On This Page – Quick Medical Summary
Michael, a 44-year-old accountant from Chicago, had been jolting awake at 3:12am every single night for six weeks. Wide-eyed, heart pounding, mind racing — then two frustrating hours of staring at the ceiling before his alarm went off. He wasn’t anxious. He wasn’t stressed. He had no idea why.
His doctor found the answer in 20 minutes: undiagnosed obstructive sleep apnea.
If you’re waking up at 3am every night, there is almost always a specific medical cause — and it is almost always fixable. The key is identifying which of the nine proven triggers is driving your nocturnal awakening, then applying the right targeted intervention.
According to the CDC’s sleep health data, more than 1 in 3 American adults regularly fail to get enough quality sleep — and middle-of-the-night waking is one of the most common complaints driving that statistic.
This guide gives you what no competitor does: a full diagnostic framework, a red-flag triage system, and a cause-by-cause fix plan — all in one place.
Why Does It Always Happen at 3am? The Science Behind the Timing
Your Sleep Cycle Is the Starting Point
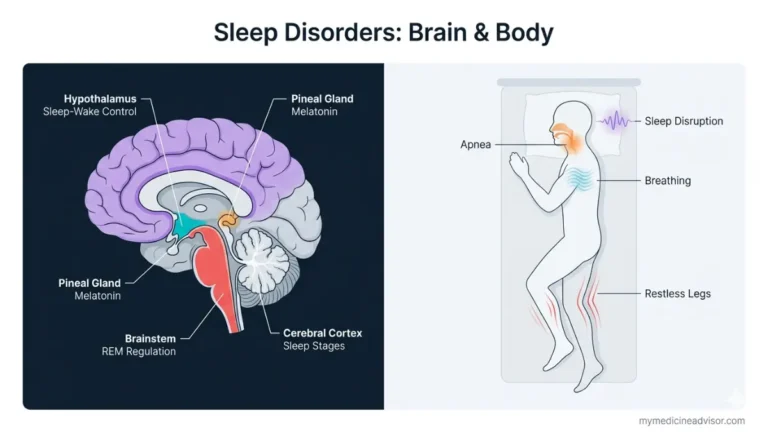
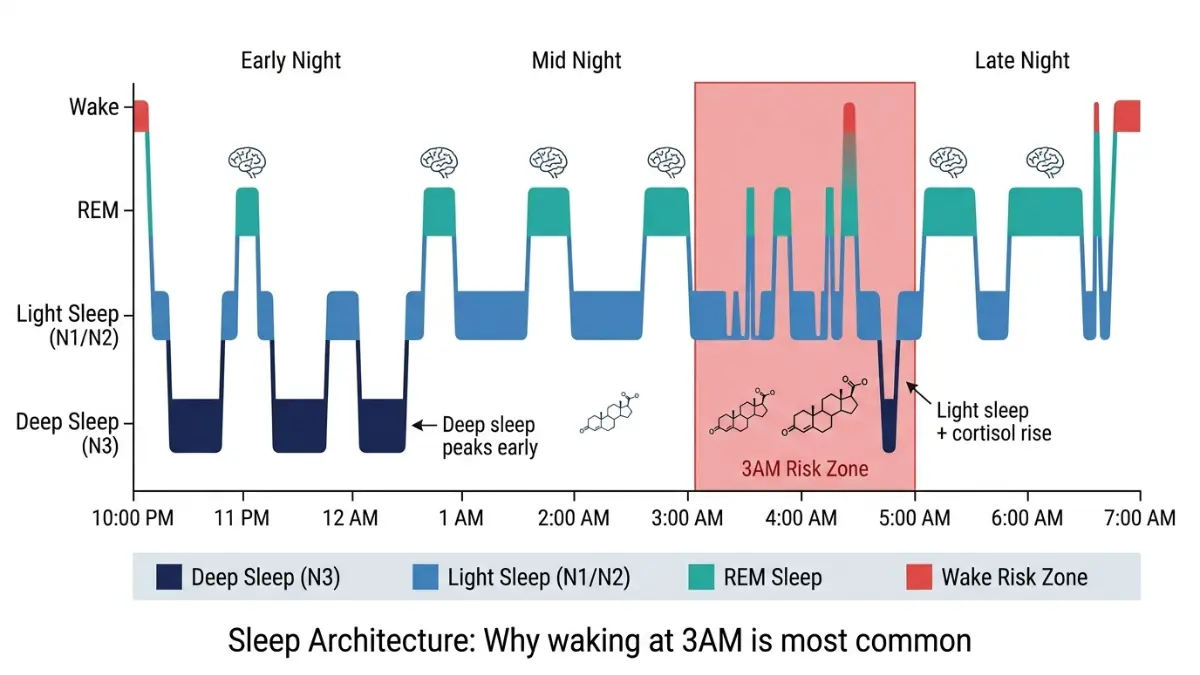
Your body doesn’t sleep in one long unbroken block. Sleep moves through four stages in roughly 90-minute cycles — cycling from light NREM sleep, into deep slow-wave sleep, and then into REM (rapid eye movement) sleep.
