Thyroid Cancer vs Nodule: Understanding the Critical Difference
Sarah, a 45-year-old marketing executive, felt a small bump on her neck while applying moisturizer one evening. “Is this thyroid cancer, or just a harmless lump?” she wondered, her mind racing with worry. Like millions of Americans discovering unexpected neck swelling, Sarah needed clear answers about the difference between thyroid nodules and thyroid cancer.
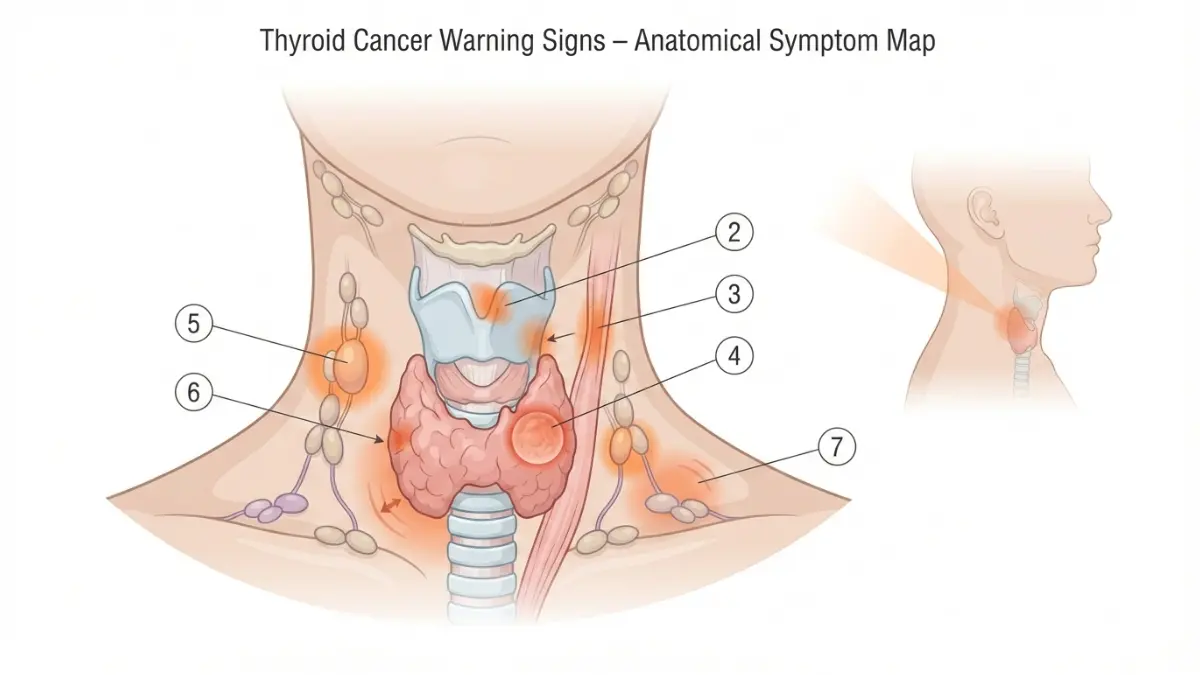
Thyroid cancer develops when abnormal cells grow uncontrollably in the thyroid gland, while thyroid nodules are lumps that form within the thyroid—and critically, 90-95% of these nodules are benign (non-cancerous). The 7 warning signs requiring immediate medical testing include: a rapidly growing neck lump, persistent voice hoarseness lasting over two weeks, difficulty swallowing or breathing, family history of thyroid conditions, a hard and immovable lump, enlarged lymph nodes in the neck, and previous radiation exposure to the head or neck area.
Why Understanding This Difference Matters
Thyroid nodules are surprisingly common—affecting up to 65% of the general population when detected through ultrasound screening. However, only 4-6.5% of these nodules turn out to be malignant, according to the National Cancer Institute. The SEER Cancer Statistics program reports that thyroid cancer affects approximately 13.5 per 100,000 people annually, with women being three times more likely to develop the disease than men.
Understanding early thyroid cancer signs and recognizing suspicious thyroid lump symptoms can dramatically improve outcomes. If you’re experiencing unexplained neck changes or have risk factors for thyroid cancer, using our Symptom Checker can help you document your symptoms before your medical appointment. For those with a family history of thyroid conditions, our Genetic Risk Assessment Tool provides personalized insights into hereditary cancer risks.
You’re not overreacting by seeking information—awareness of the difference between thyroid nodule vs cancer empowers you to advocate for appropriate testing when needed.
⚠️ MEDICAL DISCLAIMER
This article is for educational purposes and does not constitute medical advice. Always consult qualified healthcare providers for diagnosis, treatment decisions, and personalized medical guidance regarding thyroid nodules or thyroid cancer concerns.
