On This Page – Quick Medical Summary
Ryan, 41, a project manager from Chicago, had been sleeping 8 hours every night for two years — yet he woke up exhausted every single morning. His wife had started sleeping in the guest room because of his snoring. After finally seeing a sleep specialist, the diagnosis was immediate: obstructive sleep apnea, one of the most underdiagnosed sleep disorders in the United States.
His story is far from unique.
A sleep disorder is a medical condition that disrupts the quality, timing, or duration of sleep — preventing the body from performing the essential restoration it needs. There are over 80 recognized types, and according to the National Heart, Lung, and Blood Institute (NHLBI), approximately 50 to 70 million Americans are currently affected.
Sleep disorders are not just an inconvenience. Left untreated, they are directly linked to dementia, cardiovascular disease, type 2 diabetes, and significantly shortened lifespan. This 2026 guide covers every type, symptom, cause, diagnostic tool, and treatment option — the complete picture your doctor may not have time to give you.
What Is a Sleep Disorder? Types & 2026 Global Statistics
How Common Are Sleep Disorders — Really?
The scale of this problem in America is staggering. Globally, researchers estimate over 1 billion people experience some form of chronic sleep disruption. In the US alone:
- 50–70 million Americans have a diagnosed sleep disorder
- 1 in 3 American adults regularly fail to get the recommended 7–8 hours
- Undiagnosed sleep apnea alone costs the U.S. economy an estimated $150 billion annually in healthcare and lost productivity
Women are more likely to suffer from insomnia, while men are disproportionately affected by sleep apnea. Both disorders peak between ages 40–65 — but they can affect anyone, including teenagers and children.
💡 Not sure how much sleep you actually need? Use our Sleep Calculator to find your ideal sleep duration based on your age and wake-up schedule.
The 8 Most Common Sleep Disorders — Quick Reference Guide
| Sleep Disorder | Primary Symptom | Most Affected Group | US Prevalence |
|---|---|---|---|
| Insomnia | Can’t fall or stay asleep | Adults, women, elderly | 30% (10% chronic) |
| Obstructive Sleep Apnea (OSA) | Breathing pauses during sleep | Overweight adults, men | 30M+ Americans |
| Restless Legs Syndrome (RLS) | Irresistible urge to move legs at night | Adults 40–70 | 5–10% adults |
| Narcolepsy | Sudden, uncontrollable sleep attacks | All ages | 0.02–0.05% |
| Parasomnias | Sleepwalking, night terrors, sleep talking | Children primarily | Up to 20% of children |
| Circadian Rhythm Disorders | Internal clock out of sync with environment | Shift workers, teens | ~3% adults |
| Hypersomnia | Excessive daytime sleepiness despite adequate sleep | Adults 17–45 | 4–6% |
| REM Sleep Behavior Disorder (RBD) | Physically acting out dreams | Men over 50 | 0.5–1% |
These eight conditions account for the vast majority of sleep disorder diagnoses. The NHLBI’s sleep disorders research division notes that many cases remain undiagnosed for years because patients assume fatigue is “just stress.”
Sleep Disorder Symptoms — What Your Body Is Telling You
“I thought I was just a bad sleeper.” That’s what most patients say before diagnosis. The reality is that persistent sleep problems are almost always a signal of an underlying sleep disorder — not a personality trait.
Universal Warning Signs of a Sleep Disorder
Look for these symptoms occurring 3 or more nights per week, for more than a month:
- Difficulty falling asleep — consistently taking more than 30 minutes
- Frequent nighttime awakenings — waking 2+ times and struggling to return to sleep
- Loud snoring, gasping, or choking sounds during sleep (often reported by a partner)
- Unrefreshing sleep — waking exhausted despite a full night in bed
- Excessive daytime sleepiness — struggling to stay awake at work, meetings, or while driving
- Irresistible urge to move legs at night, especially when resting or lying down
- Mood changes — unexplained irritability, depression, or anxiety correlated with poor sleep
- Memory lapses or difficulty concentrating during the day
🚨 Red Flag Symptoms: Seek Medical Evaluation Within 1–2 Weeks
The following symptoms require prompt medical attention — do not wait:
- A partner witnesses you stop breathing during sleep (this is a hallmark OSA sign)
- Falling asleep involuntarily while driving, eating, or speaking mid-sentence
- Sleep paralysis lasting several minutes, accompanied by hallucinations
- Physically acting out violent or vivid dreams — kicking, punching, or falling out of bed during sleep
- Sudden loss of muscle tone triggered by laughter or emotion (cataplexy — a narcolepsy marker)
- Child over age 7 with persistent bedwetting, night terrors, and daytime behavioral issues
Not sure if your symptoms indicate a sleep disorder? Use our Symptom Checker for a personalized assessment to guide your next step.
