
On This Page – Quick Medical Summary
Melanoma 2026—Why This Year Could Save Your Life
Melanoma 2026: The Skin Cancer That Kills—Are You Next?
Sarah Martinez was 34 when she noticed a small brown mole on her shoulder blade start changing color. She was a busy healthcare worker from Phoenix, juggling two kids and 12-hour hospital shifts. The mole looked harmless—a little darker, slightly bigger—so she waited eight months before seeing a dermatologist.
That delay nearly killed her. By the time doctors biopsied the lesion in March 2024, melanoma had spread to her lymph nodes. Sarah was diagnosed with stage 3 melanoma and immediately started immunotherapy treatment that cost her family $78,000 out of pocket.
The 2026 Melanoma Crisis Every American Faces
Over 104,960 Americans will be diagnosed with invasive melanoma this year, making it the fifth most common cancer in both men and women. Another 8,430 people won’t survive—most because they waited too long to get suspicious moles checked. The Centers for Disease Control and Prevention now emphasizes that early detection through regular skin checks remains the most powerful weapon against this deadly cancer.
Here’s the brutal truth: melanoma caught at stage 1 has a 98% ten-year survival rate. Wait until stage 4, and that number plummets to 43%. The difference between life and death is often measured in weeks, not months.
Why 2026 Changes Everything for Melanoma Detection
Revolutionary artificial intelligence tools now detect melanoma with 99.5% accuracy using just your smartphone. These FDA-cleared apps analyze photos of suspicious moles in under 60 seconds, identifying dangerous changes that even trained dermatologists might miss. Virtual dermatology consultations have exploded, cutting wait times from 6-8 weeks down to 48 hours.
But technology alone won’t save you—action will. If you have a mole that’s changed in size, shape, or color in the past three months, you need evaluation within 48 hours. New moles appearing after age 40 deserve immediate medical attention.
Calculate Your Personal Melanoma Risk in 60 Seconds
Your family history, skin type, and sun exposure patterns determine your melanoma risk more than you realize. People with fair skin face 20 times higher risk compared to those with darker complexions. Having more than 50 moles increases your risk fivefold. The National Cancer Institute’s SEER database tracks these patterns, showing that early screening saves lives.
Use our free Genetic Risk Assessment Tool to evaluate your personalized melanoma risk based on proven clinical factors. This evidence-based calculator takes under one minute and provides immediate results showing whether you need urgent dermatologist screening or can safely monitor moles monthly at home.
Don’t become another statistic. Early melanoma detection transforms a potential death sentence into a highly curable disease.
Melanoma Detection 2026—From ABCDE to AI Revolution
How to Spot Melanoma Before It’s Too Late
Most melanomas start as innocent-looking moles that gradually transform into killers. The challenge? Distinguishing a harmless spot from a deadly cancer requires more than casual observation. Nearly 36% of early melanomas slip past traditional detection methods, giving cancer precious time to spread.
The ABCDE Rule: Your First Line of Defense
Dermatologists worldwide use the ABCDE method to evaluate suspicious moles, and you can master it in under five minutes. Research published by the National Institutes of Health confirms that combining multiple ABCDE criteria dramatically improves detection accuracy.