7 Signs You Need Thyroid Cancer Tests Now
Recognizing early thyroid cancer signs can be lifesaving. While many thyroid nodules remain harmless throughout a person’s lifetime, specific warning indicators require immediate medical evaluation. The following seven red flags should prompt you to schedule thyroid testing without delay.
Sign #1: Rapidly Growing Neck Lump or Thyroid Nodule
Maria, a 52-year-old teacher, noticed a small neck bump during her morning routine. Within six months, the lump had doubled in size—a critical warning sign that led to her papillary thyroid cancer diagnosis.
Growth rate matters significantly. Research published by the Journal of Clinical Endocrinology & Metabolism demonstrates that malignant thyroid nodules grow substantially faster than benign ones, with cancerous nodules showing growth rates exceeding 2 millimeters per year. Benign nodules typically remain stable or grow minimally over time.
What This Means For You: If your thyroid lump symptoms include noticeable size increase over 6-12 months, request an ultrasound evaluation immediately. Document any visible changes with monthly photographs to track progression accurately.
Sign #2: Persistent Voice Hoarseness or Changes
Thyroid cancer neck lumps can press against the recurrent laryngeal nerve, which controls vocal cord function. According to NIH research on voice characteristics, hoarseness persisting beyond two weeks warrants medical investigation, especially when accompanied by neck swelling.
Voice changes associated with thyroid conditions include breathiness, reduced vocal range, and vocal fatigue. Unlike temporary hoarseness from colds or yelling, thyroid-related voice changes develop gradually and worsen progressively. When to see a doctor for thyroid concerns becomes critical if hoarseness coincides with other symptoms like difficulty swallowing or a palpable neck mass.
Sign #3: Difficulty Swallowing or Breathing
Dysphagia (difficulty swallowing) and respiratory issues occur when enlarged thyroid tissue compresses the esophagus or trachea. These thyroid lump symptoms represent more advanced disease and require urgent evaluation. Patients may feel food sticking in the throat, experience choking sensations, or notice breathing difficulties when lying flat.
The National Cancer Institute notes that compression symptoms typically indicate larger tumors or aggressive cancer types requiring immediate intervention. If you’re experiencing these symptoms alongside weight changes, checking your BMI Calculator can help document overall health status for your physician.
Sign #4: Family History of Thyroid Cancer
Approximately 20% of medullary thyroid cancer cases are hereditary, linked to genetic mutations in the RET gene. Follicular thyroid cancer also shows familial clustering patterns. If a first-degree relative (parent, sibling, or child) has been diagnosed with thyroid cancer, your risk increases 3-10 fold depending on the cancer subtype.
Genetic syndromes associated with increased risk include:
- Multiple Endocrine Neoplasia Type 2 (MEN2)
- Familial Adenomatous Polyposis (FAP)
- Cowden Syndrome
Use our Genetic Risk Assessment Tool to evaluate your hereditary risk factors. Individuals with confirmed family history should undergo baseline thyroid screening by age 20.
Sign #5: Hard, Immovable Lump in Neck
Texture provides critical diagnostic clues. Benign thyroid nodules typically feel soft and move freely when you swallow. Cancerous lumps often feel hard, irregular, and fixed to surrounding tissues. During physical examination, physicians assess nodule mobility, consistency, and attachment to nearby structures.
Signs of thyroid cancer based on palpation include firmness comparable to the tip of your nose (rather than the softness of your earlobe), irregular borders, and restriction of movement during swallowing. These characteristics, combined with rapid growth, warrant immediate thyroid biopsy.
Sign #6: Swollen Lymph Nodes in Neck
Papillary thyroid cancer frequently spreads to cervical lymph nodes—the lymph glands running along both sides of your neck. Research indicates that approximately 30-40% of papillary thyroid cancer patients present with lymph node involvement at initial diagnosis.
Suspicious lymph nodes feel firm, painless, and non-tender. They typically appear in the lateral neck compartments (sides of the neck) rather than under the jaw where viral infections commonly cause swelling. If you notice persistent neck lumps alongside other symptoms, immediate medical evaluation becomes essential.
Sign #7: Previous Radiation Exposure
Radiation exposure, particularly during childhood, represents one of the most significant risk factors for developing thyroid cancer. According to comprehensive NIH research on radiation-induced thyroid cancer, the risk increases significantly after exposure to doses exceeding 50-100 mGy (milligray), with maximum risk occurring when exposure happens during early childhood.
