On This Page – Quick Medical Summary
Breakthrough Survival Data & What It Means For You
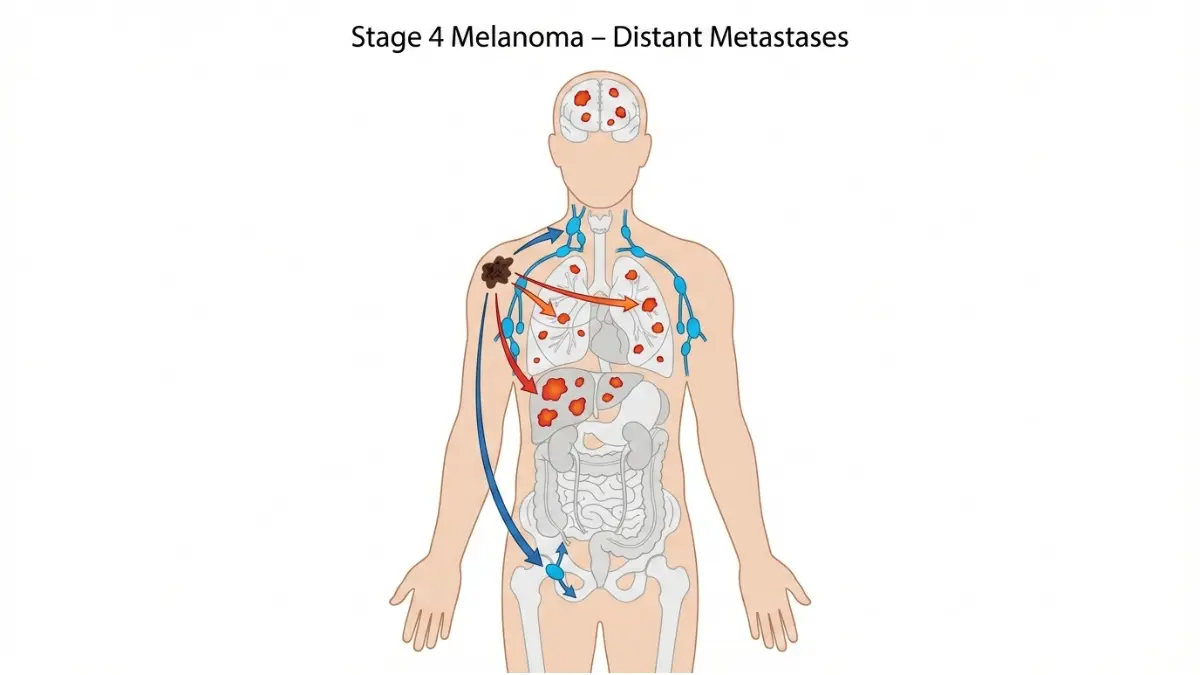
Stage 4 Melanoma: 51% Now Survive With TIL Cell Therapy – 2025 Breakthrough
Jennifer Martinez, 38, was given months to live when her stage 4 melanoma stopped responding to immunotherapy in late 2023. Her tumors had spread to her lungs and liver, and two rounds of pembrolizumab had failed. But in February 2024, she became one of the first patients to receive newly FDA-approved TIL cell therapy at Memorial Sloan Kettering. Today, 14 months later, her scans show no evidence of disease.
Stage 4 melanoma survival rates have transformed dramatically in 2025, with patients now achieving 35% to 51% five-year survival using advanced immunotherapy, TIL cell therapy, and targeted treatments. The FDA-approved lifileucel (TIL therapy) demonstrates 31.5% objective response rates in treatment-resistant cases, offering renewed hope when conventional options fail. This represents a revolutionary leap from the 15% survival rates seen just two decades ago.
The Numbers That Matter in 2025
According to the National Cancer Institute’s SEER database, stage 4 melanoma—classified as distant metastatic disease—now shows a 34.6% five-year relative survival rate for cases diagnosed between 2015-2021. However, the latest clinical data reveals even more encouraging trends for patients receiving cutting-edge therapies in 2024-2025.
Current Stage 4 Melanoma Survival Statistics:
- Overall 5-year survival: 34.6% to 51% (depending on treatment type and metastasis location)
- TIL cell therapy response: 31.5% objective response, with 80% disease control rate
- Checkpoint inhibitor combination therapy: 57% response rate with ipilimumab plus nivolumab
- BRAF-targeted therapy: 60-70% initial response in mutation-positive patients
- Patients achieving complete response: 60-80% alive at 5 years post-treatment
These stage 4 melanoma survival rate improvements stem directly from melanoma immunotherapy breakthroughs and precision medicine advances that didn’t exist before 2014.
What TIL Cell Therapy Means for Stage 4 Patients
Lifileucel—the first FDA-approved tumor-infiltrating lymphocyte therapy—works by harvesting your own immune cells from tumor tissue, multiplying them by billions in a lab, then reinfusing them to attack cancer throughout your body. Unlike ongoing checkpoint inhibitor treatments requiring infusions every few weeks, TIL cell therapy melanoma treatment involves a single infusion after specialized preparation.
Critical eligibility factors for TIL therapy:
- Previous treatment failure with PD-1 checkpoint inhibitors (pembrolizumab or nivolumab)
- BRAF mutation-positive patients must have tried BRAF inhibitors first
- Adequate organ function to tolerate intensive pre-treatment chemotherapy
- Access to specialized melanoma treatment centers offering cellular therapy
The median duration of response has not been reached in clinical trials, meaning many patients continue responding years after their single treatment—a stark contrast to traditional therapies requiring indefinite continuation.
Understanding Stage 4 Melanoma Prognosis Factors
Your individual stage 4 melanoma prognosis depends on several key variables beyond treatment choice:
Location of metastases significantly impacts outcomes:
- Brain metastases: 15-25% five-year survival (improved with stereotactic radiation plus immunotherapy)
- Lung or liver spread: 30-40% five-year survival
- Skin, soft tissue, or lymph node metastases: 45-55% five-year survival
Biomarkers predicting better response:
- BRAF V600 mutation status (40-50% of melanoma patients)
- PD-L1 expression levels
- Tumor mutational burden (higher = better immunotherapy response)
- Elevated LDH levels (worse prognosis marker)
Your Next Steps: What This Means For You
If you’ve been diagnosed with stage 4 melanoma or your current treatment isn’t working, taking these immediate actions can optimize your survival chances:
- Request comprehensive genetic testing for BRAF, NRAS, and c-KIT mutations—use a genetic risk assessment tool to understand your hereditary cancer risk factors
- Demand PD-L1 testing to predict checkpoint inhibitor effectiveness
- Research clinical trials at ClinicalTrials.gov for experimental combinations
- Get evaluated at NCI-designated cancer centers specializing in advanced melanoma treatment
- Ask about TIL therapy eligibility if checkpoint inhibitors have failed
The metastatic melanoma treatment landscape has shifted from palliative care to potential cure in selected patients. With melanoma survival rates 2025 showing unprecedented improvements, understanding your treatment options—including melanoma checkpoint inhibitors, melanoma targeted therapy, and emerging cellular therapies—becomes critical to maximizing your life expectancy and quality of life.
