On This Page – Quick Medical Summary
Head and neck cancer encompasses malignancies affecting the oral cavity, throat, larynx, sinuses, and salivary glands, with a shocking 70% of throat cancers now caused by HPV infection rather than traditional tobacco use. The 2026 survival rates show dramatic differences between HPV-positive cases (82-95% five-year survival) and HPV-negative cases (57-62%), making early detection and HPV status critical to your prognosis.
Understanding Head and Neck Cancer: The HPV Revolution
What Is Head and Neck Cancer?
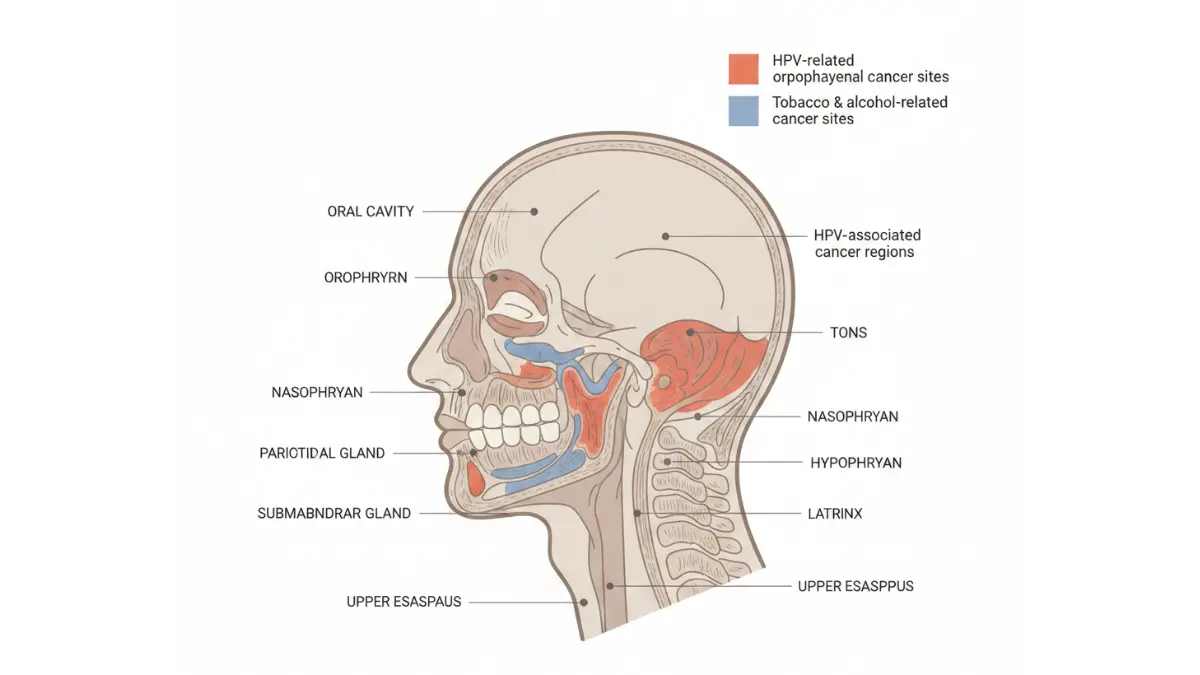
Head and neck cancer refers to a group of malignancies that develop in the squamous cells lining the moist surfaces of the mouth, throat, and nasal passages. These cancers can originate in multiple anatomical sites including the oral cavity, oropharynx (throat), larynx (voice box), hypopharynx (lower throat), nasopharynx (upper throat behind the nose), and salivary glands.
The American Cancer Society estimates 72,680 new cases of head and neck cancer will be diagnosed in the United States during 2026, with men being four times more likely to develop these cancers than women. The typical age at diagnosis ranges between 55 and 65 years old.
Types of head and neck cancer include:
- Oral cavity cancer: Affects lips, gums, tongue, floor of mouth, and hard palate
- Oropharyngeal cancer: Develops in the middle throat, including tonsils and base of tongue
- Laryngeal cancer: Forms in the voice box and vocal cords
- Hypopharyngeal cancer: Occurs in the lower throat area
- Nasopharyngeal cancer: Begins in the upper throat behind the nose
- Salivary gland cancer: Affects the glands that produce saliva
The HPV Epidemic: 70% of Throat Cancers Linked to Virus
The landscape of head and neck cancer has fundamentally shifted over the past two decades. Human papillomavirus (HPV) has emerged as the primary driver of oropharyngeal cancers, now surpassing cervical cancer as the most common HPV-related malignancy in the United States.