High-risk exposure scenarios include:
- Childhood radiation therapy for cancers like lymphoma or leukemia
- Multiple head/neck X-rays before age 18
- Proximity to nuclear accidents (Chernobyl, Fukushima)
- Dental X-rays performed repeatedly during developmental years
The latency period between radiation exposure and thyroid cancer development typically ranges from 5-30 years. Individuals with documented radiation history should undergo thyroid ultrasound screening every 1-2 years starting five years post-exposure.
Warning Sign Comparison Table
| Clinical Feature | Benign Thyroid Nodule | Suspicious for Thyroid Cancer | Recommended Action |
|---|---|---|---|
| Growth Rate | Stable or <2mm/year | >2mm/year or rapid enlargement | Immediate ultrasound + biopsy |
| Texture | Soft, rubbery, mobile | Hard, fixed, irregular borders | Fine needle aspiration required |
| Symptoms | Usually none | Voice hoarseness, dysphagia, pain | ENT and endocrinology referral |
| Lymph Nodes | Normal appearance | Enlarged, firm, painless | Comprehensive neck ultrasound |
| Voice Changes | None | Progressive hoarseness >2 weeks | Laryngoscopy examination |
| Family History | No specific pattern | Multiple relatives with thyroid cancer | Genetic testing + screening protocol |
Evidence Strength: HIGH — Based on prospective cohort studies and clinical guidelines from the American Thyroid Association and National Comprehensive Cancer Network.
Thyroid Nodule vs Cancer: Key Differences Explained
Understanding the distinction between benign thyroid nodules and malignant thyroid cancer requires knowledge of both conditions’ characteristics, prevalence, and risk factors. This section clarifies these critical differences to help you interpret your symptoms and test results more effectively.
What Are Thyroid Nodules?
Thyroid nodules are abnormal growths that develop within the thyroid gland tissue. These lumps can be solid, fluid-filled (cystic), or a combination of both. Research from NIH studies on benign thyroid disease indicates that up to 65% of the general population develops thyroid nodules by age 60, though most remain asymptomatic and undetected without imaging.
Common causes of benign thyroid nodules include:
- Hashimoto’s thyroiditis (autoimmune thyroid inflammation)
- Colloid nodules (fluid-filled sacs)
- Follicular adenomas (benign tumors)
- Multinodular goiter (multiple nodular growths)
- Iodine deficiency leading to compensatory thyroid enlargement
Benign nodules typically produce thyroid gland symptoms like visible neck swelling or, occasionally, hyperthyroidism when nodules become overactive. Unlike malignant growths, benign nodules remain stable in size over years and rarely cause compressive symptoms. Individuals experiencing unexplained thyroid-related symptoms alongside metabolic changes may benefit from comprehensive thyroid function testing.

Types of Thyroid Cancer
The National Cancer Institute classifies thyroid cancer into four primary types, each with distinct characteristics, prognosis, and treatment approaches.
Papillary Thyroid Cancer (80% of Cases)
Papillary thyroid cancer represents the most common and least aggressive form. This cancer type grows slowly, typically remains localized to the thyroid gland, and demonstrates excellent treatment outcomes. Data from NIH papillary carcinoma studies shows 5-year survival rates exceeding 99% for localized disease, with 10-year survival rates above 98%.
Key characteristics:
- Slow growth pattern over months to years
- Higher incidence in women (3:1 ratio)
- Often spreads to neck lymph nodes but remains highly curable
- Peak incidence between ages 30-50
Thyroid cancer symptoms in women often present subtly, with many papillary cancers discovered incidentally during imaging for unrelated conditions. The favorable prognosis makes papillary thyroid cancer one of the most successfully treated solid tumors.
Follicular Thyroid Cancer (10-15% of Cases)
Follicular thyroid cancer ranks as the second most common type, affecting slightly older populations than papillary cancer. According to StatPearls research on follicular carcinoma, this cancer type comprises 10-15% of all thyroid malignancies and demonstrates more aggressive behavior than papillary variants.
Unlike papillary cancer, follicular thyroid cancer can spread through blood vessels to distant organs, particularly bones and lungs. The 5-year survival rate ranges from 85-90% when diagnosed early, dropping to approximately 50-70% for cases with distant metastases.
Medullary Thyroid Cancer (3-4% of Cases)
Medullary thyroid cancer develops from parafollicular C-cells that produce calcitonin hormone rather than thyroid hormone. Approximately 20-25% of medullary cases are hereditary, linked to genetic mutations in the RET proto-oncogene. Families with multiple affected members should pursue genetic risk evaluation to identify mutation carriers who may benefit from prophylactic thyroid removal.