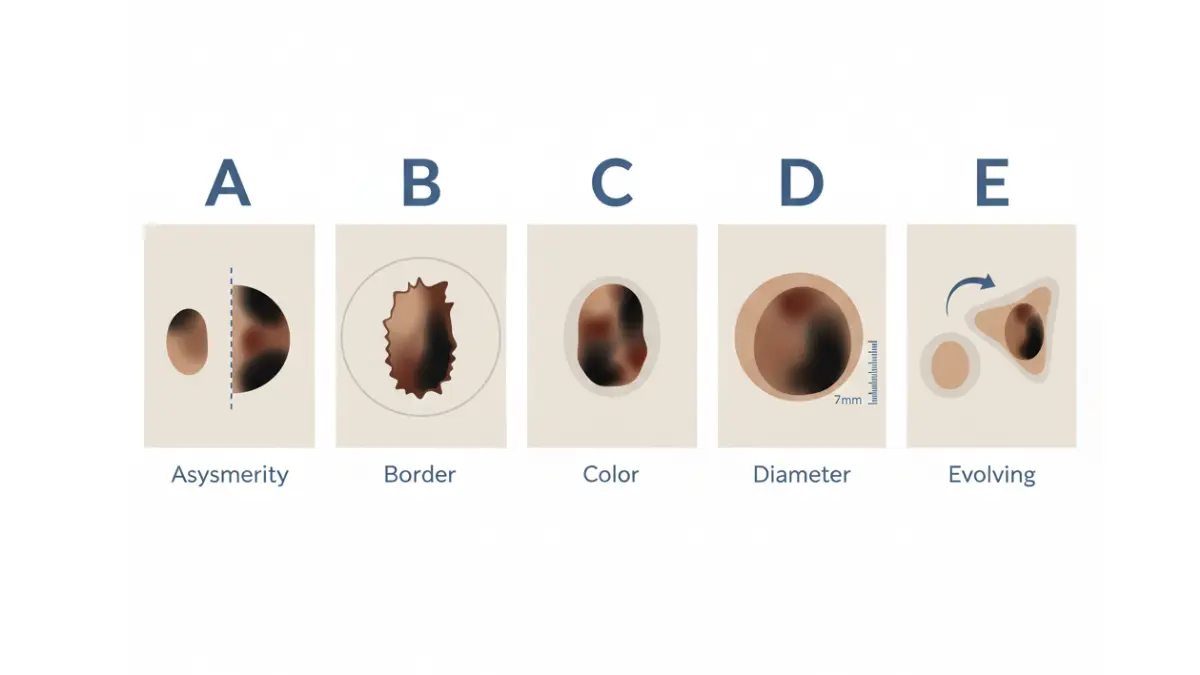
Breaking Down Each Warning Sign
Asymmetry: Draw an imaginary line through the mole’s center. If the two halves don’t match, schedule evaluation within 48 hours. Normal moles are symmetrical—melanomas rarely are.
Border irregularity: Melanoma edges look notched, scalloped, or blurred, not smooth and round. Benign moles have clear, defined borders that don’t fade into surrounding skin.
Color variation: Multiple colors within one lesion—brown mixed with black, red, white, or blue—signals danger. Healthy moles stay consistently tan or brown throughout.
Diameter exceeding 6mm: Melanomas typically grow larger than a pencil eraser (6 millimeters), though early-stage cancers can be smaller. Any mole approaching this size deserves professional assessment.
Evolving characteristics: Changes in size, shape, color, or symptoms (itching, bleeding, crusting) over weeks or months represent the single most important warning sign. Studies show evolution has an 8.4 positive likelihood ratio for melanoma diagnosis.
The ABCDE Rule Misses Over One-Third of Melanomas
Clinical trials reveal the ABCDE method alone achieves just 64-77% sensitivity when used by non-dermatologists. Aggressive nodular melanomas and amelanotic (non-pigmented) melanomas frequently bypass traditional criteria, appearing suddenly as pink or flesh-colored bumps rather than dark, irregular spots.
The Ugly Duckling Sign: A Game-Changing Addition
If you have multiple moles, identify the one that looks dramatically different from all others on your body—that’s your ugly duckling. Research from the Journal of the American Academy of Dermatology showed nine dermatologists achieved 100% melanoma detection using this comparative method, with 96% specificity that cut unnecessary biopsies nearly sevenfold.
Primary care physicians correctly identified 85% of melanomas using the ugly duckling sign alone, making it accessible even without specialized training. For comprehensive health assessment including skin changes, try our Symptom Checker to evaluate multiple symptoms simultaneously and determine urgency level.
2026 Breakthrough: FDA-Approved AI Melanoma Detection
Technology has revolutionized early detection with smartphone-based artificial intelligence that rivals expert dermatologists. The FDA cleared DermaSensor in January 2024 after clinical trials demonstrated 96% sensitivity across all skin cancers and 100% sensitivity for invasive melanomas.
How AI Detection Actually Works
These handheld devices use elastic scattering spectroscopy—shining multiple light wavelengths onto suspicious lesions and analyzing cellular characteristics invisible to the human eye. Within 60 seconds, AI algorithms trained on over 100,000 skin cancer cases provide binary results: “Monitor” for likely benign or “Investigate Further” for suspicious lesions requiring biopsy.
Primary care physicians using these tools achieve diagnostic accuracy comparable to board-certified dermatologists, eliminating 6-8 week specialist wait times that allow aggressive melanomas to advance from stage 1 to stage 3.
