On This Page – Quick Medical Summary
Nicholas, a 42-year-old accountant from Chicago, had been exhausted for four years straight. He blamed work deadlines. His doctor blamed stress. Then a sleep study revealed he was stopping breathing 47 times per hour in his sleep — severe obstructive sleep apnea, completely undiagnosed.
His story is not rare. It is the norm.
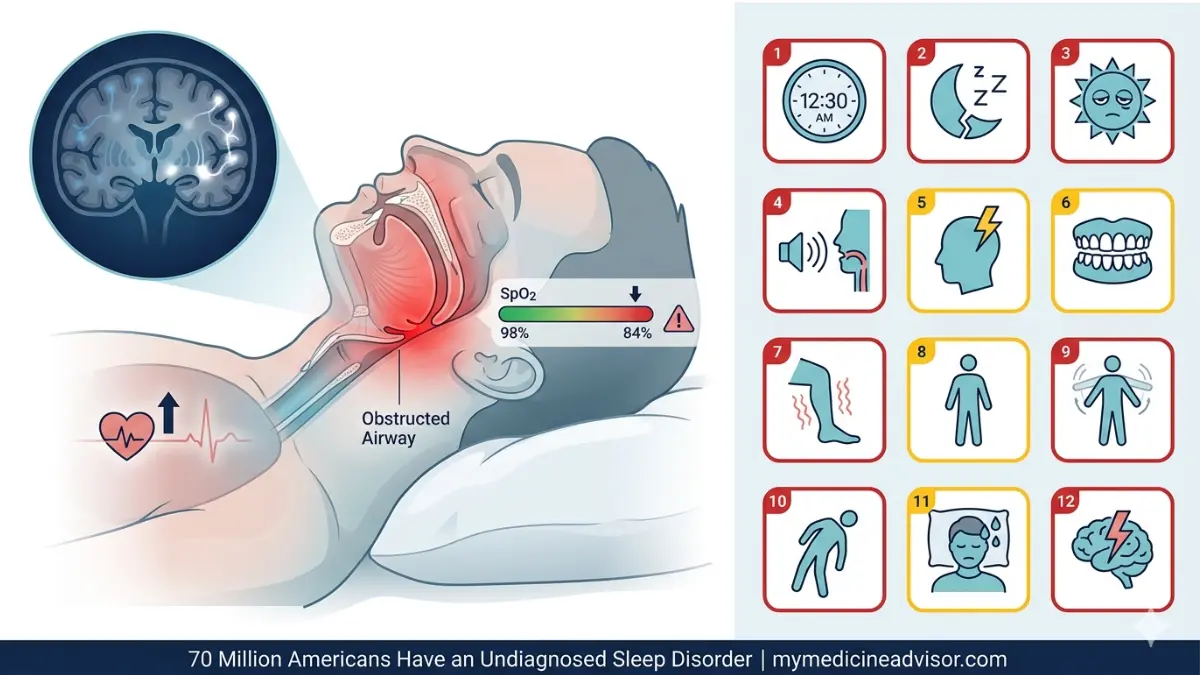
Over 70 million Americans currently live with a sleep disorder — and according to the National Heart, Lung, and Blood Institute (NHLBI), a staggering 90% of sleep apnea cases remain undiagnosed. If you regularly wake up tired, feel mentally foggy, or suspect your sleep is broken — this article may be the most important thing you read today.
Use our free Sleep Calculator to find out if you’re getting enough sleep for your age and lifestyle.
⚠️ Disclaimer: This article is for educational purposes only and does not constitute medical advice. Always consult a qualified healthcare professional for diagnosis and treatment of any sleep disorder.
What Is a Sleep Disorder — And Why Most Go Undiagnosed
More Than Just “Bad Sleep”
A sleep disorder is not the occasional rough night after a stressful day. It is a persistent, clinically significant disruption to the quality, timing, or duration of sleep that impairs your daily functioning — physically, cognitively, or emotionally.
There are over 80 recognized types of sleep disorders, according to the American Academy of Sleep Medicine. The most common include insomnia, obstructive sleep apnea (OSA), restless legs syndrome (RLS), narcolepsy, and REM sleep behavior disorder.
Why Do So Many Cases Go Undiagnosed?
The answer is both alarming and preventable. According to the CDC’s sleep health data, over 60% of adults have never been asked about the quality of their sleep by a physician. Most people normalize their symptoms — assuming tiredness is just “life.”