Early in the night, your cycles are dominated by deep, restorative slow-wave sleep. But by 3am — after 4 to 5 completed cycles — your body has largely finished its deep sleep quota. You are now spending most of your time in light REM sleep, which is the stage most vulnerable to disruption.
Understanding your sleep stages and how REM works is the foundation for understanding why 3am becomes a biological weak point every single night.
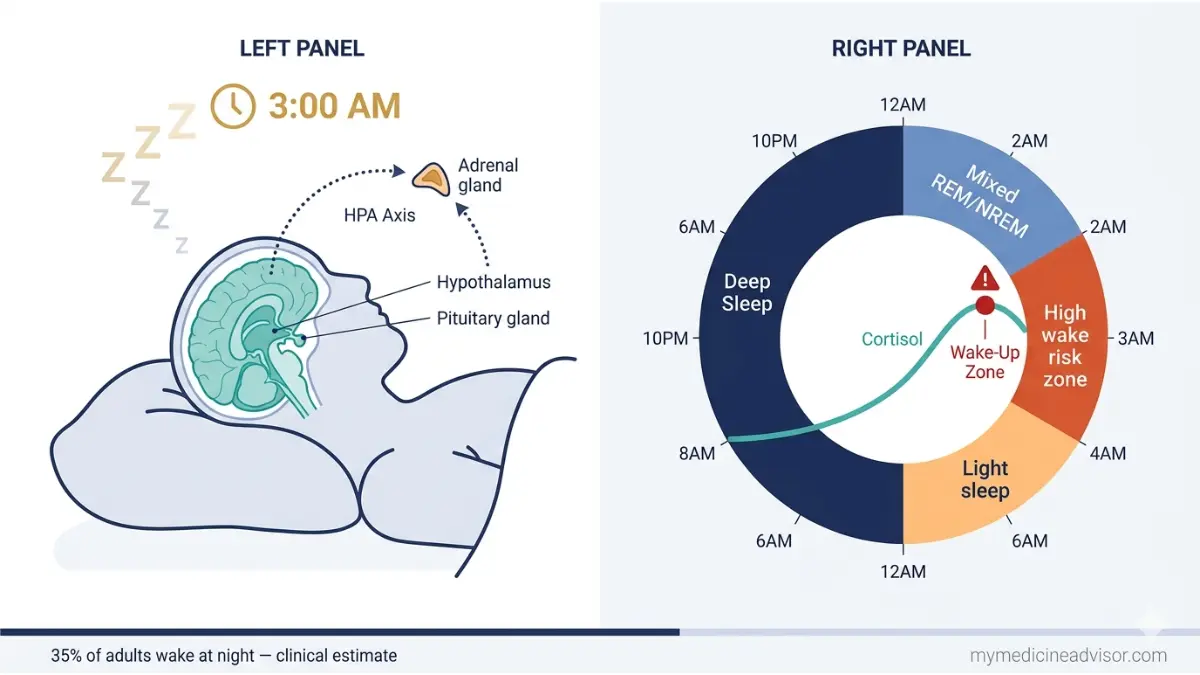
The 3am Cortisol Surge — The Most Overlooked Medical Cause
Here is what almost no other article explains clearly: cortisol — your primary stress and wakefulness hormone — follows a precise 24-hour rhythm.
Cortisol reaches its lowest point around midnight, then gradually begins rising from approximately 2am onward in preparation for morning waking. This is a normal, healthy process. But when you are under chronic stress, suffer from anxiety, or have HPA axis dysfunction, this cortisol rise starts earlier or spikes harder — jolting you awake at 3am instead of gently rising toward your 7am alarm.
The hypothalamic-pituitary-adrenal (HPA) axis — the control system governing cortisol release — is disrupted in approximately 60% of chronic insomnia patients, according to research published in peer-reviewed sleep medicine literature. This circadian rhythm disruption is one of the most under-recognized medical causes of sleep disorders in adults.
The Nervous System Handoff
Between 2am and 4am, your body also begins transitioning from its parasympathetic (rest-and-digest) state toward its sympathetic (fight-or-flight) state in preparation for the day. When this handoff tips too early or too aggressively, the result is premature waking.