Virtual Dermatology: Fast, Affordable Melanoma Screening
Telemedicine dermatology consultations now cost $50-$150, compared to $200-$400 for traditional office visits. Upload smartphone photos of suspicious moles and receive specialist evaluation within 24-48 hours—26 days faster than conventional referral pathways.
Store-and-forward teledermoscopy combines patient-submitted images with AI pre-screening, allowing dermatologists to triage urgent cases requiring immediate biopsy versus benign lesions safe for monitoring. This hybrid approach reduces unnecessary procedures while catching dangerous melanomas at thinner, more curable stages.
The bottom line: Monthly self-exams using ABCDE and ugly duckling methods, combined with annual professional screening and AI-assisted evaluation of changing moles, creates a multilayered defense against melanoma that’s transformed survival rates over the past five years.
Melanoma Stages and Types—Your Survival Depends on Early Diagnosis
Understanding Melanoma Stages 0 Through 4
Melanoma staging determines everything—your treatment plan, prognosis, and survival odds. The American Joint Committee on Cancer uses TNM classification (Tumor thickness, Node involvement, Metastasis) to assign stages that dictate clinical decisions.
Stage assignments changed significantly in the AJCC 8th Edition implemented in 2018, particularly for thin melanomas under 0.8mm. These revisions improved prognostic accuracy and allowed better treatment stratification based on real-world patient outcomes from over 46,000 cases.
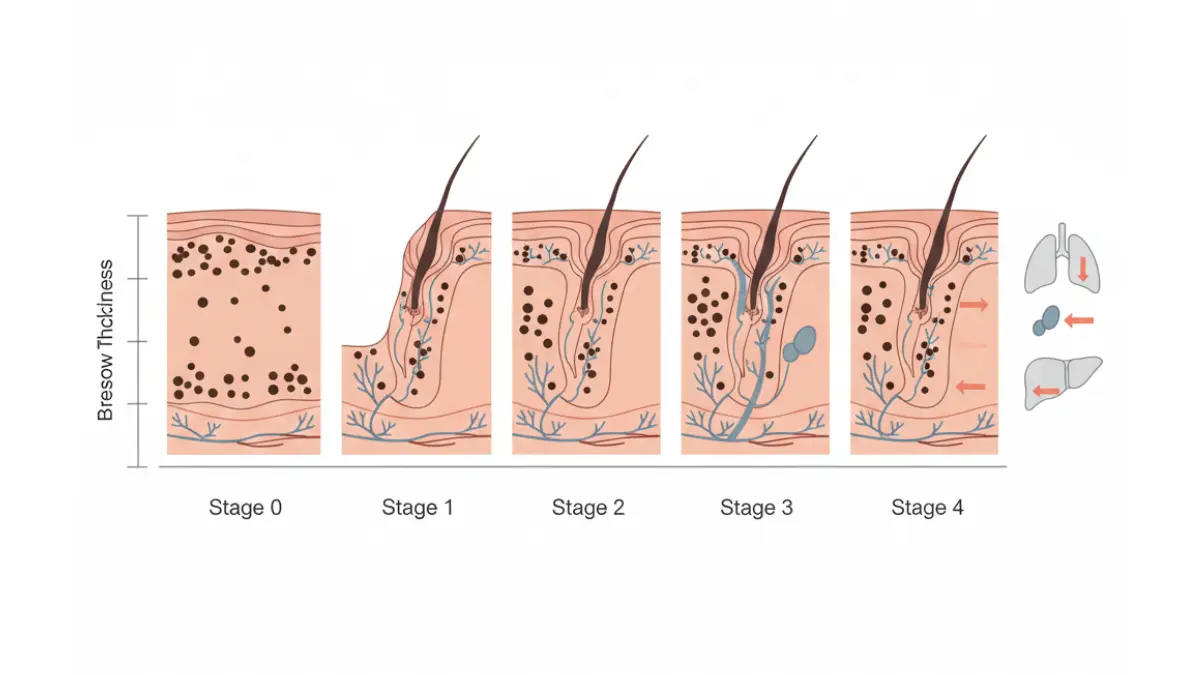
Stage 0: Melanoma In Situ
Cancer cells exist only in the epidermis—the outermost skin layer—without invasion into deeper tissue. Surgical removal achieves 99.9% cure rates. These lesions represent pre-invasive disease with virtually zero metastatic potential.