The consequences of ignoring a sleep disorder are severe:
- Increased risk of heart disease, stroke, and type 2 diabetes
- 3x higher risk of motor vehicle accidents due to excessive daytime sleepiness
- Accelerated cognitive decline — a 2024 NHLBI-funded study in Neurology found adults with disrupted sleep in their 30s and 40s showed significantly worse cognitive test scores a decade later
- Weakened immune function and elevated inflammation markers
Gender Makes a Difference
- Women are 40% more likely to develop insomnia than men
- Men are far more likely to have undiagnosed obstructive sleep apnea — yet women’s OSA is consistently underdiagnosed because their symptoms present differently (fatigue and headaches rather than loud snoring)
Quick comparison:
| Normal Sleep Disruption | Sleep Disorder Warning Sign |
|---|---|
| Trouble sleeping during a stressful week | Can’t fall asleep for 30+ minutes most nights |
| Waking once to use the bathroom | Waking 3–5 times and unable to return to sleep |
| Feeling tired after a late night | Falling asleep involuntarily during the day |
| Occasional vivid dreams | Physically acting out dreams while asleep |
Understanding your sleep stages and how disruptions affect each stage is the first step toward identifying whether your symptoms are clinical.
Warning Signs 1–4 — The “Obvious” Symptoms Most People Dismiss
Warning Sign #1: You Take More Than 30 Minutes to Fall Asleep — Almost Every Night
Possible disorder: Insomnia disorder, anxiety-related sleep disruption Urgency: 🔴 High
Lying awake for 30+ minutes at bedtime more than three nights per week for at least three months meets the clinical diagnostic threshold for insomnia disorder, according to the American Psychiatric Association.
This is not just frustrating — it is medically significant. Chronic insomnia affects an estimated 10–15% of U.S. adults and is strongly associated with depression, anxiety, and cardiovascular disease.
What This Means For You: If this has been happening for more than a month, it is time to track it in a sleep diary and speak to your doctor. This is not a lifestyle issue — it may be a diagnosable condition.
Warning Sign #2: You Wake Up Multiple Times Per Night and Struggle to Fall Back Asleep
Possible disorder: Insomnia, sleep apnea (micro-arousals), circadian rhythm disorder Urgency: 🔴 High
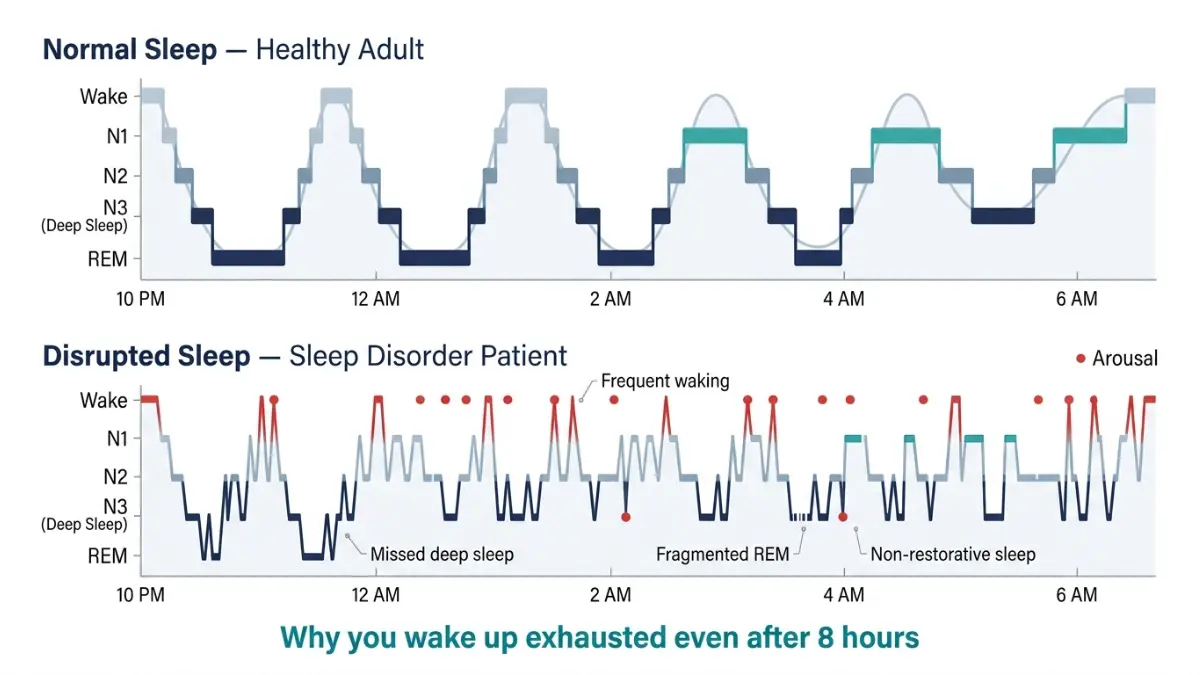
Waking frequently and lying awake for prolonged periods is called sleep fragmentation. It prevents you from completing the deep restorative sleep cycles your body requires.
