On This Page – Quick Medical Summary
William, 41, had been dealing with a throbbing face, blocked nose, and pressure behind his eyes for nine days. His urgent care doctor handed him a Z-Pack prescription and sent him home. By Day 5, he was no more improved. What William— and millions of Americans — didn’t know: the Z-Pack hasn’t been a recommended sinus infection antibiotic for years. And his doctor may have given him the wrong drug entirely.
If you have a sinus infection and you’re wondering whether antibiotics are right for you, which one works, and why your last prescription may have failed — this is the only 2026-updated guide you need.
Quick Answer: What Are the Best Sinus Infection Antibiotics in 2026?
The 2025 AAO-HNS updated clinical guidelines confirm that amoxicillin-clavulanate (Augmentin) is now the gold standard first-line antibiotic for bacterial sinusitis in most adults — replacing plain amoxicillin. Treatment duration is 5–7 days, not the outdated 10–14 days you may have been prescribed.
But here’s the critical fact most articles skip: 90–98% of sinus infections are viral. Antibiotics do nothing for viral infections. Knowing whether you actually need sinus infection antibiotics at all is the most important question — and most competitor articles never answer it properly.
Use our Symptom Checker to help identify whether your symptoms point toward a bacterial or viral cause before your doctor visit.
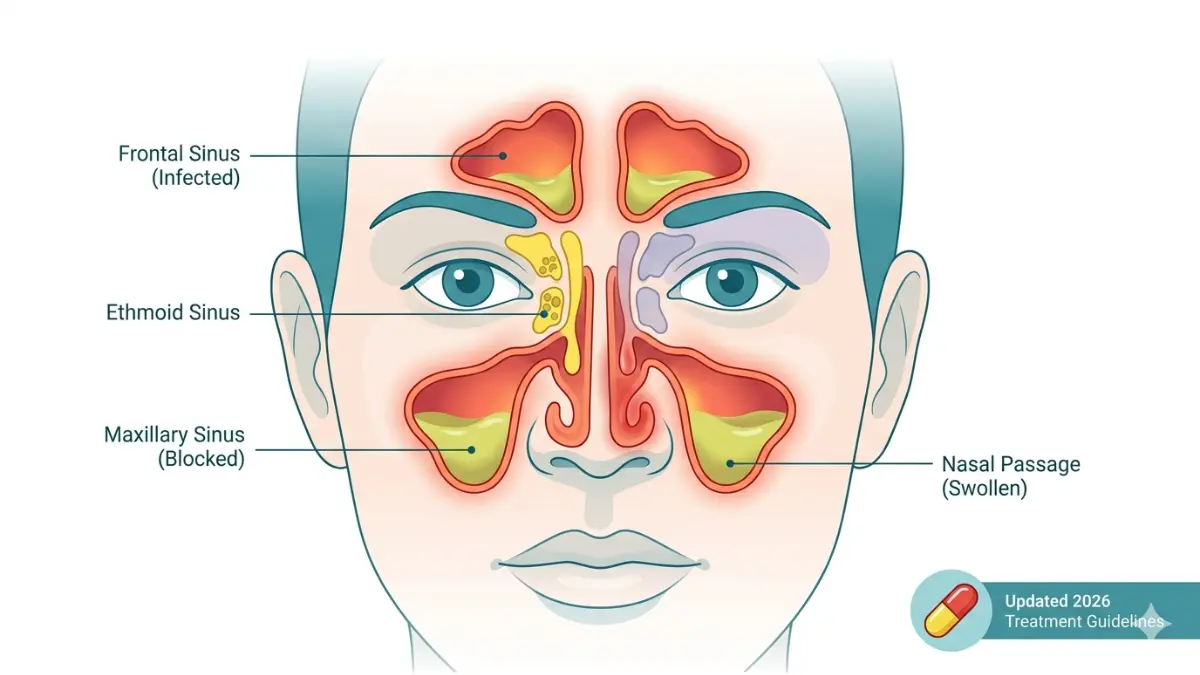
Is Your Sinus Infection Actually Bacterial?