Stage 1: Localized Thin Melanoma
The tumor measures less than 2mm thick with no lymph node involvement. Stage 1 subdivides into 1A (under 0.8mm without ulceration) and 1B (0.8-1.0mm or ulcerated lesions under 0.8mm). Five-year survival reaches 98% with simple wide excision surgery.
Stage 2: Localized Thick Melanoma
Tumors exceed 1mm thickness but haven’t spread to lymph nodes. Stage 2A (1-2mm with ulceration or 2-4mm without) has 93% five-year survival. Stage 2B (2-4mm with ulceration or over 4mm without) drops to 85%. Stage 2C (over 4mm with ulceration) shows 82% five-year survival.
Stage 3: Regional Lymph Node Involvement
Melanoma has spread to nearby lymph nodes or created satellite lesions. The AJCC 8th Edition expanded N categories to include clinically occult versus clinically detected nodes. Stage 3 ranges from 3A (single microscopic node, 93% five-year survival) to 3D (four or more involved nodes with distant skin spread, 32% five-year survival).
Stage 4: Distant Metastasis
Cancer has spread beyond regional nodes to distant organs—lungs, liver, brain, bones, or other skin sites. The 8th Edition added M1d classification specifically for central nervous system metastases. Ten-year survival with modern immunotherapy combinations reaches 52%, compared to historical rates under 10%.
Survival Rate Comparison: 2026 vs. Historical Data
| Stage | 2026 Five-Year Survival | 2009-2015 Survival | Improvement |
|---|---|---|---|
| Stage 0 (In Situ) | 99.9% | 99% | +0.9% |
| Stage 1 | 98% | 95% | +3% |
| Stage 2 | 85-93% | 79-89% | +4-6% |
| Stage 3 | 68-88% | 40-70% | +18-28% |
| Stage 4 (10-year) | 52% | <10% | +420% |
The most dramatic improvements occurred in advanced melanoma due to checkpoint inhibitor immunotherapy introduced after 2011. Early-stage survival rates were already excellent but have incrementally improved through better surgical techniques and adjuvant therapies.
Five Melanoma Types You Must Recognize
Not all melanomas look alike. Understanding subtypes helps identify dangerous lesions that bypass typical ABCDE criteria, particularly in patients with darker skin tones who face delayed diagnosis.

1. Superficial Spreading Melanoma (70% of Cases)
The most common type, appearing as flat or barely raised lesions with irregular borders and color variation. Half develop from existing moles, half from new spots. Most frequent on men’s torsos, women’s legs, and upper backs of both sexes. Spreads horizontally along skin surface for months to years before deepening.
2. Nodular Melanoma (10-15% of Cases)
The most aggressive form, growing vertically from the start rather than spreading horizontally. Appears as blue-black dome-shaped nodules, though 5% present as pink or red bumps—easily mistaken for benign lesions. More common in men, typically on trunk, head, or neck. Frequently diagnosed at greater depth with poorer prognosis than other types.
3. Lentigo Maligna Melanoma (10-15% of Cases)
Develops on chronically sun-damaged skin, usually on the face, ears, or arms of older adults. Starts as a flat tan or brown patch that slowly darkens and expands over years before becoming invasive. More common in fair-skinned individuals with extensive sun exposure history.
4. Acral Lentiginous Melanoma (5-8% of Cases)
Occurs on palms, soles, or under nails—the only melanoma type unrelated to UV exposure. Represents 70% of melanomas in Black patients and 46% in Asian populations, yet accounts for just 8% of total cases. Extremely aggressive with rapid vertical growth. Often diagnosed late due to overlooked locations.
5. Amelanotic Melanoma (2-8% of Cases)
Lacks typical dark pigmentation, appearing pink, red, or flesh-colored. Frequently misdiagnosed as eczema, psoriasis, or basal cell carcinoma. Represents one of the deadliest subtypes due to delayed recognition—patients and physicians alike miss colorless lesions.
Understanding how melanoma stage and type interact with overall health status improves risk assessment. Just as thyroid cancer symptoms require systematic evaluation, melanoma diagnosis demands comprehensive analysis beyond visual inspection alone.
The key takeaway: Stage 1 melanoma caught through routine screening offers 98% survival. Wait until symptoms force action at stage 4, and survival drops below 50% even with breakthrough treatments.