Many people with obstructive sleep apnea don’t remember waking — their brain briefly rouses them to restart breathing, sometimes hundreds of times per night, without conscious awareness.
What This Means For You: If your bed partner reports restless movement or you consistently wake feeling unrested despite “sleeping 7 hours,” fragmented sleep — not duration — may be the problem. Learn more about how circadian rhythm disruptions can drive nighttime waking.
Warning Sign #3: Excessive Daytime Sleepiness — Even After a Full Night of Sleep
Possible disorder: Obstructive sleep apnea, narcolepsy, idiopathic hypersomnia Urgency: 🔴 High
This is one of the most misattributed sleep disorder symptoms in America. Patients blame their diet, age, or workload — when the real cause is non-restorative sleep from an underlying disorder.
Clinically, excessive daytime sleepiness (EDS) is defined as an inability to maintain wakefulness or alertness during the day, despite adequate opportunity for nighttime sleep. The American Academy of Sleep Medicine estimates EDS affects up to 20% of the U.S. population.
Key red flags for EDS:
- Falling asleep within 5 minutes of sitting quietly
- Nodding off during conversations, meetings, or while driving
- Requiring multiple cups of coffee just to function before noon
What This Means For You: EDS is the #1 symptom of undiagnosed sleep apnea and narcolepsy. It is not laziness. It is a medical signal.
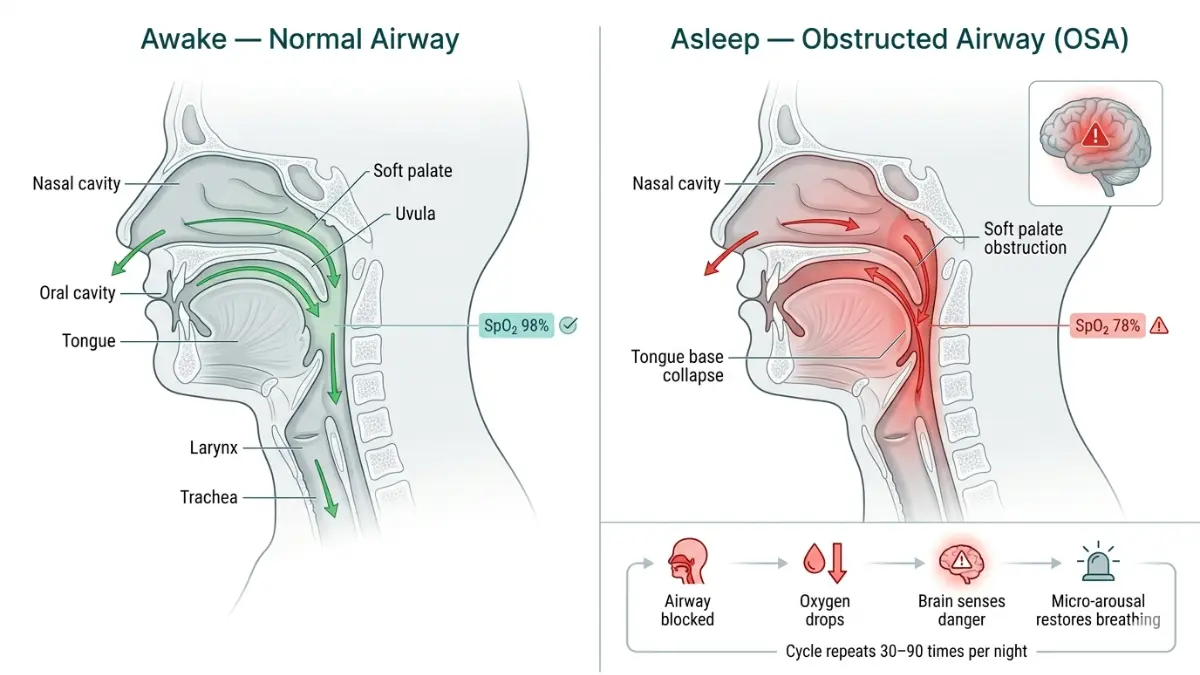
Warning Sign #4: Loud Snoring, Gasping, or Choking Sounds During Sleep
Possible disorder: Obstructive sleep apnea (OSA) Urgency: 🔴 Critical
This is the most well-known — and most ignored — warning sign of a sleep disorder. Nearly 70% of people who snore habitually have OSA, according to sleep medicine data.
