On This Page – Quick Medical Summary
Understanding Bile Duct Cancer In 2026
When David, a 58-year-old architect from Portland, noticed his eyes turning yellow, he dismissed it as exhaustion. Three weeks later, his diagnosis changed everything: bile duct cancer.
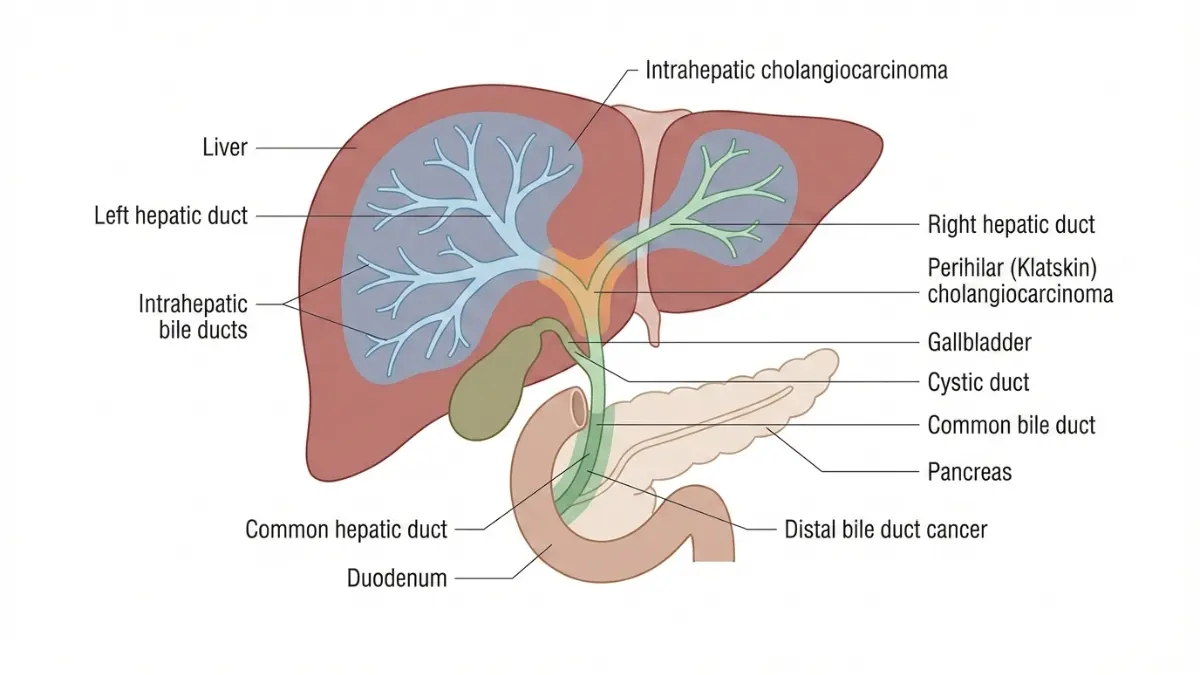
Bile duct cancer, medically known as cholangiocarcinoma, is a rare but aggressive malignancy that forms in the bile ducts—the small tubes connecting your liver to your small intestine. These ducts transport bile, a digestive fluid that breaks down fats. When cancer develops here, it often blocks bile flow, causing the telltale yellowing that prompts most diagnoses.
Approximately 8,000 Americans receive a bile duct cancer diagnosis annually, with incidence rates rising globally. The disease predominantly affects adults over 50, though younger individuals with specific risk factors face elevated threats. Unlike more common cancers, cholangiocarcinoma remains challenging to detect early because symptoms rarely appear until advanced stages.
This comprehensive guide delivers critical 2026 survival data, identifies the 7 warning signs that demand immediate medical attention, and explores breakthrough treatments transforming patient outcomes. Our analysis draws from the latest clinical trials, international consensus research, and specialized hepatobiliary centers worldwide.
Medical Disclaimer: This article provides educational information for general knowledge only and should not replace professional medical advice, diagnosis, or treatment. Always consult qualified healthcare providers for personalized medical guidance.
2026 Survival Rates—the Data That Matters
What Are Current Bile Duct Cancer Survival Rates?