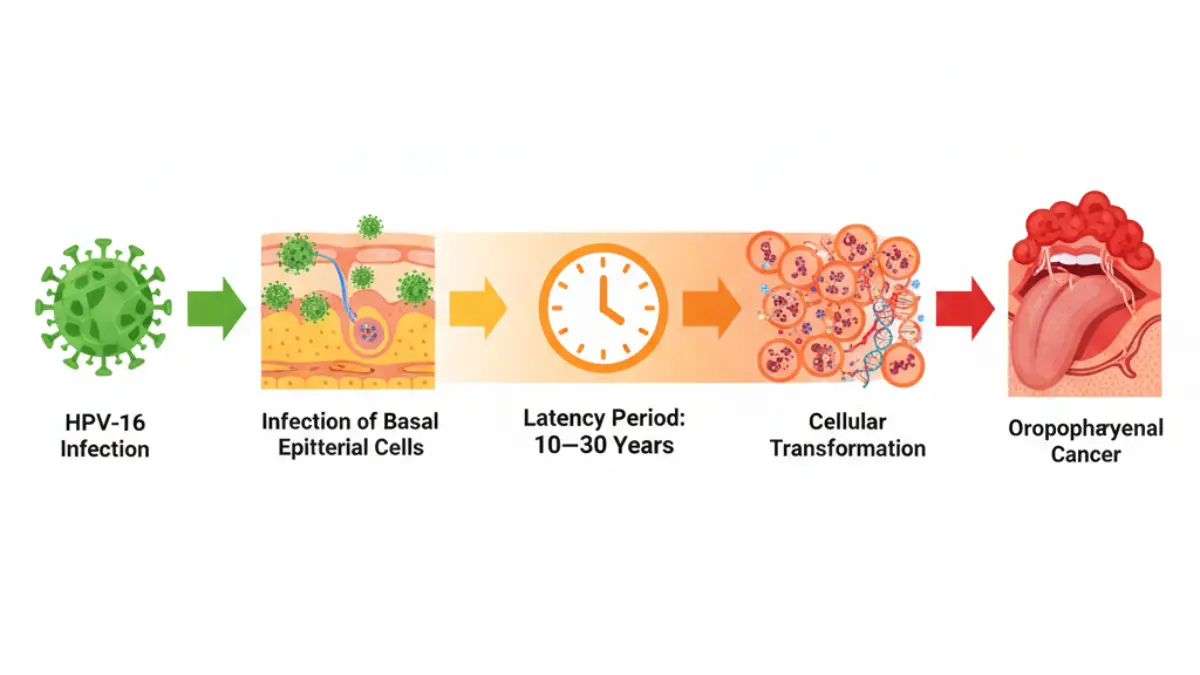
According to the Centers for Disease Control and Prevention, HPV causes approximately 39,300 cancers annually in the United States, with oropharyngeal cancer representing the largest category among men. Research published in 2026 shows that 70% of all throat cancers are now attributable to high-risk HPV types, particularly HPV-16.
This represents a dramatic epidemiological shift from historical patterns where tobacco and alcohol were the predominant risk factors. The National Cancer Institute confirms that HPV-related oropharyngeal cancer incidence has increased by more than 300% since the 1980s, with white men experiencing the highest rates at over 18 per 100,000 people.
The virus infects the basal cells of stratified squamous epithelia through microabrasions during sexual contact. HPV can remain dormant for 10 to 30 years before triggering malignant transformation, which explains why most patients diagnosed with HPV-related head and neck cancer are men in their 50s and 60s, despite acquiring the infection decades earlier.
HPV-Positive vs HPV-Negative: Two Different Diseases
Head and neck cancers must now be classified into two distinct categories based on HPV status, as they represent fundamentally different diseases with separate prognoses and treatment responses.
| Characteristic | HPV-Positive Cancer | HPV-Negative Cancer |
|---|---|---|
| Primary Cause | HPV-16 infection (>90% of cases) | Tobacco and alcohol use |
| 5-Year Survival Rate | 82-95% | 57-62% |
| Typical Patient | Non-smoker, younger (50s-60s) | Heavy smoker/drinker, older (60s-70s) |
| Treatment Response | Highly responsive to radiation/chemo | Moderate response, often requires surgery |
| Tumor Location | Base of tongue, tonsils | Oral cavity, larynx, hypopharynx |
| Genetic Profile | Fewer TP53 mutations | Frequent TP53 mutations, genomic complexity |
| Prognosis | 50% lower risk of death | Higher recurrence rates |
Research from Johns Hopkins Medicine demonstrates that patients with HPV-positive tumors have dramatically better outcomes even when presenting with advanced-stage disease. The superior prognosis relates to the tumors’ high responsiveness to radiation therapy and chemotherapy, as well as patients typically having fewer comorbidities.
A groundbreaking 2026 study published in Cancer and Metastasis Reviews revealed that genetic ancestry also influences tumor biology and survival rates. African American patients with head and neck cancer survive an average of 2.5 years compared to 4.8 years for European American patients, highlighting the importance of personalized treatment approaches.
If you’re concerned about cancer risk factors, our Genetic Risk Assessment Tool can help evaluate your personal risk profile based on family history and lifestyle factors.
Symptoms and Early Detection: When to See a Doctor
10 Warning Signs You Shouldn’t Ignore
Early detection of head and neck cancer dramatically improves survival outcomes, with stage I and II cancers showing 70-90% five-year survival rates compared to just 30-50% for stage IV disease. Recognizing warning signs promptly can be lifesaving.