Sleep Disorder Symptoms: Children vs. Adults
| Symptom | In Children | In Adults |
|---|---|---|
| Insomnia | Bedtime resistance, frequent night wakings, nightmares | Difficulty initiating or maintaining sleep, 3AM awakenings |
| Sleep Apnea | Mouth breathing, hyperactivity, poor academic performance | Loud snoring, morning headaches, daytime fatigue |
| Narcolepsy | Sudden muscle weakness (cataplexy), declining school grades | Sleep attacks at work or while driving |
| Parasomnias | Sleepwalking, night terrors, bedwetting | REM behavior disorder, sleep paralysis episodes |
| Circadian Disorders | Delayed sleep phase (can’t sleep until very late) | Shift work disorder, jet lag disorder |
What This Means For You: A 2024 study published in the Journal of Sleep Research found that just one hour of screen time before bed reduces sleep duration by 24 minutes and raises insomnia risk by 59%. Reducing screen exposure 60–90 minutes before bedtime is one of the single most evidence-backed interventions available — at zero cost.
What Causes Sleep Disorders — Medical, Psychological & Lifestyle Triggers
Sleep disorders rarely have a single cause. They typically develop from a combination of biological vulnerability, psychological stress, and lifestyle factors interacting with one another. Understanding your specific triggers is the first step toward effective treatment.
Medical Causes of Sleep Disorders
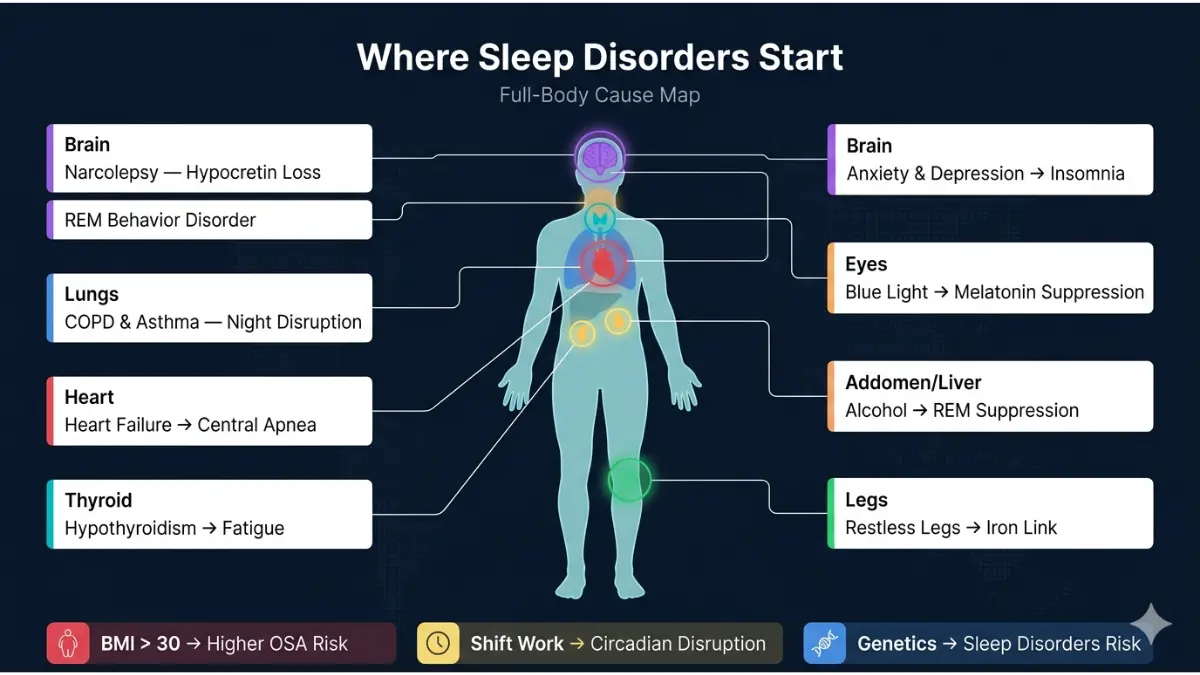
Physical health conditions are among the most common and frequently overlooked drivers of sleep disorders:
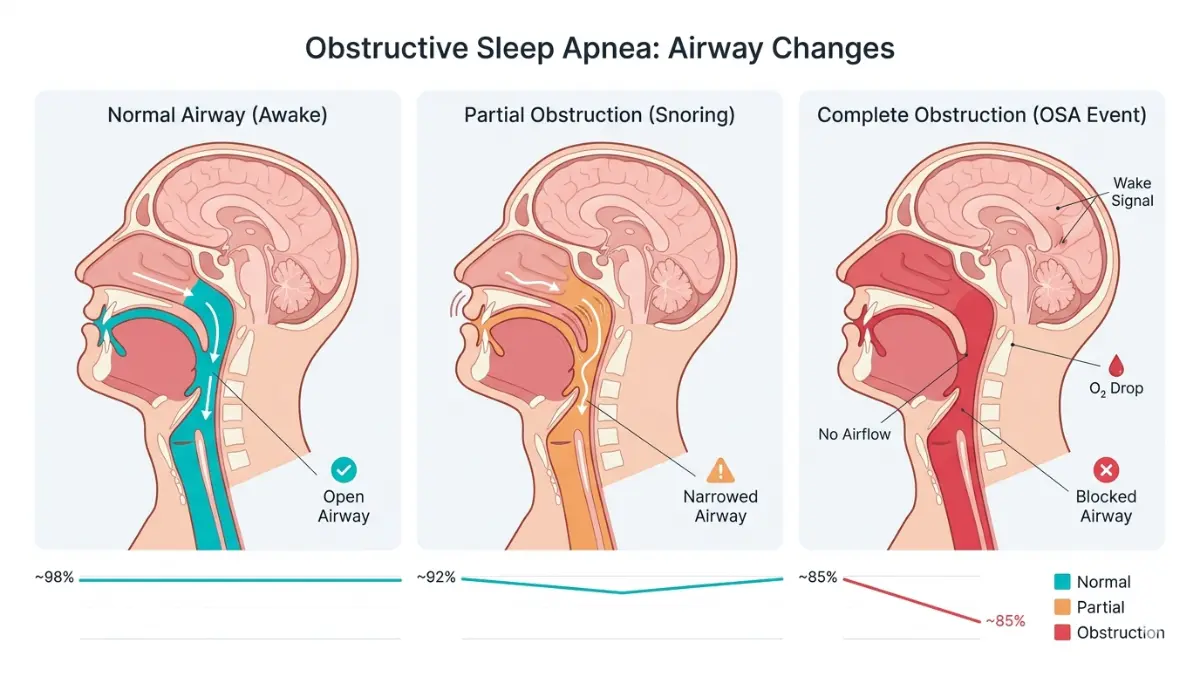
- Obesity — A BMI over 30 triples the risk of obstructive sleep apnea. Excess tissue around the neck collapses the airway during sleep. Check your weight status using our BMI Calculator if you’re concerned about OSA risk.