Key Takeaway: 3am is not random. It is the convergence of your lightest sleep stage, your natural cortisol rise, and your nervous system shift — all occurring simultaneously. Any additional medical trigger at this window becomes amplified.
| Time Zone | Sleep Stage | Cortisol Level | Wake Vulnerability |
|---|---|---|---|
| 10pm – 12am | Deep NREM (slow-wave) | Very Low | Very Low |
| 12am – 2am | Mixed REM/NREM | Rising Slightly | Low |
| 2am – 4am | Light REM (dominant) | Actively Rising | Very High |
| 4am – 6am | Light REM / early wake | High | High |
9 Proven Medical Causes of Waking Up at 3am Every Night
This is the diagnostic core of the article. Each medical cause below follows a clear pattern: what it is → what you feel at 3am → who is most at risk → what to do first.
Not sure which cause matches your pattern? Use the free Symptom Checker at mymedicineadvisor.com to map your symptoms before your next doctor’s visit.
1. Cortisol Surge & HPA Axis Dysregulation
What happens: Chronic stress shifts your cortisol awakening response earlier in the night. Instead of peaking at 7am, it fires at 3am — activating the brain’s arousal system prematurely.
What you feel: Sudden alertness, racing thoughts, inability to switch off the mind. No specific physical symptom, just wide-awake mental activation.
Who’s most at risk: High-stress professionals, caregivers, people with anxiety history, perfectionists, shift workers.
First action: Salivary cortisol panel (4-point test), cognitive behavioral therapy for insomnia (CBT-I), morning light exposure protocol to re-anchor the circadian rhythm.
2. Obstructive Sleep Apnea (OSA)
What happens: During REM sleep — which dominates after 2am — airway muscle tone drops to its lowest point. In people with OSA, this triggers breathing cessation events that cluster heavily in the 2–6am window. Oxygen drops, the brain fires an emergency arousal response, and you wake up — often not remembering why.
What you feel: Gasping or choking sensation, dry mouth, morning headache, excessive daytime sleepiness. A bed partner may report loud snoring or witnessed pauses in breathing.
Who’s most at risk: Men over 40, people with obesity, those with a thick neck circumference, post-menopausal women. Approximately 22 million Americans have sleep apnea — and most are undiagnosed.
First action: Report to your doctor immediately if you wake gasping. A home sleep apnea test (HSAT) or full polysomnography (sleep study) is required for diagnosis. The NHLBI’s sleep science resource confirms untreated sleep apnea significantly raises cardiovascular risk.
3. Nocturnal Hypoglycemia (Blood Sugar Drop)
What happens: Your brain is the most glucose-dependent organ in the body. When blood sugar drops too low overnight — typically 4–6 hours after your last meal — your body releases adrenaline, cortisol, and glucagon to bring levels back up. This counter-regulatory hormonal surge jolts you awake. This is sometimes called the Somogyi Effect and is especially common in people with insulin resistance, pre-diabetes, or type 2 diabetes.
What you feel: Heart racing, sweating, hunger, shakiness, mild confusion. Symptoms often resolve after eating.
Who’s most at risk: People with diabetes or insulin resistance, anyone who ate a high-carbohydrate dinner late at night, people who drink alcohol before bed (alcohol causes delayed glucose crashes).
First action: Use our Blood Sugar Converter to understand your readings, and discuss continuous glucose monitoring (CGM) with your doctor to detect overnight patterns invisible to fasting labs.
4. Anxiety & Nocturnal Panic
What happens: People with anxiety disorders have a chronically hyperactivated HPA axis — their brain remains on “threat alert” even during sleep. At the 3am REM/cortisol crossover point, this hyperarousal breaks through into full waking. In some people, this escalates into nocturnal panic attacks — sudden intense episodes of terror, heart pounding, and dread that feel almost indistinguishable from a cardiac event.
What you feel: Sudden heart racing, overwhelming sense of dread or doom, physical tension, difficulty breathing. Often accompanied by racing thoughts about tomorrow’s worries.
Who’s most at risk: Anyone with generalized anxiety disorder, PTSD, or chronic stress exposure. Women are statistically more likely to experience nocturnal anxiety than men.
First action: Distinguish nocturnal panic from sleep apnea (both can involve gasping and heart racing — but the cause differs fundamentally). CBT-I and trauma-informed therapy are first-line treatments. Learn more about how to reduce anxiety naturally as a first step.
5. Depression & Mood Disorders
What happens: Early morning awakening — waking between 3am and 5am and being unable to return to sleep — is a classic and highly specific diagnostic criterion for major depressive disorder (MDD). Depression disrupts serotonin and norepinephrine signalling, which directly fragments REM sleep architecture.
What you feel: Wide awake with no obvious cause, pervasive low mood, hopelessness, difficulty finding motivation to get up. Unlike anxiety waking, this awakening is quieter — no racing heart, just a flat, heavy wakefulness.
Who’s most at risk: Anyone with a history of depression or mood disorder. Sleep disruption and depression have a bidirectional relationship — each worsens the other.
First action: Do not dismiss persistent early morning waking as “just insomnia.” Discuss it explicitly with your doctor as a possible mood disorder symptom. Review our comprehensive depression guide for a full picture of what to watch for.