The Most Misunderstood Fact in Sinus Treatment
Most people assume a sinus infection means they need an antibiotic. That assumption is wrong — and it’s costing Americans billions of dollars annually while fueling antibiotic resistance.
According to the CDC’s 2025 Antibiotic Stewardship Report, about 75% of sinus infection visits in the US result in an antibiotic prescription — despite the fact that the vast majority of those infections are viral and will resolve on their own.
The 3 Clinical Signs That Confirm Bacterial Infection
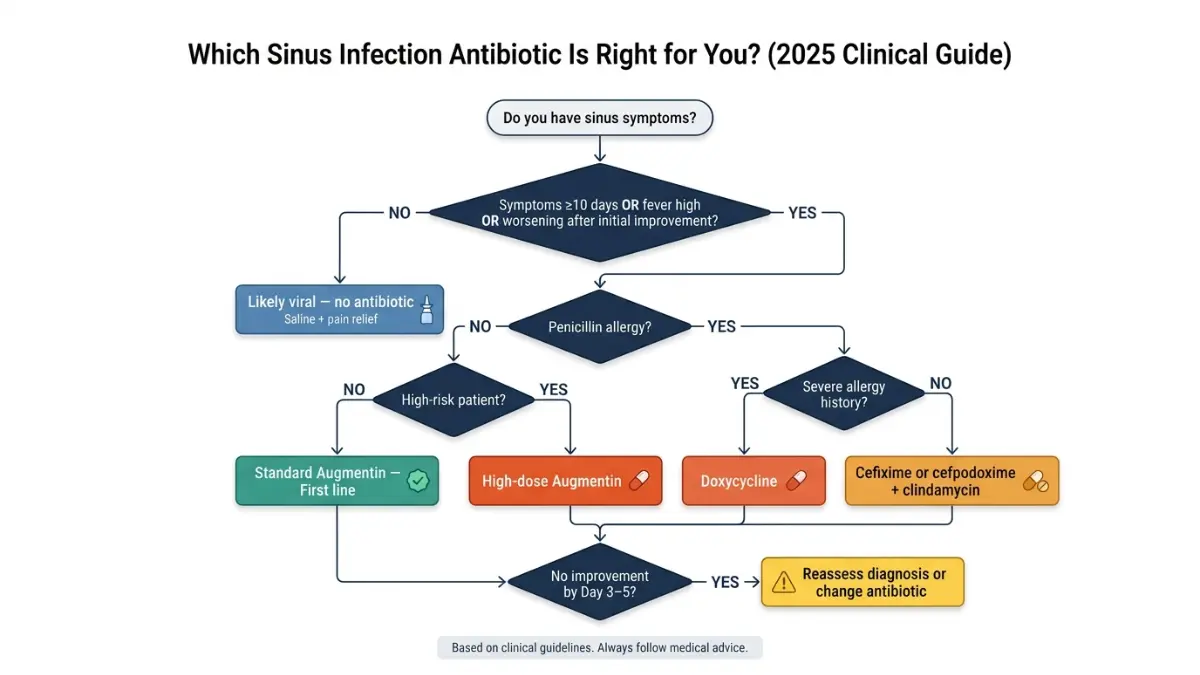
Doctors use specific clinical criteria — not just how bad you feel — to determine whether bacterial antibiotics are justified. Per IDSA and AAO-HNS guidelines, a bacterial sinus infection is confirmed when at least one of these three patterns is present:
- Persistent symptoms for 10+ days without improvement — the most common indicator
- Severe onset: fever of 102°F (39°C) or higher with facial pain and thick nasal discharge for 3–4 consecutive days
- “Double sickening”: symptoms initially improved after 5–6 days, then suddenly worsened again
If none of these apply to you, there is a strong chance you have a viral sinus infection — and sinus infection antibiotics will not help.