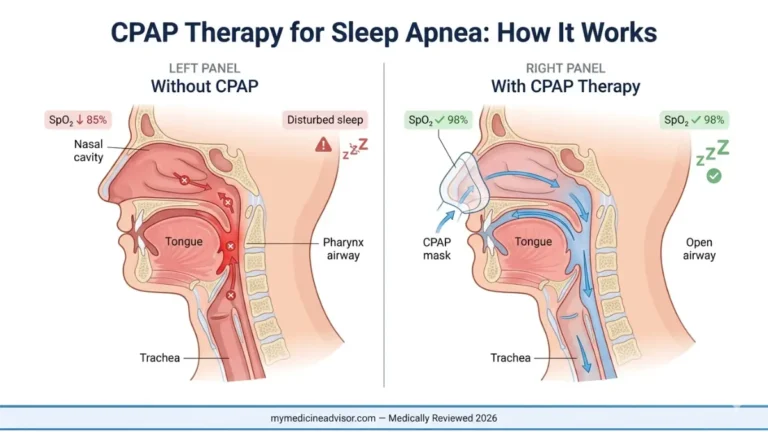
Obstructive sleep apnea occurs when throat muscles relax and block the airway. The brain detects oxygen deprivation and triggers a micro-arousal to restart breathing — producing the characteristic gasp or snort. This can happen 30 to 90+ times per hour in severe cases.
Critical 2026 data: OSA is now linked to a 2–3x increased risk of atrial fibrillation (AFib) and significantly elevated stroke risk. Undiagnosed OSA costs the U.S. an estimated $150 billion annually in healthcare costs and lost productivity, per the NHLBI.
What This Means For You: If your bed partner has ever said you stop breathing in your sleep, this is a medical emergency. Request a sleep study referral immediately.
Warning Signs 5–8 — The Subtle Signs Your Doctor Might Be Missing
These four warning signs appear in none of the top 3 ranking articles on this topic. This is where most people with a sleep disorder fall through the cracks.
Warning Sign #5: You Wake Up With a Headache Almost Every Morning
Possible disorder: Obstructive sleep apnea (nocturnal hypoxia), sleep bruxism Urgency: 🟡 Moderate–High
Morning headaches are one of the most underrecognized signs of sleep apnea in clinical practice. When breathing repeatedly stops during sleep, blood oxygen levels drop — a state called nocturnal hypoxia. This causes cerebral blood vessels to dilate, triggering a dull, pressing headache that typically resolves within 30 minutes of waking.
Studies show that 36–58% of OSA patients report morning headaches, yet the majority are initially treated for migraines or tension headaches — never screened for sleep disorders.
What This Means For You: If your headaches are worse in the morning than at any other time of day and you also snore or feel unrefreshed on waking, tell your doctor specifically about the morning timing. This detail changes the clinical picture entirely.
Warning Sign #6: You Grind or Clench Your Teeth During Sleep (Bruxism)
Possible disorder: Sleep bruxism, obstructive sleep apnea, stress-related sleep disorder Urgency: 🟡 Moderate
Sleep bruxism — the grinding or clenching of teeth during sleep — affects 8–10% of U.S. adults and is the leading cause of dental wear in people under 50. Most people discover it when their dentist mentions unusual enamel erosion, not because they notice symptoms themselves.
What makes this critical: multiple peer-reviewed studies have now confirmed a strong association between sleep bruxism and obstructive sleep apnea. The leading theory is that teeth grinding is a compensatory arousal mechanism — the jaw clenches reflexively to re-open an obstructed airway.
Signs you may have sleep bruxism:
- Sore jaw or facial muscles on waking
- Dull headache at the temples in the morning
- Chipped, cracked, or flattened teeth
- Your dentist has mentioned unusual wear
What This Means For You: If your dentist recommends a night guard, also ask your doctor about a sleep disorder screening. These two conditions are frequently co-occurring and both need treatment.
Warning Sign #7: Crawling, Tingling, or Creeping Sensations in Your Legs at Night
Possible disorder: Restless Legs Syndrome (RLS), periodic limb movement disorder (PLMD) Urgency: 🔴 High
Restless Legs Syndrome is a neurological sleep disorder characterized by an irresistible urge to move the legs, typically triggered by rest or inactivity in the evening. The sensations are often described as crawling, pulling, throbbing, or aching — temporarily relieved only by movement.
RLS affects an estimated 5–10% of U.S. adults and is significantly more common in women. It is also strongly associated with iron deficiency, pregnancy, and kidney disease — making it both a sleep disorder and a potential marker of underlying medical conditions.
What This Means For You: RLS is not “just restlessness.” It is a diagnosable condition with effective treatments. If evening leg discomfort is consistently ruining your sleep quality, ask your doctor for an iron panel and a neurology or sleep medicine referral. Understand how REM sleep disruptions tie into conditions like RLS and PLMD.
Warning Sign #8: You Feel Temporarily Paralyzed Upon Waking or While Falling Asleep
Possible disorder: Isolated sleep paralysis, narcolepsy Urgency: 🟡 Moderate
Sleep paralysis occurs when the brain transitions into or out of REM sleep while you are semi-conscious. The result: a brief inability to move or speak, often accompanied by a vivid sense of presence, pressure on the chest, or hypnagogic hallucinations.