6. GERD / Acid Reflux
What happens: Stomach acid production follows a circadian rhythm, peaking in the early morning hours. After hours of lying flat, acid migrates up into the esophagus — causing a burning sensation, cough, or chest tightness that breaks through sleep right around 3am.
What you feel: Chest burning or pressure, sour taste in the mouth, chronic nighttime cough, throat irritation.
Who’s most at risk: People who eat dinner late, those who drink alcohol in the evening, people with obesity or hiatus hernia, anyone who lies flat immediately after eating.
First action: Elevate the head of your bed 15–20cm (a wedge pillow works). Avoid meals within 3 hours of sleep. Discuss proton pump inhibitor (PPI) review with your doctor.
7. Nocturia (Nighttime Urination)
What happens: Nocturia — the medical term for waking two or more times nightly to urinate — affects roughly 1 in 3 adults over age 30 in the United States. As people age, the body produces less vasopressin (the hormone that concentrates urine at night), so bladder fill rate accelerates. The urge reaches threshold right around 3am in people who go to bed at 10–11pm.
What you feel: Strong, urgent need to urinate that wakes you completely. This is distinct from simply going once — two or more trips constitutes clinically relevant nocturia.
Who’s most at risk: Men over 50 (prostate enlargement), women with pelvic floor changes, pregnant women, people with diabetes or heart failure (fluid redistribution), anyone drinking excessive fluids within 3 hours of bed.
First action: Conduct a fluid timing audit — reduce intake after 6pm. Track bathroom trips for one week and bring the data to your GP.
8. Medications That Disrupt Sleep Architecture
What happens: A surprising number of common prescription medications alter sleep stage structure — suppressing deep sleep, activating the nervous system at night, or directly triggering waking at specific points in the night.
Key offenders:
| Medication Class | Examples | Sleep Effect |
|---|---|---|
| Beta-blockers | Metoprolol, Atenolol | Suppress melatonin, cause vivid dreams |
| SSRIs/SNRIs | Sertraline, Venlafaxine | Suppress REM, cause early waking |
| Corticosteroids | Prednisone, Dexamethasone | Elevate cortisol, disrupt sleep cycle |
| Decongestants | Pseudoephedrine | Stimulant effect lasting 6–8 hours |
| Some antihistamines | Long-acting types | Rebound waking after initial sedation |
First action: Never stop prescribed medication without medical advice. Instead, ask your prescriber about timing adjustments — taking some medications in the morning rather than at night can resolve sleep disruption entirely. Use our Pill Identifier to review your current medications before your next GP appointment.
9. Menopause & Hormonal Shifts
What happens: Declining estrogen and progesterone during perimenopause and menopause directly alter thermoregulation and sleep architecture. Hot flashes and night sweats — triggered by falling estrogen — cluster in the early morning hours, causing repeated waking around 3am. Post-menopausal women also have significantly increased rates of obstructive sleep apnea.
What you feel: Sudden heat surge, sweating, heart racing, then feeling cold — repeated multiple times per night.
Who’s most at risk: Women aged 45–60, though perimenopause can begin in the late 30s. Harvard Health confirms that women over 55 are disproportionately affected by 3am wake-ups due to precisely these hormonal mechanisms.
First action: Discuss hormone replacement therapy (HRT) evaluation with your doctor. Lifestyle measures including avoiding alcohol and late meals, maintaining a cool bedroom, and regular aerobic exercise can reduce hot flash frequency significantly.
Master Diagnostic Quick-Reference Table
| Medical Cause | Primary 3am Symptom | Highest Risk Group | First Step |
|---|---|---|---|
| Cortisol / HPA Axis | Racing mind, mental alertness | High-stress adults | CBT-I + cortisol panel |
| Sleep Apnea | Gasping, dry mouth, headache | Men 40+, obese adults | Sleep study |
| Hypoglycemia | Sweating, hunger, heart racing | Diabetic / insulin resistant | CGM + diet review |
| Anxiety | Dread, pounding heart | Any age, especially women | CBT-I + GP referral |
| Depression | Quiet wakefulness, low mood | Adults with mood history | Mental health evaluation |
| GERD | Chest burning, acid taste | Late eaters, drinkers | Bed elevation + PPI |
| Nocturia | Urgent need to urinate | Men 50+, pregnant women | Fluid timing audit |
| Medications | Timing-linked waking | All prescription users | Medication review |
| Menopause | Hot flash, night sweat | Women 45–60 | Hormone evaluation |

Red Flag Symptoms — When 3am Wake-Ups Need Urgent Attention
Most 3am wake-ups are not dangerous. But certain symptom combinations require immediate or urgent medical evaluation. Do not wait on these.