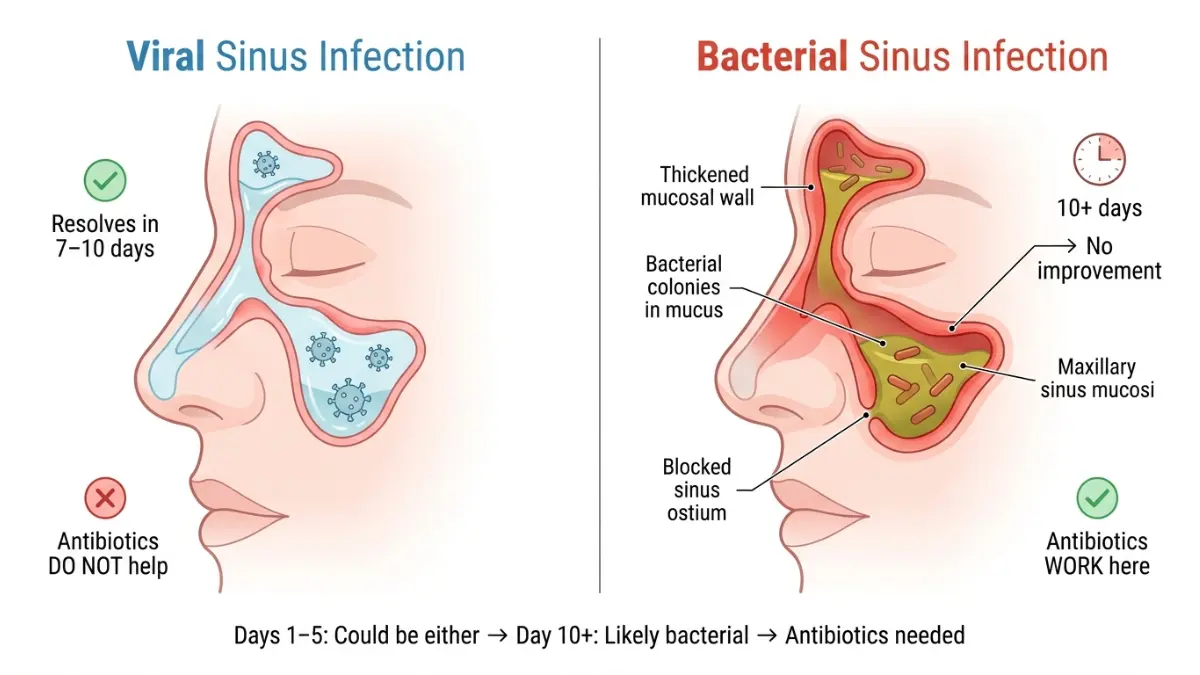
Viral vs. Bacterial Sinusitis: Side-by-Side
| Feature | Viral Sinusitis | Bacterial Sinusitis |
|---|---|---|
| Onset | Gradual, following a cold | After 10+ days, or sudden severity |
| Nasal discharge | Clear, watery or thin | Thick, yellow/green, persistent |
| Fever | Low-grade or none | High (102°F+) |
| Duration | Peaks at days 3–5, improves | Doesn’t improve after 10 days |
| Facial pain | Mild pressure | Intense, localized pain |
| Needs antibiotics? | ❌ No | ✅ Yes |
What This Means For You: If your symptoms started with a cold, peaked around day 3–5, and you’re on day 7 feeling slightly better — you almost certainly don’t need sinus infection antibiotics. Give your body the time it needs.
The 2025 Guideline Update That Changes Everything
What Your Doctor May Not Have Told You Yet
In late 2025, the American Academy of Otolaryngology–Head and Neck Surgery (AAO-HNS) released its updated Adult Sinusitis Clinical Practice Guideline — the most significant revision to sinus infection treatment in years. The changes are substantial, and most online resources have not caught up.
Here is what changed, and why it matters to you right now.