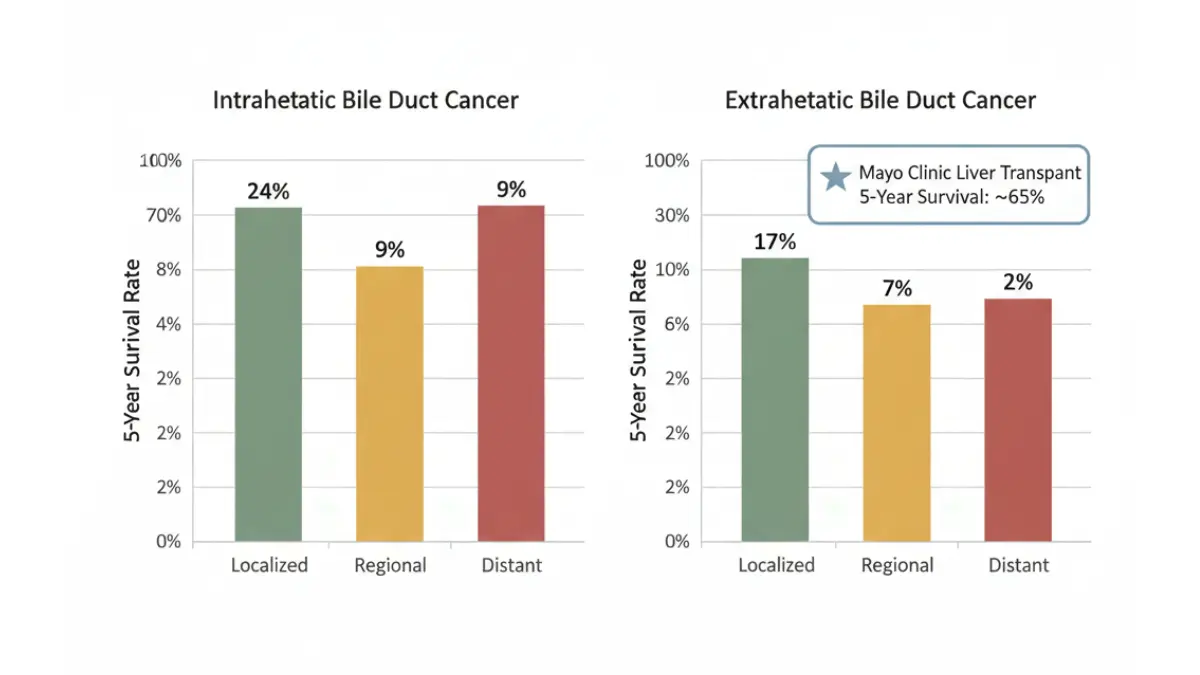
Survival rates for bile duct cancer vary dramatically based on tumor location and disease stage at diagnosis. According to the National Cancer Institute’s SEER database, 2026 data reveals stark differences:
Intrahepatic Bile Duct Cancer (Inside the Liver):
- Localized Stage: 24% 5-year survival
- Regional Spread: 9% 5-year survival
- Distant Metastases: 2% 5-year survival
Extrahepatic Bile Duct Cancer (Outside the Liver):
- Localized Stage: 17% 5-year survival
- Regional Spread: 7% 5-year survival
- Distant Metastases: 2% 5-year survival
These statistics represent significant improvements from a decade ago, largely driven by advanced surgical techniques and targeted therapies.
Breakthrough: Mayo Clinic Transplant Protocol
Perhaps the most revolutionary development comes from liver transplantation programs. Mayo Clinic reports that select patients with unresectable perihilar cholangiocarcinoma achieve 65% 5-year survival rates following neoadjuvant chemoradiation and liver transplantation—nearly triple the traditional surgical outcomes.
This protocol requires strict eligibility criteria: tumor size under 3 cm, no metastatic disease, and completion of intensive chemotherapy-radiation regimens. Only specialized transplant centers offer this curative approach.
2026 Treatment Advances Extending Survival
Recent clinical trials demonstrate unprecedented survival improvements:
TARE (Transarterial Radioembolization): A December 2025 study published in the European Network for Cholangiocarcinoma consensus report shows multimodal TARE combined with systemic chemotherapy achieves 32.5-month median overall survival, compared to 9.5 months with chemotherapy alone.
Targeted Therapy Breakthroughs: For HER2-positive bile duct tumors, tucatinib plus trastuzumab combination therapy demonstrates 53.6% 12-month overall survival rates with minimal treatment-related discontinuation.
What This Means For You: Early detection dramatically improves outcomes. Patients diagnosed at localized stages have 12-fold better survival than those with distant spread. Recognizing warning signs early creates life-saving opportunities.
| Stage at Diagnosis | Intrahepatic 5-Year Survival | Extrahepatic 5-Year Survival | Median Survival |
|---|---|---|---|
| Localized (No Spread) | 24% | 17% | 24-36 months |
| Regional (Nearby Spread) | 9% | 7% | 12-16 months |
| Distant (Metastatic) | 2% | 2% | 4-9 months |
7 Critical Early Warning Signs
Recognizing Bile Duct Cancer Before It’s Too Late
Most bile duct cancers remain asymptomatic until tumors grow large enough to obstruct bile flow. However, seven specific warning signs warrant immediate medical evaluation.