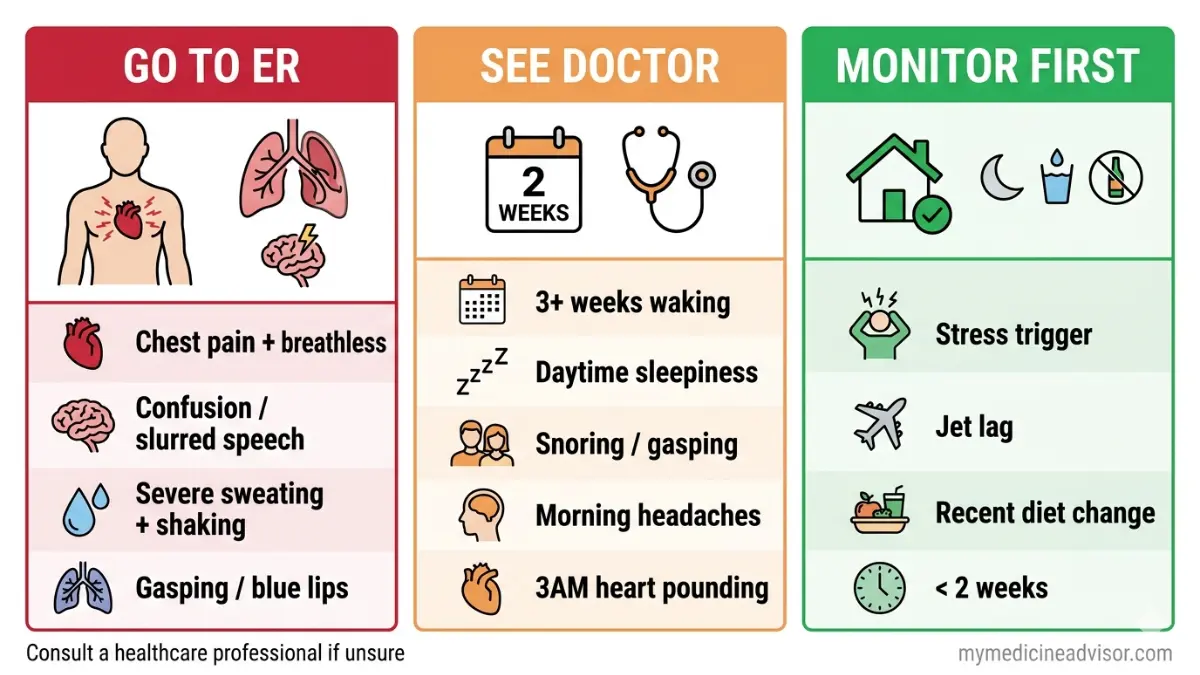
🔴 Go to the Emergency Room or Call 911 Immediately If You Wake With:
- Chest pain or pressure combined with shortness of breath (possible cardiac event)
- Sudden severe confusion, inability to speak clearly, or facial drooping (stroke symptoms)
- Severe sweating + confusion + shaking that doesn’t resolve after eating (severe hypoglycemia)
- Gasping for air with blue lips or fingertips (acute respiratory emergency)
🟡 See Your Doctor Within 2 Weeks If:
- You have woken at the same time nightly for 3 or more consecutive weeks
- Your bed partner reports loud snoring, gasping, or witnessed breathing pauses
- You experience excessive daytime sleepiness that impairs driving, work, or concentration
- You have morning headaches most days on waking
- Your 3am waking comes with heart pounding and sweating consistently
🟢 Self-Manage First (Monitor for 2 Weeks) If:
- Wake-ups started during a clearly identifiable stressful period and are lessening
- You had recent travel, jet lag, or schedule disruption and waking has been less than 2 weeks
- Dietary or alcohol change closely preceded the onset
What This Means For You: The pattern and accompanying symptoms tell your doctor far more than the time alone. Before your appointment, keep a two-week sleep diary noting: time of waking, what woke you (sound, sensation, urge), how long it took to return to sleep, and how you felt in the morning. The NHLBI recommends bringing exactly this kind of sleep diary to your first consultation.
How to Stop Waking Up at 3am — A Cause-by-Cause Fix Plan
Generic sleep hygiene advice will not fix sleep apnea. Cutting caffeine will not fix nocturnal hypoglycemia. The most important principle in treating 3am wake-ups is: match the intervention to the specific medical cause.