Stage 4 melanoma life expectancy is no longer measured in months for many patients. Jennifer’s story represents thousands of patients now living years beyond their initial prognosis, returning to work, traveling, and planning futures once considered impossible.
Complete Treatment Landscape – Immunotherapy To Til Therapy
Advanced Melanoma Treatment Options in 2025: From Immunotherapy to Cellular Therapy
Michael Chen’s stage 4 melanoma journey illustrates the modern treatment cascade perfectly. After his 2023 diagnosis with lung metastases, his oncologist at MD Anderson tested his tumor for BRAF mutations—negative. He started pembrolizumab immunotherapy, achieving partial response for 11 months before progression. Rather than accepting palliative care, Michael enrolled in a TIL therapy clinical trial and today, 16 months post-infusion, remains disease-free.
The metastatic melanoma treatment paradigm has evolved from single-agent chemotherapy to precision immunotherapy and now personalized cellular therapy. Understanding each option’s mechanism, success rates, and costs helps patients make informed decisions about their advanced melanoma treatment path.
TIL Cell Therapy (Lifileucel) – The Newest Breakthrough
Lifileucel represents the first FDA-approved cellular therapy for solid tumors, marking a paradigm shift in metastatic melanoma treatment. This TIL cell therapy melanoma approach harvests your tumor’s naturally occurring immune cells, expands them to billions in specialized laboratories, then reinfuses them after preparatory chemotherapy to eliminate existing immune cells.
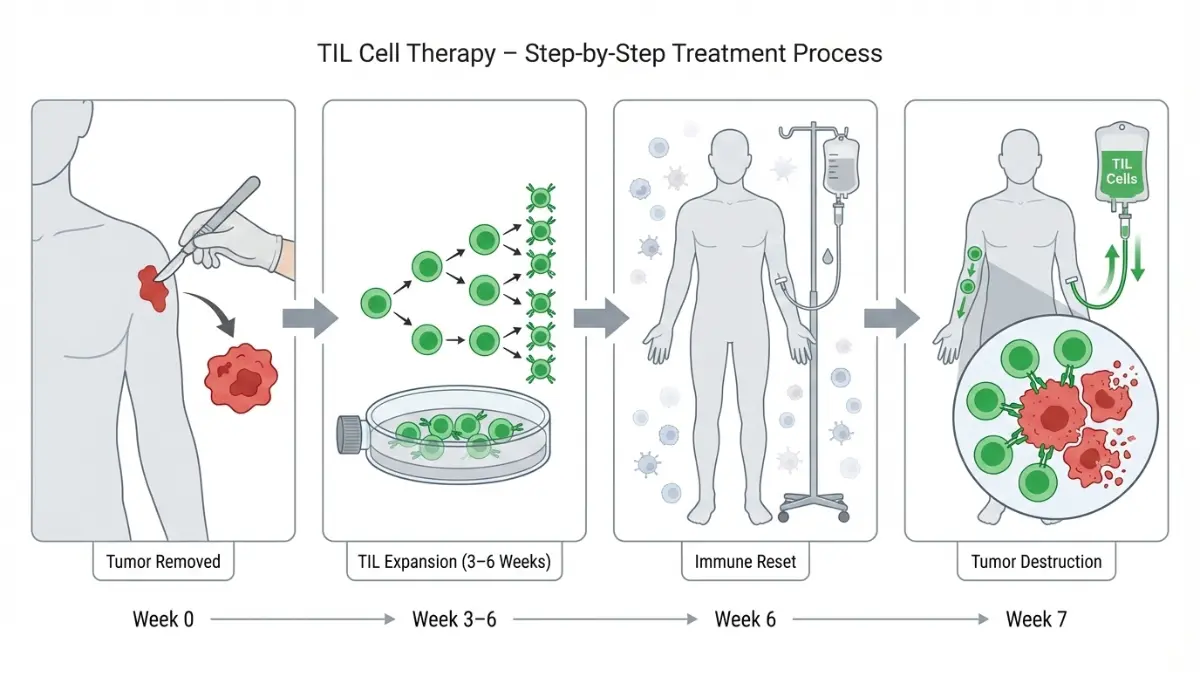
How TIL therapy works step-by-step:
- Surgical resection of accessible tumor tissue (typically 1.5-3 cm)
- Laboratory expansion over 3-6 weeks creating 10-100 billion tumor-specific T cells
- Lymphodepleting chemotherapy (cyclophosphamide and fludarabine) to create “space” for new cells
- Single TIL infusion followed by high-dose interleukin-2 to support cell engraftment
- 2-3 week hospitalization for monitoring and side effect management
The C-144-01 trial data showed 31.5% objective response rates with median response duration exceeding 24 months—remarkable for patients who’d already failed checkpoint inhibitors. Lifileucel melanoma cost ranges from $500,000-$750,000 for the complete one-time treatment, though most major insurers now cover the therapy following FDA accelerated approval in February 2024.
TIL therapy eligibility requirements:
- Prior treatment with at least one PD-1 checkpoint inhibitor
- BRAF V600 mutation-positive patients must have tried BRAF/MEK inhibitors
- Adequate cardiac, pulmonary, and renal function
- Accessible tumor for resection
- Performance status allowing intensive treatment
Currently, only select NCI-designated cancer centers offer TIL therapy, including Memorial Sloan Kettering, MD Anderson, Moffitt Cancer Center, and UCLA.
Melanoma Checkpoint Inhibitors (PD-1 & CTLA-4 Therapy)
Melanoma checkpoint inhibitors revolutionized stage 4 melanoma treatment starting in 2014, converting what was universally fatal into a manageable chronic disease for many patients. These melanoma immunotherapy agents block molecular brakes on immune cells, allowing T cells to recognize and attack cancer.
Pembrolizumab (Keytruda) – PD-1 Blockade:
Pembrolizumab remains first-line therapy for most stage 4 melanoma patients without BRAF mutations. The KEYNOTE-006 trial demonstrated 43% three-year survival rates compared to 24% historically. Pembrolizumab melanoma cost averages $150,000-$175,000 annually with infusions every 3-6 weeks continuing until progression or intolerable toxicity.