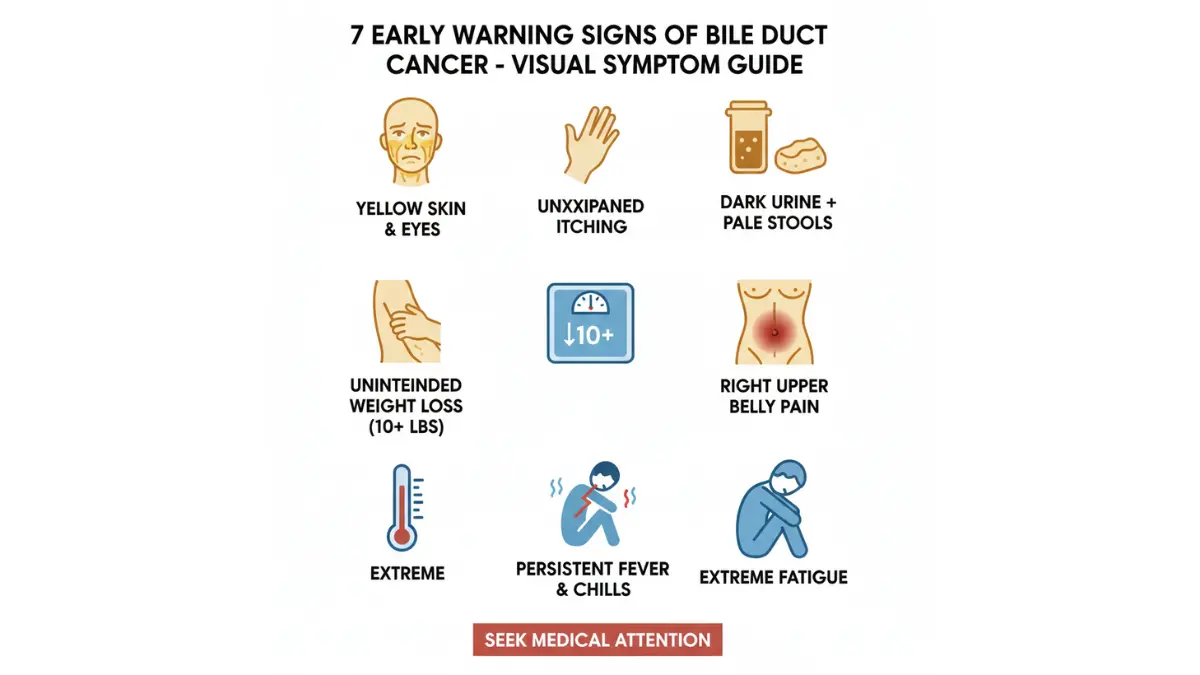
1. Jaundice (Yellowing of Skin and Eyes)
The most common presenting symptom appears in 60-90% of extrahepatic bile duct cancer cases. When tumors block bile ducts, bilirubin—a yellow pigment normally excreted in bile—accumulates in your bloodstream and deposits in tissues.
Early jaundice appears as yellowing of the eye whites (sclera) before skin discoloration becomes visible. Unlike benign causes such as Gilbert’s syndrome, cancer-related jaundice progressively worsens without intervention.
Medical Action Required: Any new-onset jaundice demands evaluation within 48 hours. Use our Symptom Checker to assess urgency, then contact your healthcare provider immediately.
2. Intense, Unexplained Itching (Pruritus)
Bile salts depositing in skin tissue trigger severe itching that often precedes visible jaundice by weeks. Unlike typical dry skin or allergic reactions, cholangiocarcinoma-related pruritus:
- Occurs without visible rash
- Intensifies at night
- Doesn’t respond to standard moisturizers
- May be generalized or localized to torso and limbs
Research from MD Anderson Cancer Center indicates 66% of patients experience significant pruritus before diagnosis.
3. Dark Urine with Clay-Colored Stools
This combination directly signals bile flow obstruction. Normally, bile gives stool its characteristic brown color while being filtered from blood by kidneys. When bile ducts are blocked:
- Urine appears tea or cola-colored (excess bilirubin excreted through kidneys)
- Stools become pale, gray, or clay-colored (absent bile pigments)
- Changes persist for more than 3-5 days
4. Unintentional Weight Loss
Losing 5-10% of body weight without dietary changes or increased activity indicates serious metabolic disruption. For a 170-pound person, this means losing 8-17 pounds within 1-3 months.
Weight loss in bile duct cancer results from:
- Decreased appetite due to tumor metabolic effects
- Malabsorption from impaired bile secretion
- Cancer cachexia (metabolic wasting syndrome)
Calculate your healthy weight range to determine if losses warrant concern.