- Chronic pain — Arthritis, fibromyalgia, and lower back pain fragment sleep architecture
- Neurological conditions — Parkinson’s disease is strongly associated with REM Sleep Behavior Disorder; Alzheimer’s disrupts circadian rhythms
- Thyroid disorders — Hypothyroidism causes excessive daytime sleepiness and fatigue mimicking hypersomnia
- Cardiovascular disease — Heart failure is linked to central sleep apnea
- COPD and asthma — Nighttime respiratory symptoms shorten and fragment sleep
Medications that disrupt sleep include: beta-blockers (linked to insomnia and vivid dreams), antidepressants (can worsen RLS), corticosteroids (stimulant effect), and decongestants. If you recently started a new medication and sleep has worsened, always discuss this with your prescribing doctor. Our Pill Identifier can help you look up known sleep-related side effects of your current medications.
Psychological Causes of Sleep Disorders
Mental health and sleep disorders have a deeply bidirectional relationship — each makes the other significantly worse:
- Anxiety and depression are present in 40–50% of chronic insomnia cases, according to the American Academy of Family Physicians
- PTSD causes hyperarousal that prevents deep sleep stages and triggers nightmare disorder
- ADHD — A landmark 2025 study confirmed that ADHD traits in adults are strongly linked to insomnia and reduced life satisfaction through a vicious sleep-deprivation cycle
If you’re managing anxiety or depression alongside sleep problems, treating both simultaneously produces the best outcomes. Our guide on reducing anxiety naturally covers evidence-based non-medication approaches used alongside sleep treatment.