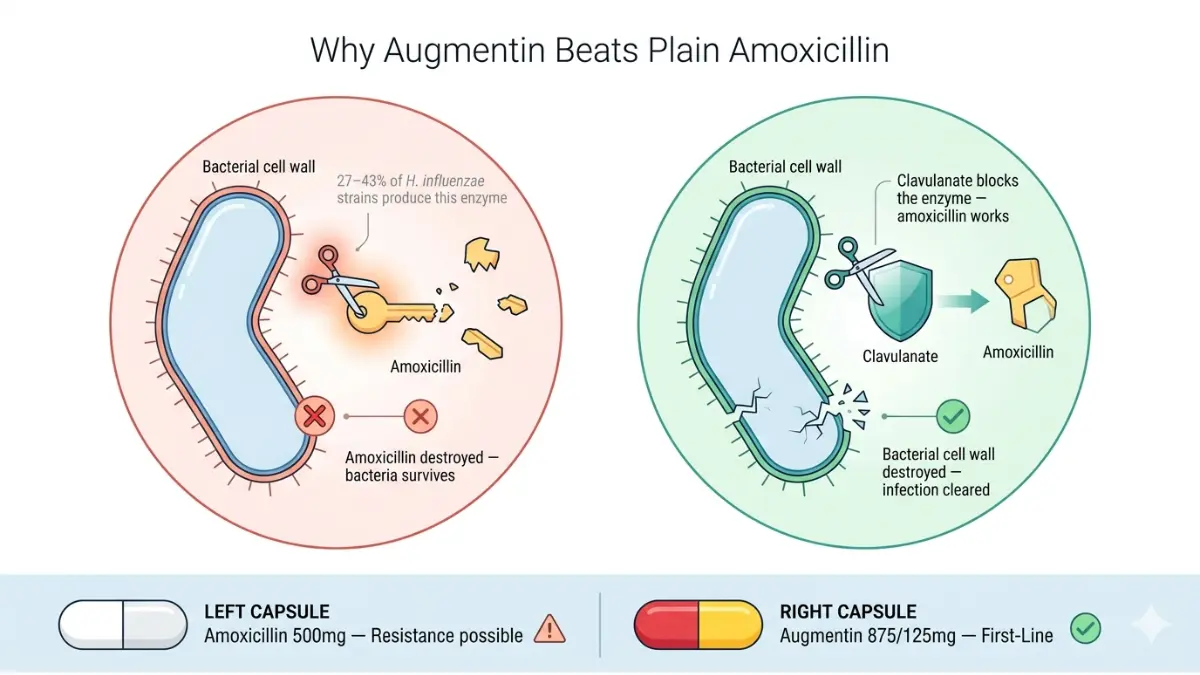
Change #1 — The First-Line Antibiotic Is No Longer Plain Amoxicillin
The previous standard was to prescribe amoxicillin alone. The 2025 guidelines now recommend amoxicillin with or without clavulanate as first-line therapy for adults with confirmed acute bacterial rhinosinusitis (ABRS).
Why the upgrade? Bacteria that cause sinus infections — particularly Haemophilus influenzae — increasingly produce beta-lactamase enzymes that break down plain amoxicillin. The clavulanate component in Augmentin blocks that enzyme, restoring the antibiotic’s effectiveness.
For full details on how Augmentin works, how it’s dosed, and what to expect, read our in-depth Augmentin guide.
Change #2 — Treatment Duration Is Now 5–7 Days
This is one of the most important updates that virtually no competitor article has published yet.
The new AAO-HNS guideline reduces the recommended antibiotic course for bacterial sinusitis from 5–10 days down to 5–7 days for most adults. If your doctor is still writing 10–14 day prescriptions for an uncomplicated sinus infection, that practice is now behind current evidence.
Shorter courses mean:
- Lower risk of antibiotic resistance
- Fewer side effects (especially GI issues from Augmentin)
- Lower cost for the patient
Change #3 — Z-Pack Is Officially Off the Table
This is the change that would have helped William immediately.
The 2025 guidelines explicitly exclude macrolide antibiotics (azithromycin/Z-Pack, clarithromycin) from recommended sinusitis treatments. Trimethoprim-sulfamethoxazole (Bactrim) is also out. Both drug classes have unacceptably high resistance rates against the bacteria that cause sinus infections in the US.
For a complete breakdown of azithromycin’s appropriate uses, see our Z-Pack guide.
Change #4 — The Watchful Waiting Strategy Is Now Standard
The 2025 guideline formally endorses a delayed prescribing approach: your doctor may hand you an antibiotic prescription but advise you to wait 2–5 days before filling it — unless symptoms are severe or worsening. This strategy:
- Allows bacterial sinusitis to resolve naturally in many patients
- Dramatically reduces unnecessary antibiotic use
- Is backed by evidence showing most ABRS resolves within 7–10 days even without treatment
Sinus Infection Antibiotics Compared — Which One Is Right for You?