5. Right Upper Abdominal Pain
Approximately 30-50% of patients develop abdominal discomfort localized beneath the right ribcage. Pain characteristics include:
- Dull, constant ache or intermittent cramping
- May radiate to right shoulder or back
- Worsens after fatty meals (when bile production increases)
- Not relieved by antacids or position changes
Unlike gallstone pain, which comes in severe “attacks,” bile duct cancer pain tends toward persistent lower-grade discomfort that gradually intensifies.
6. Unexplained Fever and Chills
Fever in bile duct cancer often indicates cholangitis—bacterial infection of obstructed bile ducts. This medical emergency requires immediate intervention and presents with:
- Temperature exceeding 100.4°F (38°C)
- Shaking chills
- Rapid onset (within hours)
- May accompany jaundice and abdominal pain (Charcot’s triad)
The National Institute of Diabetes and Digestive and Kidney Diseases emphasizes that infected bile duct obstructions can rapidly progress to life-threatening sepsis without treatment.
7. Persistent Fatigue Disproportionate to Activity
Cancer-related fatigue differs from normal tiredness. Characteristics include:
- Unrelieved by rest or sleep
- Interferes with daily activities
- Accompanied by general malaise
- Present for weeks without improvement
This systemic symptom reflects the body’s metabolic response to malignancy and impaired liver function.
When Multiple Warning Signs Appear Together
The presence of two or more symptoms simultaneously—especially jaundice combined with dark urine, pale stools, or abdominal pain—requires urgent evaluation. These combinations indicate high-probability bile duct obstruction requiring immediate imaging and diagnosis.
Critical Action Steps:
- Document all symptoms with dates and progression
- Photograph jaundiced eyes or skin changes
- Schedule appointment within 48-72 hours
- Request liver function tests and imaging
- Consider using our Genetic Risk Assessment Tool if you have family history of liver disease
Types, Causes, And Risk Factors
Three Distinct Bile Duct Cancer Types
Bile duct cancer classification depends on anatomical origin, with each type presenting unique characteristics and treatment approaches.
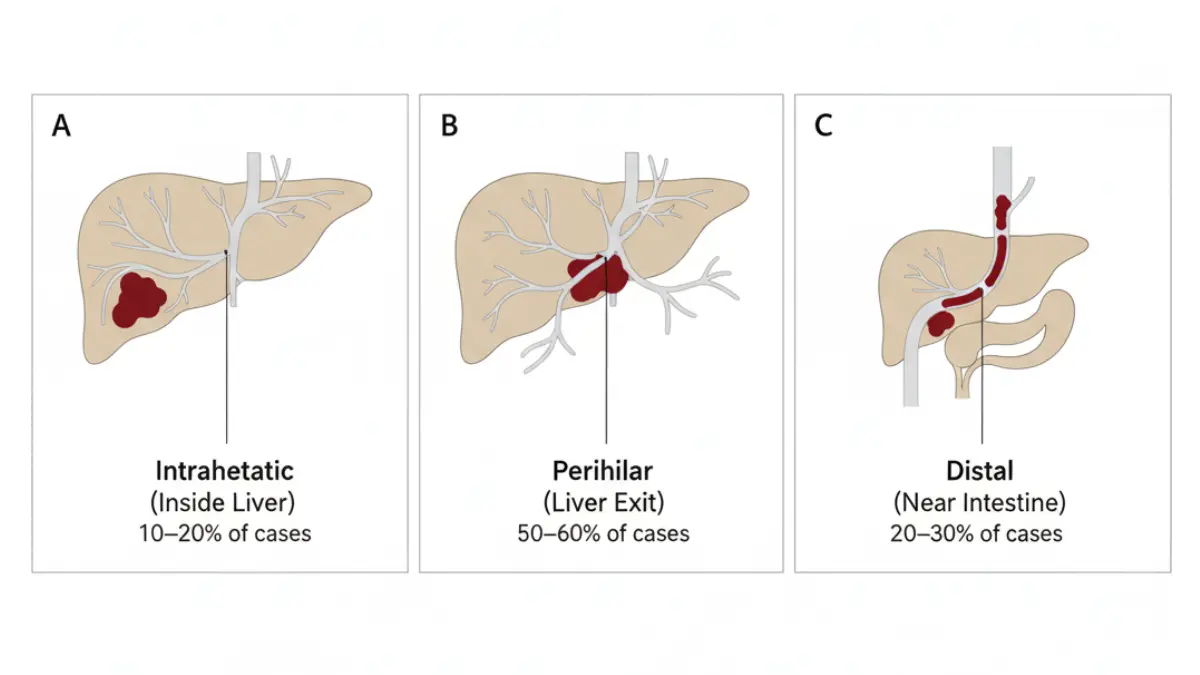
Intrahepatic Cholangiocarcinoma (10-20% of Cases)
Tumors form within bile ducts inside the liver parenchyma. These often grow silently to considerable size before causing symptoms, as they don’t immediately obstruct major bile flow. Intrahepatic tumors more closely resemble liver cancer in behavior and may be discovered incidentally during imaging for other conditions.