Lifestyle & Environmental Causes
The most modifiable causes of sleep disorders involve daily habits:
- Irregular sleep-wake schedules — rotating shifts and variable bedtimes disrupt circadian rhythm
- Caffeine after 2 PM — caffeine’s half-life is 5–7 hours, meaning afternoon coffee is still active at midnight
- Alcohol — alcohol initially sedates but causes sleep fragmentation in the second half of the night; it suppresses REM sleep and worsens OSA
- Excessive blue light exposure from phones, tablets, and computers suppresses melatonin production
- Sedentary lifestyle — regular aerobic exercise is proven to reduce insomnia severity
Genetic & Age-Related Causes
- Narcolepsy is caused by the near-total destruction of hypocretin (orexin)-producing neurons in the hypothalamus — a process that appears to involve genetic predisposition combined with an autoimmune trigger
- Circadian rhythm delays are biologically programmed into adolescence — teenagers are not “lazy,” their melatonin release is genuinely shifted later
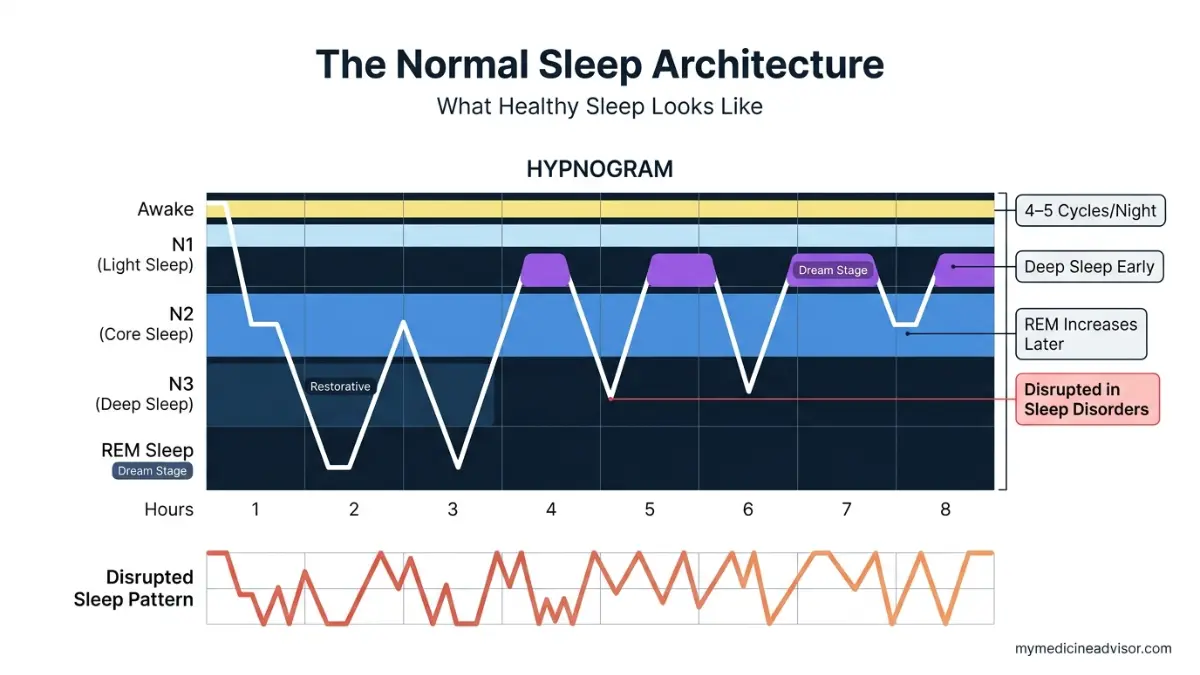
- Aging naturally reduces slow-wave (N3) deep sleep by approximately 2% per decade after age 30, making older adults more susceptible to fragmented and nonrestorative sleep
- According to NHLBI sleep disorder research, circadian disorders can also be long-term conditions caused by aging, genetics, or chronic medical illness
How Sleep Disorders Are Diagnosed — From Symptom History to Sleep Study
Getting a sleep disorder diagnosis is simpler than most Americans expect. The majority of cases are identified through clinical history alone — a sleep study is only needed in specific circumstances.
The Standard Diagnostic Journey — Step by Step
Step 1 — Clinical Sleep History Your doctor will ask about your sleep schedule, daytime symptoms, medical history, and medications. They may ask your bed partner to describe what they observe.