Melanoma Treatment Options and Costs—What to Expect in 2026
Surgery: The Gold Standard for Early Melanoma
Wide local excision remains the definitive cure for stage 0-2 melanoma, removing the tumor plus surrounding healthy tissue to ensure clear margins. Surgeons take 0.5-1cm margins for thin melanomas under 1mm, expanding to 2cm margins for lesions exceeding 2mm thickness.
Average costs range from $6,500 to $15,000 for outpatient excision, including anesthesia, pathology, and wound closure. Most private insurance covers melanoma surgery with typical copays of $500-$2,000, while Medicare Part B covers 80% after deductible.
Sentinel Lymph Node Biopsy—Staging Surgery
For melanomas exceeding 0.8mm thickness or demonstrating ulceration, surgeons perform sentinel node biopsy to detect microscopic spread. This procedure adds $15,000-$22,000 to surgical costs but transforms treatment decisions. Finding positive nodes upstages disease to stage 3, triggering adjuvant immunotherapy that reduces recurrence risk by 45-60%.
Mohs Micrographic Surgery for Facial Melanomas
Specialized layer-by-layer removal preserves maximum healthy tissue while ensuring complete cancer excision. Particularly valuable for melanomas on the face, ears, or hands where tissue preservation matters. Costs average $8,000-$12,000 but achieve 98-99% cure rates for early-stage disease.
Immunotherapy Revolution—Game-Changing Checkpoint Inhibitors
The National Cancer Institute confirms that checkpoint inhibitor immunotherapy has revolutionized advanced melanoma treatment, transforming stage 4 disease from rapidly fatal to potentially curable.
How Checkpoint Inhibitors Work
PD-1 and CTLA-4 checkpoint inhibitors remove molecular “brakes” that cancer uses to hide from immune surveillance. Once unleashed, T-cells recognize and destroy melanoma cells throughout the body. This approach works regardless of BRAF mutation status or PD-L1 expression.
FDA-Approved Immunotherapy Drugs for Melanoma
Pembrolizumab (Keytruda): PD-1 blocker administered intravenously every three weeks. List price approximately $150,000 annually or $12,500 per infusion. Median overall survival for stage 4 patients exceeds 32 months—triple the pre-immunotherapy era.
Nivolumab (Opdivo): Alternative PD-1 blocker with similar efficacy. Annual cost averages $150,000 for monotherapy. Three-year survival reaches 39% for advanced melanoma.
Ipilimumab (Yervoy): CTLA-4 blocker typically combined with nivolumab rather than used alone. Combination therapy costs $256,000 annually but delivers 62% three-year survival for stage 4 disease.
Nivolumab-Ipilimumab Combination: The most effective first-line regimen for advanced melanoma. Patients achieve mean treatment-free survival of 12.4 months compared to 8.9 months with single-agent therapy. At 36 months post-treatment, 62% remain alive versus 39% with pembrolizumab alone.
Real-World Immunotherapy Costs in 2026
Total treatment costs for stage 3-4 melanoma range from $150,000 to $400,000 over 12-24 months. Medicare covers FDA-approved immunotherapy with 20% coinsurance. Private insurers typically require prior authorization but cover checkpoint inhibitors as standard of care.
Patient assistance programs from manufacturers can reduce out-of-pocket costs to $0-$25 per treatment for qualifying individuals earning under 500% of federal poverty level ($75,000 for individuals, $154,000 for families of four).
Targeted Therapy for BRAF-Mutated Melanoma
Approximately 40-50% of melanomas harbor BRAF V600E/K mutations that drive uncontrolled growth. Targeted therapy combinations—dabrafenib plus trametinib or vemurafenib plus cobimetinib—block this pathway with 68% response rates.
These oral medications cost $15,000-$20,000 monthly ($180,000-$240,000 annually) but work faster than immunotherapy, shrinking tumors within weeks. Resistance typically develops after 12-18 months, making them ideal for rapidly progressing disease requiring immediate response.