Perihilar Cholangiocarcinoma (50-60% of Cases)
Also called Klatskin tumors, these develop where right and left hepatic ducts exit the liver and join. This strategic location near the liver hilum makes complete surgical removal challenging. Perihilar tumors cause jaundice earlier than intrahepatic types due to their location at critical bile duct junctions.
Distal Cholangiocarcinoma (20-30% of Cases)
These arise in the portion of the bile duct nearest the small intestine, often involving the pancreas. Distal tumors may be treated with pancreatoduodenectomy (Whipple procedure), offering 27-37% 5-year survival rates when complete resection achieves negative margins.
What Causes Bile Duct Cancer?
While most cases occur sporadically without identifiable cause, several established risk factors significantly increase cholangiocarcinoma likelihood.
Primary Sclerosing Cholangitis (PSC): This chronic inflammatory bile duct disease carries 10-15% lifetime cholangiocarcinoma risk. PSC causes progressive scarring and narrowing of bile ducts, creating persistent inflammation that may trigger malignant transformation. Approximately 70% of PSC patients also have inflammatory bowel disease, particularly ulcerative colitis.
Liver Fluke Parasites: In Southeast Asian regions including Thailand, Laos, and Vietnam, liver flukes (Opisthorchis viverrini and Clonorchis sinensis) cause chronic bile duct inflammation. Endemic areas report incidence rates of 60 per 100,000 population—30-fold higher than Western countries. These parasites infect humans through consumption of raw or undercooked freshwater fish.
Choledochal Cysts: Congenital bile duct cysts increase cancer risk 10-15%, typically manifesting in younger adults (ages 20-50). These abnormal bile duct dilations cause bile stasis and chronic inflammation.
Chronic Liver Disease: Hepatitis B and C infections, alcoholic cirrhosis, and non-alcoholic fatty liver disease all elevate risk through sustained hepatic inflammation and architectural disruption affecting bile ducts.
Age and Demographics: Median diagnosis age is 70 years, with incidence rising sharply after age 50. Men develop bile duct cancer slightly more often than women (1.3:1 ratio).
Risk Assessment: Do You Need Screening?
While routine population screening isn’t recommended, high-risk individuals benefit from surveillance programs including:
- Annual ultrasound or MRI for PSC patients
- CA 19-9 tumor marker monitoring in high-risk groups
- Enhanced imaging every 6-12 months for choledochal cyst patients
Discuss screening protocols with gastroenterology specialists if you have multiple risk factors. Understanding your risk profile through comprehensive health assessment tools empowers proactive monitoring.
Diagnosis And 2026 Treatment Breakthroughs
How Bile Duct Cancer Is Diagnosed
Diagnostic pathways typically follow this sequence after symptom presentation:
Initial Blood Tests: Liver function panels reveal elevated bilirubin, alkaline phosphatase, and gamma-glutamyl transferase—the “obstructive pattern” suggesting bile duct blockage. CA 19-9 tumor marker, while not diagnostic alone, provides baseline values for monitoring. Levels above 100 U/mL raise suspicion for malignancy.
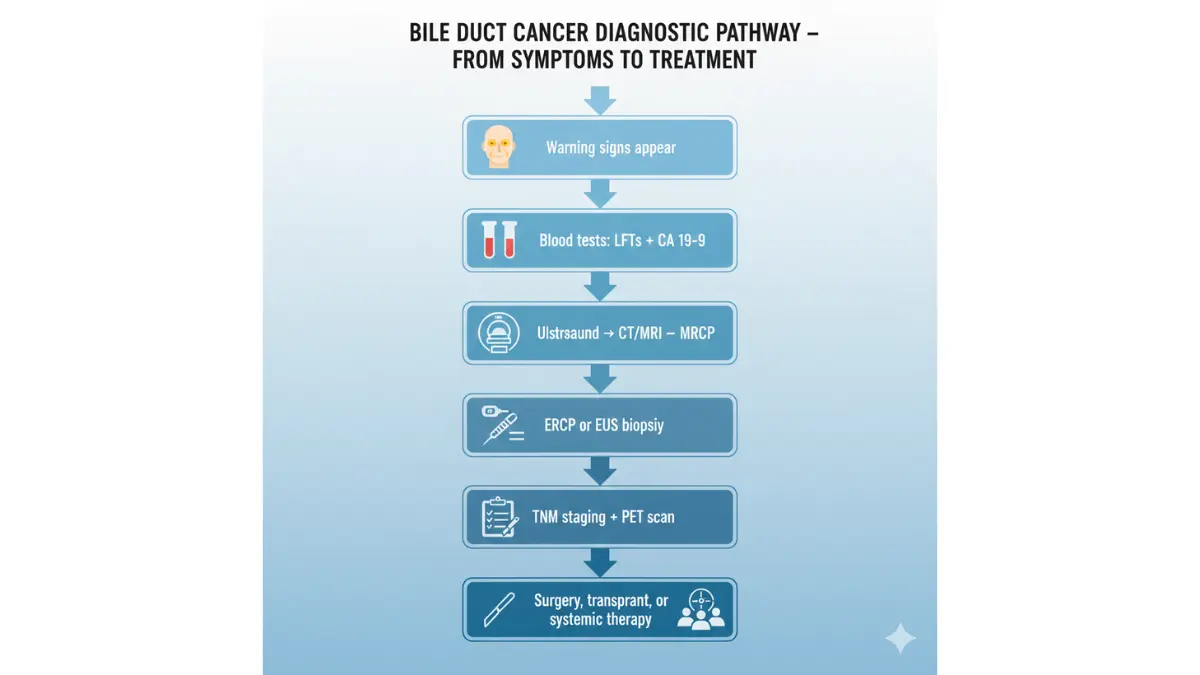
Imaging Studies:
- Abdominal Ultrasound: First-line imaging detects bile duct dilation and mass lesions
- CT/MRI Scans: Define tumor extent, vascular involvement, and metastatic disease