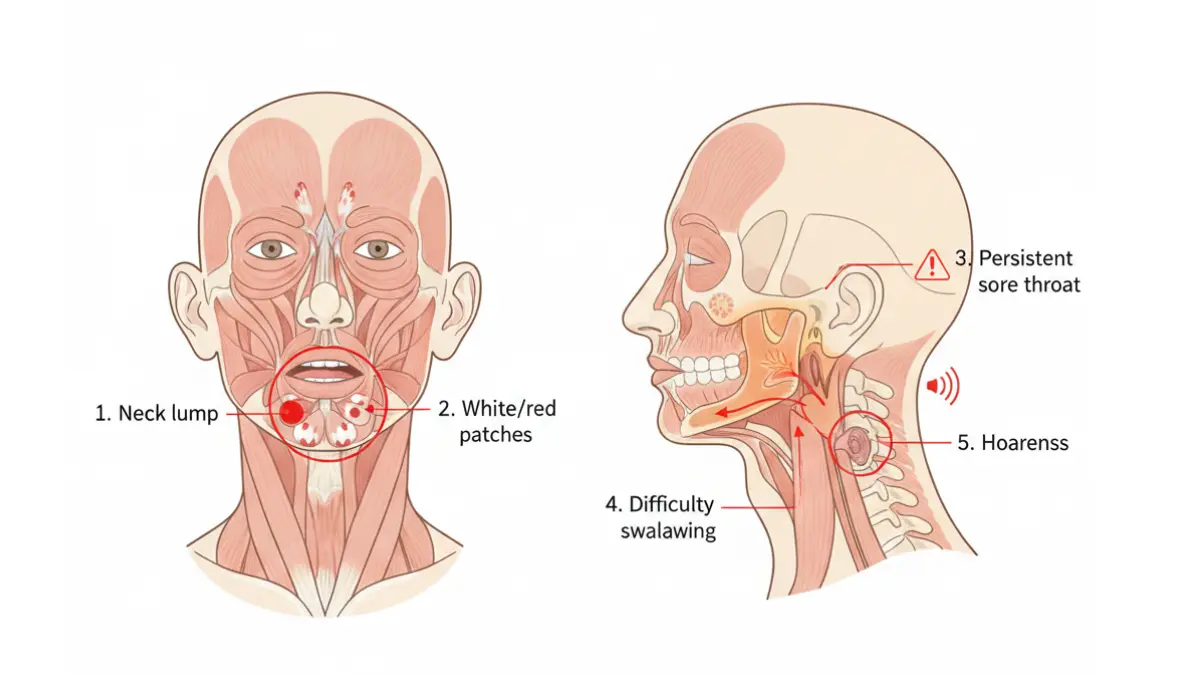
Critical symptoms requiring medical evaluation:
- Persistent sore throat: Lasting more than 2-3 weeks without improvement
- Neck lump: Painless mass that doesn’t resolve within 2-3 weeks (often the first sign of HPV-positive throat cancer)
- Hoarseness or voice changes: Raspy, weak, or altered voice persisting beyond two weeks
- Difficulty swallowing (dysphagia): Pain or obstruction when eating or drinking
- Unexplained ear pain: Especially when the ear appears normal on examination
- Non-healing mouth sore: Ulcer or lesion lasting more than three weeks
- White or red patches: Leukoplakia (white) or erythroplakia (red) patches in the mouth
- Unexplained weight loss: Significant weight reduction without dietary changes
- Persistent bad breath: Halitosis that doesn’t improve with oral hygiene
- Difficulty breathing: Obstruction or stridor (high-pitched breathing sounds)
According to the American Cancer Society, the most common initial presentation of HPV-related oropharyngeal cancer is a painless neck mass, which indicates the cancer has already spread to lymph nodes. This differs from traditional tobacco-related cancers that typically present with oral symptoms first.
Self-Check Guide: Assess Your Risk at Home
While professional medical examination remains essential, you can perform preliminary self-assessments to monitor for changes. Use our Symptom Checker to evaluate your symptoms and determine urgency levels.
Monthly oral self-examination steps:
- Visual inspection: Use a bright light and mirror to examine all surfaces inside your mouth, including cheeks, gums, tongue (top and underside), and roof of mouth
- Texture check: Run your finger along gums and inner cheeks feeling for lumps, rough patches, or tender areas
- Lymph node palpation: Gently feel both sides of your neck from jawline to collarbone, checking for enlarged, firm, or immovable masses
- Functional assessment: Note any changes in voice quality, swallowing ability, or jaw movement
High-risk indicators requiring immediate evaluation:
- Any oral lesion persisting beyond three weeks
- Leukoplakia or erythroplakia patches
- Neck mass that hasn’t resolved within 2-3 weeks
- Persistent hoarseness lasting over two weeks
- Difficulty swallowing with progressive worsening
Why Early Detection Saves Lives
The stage at diagnosis profoundly impacts survival outcomes. Data from the Surveillance, Epidemiology, and End Results (SEER) Program shows dramatic survival differences based on when head and neck cancer is detected.
Five-year survival rates by stage:
- Localized (confined to primary site): 83-85%
- Regional (spread to nearby lymph nodes): 66-68%
- Distant (metastasized to other organs): 39-42%
- All stages combined: 65-68%
Unfortunately, approximately 50% of patients present with advanced-stage disease (stage III or IV) at diagnosis, largely because early symptoms are often mistaken for common conditions like chronic sore throat or allergies. This underscores the critical importance of seeking medical evaluation for persistent symptoms, particularly if you have risk factors like HPV exposure, tobacco use, or heavy alcohol consumption.
For patients concerned about cancer detection, understanding your body’s baseline is crucial. Maintaining optimal health through proper nutrition—trackable with our Macro Calculator—supports immune function and overall wellbeing during screening and potential treatment.
2026 Survival Rates: What the Latest Data Shows
Overall Survival Statistics by Stage
The 2026 survival data for head and neck cancer reveals significant variation based on cancer subtype, stage at diagnosis, and HPV status. Understanding these statistics helps patients and families set realistic expectations while recognizing that individual outcomes vary.
Comprehensive survival rates by cancer type and stage:
| Cancer Type | Localized (Stage I-II) | Regional (Stage III) | Distant (Stage IV) | Overall 5-Year |
|---|---|---|---|---|
| Oral Cavity | 84% | 66% | 39% | 68% |
| Oropharynx (HPV+) | 92-95% | 85-90% | 70-75% | 85-90% |
| Oropharynx (HPV-) | 70-75% | 55-62% | 30-40% | 57-62% |
| Larynx | 77% | 59% | 44% | 62% |
| Hypopharynx | 59% | 50% | 32% | 50% |
| Nasopharynx | 85% | 72% | 60% | 73% |
Data compiled from the National Cancer Institute SEER database shows that overall five-year survival for all head and neck cancers combined has improved to 65.9% in 2026, up from 54.7% in the 1990s. This improvement is largely attributed to better treatment of HPV-positive oropharyngeal cancers and advances in multimodal therapy approaches.