The NCI treatment guidelines emphasize that medullary thyroid cancer requires different management than differentiated cancers, as it doesn’t respond to radioactive iodine therapy. Five-year survival rates range from 80-86% overall, with localized disease achieving nearly 100% cure rates.
Anaplastic Thyroid Cancer (<2% of Cases)
Anaplastic thyroid cancer represents the most aggressive and rarest form. This undifferentiated cancer grows rapidly, typically presents at stage IV, and carries a median survival of only 6-7 months. Despite comprising less than 2% of thyroid cancers, anaplastic disease accounts for approximately 20% of thyroid cancer deaths.
Why Most Thyroid Nodules Aren’t Cancer
The overwhelming majority (90-95%) of thyroid nodules remain benign throughout a person’s lifetime. Understanding thyroid nodule vs cancer distinctions reduces unnecessary anxiety while promoting appropriate testing when warranted.
Thyroid Cancer Type Comparison
| Cancer Type | Frequency | 5-Year Survival (Localized) | Primary Risk Factor | Treatment Response |
|---|---|---|---|---|
| Papillary | 80% | 99% | Radiation exposure | Excellent (RAI responsive) |
| Follicular | 10-15% | 85-90% | Iodine deficiency | Good (RAI responsive) |
| Medullary | 3-4% | 80-86% | Genetic mutations (RET) | Moderate (RAI resistant) |
| Anaplastic | <2% | 7% | Age >60, long-standing goiter | Poor (aggressive growth) |
Evidence Level: HIGH — Data compiled from NCI SEER databases, NIH clinical studies, and American Thyroid Association guidelines 2023-2024.
How Doctors Diagnose Thyroid Cancer: Complete Testing Guide
Accurate thyroid cancer diagnosis requires a systematic approach combining physical examination, imaging studies, tissue sampling, and blood tests. Understanding each diagnostic step helps patients navigate the evaluation process with confidence and realistic expectations.
Physical Examination for Thyroid Cancer
The diagnostic journey typically begins with a thorough neck examination. Physicians palpate the thyroid gland to assess size, texture, symmetry, and nodule characteristics. During this examination, doctors evaluate whether lumps move with swallowing (a normal thyroid feature), feel firm or hard, and whether surrounding lymph nodes show enlargement.
Key examination findings suggesting cancer include:
- Hard, irregular nodules fixed to surrounding tissues
- Rapid growth documented over weeks to months
- Painless cervical lymphadenopathy (swollen neck lymph nodes)
- Vocal cord paralysis on laryngoscopy
- Thyroid cancer neck lump characteristics differing from benign goiters
When to see a doctor for thyroid concerns becomes urgent when examination reveals these suspicious features combined with symptoms like voice changes or swallowing difficulties.
Thyroid Ultrasound: First-Line Imaging
High-resolution thyroid ultrasound serves as the cornerstone imaging modality for evaluating thyroid nodules and establishing thyroid cancer diagnosis. This non-invasive test uses sound waves to create detailed images revealing nodule size, composition, borders, and suspicious features.
The ACR TI-RADS (Thyroid Imaging Reporting and Data System) provides standardized risk stratification based on five ultrasound characteristics: composition, echogenicity, shape, margin, and echogenic foci. Research published in NIH studies on TI-RADS performance demonstrates that this system reduces unnecessary biopsies by 19.9-46.5% compared to older guidelines while maintaining high sensitivity for detecting malignancy.
Suspicious ultrasound features include:
- Microcalcifications (tiny calcium deposits)
- Hypoechoic appearance (darker than surrounding tissue)
- Taller-than-wide shape on transverse view
- Irregular or spiculated margins
- Increased vascularity on Doppler imaging
The accuracy of thyroid ultrasound ranges from 85-90% for identifying suspicious thyroid nodule symptoms warranting biopsy. Cost typically ranges from $200-500, with most insurance plans covering the procedure when medically indicated.
Thyroid Biopsy: The Gold Standard
Fine Needle Aspiration (FNA) biopsy represents the definitive test for distinguishing benign nodules from thyroid cancer. This minimally invasive procedure uses a thin needle, typically guided by ultrasound, to extract cells from suspicious nodules for microscopic analysis.
The procedure takes approximately 10-20 minutes, involves minimal discomfort similar to a blood draw, and requires only local anesthesia. Most patients return to normal activities immediately afterward. Results typically arrive within 3-7 days, providing crucial information for treatment planning.