- MRCP (Magnetic Resonance Cholangiopancreatography): Specialized imaging visualizes biliary tree without invasive procedures
- PET Scans: Identify distant metastases and assess metabolic tumor activity
Tissue Diagnosis:
- ERCP (Endoscopic Retrograde Cholangiopancreatography): Obtains bile duct biopsies while allowing stent placement for symptom relief
- EUS (Endoscopic Ultrasound): Provides high-resolution imaging with fine needle aspiration capability
- Percutaneous Biopsy: Reserved for intrahepatic tumors not accessible endoscopically
Confirming cholangiocarcinoma diagnosis often proves challenging, with biopsy sensitivity ranging 40-70%. Surgical exploration may proceed based on clinical presentation and imaging when biopsy attempts fail.
2026 Treatment Revolution: What’s Changed
Surgical Advances
Complete Resection with Negative Margins: For localized disease, aggressive surgical resection offers the only curative option. Techniques include:
- Extended Hepatectomy: Removes affected liver segments plus bile ducts, achieving R0 (microscopically negative) resection
- Pancreatoduodenectomy (Whipple Procedure): Standard for distal tumors, with 30-40% achieving long-term survival
- Bile Duct Excision with Reconstruction: Connects remaining healthy bile ducts directly to intestine
Liver Transplantation Protocols: The groundbreaking Mayo Clinic approach combines intensive neoadjuvant therapy (chemotherapy plus external beam radiation) with orthotopic liver transplantation for select perihilar cases. Houston Methodist surgical oncology studies confirm 100% one-year and two-year survival in carefully selected patients, with 75% five-year survival—transforming previously “incurable” cancers into potentially curable disease.
Eligibility requirements:
- Tumor diameter under 3 cm
- No extrahepatic metastases
- Completion of neoadjuvant chemoradiation
- Adequate performance status
Revolutionary Non-Surgical Therapies
TARE (Yttrium-90 Radioembolization): This targeted radiation therapy delivers radioactive microspheres directly to liver tumors through hepatic arteries. When combined with systemic chemotherapy, patients achieve median overall survival of 32.5 months versus 9.5 months with chemotherapy alone. Partition-model dosimetry—personalized radiation dose calculations—demonstrates superior outcomes compared to standard dosing approaches.
Targeted Molecular Therapies: Genetic profiling identifies actionable mutations in approximately 40% of cholangiocarcinomas:
- FGFR2 Fusions (10-15% of patients): Pemigatinib achieves 35% response rates with median 21-month survival
- IDH1 Mutations (15-20% of patients): Ivosidenib demonstrates disease control in 56% of patients
- HER2 Amplifications (5-10% of patients): Tucatinib plus trastuzumab yields 53.6% 12-month survival with excellent tolerability
Immunotherapy Combinations: While single-agent immunotherapy shows limited cholangiocarcinoma activity, combination regimens under investigation include:
- PD-1/PD-L1 inhibitors plus chemotherapy
- Dual checkpoint blockade (anti-PD-1 plus anti-CTLA-4)
- Immunotherapy combined with TARE radiation therapy
Standard Chemotherapy Advances: The ABC-02 trial established gemcitabine plus cisplatin as first-line therapy, achieving 11.7-month median survival. The ABC-06 trial confirmed FOLFOX (5-fluorouracil, leucovorin, oxaliplatin) as effective second-line treatment, adding 4.5 months survival versus supportive care alone.