HPV-Positive vs HPV-Negative Outcomes
The presence or absence of HPV fundamentally alters prognosis and represents one of the most important prognostic factors in head and neck cancer. Research from the Radiation Therapy Oncology Group (RTOG) demonstrated that HPV status creates distinct risk categories even among patients with identical tumor stages.
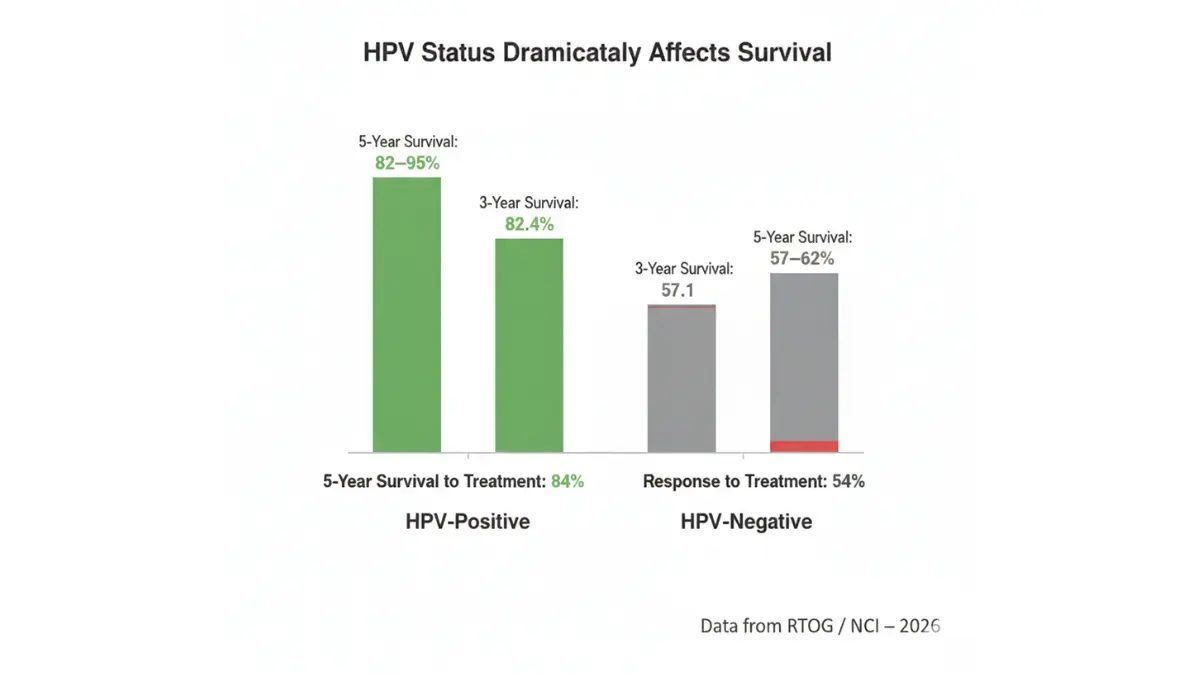
Three-year survival comparison from landmark RTOG study:
- HPV-positive patients: 82.4% overall survival
- HPV-negative patients: 57.1% overall survival
- Risk of death reduction: HPV-positive patients have 50% lower risk of death
The superior outcomes in HPV-positive disease stem from several biological factors. HPV-related tumors demonstrate exceptional radiosensitivity, meaning they respond dramatically to radiation therapy. Additionally, these patients are typically younger non-smokers with fewer medical comorbidities, allowing them to tolerate aggressive treatment regimens better.
A 2026 analysis showed that among oropharyngeal cancer patients receiving standard chemoradiation:
- HPV-positive response rate: 84% complete response
- HPV-negative response rate: 54% complete response
- Two-year survival (HPV-positive): 95%
- Two-year survival (HPV-negative): 62%
New Research: Genetic Ancestry and Survival
One of the most significant discoveries in 2026 head and neck cancer research involves the role of genetic ancestry in tumor biology and patient outcomes. A groundbreaking study from the University of Maryland School of Medicine, published in Cancer and Metastasis Reviews, analyzed data from 523 patients to reveal profound ancestry-related differences.
Key findings from genetic ancestry research:
Survival disparities:
- African American patients: 2.5-year median survival
- European American patients: 4.8-year median survival
- Nearly 2x survival difference based on genetic ancestry
Biological mechanisms identified:
- Ancestry influences patterns of tumor mutations and DNA alterations
- Different genetic backgrounds show distinct gene activity profiles
- Some ancestry-associated changes may be protective while others promote aggressive disease
- Tumor response to chemotherapy varies by ancestry-related genetic factors
This research challenges the previous assumption that survival disparities between racial groups were solely due to socioeconomic factors like healthcare access or smoking rates. While these remain important contributors, the data demonstrates that tumors arising in patients with different genetic ancestries exhibit distinct biological features, including variations in key genes affecting cell growth and treatment response.
The implications for personalized medicine are profound. As precision oncology advances, treatment protocols may need customization based on a patient’s genetic background to optimize outcomes. This represents a shift toward truly individualized cancer care rather than one-size-fits-all approaches.
For patients navigating cancer treatment, maintaining optimal nutrition becomes critical. Our Protein Intake Calculator helps ensure adequate protein consumption to support tissue repair and immune function during therapy.
Causes, Risk Factors & Prevention Strategies
Primary Risk Factors: Beyond Tobacco and Alcohol
While tobacco and alcohol historically dominated head and neck cancer etiology, the risk factor landscape has evolved dramatically. Understanding all contributing factors enables more targeted prevention strategies.