Fix by Medical Cause — Targeted Interventions
Sleep Apnea:
- CPAP therapy eliminates breathing-related arousals in most patients within 2–4 weeks of consistent use
- Weight management reduces airway obstruction severity — calculate your healthy weight range using our BMI Calculator
- Positional therapy (sleeping on your side) reduces event frequency by up to 50% in positional OSA
GERD:
- Elevate the head of your bed by 15–20cm using a wedge pillow — not just an extra pillow
- Finish all meals at least 3 hours before bedtime
- Avoid alcohol, fatty foods, and chocolate in the evening
- Discuss PPI medication timing with your prescriber
Anxiety / HPA Axis Dysregulation:
- Cognitive behavioral therapy for insomnia (CBT-I) has a 71% success rate for eliminating consistent early morning awakenings, according to a 2023 Sleep Medicine study
- Morning bright light exposure (10–30 minutes outdoors within 30 minutes of waking) re-anchors the cortisol rhythm
- Avoid caffeine within 6 hours of bedtime — a randomized controlled trial demonstrated 54% fewer second-half awakenings with this cutoff observed consistently
Nocturnal Hypoglycemia:
- Eat a small protein-rich snack (handful of nuts, hard-boiled egg) around 9pm if prone to overnight glucose crashes
- Reduce refined carbohydrates at dinner — large carb loads trigger the blood sugar spike-and-crash cycle that peaks at 3am
- If you use insulin, discuss dose timing with your endocrinologist
Menopause:
- Keep bedroom temperature at 16–18°C (60–65°F) — cooler than most people keep their rooms
- Lightweight, moisture-wicking bedding reduces hot flash disruption
- Discuss HRT options with your gynecologist — estrogen therapy significantly reduces nocturnal hot flash frequency
- Regular aerobic exercise reduces hot flash frequency by up to 55% in peer-reviewed trials
Nocturia:
- Restrict fluid intake after 6pm — your kidneys need approximately 3 hours to process excess fluid
- Avoid alcohol within 3 hours of bed — it suppresses vasopressin, dramatically increasing urine production overnight
- Elevate your legs for 30–60 minutes in the early evening to reduce nighttime fluid redistribution
Universal Evidence-Based Sleep Habits (2026 Updated)
These habits reduce 3am waking risk regardless of the specific cause:
- 15-minute anchor sleep rule: Go to bed and wake up within a 15-minute window every day — including weekends. This stabilizes circadian timing and reduces sleep maintenance insomnia in more than 80% of patients who apply it consistently.
- Cut alcohol and caffeine at least 6 hours before bed. A randomised controlled trial confirmed 54% fewer second-half awakenings (the 2–6am window) when this cutoff was observed.
- No screen or clock-checking at 3am. Even checking the time activates your sympathetic nervous system enough to prevent return to sleep in many people.
- The 20-minute rule: If you have been awake for more than 20 minutes, get out of bed. Lie still in low light doing a calming activity (audiobook, breathing exercise) until you feel genuinely sleepy — then return to bed. Lying frustrated in bed trains your brain to associate the bed with wakefulness.
- Bedroom temperature: Keep it between 16–19°C (60–67°F). Core body temperature must drop by approximately 1–2°C to initiate and maintain sleep — a warm bedroom actively prevents this.
Use our free Sleep Calculator to identify your optimal bedtime and wake time based on your specific sleep cycle needs.
The CDC’s About Sleep page reinforces that consistent bedtime and wake times are among the highest-evidence interventions for improving sleep continuity in adults.