The 2026 Decision Framework
Not every patient gets the same antibiotic. Your correct sinus infection antibiotic depends on your allergy history, risk factors for resistant bacteria, age, and symptom severity. Here is the complete clinical breakdown.
First-Line: Amoxicillin-Clavulanate (Augmentin)
Best for: Most adults with confirmed bacterial sinusitis
| Detail | Information |
|---|---|
| Brand name | Augmentin |
| Dose | 500/125 mg three times daily OR 875/125 mg twice daily |
| Duration | 5–7 days (2025 guideline) |
| High-risk dose | 2g/125 mg twice daily (for age >65, immunocompromised, recent hospitalization) |
| Common side effects | Diarrhea, nausea, yeast infection |
| Resistance profile | Low — clavulanate blocks beta-lactamase resistance |
Plain amoxicillin alone remains acceptable for low-risk, healthy adults in communities with low antibiotic resistance rates. It is cheaper and has fewer GI side effects than Augmentin. For a complete breakdown of amoxicillin, see our amoxicillin guide.
If You Have a Penicillin Allergy
Do not panic — safe alternatives exist:
- Doxycycline (100 mg twice daily for 5–7 days): First alternative for penicillin-allergic patients per 2025 guidelines. Highly effective sinus tissue penetration. For the full doxycycline profile, see our doxycycline guide.
- Levofloxacin (500 mg once daily for 5 days): Second-line only. The FDA has issued warnings about serious side effects with fluoroquinolones — use only when no alternatives exist.
- Cefixime or cefpodoxime + clindamycin: For patients with non-Type 1 (non-anaphylactic) penicillin allergy
Complete Antibiotic Comparison Table
| Antibiotic | Best For | Dose | Duration | 2025 Status |
|---|---|---|---|---|
| Amoxicillin-clavulanate | Most adults (first-line) | 875/125 mg 2x/day | 5–7 days | ✅ Recommended |
| Amoxicillin | Low-risk, healthy adults | 500 mg 3x/day | 5–7 days | ✅ Acceptable |
| Doxycycline | Penicillin allergy | 100 mg 2x/day | 5–7 days | ✅ Recommended |
| Levofloxacin | High-risk, allergy, no other options | 500 mg 1x/day | 5 days | ⚠️ Second-line only |
| Azithromycin (Z-Pack) | — | — | — | ❌ Not recommended |
| Clarithromycin | — | — | — | ❌ Not recommended |
| Trimethoprim-sulfamethoxazole | — | — | — | ❌ Not recommended |
For a detailed breakdown of ciprofloxacin’s risks in respiratory infections, read our ciprofloxacin warning guide.
Day-by-Day Recovery Timeline — When Will You Feel Better?
What No Competitor Article Tells You
One of the most searched questions about sinus infection antibiotics is: “How fast will this work?” Competitors list drug names and dosages but leave patients in the dark about what to actually expect each day. Here is the real timeline.