Major risk factors and their impact:
HPV infection (70% of oropharyngeal cancers)
- High-risk HPV types, particularly HPV-16, cause the majority of throat cancers
- 80+ million Americans currently have HPV
- 13 million new infections occur annually in the United States
- 10-30 year latency period between infection and cancer development
Tobacco use (173% increased risk even with HPV)
- Cigarette smoking remains the strongest traditional risk factor
- Smokeless tobacco (chewing tobacco, snuff) causes oral cavity cancers
- Pipe and cigar smoking carry similar risks
- Even among HPV-positive patients, tobacco use significantly worsens outcomes
Alcohol consumption (166% increased risk)
- Heavy alcohol use (more than 8-14 drinks weekly) substantially increases risk
- Alcohol and tobacco act synergistically—combined use multiplies risk
- Alcohol-related head and neck cancers typically affect the oral cavity and hypopharynx
Demographic factors:
- Age: Risk increases dramatically after age 50, peaking at 55-65
- Sex: Men are 4x more likely to develop head and neck cancer than women
- Race/ethnicity: White men show highest rates of HPV-positive oropharyngeal cancer
Occupational and environmental exposures:
- Wood dust exposure (nasopharyngeal cancer risk)
- Asbestos and synthetic fiber exposure (laryngeal cancer)
- Construction, metal, textile, and logging industries show elevated risk
- Poor oral hygiene and chronic inflammation
HPV Transmission: What You Need to Know
HPV is the most common sexually transmitted infection globally, and understanding transmission dynamics is essential for prevention. Unlike bacteria, HPV spreads through direct skin-to-skin contact during intimate activity.
HPV transmission facts:
- Transmission routes: Vaginal, anal, and oral sexual contact
- Contagiousness: Highly contagious; most sexually active people will acquire HPV at some point
- Asymptomatic spread: Most people with HPV have no symptoms and unknowingly transmit the virus
- Persistence: In some individuals, HPV persists rather than being cleared by the immune system
- Cancer development: Only a small fraction of HPV infections progress to cancer
Sexual behavior and cancer risk (research data):
According to studies published by the American Cancer Society:
- 1-5 oral sex partners: 2x higher risk of HPV-related cancer
- 6+ oral sex partners: 5x higher risk of HPV-related cancer
- Age at first sexual activity: Earlier sexual debut correlates with increased risk
- Number of lifetime partners: Direct correlation with HPV exposure probability
The latency period between HPV infection and cancer development creates a critical window. HPV can remain dormant in tonsillar crypts and the base of tongue for decades before malignant transformation occurs. This explains why typical head and neck cancer patients are diagnosed in their 50s and 60s despite likely acquiring HPV in their 20s or 30s.
5 Evidence-Based Prevention Steps
Prevention strategies must address both traditional and emerging risk factors. The following evidence-based interventions significantly reduce head and neck cancer risk.
1. HPV Vaccination (Most Effective Prevention)
The HPV vaccine (Gardasil 9) protects against nine high-risk HPV types responsible for over 90% of HPV-related cancers. CDC recommendations include:
- Routine vaccination: All children at age 11-12 (can start at age 9)
- Catch-up vaccination: Through age 26 for those not previously vaccinated
- Adult vaccination: Available through age 45 for select individuals
- Dosing schedule: 2 doses (6-12 months apart) for ages 9-14; 3 doses for ages 15+
- Effectiveness: Over 270 million doses administered with excellent safety record
- Cancer prevention: Prevents >90% of oropharyngeal, cervical, anal, vulvar, vaginal, and penile cancers
2. Tobacco Cessation
Complete tobacco avoidance provides the single greatest reduction in traditional head and neck cancer risk:
- Smoking cessation reduces risk by 35% within 1-4 years
- Risk continues declining, reaching near-baseline after 20+ years
- Even among HPV-positive patients, quitting smoking improves treatment outcomes
- Smokeless tobacco users should transition to cessation programs
- Resources: Smokefree.gov, 1-800-QUIT-NOW
3. Moderate Alcohol Consumption
Limiting alcohol intake substantially reduces risk, particularly when combined with tobacco avoidance:
- Men: Maximum 2 drinks per day
- Women: Maximum 1 drink per day
- Heavy drinkers: Greatest benefit from reduction or elimination
- Synergistic effect: Eliminating both tobacco and alcohol provides multiplicative protection
4. Regular Dental and Medical Examinations
Professional oral examinations can detect precancerous lesions and early-stage cancers:
- Dental visits: Every 6 months with complete oral cavity examination
- Medical checkups: Annual physical including neck palpation
- High-risk individuals: More frequent monitoring (every 3-4 months)
- Precancerous lesions: Leukoplakia and erythroplakia require biopsy and close monitoring
5. Safe Sexual Practices
While not fully protective, safer practices reduce HPV transmission risk:
- Barrier methods: Condoms and dental dams provide partial protection (do not eliminate risk)
- Partner limitation: Fewer lifetime sexual partners correlates with reduced HPV exposure
- Vaccination priority: Remains the most effective preventive measure
- Open communication: Discussing HPV status with partners
For individuals focused on overall health optimization during prevention efforts, maintaining ideal body composition supports immune function. Our Body Fat Calculator helps track this important health metric.
Understanding preventable cancer risks mirrors the importance of recognizing other cancer warning signs. Our comprehensive guide on cervical cancer symptoms women ignore provides additional HPV-related cancer education.