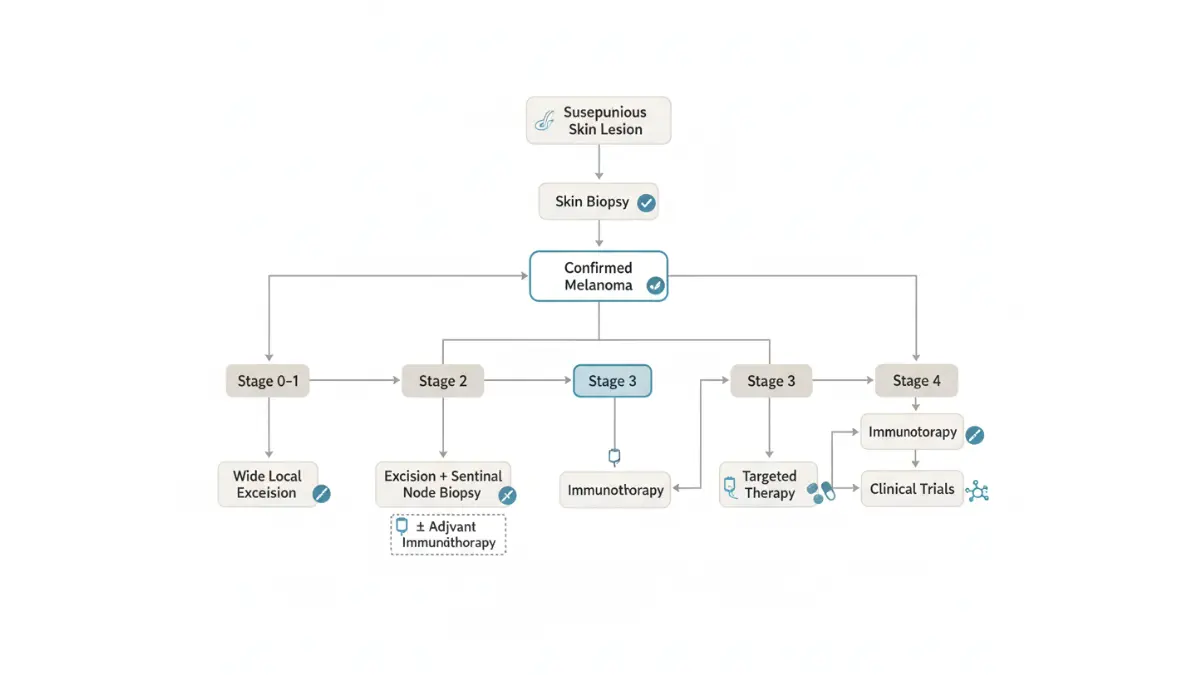
Stage-Specific Treatment Protocols
Stage 0-1A: Wide excision alone, 99% cure rate, $6,500-$10,000 total cost
Stage 1B-2A: Excision plus sentinel node biopsy, consider adjuvant immunotherapy for high-risk features, $25,000-$35,000
Stage 2B-2C: Surgery plus 12 months adjuvant pembrolizumab or nivolumab, reduces recurrence 45-60%, $200,000-$250,000
Stage 3: Complete lymph node dissection plus adjuvant immunotherapy for one year, $225,000-$300,000
Stage 4: First-line immunotherapy (nivolumab-ipilimumab or pembrolizumab) or targeted therapy for BRAF+ disease, $250,000-$400,000 for full treatment course
Similar to breakthrough treatments for other aggressive cancers covered in our lung cancer FDA-approved drugs guide, melanoma immunotherapy represents a paradigm shift that has turned previously fatal diagnoses into manageable chronic conditions for many patients.
Financial assistance resources: Cancer.gov patient support programs, pharmaceutical manufacturer copay cards, nonprofit foundations offering grants for melanoma treatment costs.
Melanoma Risk Factors and Prevention—Take Control Today
Who’s Most at Risk for Melanoma?
Understanding your personal risk profile determines screening frequency and prevention intensity. Some factors you inherit—others result from lifestyle choices you can modify starting today.
Top 8 Melanoma Risk Factors
UV radiation exposure: The single most preventable cause, accounting for 86% of melanoma cases. Both cumulative sun exposure and severe sunburns—especially during childhood—dramatically increase lifetime risk. Tanning bed use before age 35 raises melanoma risk by 75%.
Fair skin complexion: Individuals with pale skin that burns easily face 20-fold higher melanoma risk compared to darker skin tones. Red or blonde hair combined with blue or green eyes creates particularly high susceptibility.
High mole count: Having more than 50 moles increases risk fivefold. Atypical or dysplastic nevi—large, irregularly shaped moles—raise risk another 5-10 times.
Family history: First-degree relatives with melanoma create 2-3 times higher risk. Inherited BRCA2, CDKN2A, or BAP1 mutations account for 5-10% of cases and warrant genetic counseling.