Isolated episodes (not associated with narcolepsy) affect approximately 7.6% of the general population at least once in their lifetime. When sleep paralysis occurs regularly — especially alongside daytime sleepiness or cataplexy — it may indicate narcolepsy.
What This Means For You: An occasional episode is not dangerous. Recurring episodes, especially with hallucinations or emotional triggers causing muscle weakness, warrant a sleep medicine consultation.
Warning Signs 9–12 — Red Flags That Demand Immediate Medical Attention
These four signs are the most serious. Some are neurological emergencies in disguise.
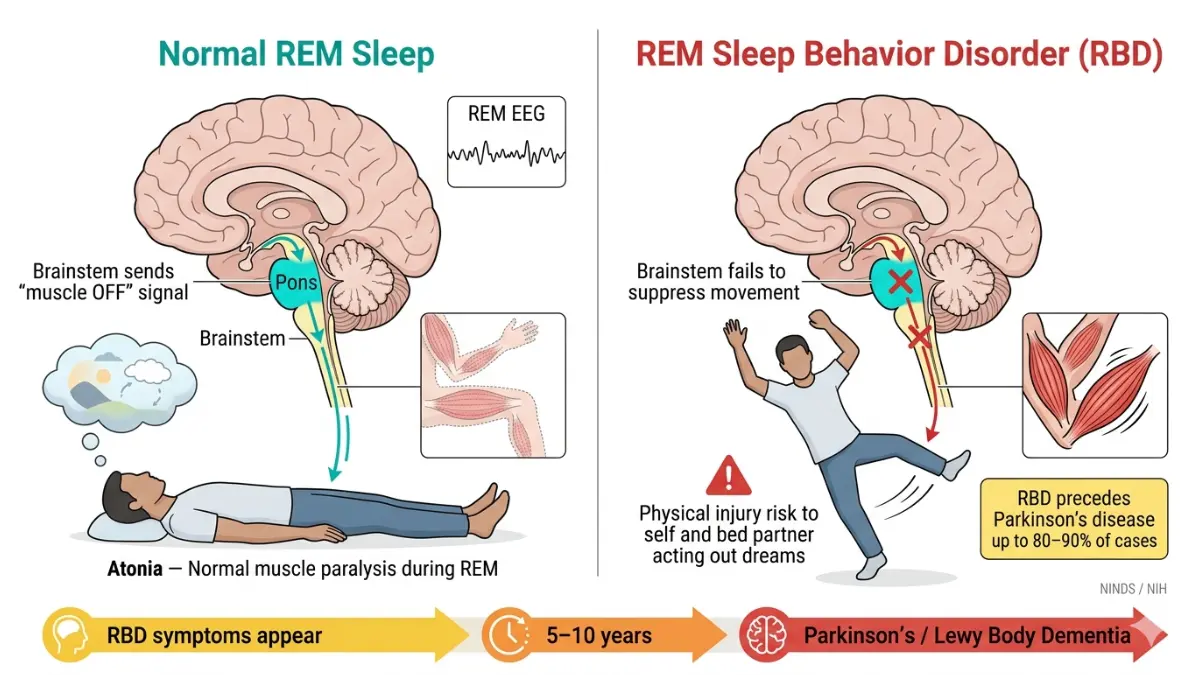
Warning Sign #9: You Physically Act Out Your Dreams During Sleep
Possible disorder: REM Sleep Behavior Disorder (RBD) Urgency: 🔴 Critical — See a Neurologist
REM Sleep Behavior Disorder is a condition where the normal muscle paralysis of REM sleep fails to occur. As a result, people physically act out their dreams — punching, kicking, shouting, or jumping out of bed — often with no memory of doing so.
This is not just disruptive. It is potentially a harbinger of serious neurological disease. According to the National Institute of Neurological Disorders and Stroke (NINDS), up to 80–90% of people with RBD eventually develop a neurodegenerative condition — most commonly Parkinson’s disease, Lewy body dementia, or multiple system atrophy — often within 10–15 years of symptom onset.
What This Means For You: This is not a quirky sleep habit. If you or your bed partner describes violent or complex movements during sleep, see a neurologist — not just a GP. Early detection matters enormously.
Warning Sign #10: You Experience Sudden Muscle Weakness Triggered by Strong Emotions
Possible disorder: Narcolepsy Type 1 (cataplexy) Urgency: 🔴 Critical
Cataplexy is the sudden, brief loss of muscle tone triggered by strong emotions — particularly laughter, surprise, or excitement. It can range from a subtle jaw drop or head nod to a complete loss of muscle control and collapse, while the person remains fully conscious.
