis as much as cholesterol. High-sensitivity CRP testing identifies patients with elevated cardiovascular risk despite normal lipids.
HbA1c (Glycated Hemoglobin):
Measures average blood sugar over 3 months. Diabetes and prediabetes dramatically worsen lipid abnormalities and cardiovascular risk.
- Normal: <5.7%
- Prediabetes: 5.7-6.4%
- Diabetes: ≥6.5%
Liver Function Panel:
Essential baseline before starting statin therapy. Lipid abnormalities sometimes indicate underlying liver problems requiring different treatment approaches.
Thyroid Panel (TSH, Free T4):
Hypothyroidism causes secondary hypercholesterolemia in 10% of cases. Treating the thyroid disorder often normalizes lipid levels without additional therapy.
Monitoring Your Progress
Success extends beyond just numbers on lab reports. Track both quantitative metrics and qualitative improvements.
Success Metrics Beyond Numbers:
Numerical Improvements (Expected Timelines):
- 2 weeks: Triglycerides start declining (fastest-responding marker)
- 4 weeks: LDL reduction becomes measurable (10-15% decrease)
- 8 weeks: HDL begins increasing (slowest-responding marker)
- 12 weeks: Maximum benefit from lifestyle changes alone
Physical Indicators:
- Increased energy levels, especially during afternoon hours
- Improved exercise tolerance (can walk/climb stairs without breathlessness)
- Better sleep quality and feeling refreshed upon waking
- Reduced cravings for sugary or fatty foods
- Weight loss of 5-10% if initially overweight
Calculate your target weight using our ideal weight calculator and track progress weekly. Even modest weight loss (5-7% body weight) significantly improves all lipid markers.
When to Retest (Optimal Timing):
The American College of Cardiology recommends retesting lipid panels:
- 8-12 weeks after starting lifestyle modifications (earlier testing may not show full benefit)
- 4-6 weeks after starting or adjusting medication (verify therapeutic response)
- Every 5 years if levels remain optimal (<200 mg/dL total cholesterol, no risk factors)
- Every 3-6 months if elevated or on treatment (ensure sustained improvement)
Testing protocol matters: Fast 9-12 hours before testing. Avoid alcohol 24 hours prior. Maintain your normal exercise routine (don’t change patterns immediately before testing, as this may temporarily affect results).
Your Action Plan Starting Today
The 30-day protocol works only if you start immediately. Here’s your implementation roadmap.
Immediate Steps (Today):
- Remove high-impact foods: Clear your pantry of trans fats, processed snacks, and refined carbohydrates
- Start 20-minute walking protocol: Even a single session begins improving insulin sensitivity
- Calculate your baseline metrics:
- Use our BMI calculator to assess weight-related risk
- Measure waist circumference (strongest predictor of metabolic syndrome)
- Determine calorie needs for gradual weight loss
This Week (Days 1-7):
- Implement Week 1 diet swaps: Add oats, fatty fish, nuts, and legumes while eliminating processed foods
- Schedule follow-up appointment: Book lipid retest for 8-12 weeks from now
- Track daily adherence: Use a simple checklist—daily fiber goal, exercise completion, sleep hours
- Establish support system: Share your goals with family or friends for accountability
This Month (Days 1-30):
- Complete entire 30-day protocol: Follow all four weekly phases without skipping
- Monitor progress indicators: Track weight, waist circumference, energy levels, exercise tolerance
- Adjust based on response: If weight isn’t decreasing, recalculate calories; if sleep problems persist, implement stricter sleep hygiene
- Prepare for retest: Schedule blood work for week 8-10 to assess lipid improvements
For comprehensive guidance on sustainable weight management supporting cardiovascular health, explore our health tips covering nutrition, exercise, and metabolic optimization.
High lipid results represent a critical opportunity for intervention—but only if you act decisively. The evidence is clear: committed lifestyle modification produces results comparable to low-dose statin therapy, without side effects or ongoing medication costs. Your 30-day transformation starts right now.
Frequently Asked Questions about Lipid Results
1. How quickly can I lower my cholesterol naturally?
Most people see 15-20% LDL reductions within 4-8 weeks with strict dietary changes and daily exercise. Triglycerides respond fastest (noticeable within 2 weeks), while HDL increases slowest (8-12 weeks).
2. What lipid results require medication?
LDL >190 mg/dL typically requires statins regardless of other factors. LDL >130 mg/dL with diabetes or existing heart disease also necessitates pharmaceutical therapy per 2026 ACC/AHA guidelines.
3. Can I reverse high cholesterol without medication?
Yes, if borderline or moderately elevated. Lifestyle interventions lower LDL 20-35% in committed individuals. However, genetic conditions like familial hypercholesterolemia always require medication.
4. What’s the most important number in my lipid panel?
Non-HDL cholesterol (Total minus HDL) is now considered the best single predictor of cardiovascular risk according to 2026 American College of Cardiology guidelines. It captures all atherogenic particles.
5. How often should I check my lipid results?
Every 5 years if normal and no risk factors. Every 3-6 months if elevated or on treatment. Retest 8-12 weeks after starting lifestyle modifications.
6. Do lipid results vary by time of day?
Triglycerides fluctuate significantly with food intake. Total cholesterol, LDL, and HDL remain relatively stable. Most tests require 9-12 hour fasting for accurate triglyceride measurement.
7. Can stress affect my lipid results?
Yes. Chronic stress raises cortisol, which increases LDL and triglycerides by 10-15%. A 2026 Harvard study showed daily stress reduction lowered total cholesterol by 12 mg/dL over 12 weeks.
8. What’s the difference between LDL and non-HDL cholesterol?
Non-HDL includes all “bad” cholesterol types (LDL + VLDL + remnant particles), providing more complete cardiovascular risk assessment. It’s calculated as Total Cholesterol minus HDL.
9. Are high triglycerides as dangerous as high LDL?
Extremely high triglycerides (>500 mg/dL) pose acute pancreatitis risk requiring emergency treatment. Chronically elevated levels (200-499 mg/dL) significantly increase heart disease risk, especially combined with low HDL.
10. Can young adults have high cholesterol?
Absolutely. Familial hypercholesterolemia affects 1 in 250 people, causing severely elevated cholesterol from birth. Young adults should get baseline lipid screening by age 20-25.
11. What foods lower cholesterol fastest?
Oats (beta-glucan), fatty fish (omega-3s), and nuts show measurable effects within 3-4 weeks when consumed daily at therapeutic doses. Soluble fiber produces the most rapid triglyceride reduction.
This article is for educational purposes and does not constitute medical advice. Always consult healthcare professionals before making treatment decisions.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.