The Bethesda System for Reporting Thyroid Cytopathology standardizes FNA results into six categories with specific malignancy risks and management recommendations. According to comprehensive NIH analysis of the Bethesda classification, this system significantly improves diagnostic accuracy and clinical decision-making.
| Bethesda Category | Risk of Malignancy | Recommended Action |
|---|---|---|
| I – Nondiagnostic | 5-10% | Repeat FNA with ultrasound guidance |
| II – Benign | 0-3% | Clinical and ultrasound follow-up |
| III – AUS/FLUS | 10-30% | Repeat FNA or molecular testing |
| IV – Follicular Neoplasm | 25-40% | Consider surgery or molecular testing |
| V – Suspicious | 50-75% | Surgery recommended |
| VI – Malignant | 97-99% | Surgery required |
Core needle biopsy serves as an alternative when FNA yields inadequate samples or indeterminate results. This technique removes a small tissue core rather than individual cells, providing architectural information that enhances diagnostic accuracy.
Blood Tests for Thyroid Cancer Diagnosis
While blood tests cannot definitively diagnose thyroid cancer, they provide essential information about thyroid function and specific tumor markers. Understanding blood test results alongside other diagnostic markers helps create a complete clinical picture.
Essential blood tests include:
- TSH (Thyroid-Stimulating Hormone): Elevated TSH may indicate hypothyroidism; suppressed TSH suggests hyperthyroidism from overactive nodules
- Free T4 and T3: Assess actual thyroid hormone levels
- Calcitonin: Elevated levels indicate medullary thyroid cancer with 95% sensitivity
- Thyroglobulin: Used post-treatment to monitor for papillary and follicular thyroid cancer recurrence
- Carcinoembryonic Antigen (CEA): Often elevated in medullary thyroid cancer
Patients managing multiple health conditions may benefit from comprehensive metabolic monitoring using tools like our Blood Sugar Converter to track endocrine function holistically.
Advanced Molecular Testing
When thyroid biopsy results fall into indeterminate categories (Bethesda III-IV), molecular testing analyzes specific gene mutations and expression patterns to refine cancer risk assessment. These advanced tests examine genetic alterations commonly found in thyroid cancer, including BRAF, RAS, RET/PTC, and PAX8/PPARγ mutations.
Benefits of molecular testing:
- Reduces need for diagnostic surgery by 30-40%
- Provides risk stratification for indeterminate nodules
- Guides surgical extent (lobectomy vs. total thyroidectomy)
- Identifies targetable mutations for precision therapy
Cost ranges from $3,000-5,000, with variable insurance coverage. Many laboratories offer financial assistance programs for uninsured or underinsured patients.
Additional Imaging Studies
Beyond ultrasound, specialized imaging helps assess thyroid cancer stages and extent of disease:
- Radioiodine scan: Identifies functioning thyroid tissue and distant metastases in differentiated thyroid cancer
- CT scan: Evaluates tracheal compression and mediastinal extension
- MRI: Superior soft tissue resolution for assessing vascular invasion
- PET-CT: Detects metabolically active disease in recurrent or aggressive cancers
Diagnostic Testing Comparison
| Test Type | Primary Use | Accuracy | Average Cost | Typical Coverage |
|---|---|---|---|---|
| Thyroid Ultrasound | Initial evaluation | 85-90% | $200-500 | Usually covered |
| FNA Biopsy | Tissue diagnosis | 95%+ | $500-1,500 | Typically covered |
| Molecular Testing | Indeterminate nodules | 90-95% | $3,000-5,000 | Variable coverage |
| Thyroid Scan | Functional assessment | 80-85% | $300-800 | Often covered |
| Blood Tests (comprehensive) | Function/markers | N/A | $100-400 | Generally covered |
Evidence Strength: HIGH — Data compiled from American College of Radiology guidelines, NIH/NCI diagnostic protocols, and peer-reviewed validation studies 2023-2024.
Understanding Your Test Results
What This Means For You: If your thyroid biopsy returns as Bethesda III or IV (indeterminate), don’t panic. Molecular testing can provide clarity in 60-80% of these cases, potentially avoiding unnecessary surgery. Always request a copy of your pathology report and ultrasound findings to facilitate second opinions when needed.
Jennifer, 52, shares her experience: “My initial biopsy was indeterminate, which terrified me. Molecular testing showed low-risk genetic markers, so we chose active surveillance instead of immediate surgery. Three years later, the nodule remains stable—I avoided an operation I didn’t need.”
Thyroid Cancer Symptoms in Women and High-Risk Groups
Recognizing early thyroid cancer signs enables timely intervention and dramatically improves outcomes. While thyroid cancer affects both sexes, understanding gender-specific patterns and modifiable risk factors empowers proactive health management.