Palliative Interventions: For unresectable disease, symptom management remains critical:
- Biliary Stenting: Relieves jaundice and pruritus through endoscopic or percutaneous stent placement
- Photodynamic Therapy (PDT): Light-activated treatment extending survival when combined with chemotherapy
- Radiation Therapy: External beam or brachytherapy for local disease control
Clinical Trial Opportunities
The BOLSTER trial evaluates certepetide—an investigational drug enhancing chemotherapy delivery to tumors—combined with standard gemcitabine/cisplatin/durvalumab therapy. Early results show promising tolerability and efficacy signals.
Access current trials through ClinicalTrials.gov searching “cholangiocarcinoma 2026” to identify cutting-edge treatment options potentially offering superior outcomes.
Taking Action—when To Seek Help
Urgent Medical Situations Requiring Immediate Evaluation
Certain symptom combinations constitute medical emergencies:
Charcot’s Triad (Cholangitis): The combination of fever, jaundice, and right upper abdominal pain indicates infected bile duct obstruction requiring emergency intervention. Without treatment, cholangitis progresses to septic shock within hours.
Reynolds’ Pentad: Adding confusion and low blood pressure to Charcot’s triad signals advanced sepsis. Call 911 immediately—this condition carries 50% mortality without urgent care.
Progressive Jaundice: Deepening yellow discoloration over 5-7 days, especially with darkening urine and pale stools, requires same-week physician evaluation.
Unexplained Weight Loss Exceeding 10 Pounds: When occurring over 4-6 weeks without dietary changes, schedule comprehensive evaluation including imaging studies.
Questions to Ask Your Oncologist
If diagnosed with bile duct cancer, these critical questions guide treatment decisions:
- What is the exact tumor location and TNM staging?
- Am I a surgical resection candidate?
- Should I be evaluated for liver transplantation protocols?
- What genetic mutations does my tumor harbor?
- Which clinical trials am I eligible for?
- What are treatment success rates at your center versus national averages?
- Should I seek consultation at specialized hepatobiliary cancer centers?
Second Opinion Guidance
Given cholangiocarcinoma’s rarity and complexity, second opinions from high-volume hepatobiliary centers often reveal additional treatment options. Consider consultations at:
- Mayo Clinic (Rochester, Minnesota)
- MD Anderson Cancer Center (Houston, Texas)
- Memorial Sloan Kettering (New York, New York)
- Cleveland Clinic (Cleveland, Ohio)
- Johns Hopkins Hospital (Baltimore, Maryland)
Specialized centers offer access to clinical trials, experimental therapies, and surgical expertise unavailable at community hospitals. The Cholangiocarcinoma Foundation maintains a comprehensive specialist directory.
Support Resources and Quality of Life
Nutritional Considerations: Bile duct obstruction impairs fat digestion. Work with oncology dietitians to optimize nutritional intake through:
- Pancreatic enzyme supplementation
- Medium-chain triglyceride supplements
- Fat-soluble vitamin replacement (A, D, E, K)
- Small, frequent meals reducing digestive burden
Managing Treatment Side Effects: Chemotherapy and radiation cause significant fatigue. Our Sleep Calculator helps optimize recovery through improved sleep hygiene during treatment.
Caregiver Support: Family members and caregivers need resources too. The Cholangiocarcinoma Foundation offers:
- Newly Connected program pairing diagnosed patients with mentors
- Support groups connecting patients and families
- Educational webinars on treatment advances
- Financial assistance programs
The Power of Early Detection
While bile duct cancer remains one of medicine’s most challenging malignancies, 2026 brings unprecedented treatment advances. Patients diagnosed at localized stages now access therapies that were experimental just five years ago.
The critical difference between 2% and 24% five-year survival often comes down to recognizing the 7 warning signs weeks or months earlier. Jaundice, unexplained itching, dark urine with pale stools, unintentional weight loss, right-sided abdominal pain, persistent fever, and unusual fatigue—individually concerning, but together potentially life-saving when they prompt timely evaluation.
Share this information with anyone at risk—those with PSC, chronic liver disease, or concerning symptoms. Early medical intervention creates treatment opportunities that simply don’t exist once cancer spreads beyond bile ducts.
Your vigilance today could mean the difference between palliative care and potential cure tomorrow.
Frequently Asked Questions
1. What is bile duct cancer and how common is it?
Bile duct cancer (cholangiocarcinoma) is a rare malignancy arising from bile duct cells lining the tubes that carry bile from liver to intestine. Approximately 8,000 Americans are diagnosed annually, representing less than 1% of all cancers. Incidence increases with age, peaking after 70 years, though younger individuals with risk factors like primary sclerosing cholangitis face elevated risk.