Treatment Options and Recovery: 2026 Advances
Standard Treatment Approaches by Stage
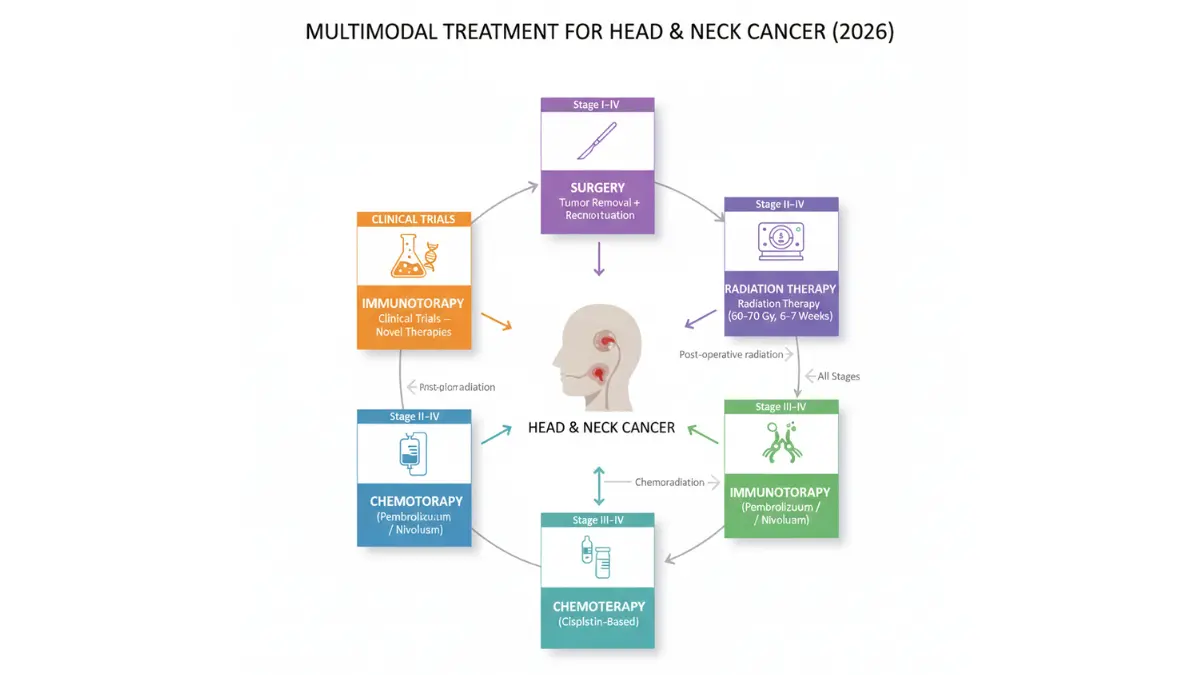
Head and neck cancer treatment requires a multimodal approach tailored to tumor stage, location, HPV status, and patient health. The goal is cancer eradication while preserving critical functions like speech, swallowing, and breathing.
Treatment strategies by stage:
Stage I-II (Early-Stage Disease)
Single-modality treatment often achieves excellent outcomes:
- Surgery alone: Wide local excision with clear margins
- Radiation therapy alone: Definitive radiation (60-70 Gy over 6-7 weeks)
- Minimally invasive options: Transoral robotic surgery (TORS) for select oropharyngeal tumors
- 5-year survival: 70-90% depending on subsite
Stage III-IV (Advanced-Stage Disease)
Multimodal therapy combining treatments:
- Surgery + adjuvant radiation: Tumor removal followed by radiation to eliminate microscopic disease
- Surgery + chemoradiation: For high-risk features (positive margins, lymph node involvement)
- Definitive chemoradiation: Concurrent chemotherapy and radiation without surgery
- Neoadjuvant chemotherapy: Pre-treatment to shrink tumors before definitive therapy
Standard chemotherapy regimens:
- Cisplatin-based: 100 mg/m² every 3 weeks during radiation (most common)
- Carboplatin + 5-FU: Alternative for cisplatin-intolerant patients
- Cetuximab: Monoclonal antibody targeting EGFR, used with radiation
Surgical approaches:
- Transoral robotic surgery (TORS): Minimally invasive approach for oropharyngeal tumors
- Open surgical resection: Traditional approach for larger tumors
- Neck dissection: Removal of lymph nodes when cancer has spread
- Reconstructive surgery: Free flap procedures to restore appearance and function
New Immunotherapy Breakthroughs
The 2026 treatment landscape includes groundbreaking immunotherapy options that harness the patient’s immune system to fight cancer. These therapies represent the most significant advance in head and neck cancer treatment in decades.
FDA-approved immunotherapy agents:
Pembrolizumab (Keytruda)
- Mechanism: PD-1 checkpoint inhibitor
- Indications: Recurrent/metastatic head and neck cancer, first-line treatment with chemotherapy
- Response rates: 15-20% as monotherapy; higher in combination
- Duration of response: Often prolonged (12+ months in responders)
Nivolumab (Opdivo)
- Mechanism: PD-1 checkpoint inhibitor
- Indications: Recurrent/metastatic disease after platinum chemotherapy
- Survival benefit: Improved overall survival vs. standard chemotherapy
- Tolerability: Generally better tolerated than traditional chemotherapy
2026 Clinical Trial Developments:
- De-escalation studies: Testing reduced-intensity treatment for HPV-positive patients to minimize side effects while maintaining cure rates
- Combination immunotherapy: Dual checkpoint blockade (PD-1 + CTLA-4 inhibitors)
- Personalized vaccines: Tumor-specific neoantigen vaccines in early trials
- CAR-T cell therapy: Engineered immune cells targeting tumor antigens
Research from the National Institutes of Health shows over 200 active clinical trials for head and neck cancer in 2026, offering patients access to cutting-edge therapies not yet widely available.
Recovery Timeline: What to Expect
Recovery from head and neck cancer treatment is a gradual process that varies based on treatment modality and individual factors. Understanding the typical timeline helps patients and caregivers prepare for the journey.