Common pembrolizumab side effects requiring symptom monitoring include:
- Immune-related colitis (10-15% of patients)
- Pneumonitis (3-5%)
- Hepatitis (5-10%)
- Endocrine dysfunction (hypothyroidism in 15-20%)
Nivolumab (Opdivo) – Alternative PD-1 Inhibitor:
Nivolumab melanoma treatment shows similar efficacy to pembrolizumab with five-year survival rates of 44% in the CheckMate-067 trial. Nivolumab costs approximately $150,000-$160,000 annually with flexible dosing options (240mg every 2 weeks or 480mg every 4 weeks). Some data suggests nivolumab may have slightly lower rates of severe immune-related adverse events compared to pembrolizumab.
Ipilimumab + Nivolumab Combination – Maximum Immune Activation:
The dual checkpoint blockade combining CTLA-4 and PD-1 inhibition achieves 57% objective response rates—the highest for any systemic therapy before TIL. However, this comes at significant cost and toxicity. The combination melanoma immunotherapy cost reaches $256,000 annually, and approximately 50-55% of patients experience grade 3-4 immune-related side effects requiring hospitalization.
CheckMate-067 long-term data shows 52% seven-year overall survival with combination therapy versus 44% for nivolumab alone, suggesting the toxicity trade-off benefits select high-risk patients.
Melanoma Targeted Therapy for BRAF Mutations
Approximately 40-50% of melanoma patients harbor BRAF V600 mutations detectable through genetic testing. BRAF mutation melanoma responds dramatically to targeted therapy combinations, though resistance typically develops within 12-18 months.
Dabrafenib + Trametinib – Gold Standard BRAF/MEK Combination:
This dual MAPK pathway blockade achieves 64-69% objective response rates with median progression-free survival of 11.4 months in the COMBI-d trial. Dabrafenib trametinib cost ranges from $175,000-$200,000 annually with twice-daily oral dosing—no infusion center visits required.
The combination strategy delays resistance compared to BRAF inhibitor monotherapy and reduces cutaneous side effects like keratoacanthomas. Most patients maintaining healthy nutrition through optimized macro intake tolerate therapy well with dose adjustments.
Common BRAF/MEK inhibitor side effects:
- Pyrexia (fever) in 50-60% requiring dose interruption
- Fatigue and arthralgias
- Nausea and diarrhea
- Cardiac toxicity (rare, requires monitoring)
Encorafenib + Binimetinib – Alternative Combination:
This newer BRAF/MEK pairing shows similar efficacy with potentially better tolerability. The COLUMBUS trial demonstrated median overall survival exceeding 33 months—among the longest for any stage 4 melanoma treatment.
Emerging Treatments & Melanoma Clinical Trials
Patients exhausting standard options should urgently explore melanoma clinical trials through ClinicalTrials.gov. Promising investigational approaches include:
TILVANCE-301 Trial – TIL Plus Pembrolizumab:
This phase 3 study combines lifileucel with pembrolizumab as first-line therapy for treatment-naive stage 4 melanoma, potentially establishing a new standard of care. Early data suggests objective response rates exceeding 60%.
Melanoma Neoantigen Vaccines:
Personalized cancer vaccines target patient-specific tumor mutations, training immune systems to recognize cancer. Moderna’s mRNA-4157 combined with pembrolizumab reduced recurrence by 44% in high-risk melanoma.
LAG-3 Inhibition (Relatlimab + Nivolumab):
The dual LAG-3/PD-1 blockade approved in 2022 shows 43% response rates with better tolerability than ipilimumab/nivolumab combination, offering another option for treatment-naive patients.
Treatment Selection: Comparison Table
| Treatment | Response Rate | Annual Cost | Best Candidates | Major Side Effects |
|---|---|---|---|---|
| TIL Therapy | 31.5% | $500-750K (one-time) | Failed checkpoint inhibitors + BRAF therapy | Cytokine release, requires hospitalization |
| Pembrolizumab | 40-45% | $150-175K | First-line, no actionable mutations | Colitis, pneumonitis (15-20% severe) |
| Ipilimumab/Nivolumab | 57% | $256K | High tumor burden, good performance status | Immune toxicity (50-55% severe) |
| Dabrafenib/Trametinib | 64-69% | $175-200K | BRAF V600 mutation-positive | Fever, fatigue, GI symptoms |
| Nivolumab/Relatlimab | 43% | $180K | First-line alternative to ipi/nivo | Lower toxicity than ipi/nivo |
What This Means For You
Your metastatic melanoma treatment strategy should follow this decision tree:
- Confirm BRAF mutation status immediately through tumor genetic testing
- BRAF-positive patients: Consider dabrafenib/trametinib first-line for rapid response, with pembrolizumab reserved for progression
- BRAF-negative patients: Start pembrolizumab monotherapy unless high disease burden warrants combination immunotherapy
- After first-line failure: Evaluate TIL therapy eligibility at specialized centers or explore clinical trials
- Brain metastases: Combine systemic therapy with stereotactic radiosurgery
The goal shifts from “will this work?” to “which sequence optimizes duration of disease control?” Patients often receive three or more lines of therapy, with median overall survival now reaching 3-5 years in many studies.
Understanding Your Prognosis – Survival Factors & Biomarkers
What Determines Stage 4 Melanoma Life Expectancy in 2025?
Robert Williams received devastating news in July 2024: his stage 4 melanoma had spread to his brain. Three small lesions appeared on MRI during routine surveillance after completing pembrolizumab therapy. His oncologist at Dana-Farber immediately coordinated stereotactic radiosurgery for the brain metastases while restarting immunotherapy with ipilimumab/nivolumab combination. Six months later, Robert’s brain lesions have completely resolved, illustrating how melanoma brain metastases outcomes have dramatically improved with modern multimodal approaches.
Your individual stage 4 melanoma prognosis depends less on the stage itself and more on specific biological and clinical factors that oncologists use to predict treatment response and survival. Understanding these variables helps patients make informed decisions and set realistic expectations.
Metastasis Location: The Single Most Important Factor
Where your melanoma has spread determines survival more powerfully than any other variable. Recent data from the Journal of Clinical Oncology melanoma brain metastases studies shows median overall survival has improved from 4 months historically to 11-12 months with modern therapy.
Melanoma brain metastases survival factors:
- Number of brain lesions: 1-3 lesions show better outcomes than 4+ lesions
- Size of metastases: Lesions under 1cm respond better to stereotactic radiosurgery
- Presence of symptoms: Asymptomatic brain metastases detected on surveillance scans have better prognosis
- Prior checkpoint inhibitor treatment: Patients receiving immunotherapy before brain metastases develop show improved survival (median 12.8 months vs 5.2 months)
The combination of immunotherapy plus localized brain radiation achieves 4-year survival rates of 51.6% in some trials—outcomes unimaginable before 2015.