Should You Get a Sleep Study? The Diagnostic Roadmap
If your 3am wake-ups persist beyond 3–4 weeks, or if any red-flag symptoms are present, objective testing moves you from guessing to knowing.
The Tests Available to You
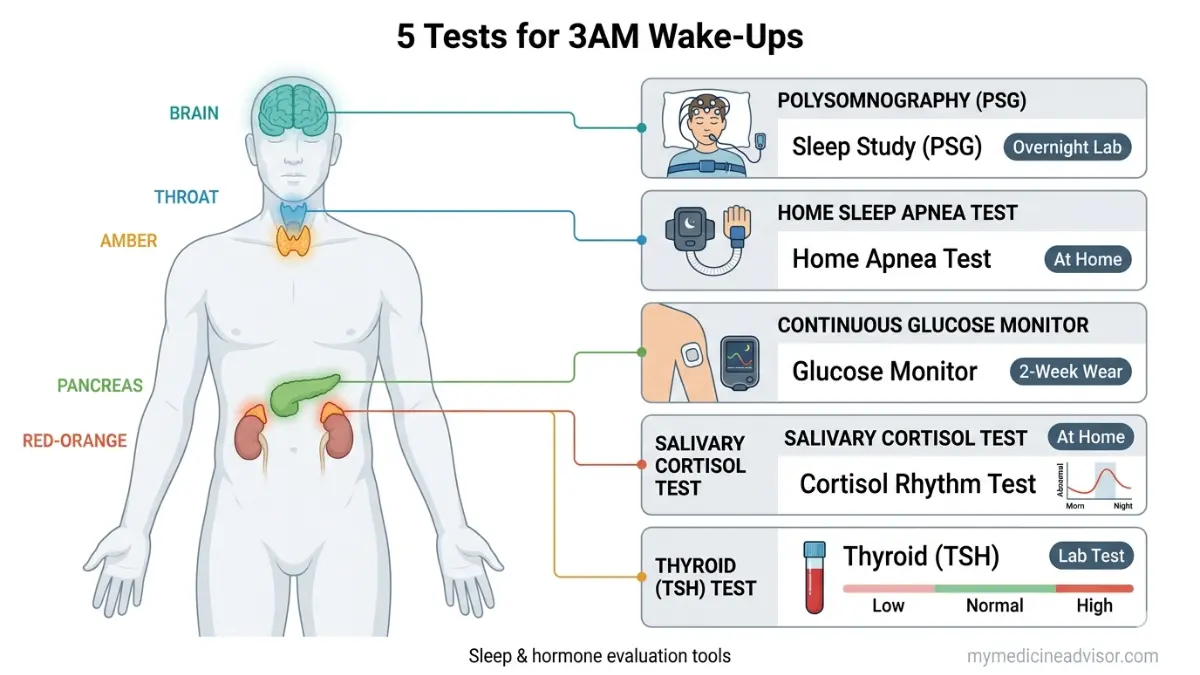
Polysomnography (PSG) — Full Sleep Study The gold standard. Conducted in a sleep lab overnight, it measures brain waves (EEG), blood oxygen levels, heart rate, breathing, and limb movement simultaneously. Required for diagnosing complex sleep disorders, REM sleep behaviour disorder, and central sleep apnea.
Home Sleep Apnea Test (HSAT) A portable device you wear overnight at home. Measures breathing patterns, oxygen saturation, and pulse. Appropriate for moderate-to-high probability obstructive sleep apnea. Far more accessible and lower cost than in-lab PSG. Most US insurers cover this when ordered by a physician.
Continuous Glucose Monitor (CGM) Worn as a small patch on the arm, a CGM measures blood glucose every few minutes throughout the night. It captures the overnight glucose patterns — including the 3am crash — that standard fasting blood tests completely miss.
4-Point Salivary Cortisol Panel Saliva samples taken at four points across the day (morning, noon, evening, midnight) map your full HPA axis rhythm. An elevated midnight cortisol with a premature morning rise is a direct biomarker of the cortisol-driven 3am wake-up pattern. Your GP or an endocrinologist can order this.
Thyroid Function Test (TSH) Hypothyroidism worsens sleep apnea severity, disrupts temperature regulation, and alters sleep architecture. It is a simple GP-ordered blood test and worth ruling out — especially in women over 40 and anyone with unexplained weight changes or fatigue.
If you have a family history of sleep apnea or metabolic disorders, our Genetic Risk Assessment Tool can help you understand your inherited risk factors before your first consultation.
When to Request What — Quick Decision Guide
| Your Primary Symptom | Recommended First Test |
|---|---|
| Gasping / snoring / daytime sleepiness | Home Sleep Apnea Test (HSAT) |
| Sweating / racing heart / shaking at 3am | Fasting glucose + CGM trial |
| Racing mind / anxiety / burnout | Salivary cortisol panel |
| Quiet waking / low mood / hopelessness | GP mental health screening |
| Frequent urination | Urine analysis + PSA (men) |
| Hot flashes / night sweats | Hormonal panel (FSH, estradiol) |
| Morning headaches / always tired | Full PSG sleep study |
What Patients and Specialists Say
Patient Vignette 1 — The Cortisol Case Rachel, 39, a healthcare administrator from Texas, woke at 3:07am every night for four months. No snoring, no sweating — just total mental alertness. A 4-point salivary cortisol test revealed her midnight cortisol was nearly double the normal upper range. Six weeks of CBT-I plus morning light therapy resolved 90% of her wake-ups.
Patient Vignette 2 — The Apnea Case James, 52, from Ohio, assumed his 3am wake-ups were stress-related. His wife had been nudging him about his snoring for years. A home sleep apnea test revealed 34 apnea events per hour during REM sleep. Three weeks on CPAP, and his 3am wake-ups disappeared entirely.
Patient Vignette 3 — The Glucose Case Priya, 47, from California, woke drenched in sweat at 3am with a pounding heart. Her fasting blood sugar was “normal” at every check. A two-week CGM revealed consistent glucose crashes to 62 mg/dL between 2:30am and 4am. Adjusting her evening meal composition eliminated the problem in 10 days.