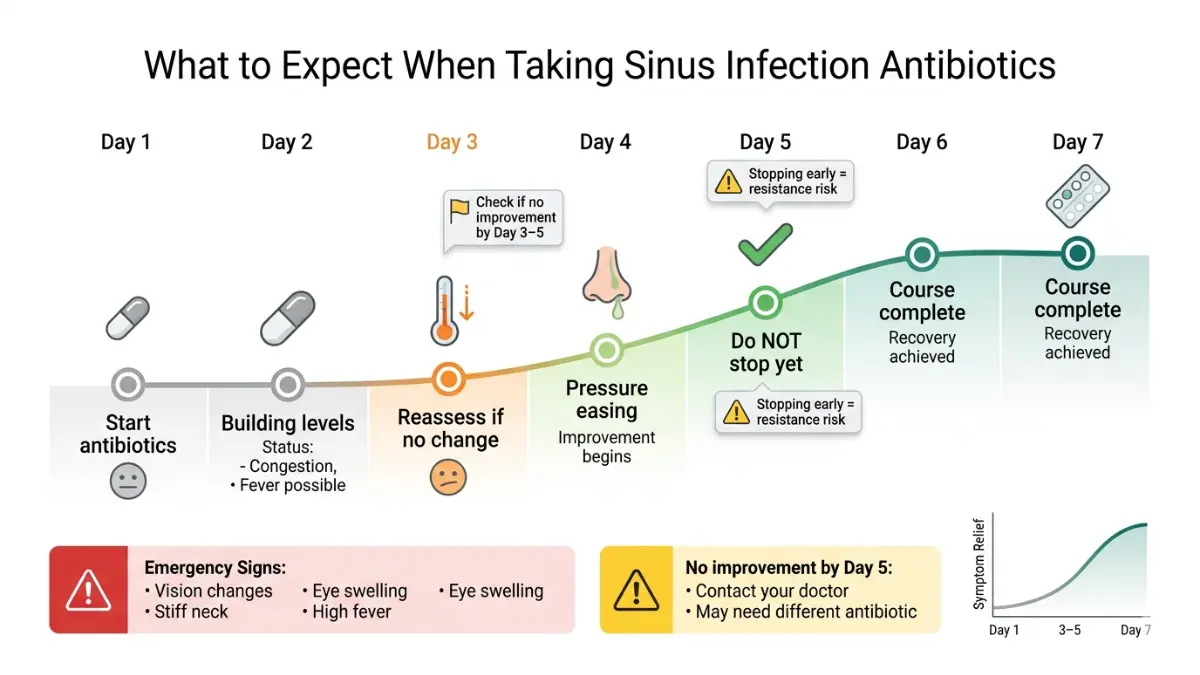
Day 1–2: Don’t Panic — Nothing May Feel Different
Antibiotics need 24–48 hours to reach therapeutic concentration in your sinus tissues. Expect:
- Continued congestion and facial pressure — normal
- Fever may persist on day 1
- No improvement in nasal discharge yet
Action steps for Day 1–2:
- Take antibiotics at consistent times — never skip a dose
- Use saline nasal rinse to help clear congestion (evidence-based, guideline-supported)
- Stay well-hydrated — your immune system needs it. Track your daily fluid needs with our Water Intake Calculator
- Use analgesics (acetaminophen or ibuprofen) for pain and fever management
Day 3–4: The Green Light Phase
This is when most patients begin to see improvement:
- Fever breaks or drops significantly
- Nasal discharge begins to thin and may change from yellow/green back toward clear
- Facial pressure reduces — not gone, but noticeably less intense
- Energy begins to return
⚠️ Critical warning: If by Day 3–5 you are no worse but not improving at all, this is the 2025 guideline’s reassessment trigger. Contact your doctor. You may need a different antibiotic, or it may not be a bacterial infection at all.
Day 5–7: Completing the Course
This is where many patients make a critical mistake — they feel better on day 5 and stop their antibiotic.
Do not stop early. Incomplete antibiotic courses:
- Allow partially killed bacteria to develop resistance
- Increase risk of relapse within 2–4 weeks
- Contribute to community-level antibiotic resistance
Complete your full prescribed course even if you feel 100% better.
Red Flags — Go to the ER Immediately
These symptoms during a sinus infection indicate a serious complication and require emergency care:
- Severe headache that is different from your usual sinus headache
- Vision changes, double vision, or eye swelling
- Stiff neck or light sensitivity
- High fever (>103°F) that does not respond to medication
- Swelling around the eyes or forehead
- Confusion or altered mental status
These may indicate orbital cellulitis or — rarely — meningitis, both of which are life-threatening complications of untreated bacterial sinusitis.
Special Cases — Pregnancy, Children, and Chronic Sinusitis
Sinus Infection Antibiotics During Pregnancy
Treating a sinus infection during pregnancy requires careful antibiotic selection because certain drugs cross the placenta and can harm fetal development.