Step 2 — Sleep Diary (2 Weeks) You record daily sleep and wake times, caffeine intake, and daytime energy. This reveals patterns invisible in a one-time office visit.
Step 3 — Standardized Questionnaires
- Epworth Sleepiness Scale — scores daytime sleepiness from 0 to 24 (score of 10+ suggests a sleep disorder)
- STOP-BANG questionnaire — screens specifically for obstructive sleep apnea risk
Step 4 — Home Sleep Apnea Test (HSAT) A portable monitor worn overnight at home, measuring oxygen levels, airflow, and respiratory effort. Now the first-line diagnostic tool for most OSA cases. You do not need an overnight hospital stay for most sleep apnea diagnoses.
Step 5 — Polysomnography (In-Lab Sleep Study) The gold standard for complex or ambiguous cases. Sensors monitor brain waves (EEG), eye movements, heart rate, blood oxygen, and limb movements simultaneously throughout the night.
Step 6 — Multiple Sleep Latency Test (MSLT) Measures how quickly you fall asleep during five scheduled 20-minute nap opportunities throughout the day. A mean sleep latency of under 8 minutes confirms excessive daytime sleepiness; under 5 minutes with REM intrusions confirms narcolepsy.
As described in the NHLBI’s diagnostic guidelines, doctors select the appropriate test based on your specific symptom profile — not every patient needs a full polysomnography.
Sleep Disorder Diagnostic Tests — Quick Comparison
| Test | Best Used For | Setting | Approximate US Cost |
|---|---|---|---|
| Sleep Diary | All disorders — initial evaluation | Home | Free |
| Epworth Scale | Screening for daytime sleepiness | Office | Free |
| Home Sleep Apnea Test | Suspected obstructive sleep apnea | Home | $150–$500 |
| Polysomnography (PSG) | Complex/multiple suspected disorders | Sleep lab | $1,000–$3,500 |
| MSLT | Narcolepsy, hypersomnia confirmation | Sleep lab | $1,500–$3,000 |
| Actigraphy | Circadian rhythm disorders | Home (wrist device) | $200–$400 |
2025 Technology Breakthrough: AI-powered sleep analysis algorithms can now predict insomnia onset with 89% accuracy — up to three months before traditional methods detect it (Nature Digital Medicine, 2025). Wearables like the Apple Watch detect sleep stages with 78% accuracy compared to polysomnography. While not yet diagnostic, these tools are transforming early identification of sleep disorders.
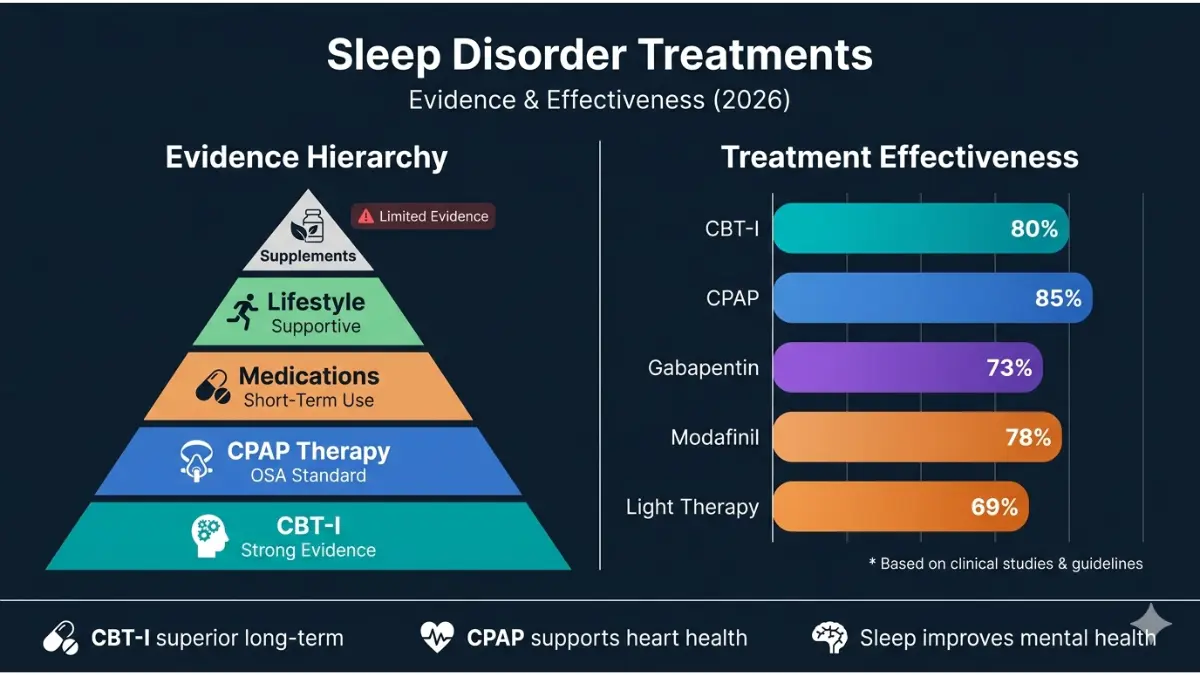
Sleep Disorder Treatments That Actually Work — Complete 2026 Evidence Guide
Treatment success rates exceed 80% when the right therapy is matched to the right disorder. Yet the average American waits nearly 7 years from first symptoms to receiving appropriate treatment — mostly because sleep disorders are normalized rather than recognized.