Cataplexy is pathognomonic for narcolepsy Type 1 — meaning if you have cataplexy, you have narcolepsy. Despite this, the average delay from first symptom to diagnosis is 8–10 years in the U.S.
What This Means For You: If strong laughter or emotional reactions consistently cause your knees to buckle, your head to drop, or sudden facial weakness — this is not anxiety or clumsiness. This requires urgent neurological evaluation.
Warning Sign #11: You Wake Up Drenched in Night Sweats Not Explained by Menopause or Fever
Possible disorder: Obstructive sleep apnea, circadian rhythm disorder, sleep-related GERD Urgency: 🟡 Moderate
Unexplained night sweats — defined as soaking perspiration requiring a change of clothes or bedding — are strongly associated with undiagnosed obstructive sleep apnea in both men and women. The mechanism involves the body’s fight-or-flight response activation during repeated apnea episodes.
This warning sign is almost entirely absent from mainstream sleep disorder content — yet a 2023 study found that 30% of OSA patients reported significant night sweats as a primary complaint. For many, it was their only clearly identifiable symptom.
What This Means For You: If night sweats are unexplained by hormonal changes, infection, or medication, add this symptom explicitly to the list when speaking with your doctor. Combined with fatigue or morning headaches, it significantly raises OSA suspicion.
Warning Sign #12: Persistent Irritability, Anxiety, Depression, or Brain Fog That Won’t Lift
Possible disorder: Chronic sleep deprivation from untreated sleep disorder, comorbid insomnia and depression Urgency: 🔴 High
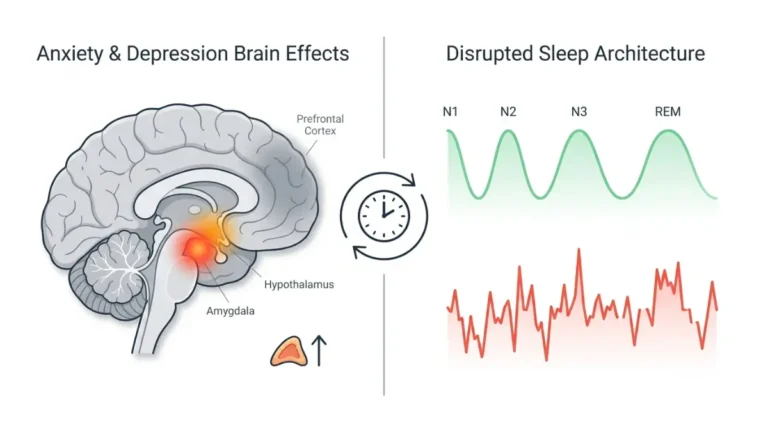
Chronic poor sleep caused by an untreated sleep disorder does not stay confined to the bedroom. It systematically erodes mental health. According to the American Psychiatric Association, 40–50% of people with chronic insomnia have a comorbid mental health disorder — most commonly depression or anxiety.
The causal arrow runs both ways: sleep disorders worsen mood disorders, and mood disorders deepen sleep problems. This cycle is one of the most common reasons people remain undiagnosed — their mental health symptoms are treated while the underlying sleep disorder continues unchecked.
2024 research note: NHLBI-funded research confirmed that adults with disrupted sleep in midlife showed markedly worse performance on cognitive function tests a decade later — underscoring the long-term brain costs of ignoring sleep disorder warning signs.
What This Means For You: If antidepressants or anxiety medication aren’t working as expected, and you also have poor sleep, raise this pattern explicitly with your psychiatrist or GP. A sleep disorder evaluation may be the missing piece.
If you’re experiencing mental health symptoms alongside these signs, you can begin a preliminary self-evaluation using our Symptom Checker.