History of severe sunburns: Five or more blistering sunburns during childhood doubles melanoma risk. Each additional severe burn compounds cumulative DNA damage that manifests decades later.
Previous skin cancer: Surviving one melanoma creates 9-fold increased risk of developing a second primary melanoma. Previous basal or squamous cell carcinomas raise melanoma risk 3-5 times.
Immunosuppression: Organ transplant recipients taking immunosuppressive medications face 8-fold elevated melanoma risk. HIV/AIDS and autoimmune diseases requiring chronic immunosuppression similarly increase vulnerability.
Geographic location and altitude: Living at higher elevations or closer to the equator intensifies UV exposure. Every 1,000-foot altitude increase raises UV intensity 8-10%.
Evidence-Based Melanoma Prevention Strategies
Sun Protection Protocol
The CDC recommends comprehensive sun safety strategies that extend beyond sunscreen alone. Seek shade during peak UV hours between 10 AM and 4 PM when the sun’s rays are most intense. UV exposure causes oxidative stress that damages melanocyte DNA, triggering malignant transformation over time.
Sunscreen selection and application: Choose broad-spectrum SPF 30+ that blocks both UVA aging rays and UVB burning rays. SPF 30 filters 97% of UVB radiation, while SPF 50 blocks 98%—higher numbers offer minimal additional protection. Apply one ounce (shot glass full) to all exposed skin 15 minutes before sun exposure, reapplying every two hours or immediately after swimming or heavy sweating.
Protective clothing: UPF 50+ fabrics block 98% of UV rays. Wide-brimmed hats (3+ inch brims) shade face, ears, and neck—common melanoma sites. UV-blocking sunglasses prevent ocular melanoma.
Complete tanning bed avoidance: Indoor tanning delivers 10-15 times more UV radiation than midday sun. No “base tan” provides meaningful protection—any tan represents DNA damage.
Lifestyle Modifications for Lower Risk
Monthly self-examinations: Check entire body including scalp, between toes, under nails, and genital areas. Photograph moles to track changes over time. Partners should examine hard-to-see areas like the back and posterior scalp.
Annual dermatologist screening: Essential for individuals with 50+ moles, fair skin, family history, or previous skin cancer. Professional full-body exams with dermoscopy detect melanomas invisible to untrained eyes.
Vitamin D optimization: Obtain recommended 1,000-2,000 IU daily through supplements or fortified foods rather than UV exposure. Maintaining adequate levels supports immune function that may help prevent cancer development.
Weight management: Obesity increases melanoma recurrence risk and worsens outcomes. Use our BMI Calculator to assess whether your weight falls within healthy ranges that optimize immune function and reduce systemic inflammation linked to cancer progression.
Mediterranean dietary pattern: Emerging research suggests high consumption of olive oil, fish, vegetables, and antioxidants may reduce melanoma risk by 20% through anti-inflammatory mechanisms. Limit alcohol to under two drinks daily—heavier consumption increases risk.
When to See a Doctor—Your Melanoma Action Plan
Emergency Warning Signs Requiring Immediate Evaluation
Certain melanoma symptoms demand urgent dermatologist consultation within 48-72 hours. Delays can allow aggressive tumors to advance from early-stage curable disease to metastatic cancer requiring intensive systemic treatment.
See a Dermatologist Immediately If You Notice:
- Mole changed size, shape, or color in the past 1-3 months
- New dark spot appeared after age 40, especially on sun-exposed skin
- Bleeding, oozing, or crusting lesion that won’t heal within 2 weeks
- Itching or tenderness in a previously asymptomatic mole
- “Ugly duckling” appearance—one lesion dramatically different from all others
- Family history plus suspicious new growth—genetic predisposition increases urgency
- Rapidly expanding nodule over 4-6 weeks (possible nodular melanoma)
Similar to recognizing early breast cancer warning signs, melanoma detection requires vigilant self-monitoring combined with professional evaluation of suspicious changes.
2026 Melanoma Screening Options
Virtual Dermatology Consultations
Telemedicine skin checks cost $50-$150 and provide board-certified dermatologist review within 24-48 hours. Upload high-quality photos of suspicious lesions from multiple angles. Dermatologists assess whether urgent in-person biopsy is needed or routine monitoring suffices.