Safe options (generally Category B):
- Amoxicillin: Widely used in pregnancy, strong safety record
- Amoxicillin-clavulanate: Generally considered safe in all trimesters — though some providers prefer to use it cautiously in the third trimester
- Cephalosporins (cefixime, cefpodoxime): Safe alternatives if penicillin allergy is non-severe
Avoid during pregnancy:
- Doxycycline — impairs fetal bone and tooth development; contraindicated in all trimesters
- Fluoroquinolones (levofloxacin, ciprofloxacin) — associated with fetal cartilage damage in animal studies; avoid unless no alternatives exist
- Trimethoprim-sulfamethoxazole — folate antagonism risk, especially in first trimester
Always consult your OB-GYN before starting any antibiotic during pregnancy. Use our Pregnancy Weight Gain Calculator to stay on track with healthy pregnancy metrics.
Sinus Infection Antibiotics for Children
Pediatric dosing is weight-based — never use adult dosing for children. Per the American Academy of Pediatrics (AAP):
- First-line: Amoxicillin-clavulanate (weight-based dosing, typically 45 mg/kg/day divided twice daily)
- Duration: 10 days for children under 2 years old; 5–7 days for older children with mild-moderate ABRS
- Reassessment: If no improvement within 72 hours (not 7 days as in adults), guidelines recommend switching antibiotics sooner in children
Watch for diarrhea — it is significantly more common in children taking amoxicillin-clavulanate due to the clavulanate component. Probiotic co-administration may help.
For official pediatric antibiotic guidance, see the AAP Healthy Children resource.
Chronic Sinusitis Is a Completely Different Condition
If your symptoms have lasted 12 weeks or longer, you no longer have acute sinusitis — you have chronic rhinosinusitis (CRS), and the entire treatment approach changes.
Key facts about chronic sinusitis treatment in 2026:
- Standard short-course antibiotics are NOT appropriate as primary treatment
- The 2025 AAO-HNS guideline added biologic therapy (e.g., dupilumab) as a new recommended option for CRS with nasal polyps
- CT imaging is required to confirm CRS before any antibiotic prescribing
- The 2025 guidelines explicitly discourage prescribing empiric antibiotics for CRS solely to satisfy insurance criteria for imaging or surgery authorization
If your sinus issues keep recurring, the underlying cause may be allergic — consult an allergist or immunologist for proper evaluation.
When Antibiotics Aren’t Working — And What to Do Next
The Watch-and-Wait Strategy (What Smart Doctors Do in 2026)
One of the most evidence-backed — and least communicated — strategies for bacterial sinusitis is delayed antibiotic prescribing. Here is how it works in practice:
Your doctor writes you a prescription for amoxicillin-clavulanate, hands it to you, and says: “Wait 2–5 days before filling this. If you’re not improving or are getting worse, fill it.”
This approach is now explicitly endorsed in the 2025 AAO-HNS guidelines and is backed by multiple randomized controlled trials. The key insight: the majority of even confirmed bacterial sinus infections resolve on their own within 7–10 days. Delaying the antibiotic by just a few days gives your immune system the chance to clear the infection — and saves you from unnecessary drug exposure and resistance risk.
Why Your Sinus Infection Antibiotics Might Not Be Working
If you’ve been on antibiotics for 5+ days and feel no different, here are the real reasons:
- Wrong drug class: You were given a Z-Pack, Bactrim, or another drug now excluded from guidelines due to resistance
- It’s viral: Antibiotics never work on viruses — this is the most common reason for antibiotic treatment failure
- Resistant organism: A culture-guided antibiotic switch is needed
- Fungal sinusitis: An entirely different condition requiring antifungal therapy — cannot be treated with standard antibiotics
- Misdiagnosis: Allergic rhinitis, nasal polyps, or structural issues can mimic sinusitis
2025 guideline trigger: If no improvement or worsening occurs within 3–5 days of starting the correct antibiotic, reassessment is mandatory — not at Day 7 as the older guidelines stated.