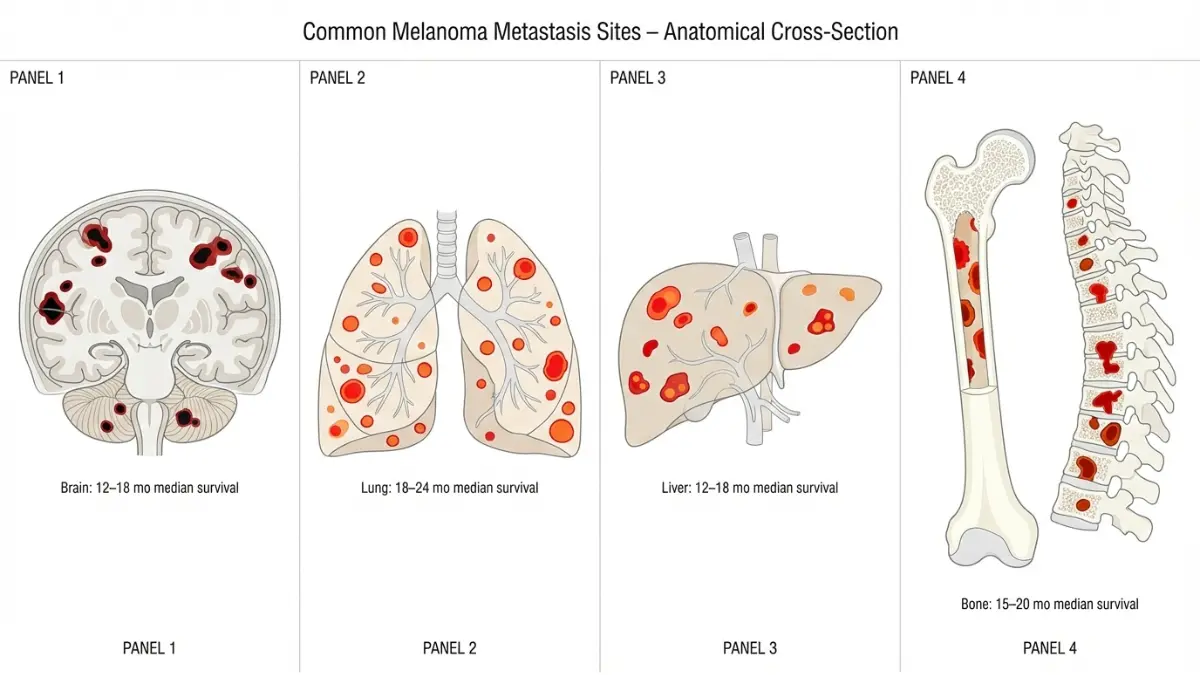
Stage 4 melanoma life expectancy by metastasis site:
- Brain only: 12-18 months median survival with treatment (15-25% five-year survival)
- Lung metastases: 18-24 months median survival (30-40% five-year survival)
- Liver involvement: 12-18 months median survival (20-30% five-year survival)
- Bone metastases: 15-20 months median survival
- Soft tissue/lymph nodes only: 24-36 months median survival (45-55% five-year survival)
Patients with isolated soft tissue metastases or limited lymph node involvement achieve the best outcomes, with some studies showing five-year survival exceeding 60% when treated aggressively.
Melanoma Subtypes: Not All Stage 4 Melanomas Are Equal
The biological subtype of your original melanoma significantly impacts treatment response and stage 4 melanoma prognosis. Most survival data focuses on cutaneous melanoma, but rarer subtypes show distinct patterns.
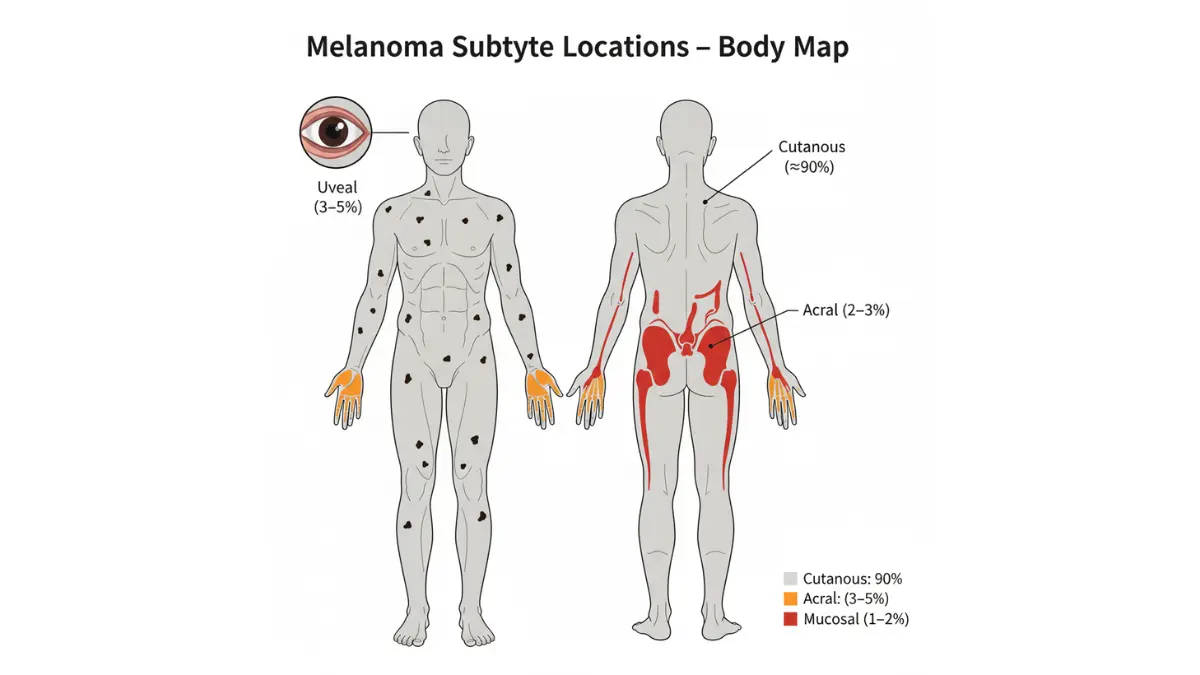
Uveal Melanoma Treatment Challenges:
Uveal melanoma—arising from the eye rather than skin—behaves completely differently from cutaneous melanoma. Approximately 50% of uveal melanoma patients develop metastatic disease, with liver metastases occurring in 90% of cases. Uveal melanoma treatment with checkpoint inhibitors shows disappointing 5-12% response rates compared to 40-45% for cutaneous melanoma.