Common Thyroid Cancer Symptoms
Most thyroid cancers develop gradually, with symptoms appearing as the tumor grows or spreads beyond the thyroid gland. The most frequently reported signs of thyroid cancer include:
- Painless neck lump or swelling (present in 70-80% of cases at diagnosis)
- Persistent voice hoarseness lasting more than two weeks
- Difficulty swallowing (dysphagia) or sensation of food sticking
- Unexplained neck pain radiating to the ears
- Persistent cough unrelated to respiratory illness
- Breathing difficulties when lying flat
Thyroid lump symptoms often emerge slowly, with many patients dismissing initial changes as minor swellings. The hypothyroidism symptoms associated with underactive thyroid differ from cancer indicators, though both conditions can coexist.
Why Thyroid Cancer Affects Women More
Women develop thyroid cancer three times more frequently than men, with U.S. incidence rates of 20.2 per 100,000 women compared to 7.4 per 100,000 men. Research published in NIH studies on reproductive factors identifies hormonal influences as significant contributors to this gender disparity.
Thyroid cancer symptoms in women peak during reproductive years, with highest incidence occurring between ages 30-50. The age-specific pattern differs markedly from men, whose thyroid cancer rates peak later (ages 60-69). Hormonal factors including estrogen exposure, pregnancy history, and menopause timing appear to modulate thyroid cancer risk through mechanisms still under investigation.
Gender-specific considerations include:
- Pregnancy and postpartum periods show increased thyroid nodule detection
- Oral contraceptive use shows inconsistent associations across studies
- Early menopause (before age 45) may slightly increase risk
- Multiple pregnancies correlate with modest risk elevation
Women experiencing thyroid-related symptoms should track changes through our Symptom Checker before medical appointments to provide physicians with detailed symptom timelines.
Major Risk Factors for Thyroid Cancer
Radiation Exposure — Childhood radiation therapy to the head, neck, or chest represents the strongest established risk factor. The latency period between exposure and cancer development typically spans 5-30 years. Individuals with documented childhood radiation should undergo thyroid ultrasound screening beginning five years post-exposure.
Family History and Genetic Syndromes — Approximately 5% of papillary thyroid cancers and 20-25% of medullary thyroid cancers demonstrate hereditary patterns. Families with multiple affected relatives should pursue genetic counseling and consider prophylactic screening.
Gender — The 3:1 female-to-male ratio persists across all thyroid cancer subtypes except anaplastic, suggesting sex hormones influence cancer development.
Age — While thyroid cancer occurs across all age groups, differentiated types (papillary and follicular) peak during ages 30-60, whereas anaplastic cancer predominantly affects individuals over age 60.
Obesity — Elevated body mass index correlates with increased thyroid cancer risk. Analysis published in NIH obesity and thyroid cancer research demonstrates that each 5-point BMI increase raises thyroid cancer risk by approximately 30%. Calculate your current BMI using our BMI Calculator to assess this modifiable risk factor.
Iodine Deficiency or Excess — Both insufficient and excessive iodine intake alter thyroid cancer patterns, with deficiency increasing follicular cancer risk and excess potentially elevating papillary cancer incidence.
Early Detection Saves Lives
The overall 5-year survival rate for thyroid cancer exceeds 98%, largely due to early detection and effective treatment options. However, early thyroid cancer signs often manifest subtly, making awareness critical.
Self-neck examination technique:
- Stand before a mirror, tilt your head slightly backward
- Swallow water while observing your neck for unusual bulges
- Gently palpate both sides of your thyroid (below Adam’s apple, above collarbones)
- Note any lumps, asymmetry, or changes in texture
When to see a doctor for thyroid evaluation becomes urgent when you notice rapidly growing lumps, voice changes lasting beyond two weeks, or difficulty swallowing. Recognizing these warning signs parallels the importance of identifying early warning signs in other cancers, where prompt medical attention significantly impacts outcomes.
Can You Prevent Thyroid Cancer?
Most thyroid cancers arise without clear preventable causes. However, certain risk-reduction strategies include:
- Minimize unnecessary radiation exposure, especially during childhood
- Maintain healthy body weight through balanced nutrition; our Weight Loss Calculator provides personalized weight management guidance
- Genetic testing for high-risk families enables early intervention
- Avoid excessive iodine supplementation without medical indication
- Regular screening for individuals with identified risk factors
Thyroid Cancer Treatment Options and Survival Rates
Understanding thyroid cancer treatment approaches and prognosis empowers patients to make informed decisions and maintain realistic expectations throughout their cancer journey. Modern treatments offer exceptional outcomes, with overall 5-year survival rates exceeding 98%.