The Complete Warning Sign–to–Diagnosis Reference Table
Which Sleep Disorder Do You Have? (2026 Master Table)
| Warning Sign | Most Likely Sleep Disorder | Urgency | Recommended Next Step |
|---|---|---|---|
| 30+ minutes to fall asleep nightly | Insomnia disorder | 🔴 High | Sleep diary + GP referral |
| Waking 3–5x per night | Insomnia / Sleep fragmentation | 🔴 High | Sleep diary, GP |
| Excessive daytime sleepiness | Sleep apnea / Narcolepsy | 🔴 High | Sleep study referral |
| Loud snoring / gasping / choking | Obstructive sleep apnea | 🔴 Critical | Urgent sleep study |
| Morning headaches on waking | Sleep apnea (nocturnal hypoxia) | 🟡 Moderate–High | Mention to GP + OSA screen |
| Teeth grinding / jaw soreness | Sleep bruxism / OSA | 🟡 Moderate | Dentist + sleep evaluation |
| Crawling leg sensations at night | Restless Legs Syndrome | 🔴 High | Iron panel + GP / neurologist |
| Sleep paralysis on waking | Narcolepsy / Isolated REM issue | 🟡 Moderate | GP consult |
| Physically acting out dreams | REM Sleep Behavior Disorder | 🔴 Critical | Neurologist — urgent |
| Sudden muscle weakness with emotion | Narcolepsy Type 1 (cataplexy) | 🔴 Critical | Neurologist — urgent |
| Unexplained drenching night sweats | Sleep apnea / Circadian disorder | 🟡 Moderate | GP + OSA screening |
| Persistent mood changes / brain fog | Chronic sleep deprivation / comorbid insomnia | 🔴 High | GP + mental health consult |
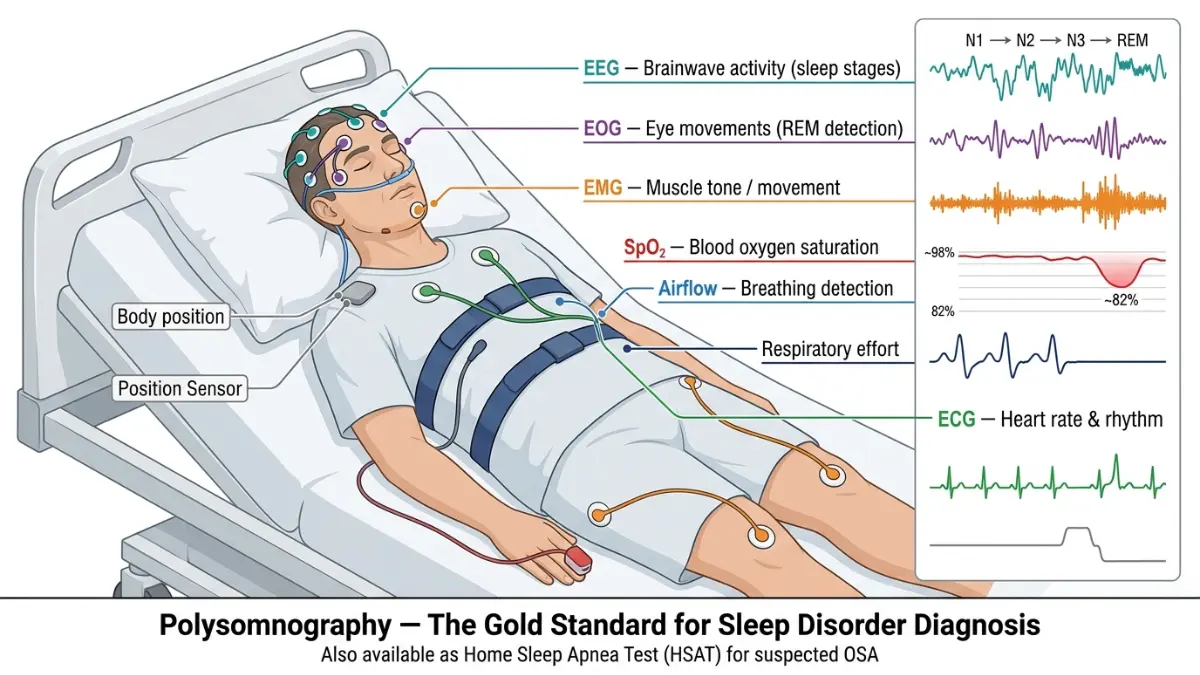
How Is a Sleep Disorder Diagnosed?
- Polysomnography (sleep study): The gold standard. Conducted in a sleep lab or via home device, it monitors brainwaves, oxygen levels, heart rate, breathing, and limb movements simultaneously.
- MSLT (Multiple Sleep Latency Test): Measures how quickly you fall asleep during five daytime nap opportunities — used to diagnose narcolepsy and idiopathic hypersomnia.
- Sleep diary: 2-week log of bedtimes, wake times, sleep quality, and daytime function — the first tool most clinicians request.
- Actigraphy: Wrist-worn sensor tracking movement patterns over days to weeks to assess sleep-wake cycles.
Important note: Obesity is one of the strongest modifiable risk factors for obstructive sleep apnea. Check your BMI Calculator to understand your risk profile. People with a BMI over 30 are significantly more likely to develop OSA.
What To Do Now — Your 5-Step Sleep Disorder Action Plan
If you recognized two or more of the warning signs above, take these steps:
Step 1: Track Your Symptoms for 2 Weeks
Start a simple sleep diary. Record:
- Bedtime and estimated time to fall asleep
- Number of times you woke during the night
- Wake time and how you felt on rising
- Afternoon energy levels (scale of 1–10)
- Any notable symptoms: headaches, leg sensations, jaw soreness
This diary is the single most useful document you can bring to a doctor’s appointment.
Step 2: Run a Preliminary Self-Check
Use our Symptom Checker to map your symptoms and generate a starting point for your GP conversation. Knowledge of your specific symptom pattern dramatically improves the quality of clinical consultations.