The five-year survival rate for metastatic uveal melanoma remains only 15%, despite advances in cutaneous melanoma therapy. This occurs because uveal melanoma lacks the high mutational burden that makes cutaneous melanoma responsive to immunotherapy. Emerging treatments like tebentafusp (a bispecific T-cell engager) show promise, with 73% one-year survival in recent trials.
Acral Melanoma Survival Disparities:
Acral lentiginous melanoma develops on palms, soles, and under nails, representing only 2-3% of melanomas in Caucasians but 35-60% in Asian, African, and Hispanic populations. Acral melanoma survival rates lag significantly behind other melanoma subtypes, with five-year survival of 60.5% and ten-year survival of only 41.6%.
These poorer outcomes result from:
- Later stage at diagnosis (average tumor thickness 3.86mm vs 1.2mm for other melanomas)
- 18-month average diagnostic delay (often mistaken for warts or fungal infections)
- 60% sentinel lymph node positivity rate at diagnosis
- Lower response to immunotherapy (30-35% vs 40-45% for cutaneous)
Mucosal Melanoma Realities:
Mucosal melanoma arising from nasal passages, oral cavity, gastrointestinal, or genital tract represents 1-2% of all melanomas but carries particularly poor prognosis. Five-year survival for stage 4 mucosal melanoma ranges from 8-15%, with median overall survival of 8-12 months even with aggressive treatment.
Critical Biomarkers Predicting Treatment Response
Modern precision oncology relies on molecular testing to guide therapy selection. Every stage 4 melanoma patient should undergo comprehensive melanoma genetic testing and biomarker analysis before starting treatment.
Essential melanoma diagnosis tests:
BRAF V600 Mutation Testing:
- Present in 40-50% of cutaneous melanoma patients
- Predicts response to dabrafenib/trametinib or encorafenib/binimetinib
- Mandatory before starting any systemic therapy
- Testing completed within 7-10 days through specialized cancer genomic laboratories
Melanoma PD-L1 Testing:
- Measures PD-L1 protein expression on tumor cells
- Higher expression (>50%) correlates with better pembrolizumab response
- Not required for treatment decisions but helps predict outcomes
- Performed via immunohistochemistry on tumor biopsy
Tumor Mutational Burden (TMB):
- Measures number of mutations per megabase of DNA
- High TMB (>10 mutations/Mb) predicts better immunotherapy response
- Melanoma typically has highest TMB of any cancer (average 15-20 mutations/Mb)
- Explains why melanoma responds so dramatically to checkpoint inhibitors
Lactate Dehydrogenase (LDH) Levels:
- Elevated LDH (>2x upper limit of normal) indicates aggressive disease
- Independent predictor of poor survival
- Used in melanoma staging (M1c vs M1a/M1b classification)
- Monitored every 3-6 months during treatment
Survival Statistics: The 2025 Reality
| Prognostic Factor | Five-Year Survival | Median Overall Survival |
|---|---|---|
| Overall Stage 4 | 35-51% | 24-36 months |
| Brain metastases present | 15-25% | 12-18 months |
| No brain metastases | 40-55% | 30-42 months |
| BRAF+ with targeted therapy | 45-60% | 36-48 months |
| Complete response to immunotherapy | 60-80% | Not reached (many alive >5 years) |
| Elevated LDH (>2x normal) | 15-25% | 12-18 months |
| Normal LDH | 45-60% | 36-48 months |
What This Means For You: Action Steps
Understanding your specific prognostic factors allows personalized treatment planning:
- Demand comprehensive testing before starting treatment:
- BRAF, NRAS, c-KIT mutation analysis
- PD-L1 expression testing
- Tumor mutational burden assessment
- Baseline LDH and complete metabolic panel
- Brain MRI surveillance is critical:
- Every 3-4 months during first 2 years of metastatic disease
- Brain metastases caught asymptomatically respond better to treatment
- Consider prophylactic brain radiation if high-risk features present
- Seek second opinions at melanoma specialty centers if you have:
- Uveal, acral, or mucosal melanoma (different treatment approaches)
- Brain metastases requiring coordinated multidisciplinary care
- Rare mutations requiring specialized targeted therapies
- Monitor for new symptoms vigilantly and track with a symptom checker tool to recognize progression early.
The difference between 15% five-year survival and 60% five-year survival often hinges on these specific factors. Patients with favorable prognostics—no brain metastases, BRAF mutations, normal LDH, limited disease burden—now frequently achieve long-term survival approaching that of stage 3 disease.
Melanoma Treatment Cost Breakdown & Financial Navigation Guide
When Emma’s stage 4 melanoma progressed after a year of immunotherapy, her oncologist recommended lifileucel TIL therapy. The survival benefit looked promising, but the estimated $600,000 hospital bill almost made her refuse. Only after a hospital financial counselor walked her through insurance coverage, copay caps, and patient-assistance programs did TIL cell therapy become realistic. Her story shows that melanoma treatment cost is not just a medical question; it is a financial planning emergency that you can’t afford to ignore.
Real-World Melanoma Treatment Costs in 2025
Stage 4 melanoma treatment cost varies massively depending on whether you receive immunotherapy, targeted therapy, or TIL cell therapy. Population-level analyses of checkpoint inhibitors estimate pembrolizumab or nivolumab at roughly $150,000–$175,000 per year in the United States, not including additional costs for imaging, lab monitoring, and managing melanoma immunotherapy side effects such as colitis or hepatitis.
For BRAF mutation melanoma, dabrafenib plus trametinib cost typically reaches $175,000–$200,000 per year when dosed at standard adult regimens. Many patients require dose reductions but remain on therapy for 12–18 months, which means lifetime drug spend can easily cross $250,000.
The newest and most expensive option is lifileucel melanoma cost. Published economic models and early commercialization estimates suggest a one-time episode cost of approximately $500,000–$750,000, which includes tumor surgery, cell manufacturing, inpatient lymphodepleting chemotherapy, the TIL infusion, and intensive monitoring. While that number is shocking, many insurers now treat lifileucel as a covered benefit for eligible stage 4 melanoma patients after the 2024 FDA accelerated approval.
Insurance Coverage, Out-of-Pocket Spend, and Hidden Bills
Melanoma insurance coverage is highly dependent on your plan type (employer-sponsored, ACA exchange, Medicare, or Medicaid), but most U.S. commercial plans cover FDA-approved checkpoint inhibitors and BRAF/MEK combinations for metastatic melanoma treatment according to National Cancer Institute treatment guidance.
However, melanoma immunotherapy cost for the patient is driven by deductibles, coinsurance, and out-of-pocket maximums. For example: a 20% coinsurance on $150,000 of pembrolizumab charges could mean $30,000 in annual out-of-pocket exposure without financial assistance. Hospital-based infusion billing can further inflate melanoma treatment cost because facility charges are higher than freestanding infusion centers, a detail rarely explained during consent.