Treatment Approaches Based on Cancer Type
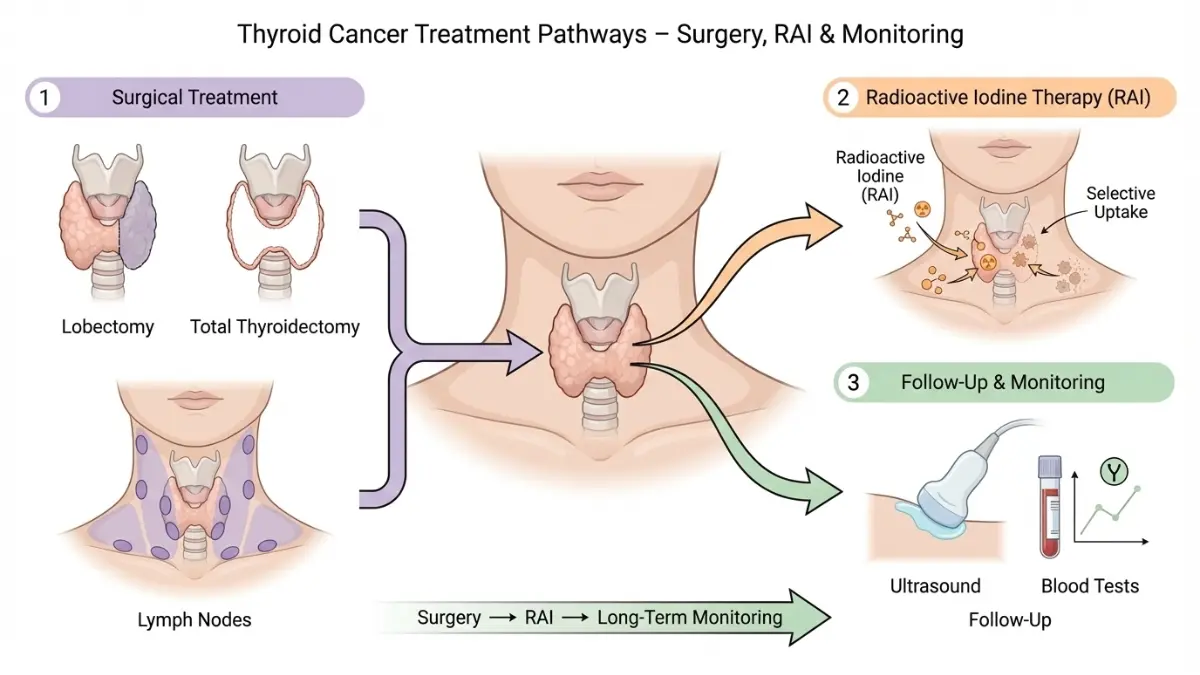
Surgical Treatment remains the primary intervention for most thyroid cancers. The National Cancer Institute treatment guidelines recommend either thyroid lobectomy (removal of one lobe) for small, low-risk tumors or total thyroidectomy (complete thyroid removal) for larger cancers or those with concerning features.
Lymph node dissection accompanies surgery when papillary thyroid cancer spreads to cervical lymph nodes—a common occurrence affecting 30-40% of patients at diagnosis. Surgical success rates exceed 95% for localized disease, with most patients returning to normal activities within 2-4 weeks. Post-operative care requires lifelong thyroid hormone replacement therapy to maintain metabolic functions, and patients should monitor their BMR Calculator results to ensure proper hormone dosing.
Radioactive Iodine (RAI) Therapy destroys remaining thyroid tissue and microscopic cancer cells after surgery. This targeted treatment works because thyroid cells uniquely absorb iodine. Research published in NIH studies on radioactive iodine mechanisms demonstrates that RAI selectively delivers beta-particle radiation to thyroid cells while sparing surrounding tissues.
RAI therapy proves most effective for papillary and follicular thyroid cancer but doesn’t benefit medullary or anaplastic types. Common temporary side effects include dry mouth, altered taste, and fatigue—conditions that often improve with adequate hydration using our Water Intake Calculator for personalized fluid requirements.
Advanced Treatment Options for aggressive or recurrent thyroid cancer include:
- External beam radiation therapy for tumors not responding to RAI
- Targeted therapy drugs (lenvatinib, sorafenib) for advanced medullary and anaplastic cancers
- Chemotherapy reserved for anaplastic thyroid cancer
- Clinical trials offering experimental treatments for refractory disease
Thyroid Cancer Prognosis by Stage
Thyroid cancer stages significantly influence survival outcomes. The American Joint Committee on Cancer (AJCC) staging system considers tumor size, lymph node involvement, distant metastases, patient age, and cancer type.