Step 3: See Your GP — With This Script
Many patients under-report sleep symptoms to their doctors. Be specific. Say:
“I’ve been tracking my sleep for two weeks. I have trouble [falling asleep / staying asleep / feeling rested]. I also notice [morning headaches / daytime sleepiness / leg sensations / etc.]. I’d like to discuss whether a sleep disorder evaluation or sleep study is appropriate.”
This framing is far more likely to result in a referral than simply saying “I’m tired.”
Step 4: Ask for a Sleep Study Referral If Warranted
A home sleep apnea test (HSAT) or in-lab polysomnography can definitively diagnose or rule out the most dangerous sleep disorders. Ask specifically if your symptoms warrant this — do not wait for your doctor to offer it unprompted.
Step 5: Implement Evidence-Based Sleep Hygiene While You Wait
These strategies are supported by the CDC’s sleep health guidelines:
- Fix your sleep schedule: Same bedtime and wake time every day, including weekends
- Create a wind-down routine: 30–60 minutes of low stimulation before bed (no screens)
- Optimize your sleep environment: Dark, cool (65–68°F), and quiet
- Limit alcohol: Even moderate alcohol suppresses REM sleep and worsens sleep apnea
- Address weight if applicable: Use our Weight Loss Calculator — even a 10% reduction in body weight can reduce sleep apnea severity by 30%
- Check your water intake: Dehydration disrupts sleep quality; use our Water Intake Calculator to find your daily target
Also review our in-depth guide on how many hours of sleep you need by age — the answer changes significantly across the lifespan.
Don’t wait. Sleep disorders are highly treatable — but only if you take the warning signs seriously. The difference between diagnosed and undiagnosed can be measured in decades of health outcomes.
Frequently Asked Questions About Sleep Disorders
1. What are the most common types of sleep disorders?
The five most common are insomnia, obstructive sleep apnea, restless legs syndrome, narcolepsy, and REM sleep behavior disorder. Together they account for the majority of the 70+ million diagnosed cases in the U.S.
2. How do I know if I have a sleep disorder or just stress-related poor sleep?
Stress-related poor sleep typically resolves when the stressor resolves. A sleep disorder persists regardless of life circumstances, occurs at least 3 nights per week for 3+ months, and significantly impacts your daytime functioning.
3. Can a sleep disorder go away on its own without treatment?
Rarely without intervention. Insomnia can improve with behavioral therapy (CBT-I). Sleep apnea, RLS, and narcolepsy typically require medical management and do not resolve spontaneously.
4. What is the #1 warning sign of sleep apnea specifically?
Loud, chronic snoring combined with observed breathing pauses during sleep. If your bed partner reports you stop breathing, this is the highest-urgency warning sign — request a sleep study immediately.
5. Do sleep disorders cause weight gain?
Yes. Sleep deprivation disrupts the hormones leptin and ghrelin — increasing hunger and reducing satiety signals. Untreated sleep apnea is independently associated with weight gain, insulin resistance, and type 2 diabetes.
6. Can children have sleep disorders?
Yes. Childhood sleep apnea, night terrors, sleepwalking, and RLS all occur in pediatric populations. Loud snoring in a child is never normal and warrants evaluation.
7. What does a sleep study actually involve?
A polysomnography records brainwave activity (EEG), eye movement, oxygen saturation, heart rate, breathing effort, and limb movement simultaneously during sleep. Home-based alternatives (HSAT) are now available for suspected OSA cases.
8. Is insomnia a serious sleep disorder or just a nuisance?
Insomnia disorder is clinically serious. Chronic insomnia costs the U.S. approximately $31 billion annually in workplace accidents and errors alone, and is strongly associated with depression, anxiety, hypertension, and cardiovascular disease.
9. Can anxiety cause a sleep disorder, or does the sleep disorder cause anxiety?
Both. This is one of the best-documented bidirectional relationships in sleep medicine. Anxiety disrupts sleep architecture; disrupted sleep amplifies anxiety and threat perception. Treating one without addressing the other is rarely effective long-term.
10. How many hours of sleep do adults actually need?
The American Academy of Sleep Medicine recommends 7–9 hours for adults aged 18–60. Consistently sleeping fewer than 7 hours is associated with significant health risks regardless of how rested you feel. Check our hours of sleep by age guide for age-specific guidance.
11. When should I stop Googling and actually see a doctor about my sleep?
Right now, if: you’ve had symptoms for more than one month, your daytime function is impaired, your bed partner reports gasping or breath pauses, or you recognize signs #9 or #10 from this article. These warrant same-week medical contact.
Article reviewed by the mymedicineadvisor.com Medical Expert Panel. For more health insights, visit our Health Tips hub.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.