Key melanoma treatment cost drivers include:
- Drug list price (Keytruda, Opdivo, dabrafenib, trametinib, lifileucel)
- Infusion center facility fees and chair time
- Radiology (CT, PET/CT, brain MRI every 3–4 months)
- Lab monitoring for melanoma tumor markers and organ function
- Hospitalizations to manage melanoma immunotherapy side effects
Cost Comparison: Immunotherapy, Targeted Therapy, and TIL
How to Reduce Melanoma Treatment Cost Without Compromising Care
1. Meet Early With a Cancer Center Financial Counselor
Every major melanoma treatment center now employs financial navigators who can estimate your stage 4 melanoma treatment cost before the first infusion. They can model worst-case and best-case out-of-pocket scenarios using your plan’s deductible, coinsurance, and annual out-of-pocket maximum, similar to how you might run scenario planning with a household budget or a weight-change projection using a structured calculator.
2. Apply for Manufacturer Copay and Free-Drug Programs
All major checkpoint inhibitor and BRAF/MEK manufacturers run patient assistance programs for underinsured patients. These programs can reduce melanoma immunotherapy cost by covering copays or, in some cases, providing free drug when income thresholds are met.
3. Use Clinical Trials Strategically
Enrolling in melanoma clinical trials at NCI‑designated centers often means the investigational drug and many associated tests are covered by the sponsor, with your insurance only charged for standard-of-care components. You can search actively recruiting stage 4 melanoma trials by location and treatment type through the U.S. government’s clinical trial registry at ClinicalTrials.gov.
4. Understand Medicare and Public Coverage Rules
If you are 65+ or disabled, Medicare will typically cover FDA‑approved melanoma checkpoint inhibitors and BRAF/MEK combinations under Part B (infused/office-administered) or Part D (oral drugs), subject to plan design. The Centers for Medicare & Medicaid Services site provides coverage details and prior authorization rules by drug category.
Choosing the Right Melanoma Treatment Center
Financial toxicity is lower when you receive care at high-volume melanoma treatment centers that know how to navigate copay foundations, charity care, and trial enrollment. The National Cancer Institute’s cancer center directory lists NCI‑designated hospitals that frequently lead advanced melanoma treatment research and offer lifileucel or other cellular therapies.
Patients who travel to such centers often combine aggressive treatment with structured lifestyle optimization. Working with dietitians to maintain muscle mass and energy during therapy—using tools like a protein intake calculator to align daily protein targets with body weight and treatment side effects—helps reduce hospitalizations and may indirectly lower total melanoma treatment cost.
At the same time, patients facing complex cancer decisions often benefit from reading other oncology cost guides, such as detailed breakdowns of lung cancer drug expenses or surgical cost explainer articles, to better understand how hospitals structure bills and how to question unexpected charges in real time.
Stage 4 Melanoma Treatment Timeline: What to Expect Month by Month
When Priya was told her stage 4 melanoma had spread to her lungs, everything blurred into a list of scans, biopsies, and drug names she couldn’t pronounce. What finally calmed her was seeing a clear month‑by‑month roadmap of what advanced melanoma treatment actually looks like—who she would see, which tests came first, and when she could expect to know if anything was working. This section gives you that same roadmap.
Months 0–2: Staging, Biomarker Testing, and First Big Decisions
The first 4–8 weeks after a stage 4 melanoma diagnosis focus on confirming where the cancer is, which mutations it carries, and how fast it is growing. Oncologists follow evidence‑based staging and workup algorithms similar to those described in the National Cancer Institute’s melanoma treatment PDQ, which integrates PET/CT, MRI, and pathology findings into a final treatment plan.
You will typically move through:
- Baseline imaging: CT of chest/abdomen, PET/CT, and brain MRI to find melanoma brain metastases or hidden lesions.
- Tissue confirmation: Biopsy or resection of at least one metastatic lesion if prior tissue is old or inadequate.
- Melanoma diagnosis tests: Comprehensive molecular profiling (BRAF, NRAS, c‑KIT), melanoma PDL‑1 testing, and possibly tumor mutational burden, often performed through labs that follow NCI‑endorsed precision medicine standards.
During this window, many patients also begin using a structured symptom tracking tool to log new pain, fevers, headaches, or neurologic changes between visits so they can escalate care quickly if signs of progression or serious melanoma immunotherapy side effects appear.
Months 2–6: Active Systemic Treatment Phase
Once staging and biomarkers are complete, most patients enter their first systemic treatment block. The exact regimen depends on whether the tumor has a BRAF mutation and the patient’s performance status.
Typical frontline pathways include:
- BRAF‑negative or unknown:
- BRAF‑positive (BRAF mutation melanoma):
- High‑risk or treatment‑refractory patients:
During months 2–6, you can expect:
- Infusion visits or daily oral therapy
- Lab monitoring every 3–6 weeks (CBC, liver, kidney, LDH)
- CT or PET/CT scans about every 12 weeks to assess response
- Management of side effects like fatigue, diarrhea, rash, or endocrine dysfunction, which may require temporary treatment holds or steroids.
TIL Cell Therapy Timeline Within the Journey
For patients pursuing TIL cell therapy melanoma treatment after failing checkpoint inhibitors, the process overlays the standard timeline and compresses into a 6–8‑week block:
- Week 0–1: Tumor resection to harvest tumor‑infiltrating lymphocytes.
- Week 2–5: Laboratory expansion of TIL product; you may remain on bridging therapy if disease is aggressive.
- Week 5–6: Hospital admission for lymphodepleting chemotherapy, TIL infusion, and high‑dose IL‑2 support.
- Week 6–8: Intensive recovery; early scans often show mixed responses that may improve over time as TIL cells continue attacking melanoma cells.
Months 6–12: Response Assessment, Switching Lines, and Dealing With Recurrence
By 6–9 months into stage 4 melanoma treatment, most patients fall into one of four response categories used in clinical trials and guideline documents from groups like the National Cancer Institute and professional oncology societies.
- Complete response (CR): All measurable disease disappears.
- Partial response (PR): Tumor burden shrinks by ≥30%.
- Stable disease (SD): Changes do not meet CR/PR or progression criteria.
- Progressive disease (PD): Tumor burden grows by ≥20% or new lesions appear.
If scans show progression despite adequate time on therapy:
- BRAF‑negative patients often switch from single‑agent PD‑1 to combination immunotherapy, enroll in melanoma clinical trials, or move to TIL therapy if eligible.
- BRAF‑positive patients who progressed on targeted therapy may transition to PD‑1 ± CTLA‑4 combinations or explore cellular or vaccine‑based trials.