Here is every evidence-based treatment option, ranked by evidence strength:
Cognitive Behavioral Therapy for Insomnia (CBT-I) — The Gold Standard
CBT-I is the #1 first-line treatment for chronic insomnia, recommended ahead of medication by the American College of Physicians, the American Academy of Sleep Medicine, and the NIH.
A landmark meta-analysis of 61 randomized controlled trials involving 11,571 patients confirmed that CBT-I significantly:
- Reduces time to fall asleep (sleep onset latency)
- Reduces nighttime awakenings
- Improves overall sleep efficiency
- Produces more durable results than sleeping pills — effects persist after therapy ends
CBT-I core techniques:
- Sleep restriction therapy — limits time in bed to match actual sleep time, consolidating sleep
- Stimulus control — bed is for sleep only; leave if you can’t sleep within 20 minutes
- Cognitive restructuring — identifies and challenges catastrophic thoughts about sleep
- Relaxation training — progressive muscle relaxation, diaphragmatic breathing
- Sleep hygiene education — consistent schedule, light exposure, caffeine management
CBT-I is now available digitally. Apps like Sleepio and Somryst (FDA-cleared) deliver CBT-I with outcomes equivalent to in-person therapy. This removes the access barrier for millions of Americans who can’t reach a sleep specialist.
The NHLBI’s treatment guidelines confirm CBT-I as the recommended behavioral approach before any pharmacological treatment is considered.
CPAP Therapy for Sleep Apnea
Continuous Positive Airway Pressure (CPAP) remains the gold standard for moderate-to-severe OSA. It delivers a gentle stream of pressurized air that prevents throat tissue from collapsing during sleep.
Key 2024–2025 CPAP developments:
- A new once-nightly medication formulation for OSA (approved 2024) improved patient CPAP compliance by 40%, per American Academy of Sleep Medicine data
- Auto-adjusting CPAP (APAP) now automatically calibrates pressure throughout the night, eliminating the need for in-lab titration in most patients
Alternatives to CPAP for sleep apnea:
- Oral appliances (mandibular advancement devices) — repositions the jaw; effective for mild-moderate OSA
- Positional therapy — for patients whose OSA only occurs sleeping on their back
- Surgical options — uvulopalatopharyngoplasty (UPPP), hypoglossal nerve stimulation (Inspire device) for CPAP-intolerant patients with severe OSA
Medications for Sleep Disorders — What Works, What Doesn’t, and the 2025 Safety Alert
| Sleep Disorder | Medication Options | Key Consideration |
|---|---|---|
| Chronic Insomnia | Zolpidem, Eszopiclone, Suvorexant, Ramelteon | Short-term use only; risk of dependence |
| Narcolepsy | Modafinil, Armodafinil, Sodium oxybate, Pitolisant | Pitolisant (non-stimulant) gaining favor in 2025 guidelines |
| RLS | Gabapentin, Pregabalin, Pramipexole, Ropinirole | Dopamine agonists risk “augmentation” with long-term use |
| REM Behavior Disorder | Melatonin (high-dose), Clonazepam | Melatonin first-line due to better safety profile |
| Circadian Disorders | Low-dose melatonin, Light therapy | See critical 2025 warning below |
⚠️ 2025 Cardiac Safety Alert — Melatonin: Melatonin is widely perceived as harmless. However, a 2025 study found that chronic long-term melatonin users were nearly twice as likely to die and 3.5 times more likely to be hospitalized for heart failure compared to non-users. Short-term use for jet lag or circadian adjustment remains considered low-risk. Always consult your doctor before taking melatonin regularly. Do not use it as a nightly sleep aid indefinitely without medical supervision.