Survival Rates by Stage and Type
| Stage | Description | 5-Year Survival Rate | Primary Treatment |
|---|---|---|---|
| Stage I | Localized, small tumor | 99.9% | Surgery ± RAI therapy |
| Stage II | Larger tumor, confined to thyroid | 98.3% | Surgery + RAI therapy |
| Stage III | Regional lymph node spread | 93-95% | Surgery + RAI + monitoring |
| Stage IV | Distant metastasis | 55-74% (papillary) | Multi-modal therapy |
Evidence Strength: HIGH — Data from NCI SEER database, American Cancer Society statistics 2024, and peer-reviewed survival analyses.
Life After Thyroid Cancer Diagnosis
Most thyroid cancer survivors return to normal, healthy lives with appropriate follow-up care. Long-term management includes:
Regular Monitoring Schedule:
- Thyroid hormone blood tests every 6-12 months
- Thyroglobulin tumor marker checks for papillary and follicular cancers
- Neck ultrasound annually for 5 years, then as needed
- Whole-body radioiodine scans for high-risk patients
Hormone Replacement Management: Levothyroxine replaces thyroid hormone production after total thyroidectomy. Proper dosing maintains metabolism, energy levels, and prevents hypothyroidism symptoms. Patients experiencing persistent fatigue despite treatment should consult endocrinologists for medication adjustments.
Maintaining optimal sleep patterns supports recovery and hormone balance; our Sleep Calculator helps establish healthy sleep schedules during the recovery period.
What This Means For You: Even with stage IV thyroid cancer, targeted therapies and multimodal treatments extend life expectancy and maintain quality of life. The key lies in consistent follow-up care and staying committed to prescribed monitoring protocols.
When to Seek Immediate Medical Attention
Contact your healthcare provider urgently if you experience:
- New rapidly growing neck lumps after treatment
- Severe difficulty breathing or swallowing
- Persistent bone pain (possible metastasis)
- Sudden voice changes or hoarseness
- Unexplained weight fluctuations despite stable medication
Early intervention for recurrence significantly improves treatment success. Understanding warning signs across cancer types—similar to recognizing early lung cancer symptoms—enables prompt medical evaluation.
Frequently Asked Questions about Thyroid Cancer vs Nodule
1. What is the difference between a thyroid nodule and thyroid cancer?
A thyroid nodule is a lump in the thyroid gland, and 90-95% are benign. Thyroid cancer occurs when nodule cells become malignant and grow uncontrollably.
2. Can a thyroid nodule turn into cancer?
Yes, but only 4-6.5% of thyroid nodules become cancerous. Most remain benign throughout life with proper monitoring.
3. What are the first signs of thyroid cancer?
A painless neck lump, persistent hoarseness lasting over 2 weeks, difficulty swallowing, and enlarged lymph nodes in the neck are common first signs.
4. Is thyroid cancer curable?
Yes. Thyroid cancer has a 98% overall cure rate, with papillary thyroid cancer showing 99% 5-year survival when detected early.
5. How do doctors test for thyroid cancer?
Doctors use thyroid ultrasound, fine needle aspiration (FNA) biopsy, blood tests (TSH, calcitonin), and molecular testing to diagnose thyroid cancer.
6. Why is thyroid cancer more common in women?
Hormonal factors, including estrogen exposure, pregnancy, and reproductive history, increase thyroid cancer risk in women by 3-fold compared to men.
7. How fast does thyroid cancer grow?
Papillary and follicular thyroid cancers grow slowly over months to years. Anaplastic thyroid cancer grows rapidly within weeks to months.
8. Do all thyroid nodules need to be removed?
No. Only nodules with suspicious ultrasound features, rapid growth, or concerning biopsy results require surgery. Most are monitored with imaging.
9. What is the main treatment for thyroid cancer?
Surgery (thyroidectomy) is the primary treatment, often followed by radioactive iodine therapy to destroy remaining cancer cells.
10. Can thyroid cancer come back after treatment?
Yes, thyroid cancer can recur in 10-30% of cases, but recurrence is usually detected early through regular monitoring and remains highly treatable.
11. When should I see a doctor for a thyroid lump?
See a doctor immediately if your neck lump grows rapidly, feels hard and fixed, causes voice changes, or you have difficulty swallowing or breathing.
Take Action: Your Next Steps
Early detection through awareness of the 7 warning signs, combined with modern diagnostic tools and treatment options, means thyroid cancer ranks among the most successfully treated cancers. Trust your instincts when you notice unusual neck changes, advocate for appropriate testing when concerned, and remember that most thyroid nodules prove benign.
If you’re experiencing symptoms, document them using our comprehensive Symptom Checker before your appointment. For additional health guidance and tools, explore our complete health resources covering cancer prevention, diagnostic testing, and treatment support.
Your health deserves attention, and early action saves lives.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.