Comprehensive recovery timeline:
| Time Period | Physical Recovery | Treatment Milestones | Common Challenges |
|---|---|---|---|
| Week 1-2 | Post-surgical healing, hospitalization | Pain management, nutrition support (feeding tube possible) | Swelling, pain, limited oral intake |
| Week 3-6 | Radiation/chemo side effects peak | Ongoing daily radiation, weekly chemo | Mucositis, fatigue, taste changes, weight loss |
| Week 7-12 | Acute side effects begin resolving | Treatment completion, first post-treatment scans | Persistent dysphagia, continued weight loss |
| Month 3-6 | Gradual functional improvement | Speech/swallow therapy intensive | Difficulty eating solid foods, voice changes |
| Month 6-12 | Continued healing and adaptation | Surveillance imaging (PET/CT at 3 months) | Dry mouth (xerostomia), dental complications |
| Year 1-2 | New baseline established | Follow-up every 2-3 months | Thyroid dysfunction, lymphedema |
| Year 2-5 | Long-term adaptation | Follow-up every 3-6 months | Chronic effects management |
| Year 5+ | Survivorship phase | Annual follow-up | Late effects surveillance |
Common treatment side effects:
Immediate (during treatment):
- Severe mucositis (mouth and throat sores)
- Dysphagia (difficulty swallowing)
- Odynophagia (painful swallowing)
- Dermatitis (skin inflammation in radiation field)
- Fatigue
- Taste alterations
- Nausea
Intermediate (weeks to months after treatment):
- Xerostomia (dry mouth) from salivary gland damage
- Trismus (limited jaw opening)
- Voice changes and hoarseness
- Nutritional deficiencies requiring feeding tube
- Weight loss (average 10-20% of body weight)
- Dental decay from reduced saliva
Long-term (months to years):
- Chronic xerostomia (often permanent)
- Hypothyroidism requiring hormone replacement
- Lymphedema of face and neck
- Osteoradionecrosis (bone damage from radiation)
- Carotid artery stenosis
- Secondary malignancies
Supportive care essentials:
- Speech/language pathology: Swallowing therapy (dysphagia rehabilitation) and voice therapy
- Nutrition support: Dietitian guidance, possible feeding tube (PEG or NG tube)
- Dental care: Fluoride treatments, preventive care for radiation-related decay
- Physical therapy: Neck and shoulder exercises after surgery/radiation
- Pain management: Multimodal approach including medications, nerve blocks
- Mental health: Counseling for anxiety, depression, body image concerns
Maintaining adequate nutrition during treatment remains paramount. Our Calorie Deficit Calculator helps patients and caregivers ensure appropriate caloric intake during recovery when eating becomes challenging.
For patients undergoing surgery as part of their treatment plan, understanding surgical recovery timelines across different procedures can be valuable. Our guide on laparoscopic surgery success rates provides additional surgical outcome information.
Living with Head and Neck Cancer: Support and Outlook
Emotional and Psychological Support
The psychological impact of head and neck cancer extends beyond physical symptoms. Patients face unique emotional challenges due to visible treatment effects, functional impairments, and concerns about appearance and social interaction.
Common psychological challenges:
- Anxiety and depression: Affecting 30-50% of patients
- Body image concerns: Surgical changes, weight loss, scarring
- Social withdrawal: Due to speech difficulties or appearance changes
- Fear of recurrence: Particularly intense in the first 2-3 years
- Role changes: Career interruptions, dependency on caregivers
- Relationship strain: Communication difficulties, intimacy concerns
A 52-year-old teacher named Michael was diagnosed with HPV-positive tonsil cancer in 2024. After completing chemoradiation therapy, he experienced profound depression related to his altered voice and difficulty teaching. Through participation in a head and neck cancer support group and individual counseling, he gradually adapted to his “new normal” and successfully returned to teaching part-time within one year. His five-year prognosis remains excellent at 90%+ given his HPV-positive status and complete response to treatment.
Support resources:
- Multidisciplinary care teams: Oncologists, surgeons, nurses, social workers coordinating care
- Support groups: CancerCare, Cancer Support Community, hospital-based programs
- Speech-language pathologists: Voice and swallowing rehabilitation specialists
- Nutritionists: Specialized guidance for patients with eating difficulties
- Mental health professionals: Psychologists and psychiatrists familiar with cancer patients
- Patient navigators: Assistance coordinating appointments and resources
Caregiver considerations:
Research shows that caregivers of head and neck cancer patients experience higher stress levels, depression rates, and anxiety compared to both the general population and caregivers of patients with other cancer types. The complex care requirements—including wound management, feeding tube care, and tracheostomy maintenance—create substantial caregiver burden.
Caregivers should:
- Attend medical appointments when possible
- Participate in training for home care procedures
- Seek respite care when available
- Join caregiver support groups
- Maintain their own health through regular checkups
- Recognize signs of caregiver burnout
Long-Term Surveillance and Follow-Up
Lifelong surveillance remains essential for head and neck cancer survivors due to risks of recurrence and second primary cancers. The intensity of follow-up gradually decreases over time.