Lifestyle & Sleep Hygiene — The Foundation Every Treatment Builds On
No medication or therapy works optimally without strong sleep hygiene foundations. Evidence-based recommendations for 2026:
- Fixed sleep/wake time — same time every day, including weekends; this is the single highest-impact habit change
- Sleep environment: Dark (blackout curtains), cool (18–20°C / 64–68°F), and quiet or with white noise
- Caffeine cutoff: No caffeine after 1–2 PM — caffeine’s 5–7 hour half-life means afternoon consumption directly impairs sleep architecture
- Alcohol: Avoid within 3 hours of bedtime — it suppresses REM sleep and worsens breathing disorders
- Exercise: A 2025 large-scale meta-analysis confirmed yoga, Tai Chi, walking, and jogging are among the best non-pharmacological interventions for insomnia — effective even in older adults
- Blue light: Reduce screen exposure 60–90 minutes before bed; blue-light filtering increases melatonin production by up to 58% (Journal of Applied Physiology, 2025)
Weight management matters more than most patients realize. Because obesity is a primary driver of sleep apnea, losing even 10% of body weight can reduce OSA severity significantly. Our Weight Loss Calculator and Calorie Deficit Calculator can help you build a sustainable plan alongside your treatment program.
Emerging Treatments: What’s Coming in 2025–2026
- Hypocretin (orexin) replacement therapy — currently in Phase III trials for narcolepsy; aims to replace the exact neurons destroyed in the condition. Potentially the first true cure for narcolepsy Type 1.
- New narcolepsy brain circuit target — A 2024 Nature Neuroscience study identified a specific brain circuit responsible for maintaining wakefulness, opening new pharmacological targets
- AI-integrated sleep coaching — algorithm-guided CBT-I delivery with real-time wearable data input; showing outcomes comparable to specialist-delivered therapy at a fraction of the cost
- Transcranial magnetic stimulation (TMS) — emerging evidence for treatment-resistant insomnia in patients with comorbid depression
Long-Term Risks, Prevention & When to See a Doctor
What Happens When Sleep Disorders Go Untreated?
The consequences extend far beyond feeling tired. Chronic untreated sleep disorders are now recognized as independent risk factors for some of the most serious medical conditions in America:
Brain and cognitive health:
- A landmark Mayo Clinic study (September 2025) found chronic insomnia raises dementia and cognitive impairment risk by 40%. Brain scans showed measurable structural changes in long-term poor sleepers.
- Sleep apnea during REM sleep is specifically linked to degeneration of memory-related brain regions via damage to cerebral small blood vessels (May 2025, major neurology journal)
Heart and cardiovascular health:
- Severe OSA is associated with a twofold increase in sudden cardiac death and cardiovascular mortality, per meta-analysis data cited by the American Academy of Family Physicians
- A 2025 study confirmed sleep apnea during REM sleep contributes to dementia especially in women over 65
Metabolic and hormonal effects:
- Sleep deprivation dysregulates leptin and ghrelin — the hormones controlling hunger and satiety. Sleeping under 6 hours increases obesity risk by 55% in adults and 89% in children
- Chronic sleep disorder is an independent risk factor for Type 2 diabetes through insulin resistance mechanisms
- Tracking your metabolic health while managing sleep disorders is important — our Blood Sugar Converter and BMR Calculator can support this monitoring
Mental health:
- The insomnia-depression cycle is vicious and bidirectional: insomnia increases depression risk by 2–3x, and depression worsens insomnia severity
- Untreated ADHD-sleep disorder comorbidity significantly reduces quality of life and occupational performance
Safety:
- Daytime sleepiness from undiagnosed sleep disorders produces impairment equivalent to a blood alcohol level of 0.08% — the US legal driving limit
- Sleep disorders are implicated in an estimated 100,000 motor vehicle accidents annually in the United States
Prevention: Protecting Your Sleep Long-Term
- Treat underlying conditions proactively — obesity, anxiety, thyroid disorders, and cardiovascular disease are the top modifiable risk factors
- Protect your circadian rhythm: consistent meal times, morning light exposure, and a fixed wake time signal your internal clock
- Annual sleep health review after age 50 — when sleep architecture changes accelerate and OSA risk rises sharply
- Limit shift work where possible; if unavoidable, use strategic light exposure and melatonin timing (short-term) to help circadian adaptation
- The NHLBI’s circadian rhythm disorder resource provides detailed guidance on protecting your body clock in high-risk occupations
When Should You See a Doctor? — Your Decision Guide
| Your Situation | Recommended Action |
|---|---|
| Occasional poor sleep (1–2 nights/week) | Self-care: sleep hygiene improvements first |
| Poor sleep 3+ nights/week for more than 1 month | See your primary care physician |
| Partner witnesses breathing pauses during sleep | Urgent: OSA evaluation within 1–2 weeks |
| Excessive daytime sleepiness affecting work or driving | Prompt: Medical evaluation within 1 week |
| Sleep paralysis, acting out dreams violently | Specialist referral (sleep neurologist) |
| Child with persistent snoring + behavioral/school issues | Pediatric sleep evaluation |
| Senior adult with new sleep difficulties + memory concerns | Neurological + sleep evaluation |
📋 Disclaimer: This article is for educational purposes only and does not constitute medical advice, diagnosis, or treatment. Always consult a qualified and licensed healthcare professional for the diagnosis and management of sleep disorders or any other medical condition.