Evidence-Based Non-Antibiotic Treatments That Actually Help
Whether your infection is viral or bacterial, these adjunctive treatments have strong evidence:
✅ Proven effective:
- Intranasal corticosteroid sprays (e.g., fluticasone, budesonide) — Level A evidence, guideline-recommended as adjunctive therapy
- Saline nasal irrigation (e.g., Neti pot or saline spray) — reduces congestion, flushes bacteria, improves drainage
- Analgesics (acetaminophen or ibuprofen) — for pain and fever control
❌ Not evidence-supported for acute sinusitis:
- Antihistamines (may worsen congestion by drying out mucus)
- Oral decongestants (limited benefit, significant cardiovascular risks in some patients)
- Steam inhalation (no clinical trial support — despite widespread belief)
For guidance on managing antibiotic interactions and other drug-related questions, review our Drug Interactions guide.
The CDC’s Be Antibiotics Aware initiative provides excellent patient resources on understanding when antibiotics are truly needed — and when they aren’t.
What This Means For You: If antibiotics aren’t working, do not request a stronger antibiotic — request a proper clinical reassessment first. The problem may not be the antibiotic’s strength; it may be that you never needed one at all.
FAQs — Sinus Infection Antibiotics
Q1. Do I always need antibiotics for a sinus infection?
No. 90–98% of sinus infections are viral. Antibiotics are only appropriate when bacterial infection is confirmed or strongly suspected based on the three clinical criteria above.
Q2. What is the #1 recommended antibiotic for sinus infection in 2026?
Amoxicillin-clavulanate (Augmentin) is the first-line recommendation per the 2025 AAO-HNS and IDSA guidelines for most adults with confirmed bacterial sinusitis.
Q3. Is the Z-Pack good for sinus infections?
No. The 2025 updated guidelines explicitly exclude azithromycin (Z-Pack) from sinusitis treatment due to widespread bacterial resistance. It is no longer an appropriate first-line sinus infection antibiotic in the US.
Q4. How long should I take sinus infection antibiotics?
The 2025 guideline update shortened the recommended course to 5–7 days for most adults — down from the previously recommended 10–14 days.
Q5. Can sinus infection antibiotics make me feel worse before better?
Yes. Days 1–2 often show little change as the antibiotic builds to therapeutic levels. Improvement typically begins at Day 3–4.
Q6. What antibiotic for sinus infection is safe during pregnancy?
Amoxicillin and amoxicillin-clavulanate are generally considered safe. Avoid doxycycline and fluoroquinolones during pregnancy. Always consult your OB-GYN first.
Q7. What happens if bacterial sinusitis goes untreated?
Most cases still resolve on their own. However, a small percentage can progress to serious complications including orbital cellulitis, meningitis, or brain abscess — which is why reassessment at Day 3–5 of antibiotic therapy matters.
Q8. Can I get sinus infection antibiotics without a prescription?
No. All antibiotics for sinus infections require a prescription in the USA, UK, Canada, and Australia.
Q9. Is amoxicillin or Augmentin better for sinus infection?
For most adults with bacterial sinusitis: Augmentin (amoxicillin-clavulanate) per 2025 guidelines. For healthy, low-risk patients in low-resistance communities: plain amoxicillin may suffice.
Q10. Why did my doctor tell me to wait before taking my antibiotic prescription?
This is the evidence-based “delayed prescribing” strategy endorsed by the 2025 AAO-HNS guidelines. It allows most bacterial sinus infections to resolve naturally, reducing unnecessary antibiotic resistance.
Q11. How do I know my sinus infection is getting better on antibiotics?
Look for fever reduction, thinning nasal discharge, and decreasing facial pressure by Day 3–4. No improvement by Day 5 warrants a call to your doctor.
Key Takeaways: Sinus Infection Antibiotics in 2026
- 90–98% of sinus infections are viral — most people do not need an antibiotic
- Amoxicillin-clavulanate is now the first-line sinus infection antibiotic per 2025 guidelines
- Z-Pack, Bactrim, and other macrolides are no longer recommended — resistance is too high
- Treatment duration is 5–7 days — not the outdated 10–14 day courses still being prescribed
- No improvement by Day 3–5 on the correct antibiotic = mandatory reassessment
- Delayed prescribing is now a legitimate, guideline-endorsed strategy
For official guidance, visit the CDC’s Sinus Infection page — and always follow your doctor’s direct clinical assessment over any online resource.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.