In-Person Screening Visits
Full-body skin exams range from $150-$300 with insurance copays, or $120-$400 without coverage. Medicare covers annual preventive screenings when ordered by your primary care physician. Most appointments last 15-30 minutes including dermoscopy examination of concerning moles.
What Happens During Melanoma Biopsy
If your dermatologist identifies a suspicious lesion, they’ll perform an excisional biopsy during the same visit or schedule within 1-2 weeks. The National Cancer Institute recommends complete excision rather than partial removal to ensure accurate diagnosis and staging.
Biopsy procedure: Local anesthetic injection (10 seconds burning sensation), then surgical removal of entire lesion plus 1-2mm margin. The procedure takes 10-15 minutes. Most patients describe pressure but no pain once anesthetized. Stitches dissolve in 7-14 days.
Results timeline: Pathology reports arrive in 5-7 days, confirming benign versus malignant diagnosis plus Breslow thickness if melanoma is detected.
Take Action Today—Don’t Wait
Use our comprehensive Symptom Checker right now to evaluate skin changes alongside other health symptoms and receive personalized urgency recommendations. Then schedule screening with a board-certified dermatologist within 48 hours if any warning signs are present. For broader cancer awareness, explore our complete health resources library covering early detection strategies for multiple cancer types.
Melanoma caught at stage 1 offers 98% survival. Stage 4 drops to 43%. The difference is testing now versus waiting. Your life depends on action today.
Medical Disclaimer
This article is for educational purposes only and does not constitute medical advice. Information presented is based on peer-reviewed research and clinical guidelines current as of January 2026. Always consult a board-certified dermatologist for personalized melanoma risk assessment, diagnosis, and treatment recommendations. Individual outcomes vary based on tumor characteristics, stage at diagnosis, patient health status, and treatment response. Emergency medical situations require immediate evaluation—do not delay seeking professional care.
Frequently Asked Questions About Melanoma
1. What are the first signs of melanoma?
Changes in existing moles or new dark spots showing asymmetry, irregular borders, multiple colors, diameter over 6mm, or evolving size/shape. Any mole that bleeds, itches, or looks different from others requires immediate evaluation.
2. Can melanoma be cured if caught early?
Yes. Stage 0-1 melanoma has 98-99% cure rates with simple surgical excision. Early detection through monthly self-exams and annual dermatologist screenings is critical for survival.
3. What does early stage melanoma look like?
Flat or slightly raised spots with irregular borders, uneven coloring (brown, black, red, blue), asymmetrical shape, and diameter exceeding a pencil eraser. Some appear as new dark moles after age 40.
4. How fast does melanoma spread?
Superficial spreading melanoma grows slowly over months to years. Nodular melanoma—the aggressive type—can metastasize within weeks to months if untreated. Stage determines spread speed.
5. What is the survival rate for stage 4 melanoma?
52% ten-year survival with modern immunotherapy combinations (nivolumab plus ipilimumab), compared to under 10% survival in the pre-immunotherapy era before 2011.
6. How much does melanoma treatment cost?
Stage 1 surgery: $6,500-$15,000. Stage 2-3 with immunotherapy: $200,000-$300,000. Stage 4 advanced treatment: $250,000-$400,000. Most insurance plans cover FDA-approved melanoma treatments.
7. Is melanoma only caused by sun exposure?
UV radiation causes 86% of melanomas, but genetic mutations, family history, immunosuppression, and other factors contribute. Acral lentiginous melanoma (on palms/soles) occurs without sun exposure.
8. Can you have melanoma with normal-looking moles?
Yes. Amelanotic melanoma lacks pigmentation and appears pink, red, or flesh-colored. These represent 2-8% of cases and are frequently misdiagnosed as benign lesions or eczema.
9. How long does a melanoma biopsy take?
10-15 minutes for the excisional biopsy procedure under local anesthesia. Pathology results return in 5-7 days confirming benign versus malignant diagnosis and Breslow thickness if cancer detected.
10. Does insurance cover melanoma screening?
Most private insurance covers annual full-body skin exams with copays of $0-$50. Medicare Part B covers preventive screenings when ordered by your primary care physician after deductible.
11. What’s the difference between moles and melanoma?
Normal moles are symmetrical, uniformly colored (tan/brown), under 6mm, with smooth borders that stay stable over time. Melanoma shows irregular shape, multiple colors, evolving characteristics, and the “ugly duckling” appearance—looking dramatically different from other moles on your body.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.