Frequently Asked Questions About Sleep Disorders
1. What is the most common sleep disorder in the United States?
Insomnia is the most common sleep disorder, affecting up to 30% of the US adult population. Approximately 10% of American adults have chronic insomnia — defined as difficulty sleeping at least 3 nights per week for more than 3 months.
2. Can a sleep disorder be permanently cured?
Many sleep disorders are highly treatable, though not always curable. Insomnia often resolves completely with CBT-I. Sleep apnea is managed long-term with CPAP or through weight loss and surgery in some patients. Narcolepsy currently has no cure, though treatments effectively control symptoms.
3. How do I know if I have a sleep disorder or just poor sleep habits?
If sleep problems occur 3+ nights per week for more than a month, cause daytime impairment, and persist despite basic sleep hygiene improvements, this strongly suggests a sleep disorder rather than simple poor habits. A clinical evaluation confirms the distinction.
4. Are sleep disorders genetic?
Yes, for several types. Narcolepsy involves a specific genetic predisposition affecting hypocretin neurons. Restless legs syndrome shows clear familial inheritance patterns. Circadian rhythm disorders and sleep apnea also have documented heritable components.
5. Can anxiety and stress cause a sleep disorder?
Absolutely. Anxiety and depression are present in 40–50% of chronic insomnia cases. More importantly, the relationship is bidirectional — insomnia worsens anxiety, and anxiety worsens insomnia. Treating both simultaneously produces the best long-term outcomes.
6. What is the best treatment for insomnia without medication?
Cognitive Behavioral Therapy for Insomnia (CBT-I) is the most effective non-medication treatment for chronic insomnia — consistently outperforming sleeping pills in long-term outcomes across 61 randomized controlled trials. Sleep restriction, stimulus control, and cognitive restructuring are its core tools.
7. Do children get sleep disorders?
Yes. Up to 20% of children experience parasomnias (sleepwalking, night terrors). Sleep apnea, circadian disorders, and insomnia also affect school-age children — often misidentified as ADHD or behavioral problems due to overlapping symptoms.
8. Does poor sleep cause weight gain?
Directly, yes. Sleep deprivation elevates ghrelin (hunger hormone) and suppresses leptin (satiety hormone), driving increased calorie intake. Adults consistently sleeping under 6 hours per night are 55% more likely to become obese over time.
9. Is untreated sleep apnea dangerous?
Untreated severe sleep apnea doubles the risk of sudden cardiac death and is strongly associated with hypertension, stroke, atrial fibrillation, and type 2 diabetes. It also significantly increases dementia risk — particularly in women over 65, per 2024 research.
10. Is it safe to take melatonin every night?
Short-term melatonin use (2–4 weeks) for jet lag or circadian adjustment is generally considered low-risk. However, a 2025 study linked chronic long-term melatonin use to nearly doubled mortality and 3.5x elevated heart failure hospitalization risk. Do not use melatonin as a permanent nightly sleep aid without physician guidance.
11. When is it an emergency to see a doctor about sleep problems?
Seek urgent evaluation if: your partner witnesses you stop breathing during sleep, you fall asleep uncontrollably while driving or operating machinery, or you physically act out violent dreams. These symptoms require evaluation within days, not months.
Reviewed by the mymedicineadvisor.com Medical Panel | mymedicineadvisor.com | For more health guidance, explore our Health Tips Library
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.