Melanoma recurrence rate remains substantial even after partial or complete response, which is why imaging and lab surveillance typically continue every 3–6 months for several years, following patterns described in long‑term checkpoint inhibitor outcome studies.
Year 2 and Beyond: Long‑Term Survivorship and Chronic Management
For the growing group of patients whose stage 4 melanoma becomes a chronic or controlled condition, life between scans can feel like living with a “shadow” in the background. Oncologists increasingly frame this phase as survivorship rather than end‑stage care, especially for those with durable complete responses to checkpoint inhibitors or TIL cell therapy.
Long‑term follow‑up usually includes:
- Physical exams every 3–6 months for the first 2–3 years, then annually
- Periodic CT or PET/CT, plus brain MRI if there is any history of melanoma brain metastases
- Endocrinology follow‑up for permanent thyroid, adrenal, or pituitary damage caused by immunotherapy
- Lifestyle counseling on exercise, diet, and cardiovascular risk, given emerging data that metabolic health influences both tolerance of therapy and long‑term outcomes in cancer survivors.
Many patients in this phase also benefit from cancer‑specific mental health support and practical guides on returning to work, navigating long‑term disability insurance, and recognizing subtle signs of recurrence early so they can re‑engage with their oncology team before the disease regains momentum.
Preventing Melanoma Progression & Catching Recurrence Early
Carlos completed 18 months of pembrolizumab for his stage 4 melanoma and achieved complete response in 2024. His oncologist warned him that while scans showed no evidence of disease, his melanoma recurrence rate risk remained 15–25% over the next five years. Carlos now follows a disciplined surveillance protocol: quarterly skin checks, biannual imaging, and monthly self-examinations of every mole using his phone’s camera to track changes over time. This vigilance is what separates patients who catch recurrence at a treatable stage from those who present with widespread progression.
For Stage 4 Survivors: Preventing New Primaries and Detecting Recurrence
Even after successful treatment of metastatic disease, melanoma prevention becomes a lifelong priority. Patients who had one melanoma face a 10–15% lifetime risk of developing a second primary melanoma, independent of their initial stage, according to long-term cohort studies tracked through registries like those maintained by the National Cancer Institute.
Risk-reduction strategies for melanoma survivors:
- Strict sun protection: Daily broad-spectrum SPF 50+ sunscreen, protective clothing, and avoidance of midday UV exposure (10 AM–4 PM).
- Complete tanning bed avoidance: Indoor tanning raises melanoma risk by 59% in meta-analyses, with higher risk in those who start before age 35.
- Quarterly to biannual full-body skin exams by a dermatologist trained in dermoscopy melanoma techniques, which improve early detection sensitivity by 10–30% compared to naked-eye examination.
- Monthly self-skin checks using the ABCDE rule to identify suspicious moles melanoma may cause.
Melanoma Early Detection: The ABCDE Rule and Modern Tools
Melanoma early detection saves lives by catching disease when it is still surgically curable. Most early melanomas are identified by patients or family members noticing changing moles, which is why patient education on melanoma risk factors and warning signs remains a cornerstone of public health guidance from organizations like the Centers for Disease Control and Prevention.
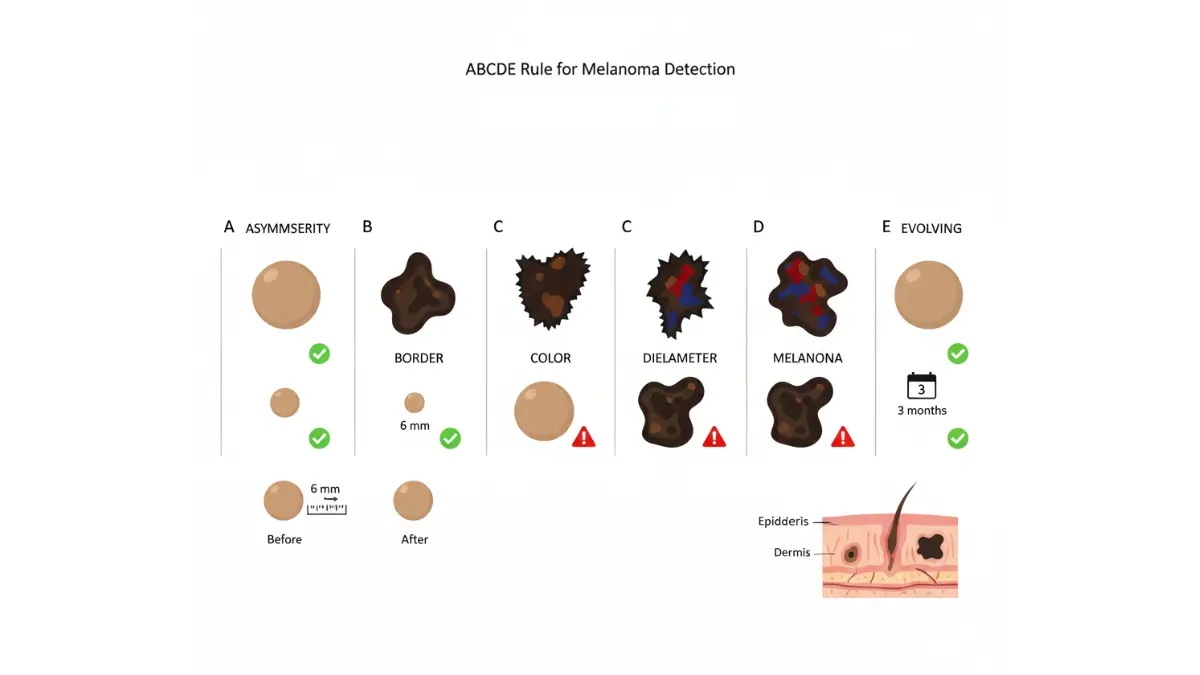
ABCDE criteria for suspicious moles melanoma screening:
- A – Asymmetry: One half does not match the other half.
- B – Border irregularity: Edges are ragged, notched, or blurred.
- C – Color variation: Multiple shades of brown, black, tan, red, white, or blue within one lesion.
- D – Diameter: Larger than 6 mm (pencil eraser size), though some melanomas are smaller.
- E – Evolving: Any mole that changes in size, shape, color, elevation, or develops new symptoms like bleeding, itching, or crusting.
AI Melanoma Detection and Advanced Screening
New technologies are transforming melanoma skin check accuracy. DermaSensor, an AI melanoma detection device approved by the FDA in 2024, uses elastic scattering spectroscopy to evaluate suspicious lesions in real time during office visits, achieving 96% sensitivity for melanoma detection in pivotal trials. Dermatology practices increasingly integrate AI tools with traditional dermoscopy melanoma protocols to reduce missed diagnoses.