2. Can bile duct cancer be detected early through screening?
No routine screening exists for average-risk populations. However, high-risk individuals—particularly those with primary sclerosing cholangitis, choledochal cysts, or chronic liver fluke infections—benefit from surveillance including annual MRI/MRCP and CA 19-9 tumor marker monitoring. Most diagnoses occur after symptoms develop because early-stage disease rarely causes detectable changes.
3. What are the 2026 survival rates for bile duct cancer?
Five-year survival rates vary dramatically by stage: localized intrahepatic (24%), localized extrahepatic (17%), regional spread (7-9%), and distant metastases (2%). Revolutionary liver transplantation protocols at specialized centers achieve 65% five-year survival for select perihilar cases. New targeted therapies and TARE radioembolization extend median survival from historical 9 months to over 32 months in some treatment combinations.
4. Is bile duct cancer hereditary or genetic?
Cholangiocarcinoma is not typically hereditary, with most cases occurring sporadically. However, genetic mutations within tumors (FGFR2, IDH1, HER2) guide targeted treatment selection. Family history plays minimal role except in rare cancer syndromes. Primary risk factors involve chronic inflammation (PSC, liver flukes, bile duct cysts) rather than inherited genetics.
5. What causes bile duct cancer to develop?
Chronic bile duct inflammation represents the primary causative pathway. Specific triggers include primary sclerosing cholangitis (10-15% lifetime cancer risk), liver fluke parasites in endemic Asian regions, choledochal cysts, hepatitis B/C infections causing cirrhosis, and bile duct stones causing repeated inflammation. Most Western cases occur without identifiable cause, representing spontaneous malignant transformation in aging bile duct cells.
6. How is bile duct cancer different from liver cancer?
While both affect liver region anatomy, they originate from different cell types requiring distinct treatments. Hepatocellular carcinoma (liver cancer) arises from hepatocytes performing liver metabolic functions. Cholangiocarcinoma originates from cholangiocytes lining bile ducts. Even intrahepatic cholangiocarcinoma occurring within liver tissue differs biologically from HCC, responding to different chemotherapy regimens and having separate staging systems.
7. What are the newest treatment options for bile duct cancer in 2026?
Breakthrough therapies include: (1) Liver transplantation following neoadjuvant chemoradiation achieving 65% five-year survival at Mayo Clinic, (2) TARE radioembolization with systemic therapy extending survival to 32.5 months, (3) Targeted therapies for FGFR2 (pemigatinib), IDH1 (ivosidenib), and HER2 (tucatinib/trastuzumab) mutations, (4) Certepetide investigational drug enhancing chemotherapy delivery in BOLSTER trials, and (5) Immunotherapy combinations under clinical investigation.
8. Can bile duct cancer be cured completely?
Cure remains possible when disease is localized and completely resected surgically with negative margins. Approximately 17-24% of localized-stage patients survive five years, with some achieving long-term remission. Liver transplantation protocols extend cure possibilities to select previously unresectable perihilar cases. However, most diagnoses occur at advanced stages when cure becomes unlikely, shifting treatment goals toward life extension and symptom management.
9. What is the typical life expectancy after bile duct cancer diagnosis?
Prognosis varies dramatically by stage and treatment approach. Localized disease with complete surgical resection: 24-36 months median survival. Regional lymph node involvement: 12-16 months. Distant metastases: 4-9 months with chemotherapy, 2-4 months with supportive care alone. Specialized liver transplant candidates may achieve decades of survival. Individual factors including age, liver function, performance status, and tumor biology influence outcomes significantly.
10. Should I get genetic testing if diagnosed with bile duct cancer?
Yes, comprehensive genomic profiling identifies targetable mutations in approximately 40% of cholangiocarcinomas. Actionable alterations include FGFR2 fusions (10-15% of cases, treated with pemigatinib), IDH1 mutations (15-20%, treated with ivosidenib), and HER2 amplifications (5-10%, treated with tucatinib/trastuzumab). Testing guides personalized therapy selection potentially doubling response rates versus standard chemotherapy alone. Insurance typically covers testing for advanced-stage disease.
11. Where can I find bile duct cancer specialists and treatment centers?
Seek hepatobiliary surgical oncologists at high-volume cancer centers including Mayo Clinic, MD Anderson, Memorial Sloan Kettering, Cleveland Clinic, Johns Hopkins, and UCSF. These institutions offer multidisciplinary teams, access to clinical trials, advanced surgical techniques including liver transplantation protocols, and outcomes data exceeding community hospitals. The Cholangiocarcinoma Foundation (cholangiocarcinoma.org) maintains a comprehensive specialist directory and patient navigation services connecting individuals with appropriate expertise.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.