Standard surveillance schedule:
Year 1 (highest recurrence risk):
- Clinic visits: Every 1-3 months
- Physical examination: Complete head and neck exam including laryngoscopy
- Imaging: PET/CT at 3 months post-treatment (baseline), additional imaging as clinically indicated
- Laboratory tests: Thyroid function testing (TSH) every 6 months
Years 2-3:
- Clinic visits: Every 2-4 months
- Physical examination: Continued vigilance for recurrence
- Imaging: Annual chest imaging to screen for lung cancer (especially in smokers)
- Dental evaluation: Every 3-4 months due to radiation effects
Years 4-5:
- Clinic visits: Every 4-6 months
- Physical examination: Ongoing surveillance
- Imaging: As clinically indicated
Beyond year 5:
- Clinic visits: Annually
- Screening: Continue screening for second primary cancers
- Lifestyle: Maintain tobacco/alcohol avoidance, HPV awareness
Second primary cancer risk:
Head and neck cancer survivors face elevated risk of developing new primary cancers:
- Lung cancer: Highest risk, particularly in former smokers (3-7% annual risk)
- Esophageal cancer: Elevated risk from shared risk factors
- Second head and neck cancer: 3-5% annual risk
- Other tobacco-related cancers: Bladder, kidney, pancreas
When to Seek Immediate Medical Attention
Despite successful treatment, head and neck cancer can recur. Recognizing recurrence warning signs enables early intervention.
Red flags requiring immediate evaluation:
- New or enlarging neck mass: Especially firm, fixed, or painless lumps
- Progressive swallowing difficulty: Worsening dysphagia or complete obstruction
- Increasing pain: New or escalating pain in the head, neck, or throat
- Unexplained bleeding: From mouth, nose, or throat
- Voice changes: New hoarseness or voice quality deterioration
- Neurological symptoms: Numbness, weakness, vision changes
- Breathing difficulty: Stridor or progressive shortness of breath
- Unexplained weight loss: Significant unintentional weight reduction
Emergency situations:
- Severe bleeding that doesn’t stop with pressure
- Inability to swallow saliva or medications
- Acute breathing difficulty or airway obstruction
- Sudden severe pain uncontrolled by medications
- Signs of infection (high fever, wound drainage, severe swelling)
Recurrence patterns:
According to data from the American Society of Clinical Oncology, approximately 50-60% of recurrences occur within the first two years after treatment, with 80-90% occurring within five years. This pattern reinforces the importance of intensive early surveillance.
Hope and improving outcomes:
The outlook for head and neck cancer patients has never been better, particularly for those with HPV-positive disease. Five-year survival rates have increased by more than 20 percentage points over the past three decades. Advances in immunotherapy, targeted therapy, and de-escalation protocols for HPV-positive patients promise further improvements.
For individuals who have completed treatment and are focused on long-term health maintenance, understanding overall wellness markers becomes important. Tools like our Sleep Calculator help optimize recovery through proper rest patterns.
The cancer survivorship journey includes monitoring for other health concerns. Our comprehensive guides on thyroid cancer symptoms and lung cancer early warning signs provide additional screening education for survivors at elevated risk of second primary cancers.
Frequently Asked Questions
1. Can HPV vaccine prevent head and neck cancer?
Yes, the HPV vaccine (Gardasil 9) prevents infection with HPV types 16 and 18, which cause over 90% of HPV-related head and neck cancers. Vaccination is most effective when given before sexual activity begins (ages 11-12) but provides benefits through age 45.
2. What’s the difference between HPV-positive and HPV-negative throat cancer?
HPV-positive throat cancer has an 82-95% five-year survival rate, responds better to treatment, and typically affects younger non-smokers. HPV-negative cancer has a 57-62% five-year survival rate, often requires more aggressive treatment, and occurs primarily in older smokers and heavy drinkers.
3. How long can you live with untreated head and neck cancer?
Median survival for untreated head and neck cancer ranges from 4-11 months depending on tumor site and stage. Early treatment dramatically improves outcomes, with stage I-II cancers showing 70-90% five-year survival with appropriate therapy.
4. Is head and neck cancer curable if caught early?
Yes, early-stage (I-II) head and neck cancer is highly curable, with 70-90% of patients achieving five-year disease-free survival. Treatment typically involves surgery or radiation alone, avoiding the need for chemotherapy.
5. Can you get throat cancer from oral sex?
Yes, HPV transmission during oral sex can lead to throat cancer years or decades later. Research shows that having 6+ oral sex partners increases HPV-related head and neck cancer risk by 5 times compared to those with 0-1 partners.
6. What are the first signs of throat cancer?
The most common first sign of throat cancer is a painless neck lump (enlarged lymph node). Other early symptoms include persistent sore throat lasting 2+ weeks, hoarseness, difficulty swallowing, and unexplained ear pain.
7. Do all head and neck cancers require surgery?
No, many head and neck cancers can be treated with radiation therapy alone or combined with chemotherapy (chemoradiation). Treatment choice depends on tumor location, stage, HPV status, and patient preferences. Some early-stage cancers respond excellently to non-surgical approaches.
8. Can head and neck cancer spread to other parts of the body?
Yes, head and neck cancer can metastasize, most commonly to the lungs. Regional spread to neck lymph nodes occurs frequently and is often the initial presentation. Distant metastasis significantly reduces five-year survival to 39-42%.
9. Is head and neck cancer genetic?
While head and neck cancer is not typically inherited, genetic ancestry influences tumor biology and survival. A 2026 study revealed African American patients survive 2.5 years on average compared to 4.8 years for European American patients due to genetic differences in tumor characteristics.
10. What’s the survival rate for stage 4 head and neck cancer?
Stage IV head and neck cancer five-year survival ranges from 30-42% overall, but HPV-positive patients have significantly better outcomes (60-75%) compared to HPV-negative patients (30-40%). Modern immunotherapy and clinical trials continue improving these rates.
11. How often should I get screened for oral cancer?
No routine screening exists for head and neck cancer in average-risk individuals. However, dental examinations every 6 months with complete oral cavity inspection help detect early changes. High-risk individuals (tobacco users, heavy drinkers, prior HPV diagnosis) should request thorough examinations every 3-4 months.
For more health information and medical guidance, visit our Health Tips section or explore our comprehensive library at MyMedicineAdvisor.com.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.