For high-risk patients—including those with a personal history of stage 4 melanoma, multiple atypical nevi, or strong family history—many centers now offer total-body photography with digital mole mapping, which creates a baseline record of all existing lesions and uses computer algorithms to flag new or changing spots at follow-up visits.
Lifestyle Optimization During and After Treatment
Stage 4 melanoma patients who maintain healthy body composition and metabolic function tend to tolerate treatment better and may experience improved outcomes. Practical steps include maintaining appropriate caloric intake using tools like an ideal weight calculator to set realistic targets during therapy, ensuring adequate hydration by following personalized recommendations from a water intake calculator, and prioritizing restorative sleep cycles with guidance from a sleep calculator to support immune recovery.
Emerging data suggest that cardiovascular fitness and structured exercise programs may reduce cancer recurrence risk across multiple tumor types, though melanoma-specific evidence remains limited. Patients cleared for physical activity often benefit from moderate-intensity aerobic exercise tracked with a heart rate zone calculator to stay within safe training zones during recovery.
Your Immediate Action Plan
If you or a loved one is navigating stage 4 melanoma, take these steps this week:
- Schedule comprehensive biomarker testing (BRAF, PD-L1, TMB) if not already completed.
- Request a financial counseling session at your cancer center to model out-of-pocket costs before starting therapy.
- Search for relevant clinical trials using the federal trial registry and discuss eligibility with your oncology team.
- Establish baseline imaging including brain MRI to guide future surveillance.
- Connect with melanoma survivor support groups for peer guidance on treatment decisions, side effect management, and long-term coping strategies.
For patients with other cancer concerns or family members seeking to understand cancer risk across types, exploring related resources on lung cancer treatment advances or small cell lung cancer survival data can provide broader context on how immunotherapy and targeted treatments are transforming outcomes across solid tumors. Understanding the interconnected nature of cancer biology and treatment helps patients advocate more effectively for cutting-edge care.
Stage 4 melanoma is no longer an automatic death sentence. With TIL cell therapy, advanced checkpoint inhibitors, targeted BRAF therapies, and emerging melanoma vaccine therapy approaches in clinical trials, survival has improved from months to years—and for some, to decades. The key is aggressive early treatment, vigilant monitoring for progression, and refusing to accept “no options left” until you have exhausted trials at major melanoma treatment centers and explored every cellular and immunotherapy avenue.
DISCLAIMER:
This article is for educational purposes and does not constitute medical advice. Stage 4 melanoma treatment decisions should be made in consultation with a board-certified medical oncologist after comprehensive evaluation. Treatment options, costs, and outcomes vary based on individual patient factors, insurance coverage, and geographic location. Information is current as of January 2026 and reflects FDA approvals, clinical trial data, and SEER statistics available at time of publication. Always verify drug costs, insurance coverage, and clinical trial eligibility directly with treatment centers and payers.
Frequently Asked Questions About Stage 4 Melanoma
1. What is the survival rate for stage 4 melanoma in 2025?
Stage 4 melanoma five-year survival rates now reach 35–51% with modern treatments including checkpoint inhibitors, TIL cell therapy, and targeted therapies. Patients achieving complete response to immunotherapy show 60–80% five-year survival, a dramatic improvement from the 15% rates seen before 2014.
2. How much does TIL cell therapy cost for melanoma?
TIL cell therapy (lifileucel) costs approximately $500,000–$750,000 for the complete one-time treatment including tumor surgery, cell manufacturing, hospitalization, and monitoring. Most major insurance plans now cover TIL therapy following FDA approval in February 2024 for patients who have failed checkpoint inhibitors.
3. What is the life expectancy with stage 4 melanoma brain metastases?
Median survival with melanoma brain metastases has improved from 4 months historically to 12–18 months with modern combination therapy (immunotherapy plus stereotactic radiosurgery). Patients with 1–3 small brain lesions caught on surveillance scans achieve up to 51% four-year survival with aggressive multimodal treatment.
4. Does insurance cover melanoma immunotherapy?
Yes, most U.S. commercial insurance, Medicare, and Medicaid plans cover FDA-approved checkpoint inhibitors (pembrolizumab, nivolumab, ipilimumab) for metastatic melanoma. Manufacturer copay assistance programs can reduce out-of-pocket costs significantly, though patients may still face $30,000–$51,000 annual copays on high-deductible plans without financial aid.
5. How long does stage 4 melanoma treatment last?
Treatment duration varies by type: immunotherapy typically continues for 1–2 years or until progression, BRAF/MEK targeted therapy averages 12–18 months before resistance develops, and TIL cell therapy is a one-time infusion requiring 2–3 weeks hospitalization. Long-term responders may receive maintenance therapy for several years.
6. What are the side effects of melanoma immunotherapy?
Common melanoma immunotherapy side effects include fatigue, diarrhea, colitis (10–15%), skin rash, and endocrine dysfunction like hypothyroidism (15–20%). Severe immune-related adverse events requiring hospitalization occur in 15–20% of patients on single-agent therapy and 50–55% on combination checkpoint blockade.
7. Can you be cured of stage 4 melanoma?
While “cure” is difficult to define in metastatic cancer, 15–25% of stage 4 melanoma patients achieve durable complete responses lasting 5+ years with modern immunotherapy or TIL therapy. Some patients remain disease-free a decade after treatment, functionally cured, though lifelong surveillance continues.
8. What is the difference between acral and cutaneous melanoma?
Acral melanoma develops on palms, soles, or under nails and represents 2–3% of melanomas in Caucasians but 35–60% in Asian, African, and Hispanic populations. It has worse prognosis (41.6% ten-year survival vs 60–70% for cutaneous) due to later diagnosis and lower immunotherapy response rates.
9. How do I find the best melanoma treatment centers?
Search the National Cancer Institute’s directory of NCI-designated cancer centers, which specialize in advanced melanoma treatment and offer TIL therapy, cutting-edge clinical trials, and multidisciplinary care. Top centers include Memorial Sloan Kettering, MD Anderson, Mayo Clinic, Dana-Farber, and Moffitt Cancer Center.
10. What biomarker tests do I need before starting treatment?
Essential tests include BRAF V600 mutation testing (present in 40–50% of patients), PD-L1 expression levels, tumor mutational burden (TMB), NRAS and c-KIT mutation analysis, and baseline LDH levels. These results guide treatment selection between targeted therapy, immunotherapy, or cellular therapy approaches.
11. Does melanoma recur after complete response?
Yes, melanoma recurrence occurs in 15–25% of stage 4 patients who achieved complete response over the following 5 years. Regular surveillance with imaging every 3–6 months, quarterly dermatology exams, and monthly self-skin checks help detect recurrence early when it remains treatable with second-line therapies or clinical trials.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.