Expert Panel Consensus — mymedicineadvisor.com Medical Advisory Board
“The 3am wake-up is one of the most common complaints I see in practice, and it almost always has a traceable medical cause. The mistake patients make is treating the symptom — taking a sleeping pill — rather than identifying the underlying driver.” — Dr. Omar Hassan, MD, Internal Medicine
“Nocturnal hypoglycemia is dramatically under-recognized as a cause of middle-of-the-night waking, even in non-diabetic patients with insulin resistance. A CGM tells you in two weeks what years of fasting labs never will.” — Dr. Vikram Nair, MD, Endocrinology
“Waking at 3am every night is your body sending a consistent signal. The circadian rhythm disruption causing it is almost always reversible once the medical cause is identified and addressed directly.” — Dr. Aditi Menon, MD, General Practice & Sleep Health
Bottom Line: Waking up at 3am every night is not a mystery and it is not something you have to accept. The circadian rhythm mechanisms driving this pattern are well understood, the medical causes are identifiable, and the solutions are evidence-based. Start by identifying your symptom pattern, use the triage framework above, and see your doctor with specific, documented information — not just “I can’t sleep.”
If you’re also experiencing unexplained fatigue during the day, our in-depth guide on always feeling tired no matter how much sleep you get covers the overlap between sleep disruption and daytime exhaustion in full detail.
For a deeper look at the warning signs that your sleep problem may have crossed into a clinical sleep disorder, read our guide on warning signs of a sleep disorder.
⚠️ Medical Disclaimer: This article is for educational purposes only and does not constitute medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional for any sleep concerns, particularly if symptoms include chest pain, gasping, or persistent daytime impairment.
FAQs: Waking Up at 3am Every Night
Q1. Why do I wake up at exactly 3am every night?
Your body’s cortisol begins rising around 2–3am as part of its natural wake-preparation cycle, coinciding with your lightest REM sleep stage after 4–5 sleep cycles. This biological convergence makes 3am the highest-vulnerability point for any underlying medical trigger to break through.
Q2. What is the most common medical cause of waking up at 3am?
The most common identifiable medical causes are HPA axis cortisol dysregulation, obstructive sleep apnea, and nocturnal hypoglycemia — with anxiety and GERD close behind. Often more than one cause is present simultaneously.
Q3. Is waking up at 3am every night a sign of sleep apnea?
It can be. Sleep apnea events cluster heavily in the 2–6am REM-dominant window. If you wake gasping, with a morning headache, dry mouth, or your partner reports snoring — request a home sleep apnea test from your doctor.
Q4. Can anxiety cause you to wake at 3am every night?
Yes. Anxiety chronically elevates cortisol and creates a hyperarousal state that makes the natural 3am cortisol surge significantly stronger, pushing it past the threshold for waking. Anxiety is one of the most treatable causes of sleep maintenance insomnia.
Q5. Can blood sugar dropping cause a 3am wake-up?
Yes. Nocturnal hypoglycemia triggers a counter-regulatory hormonal response — adrenaline, cortisol, and glucagon — that physically jolts you awake. This is particularly common in insulin resistance, diabetes, and after high-carbohydrate or alcohol-heavy evening meals.
Q6. What does waking at 3am every night mean for long-term health?
Chronic sleep fragmentation increases cardiovascular risk, raises cortisol chronically, impairs immune function, and worsens metabolic markers. The NHLBI confirms that adults who regularly fail to achieve uninterrupted sleep face significantly elevated risks for heart disease, hypertension, and diabetes.
Q7. What should I do immediately when I wake up at 3am?
Do not check your phone or the clock. Lie still in the dark and practise slow diaphragmatic breathing (4 counts in, 6 counts out). If you are fully awake after 20 minutes, get up and do a calm, non-stimulating activity in low light until you feel sleepy again.
Q8. Which medications commonly cause 3am wake-ups?
Beta-blockers (suppress melatonin), SSRIs and SNRIs (fragment REM sleep), corticosteroids (directly elevate cortisol), decongestants containing pseudoephedrine, and some long-acting antihistamines. Timing adjustments — rather than stopping medication — often resolve this.
Q9. Why do women wake up at 3am more often than men?
Women are more susceptible due to hormonal influences (estrogen and progesterone changes during perimenopause and menopause), higher rates of anxiety and depression, and greater sleep reactivity. Post-menopausal women also have increased sleep apnea risk that is frequently under-diagnosed.
Q10. How long does it take to fix 3am wake-ups?
With the correct targeted intervention, most people see significant improvement within 2–6 weeks. CBT-I shows a 71% resolution rate at 6 weeks. CPAP therapy for sleep apnea typically delivers results within 2–3 weeks of consistent use. Lifestyle-driven causes (diet, alcohol, fluid timing) can improve within days.
Q11. When should I see a doctor about waking at 3am?
See your doctor if wake-ups occur 3 or more nights per week for 3 or more consecutive weeks, if daytime function is impaired, or if any red-flag symptom is present (gasping, chest pain, morning headaches, sweating with confusion). Do not wait — most causes are readily treatable once identified.
Explore more at mymedicineadvisor.com/health/ — your trusted source for evidence-based health information reviewed by internationally credentialed medical experts.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.