On This Page – Quick Medical Summary
Yes — anxiety and depression are two of the most clinically proven causes of sleep problems in adults.
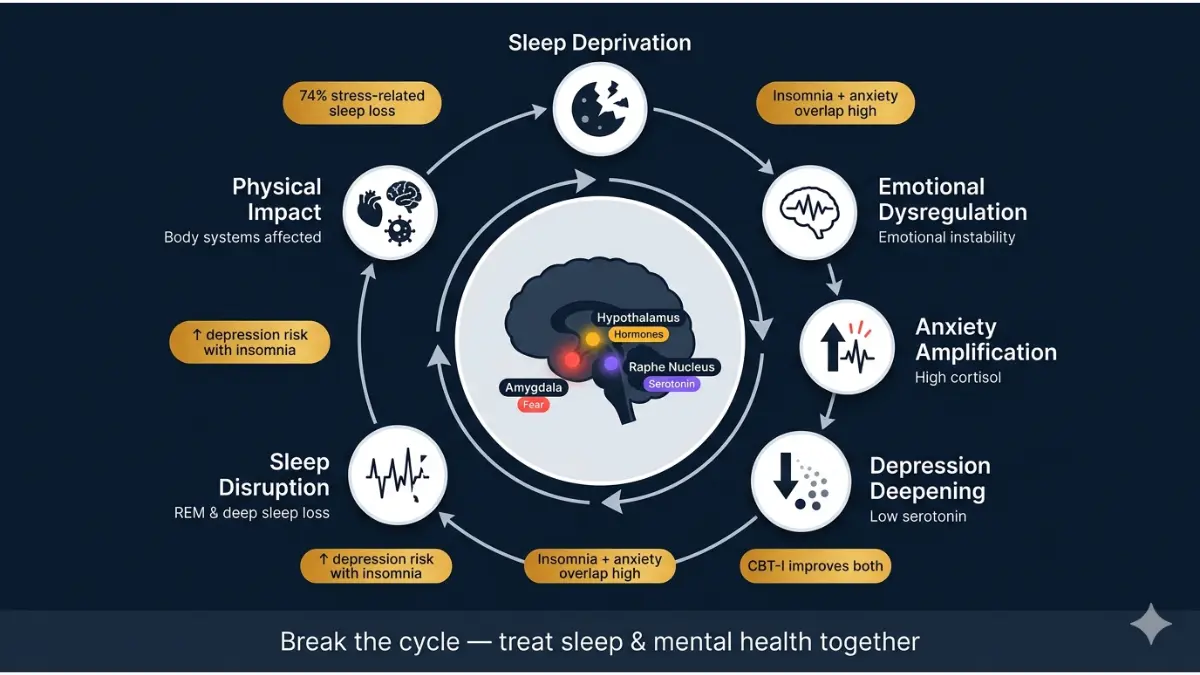
And the relationship runs both ways. Poor sleep worsens anxiety and depression. Anxiety and depression worsen sleep. This is called the bidirectional cycle — and millions of Americans are trapped inside it right now without knowing why.
According to a 2024 survey by the American Academy of Sleep Medicine (AASM), nearly 74% of Americans report disrupted sleep due to stress, 68% lose sleep specifically due to anxiety, and over 55% experience disrupted sleep from depression.
If you’re lying awake at 2am with a racing mind, exhausted but unable to switch off — this article explains exactly what is happening in your brain, and what actually fixes it.
Use our free Sleep Calculator to calculate your optimal sleep window and find out how much sleep debt you’ve built up.
How Anxiety Causes Sleep Problems — The Brain Science
The Fight-or-Flight System That Won’t Shut Off
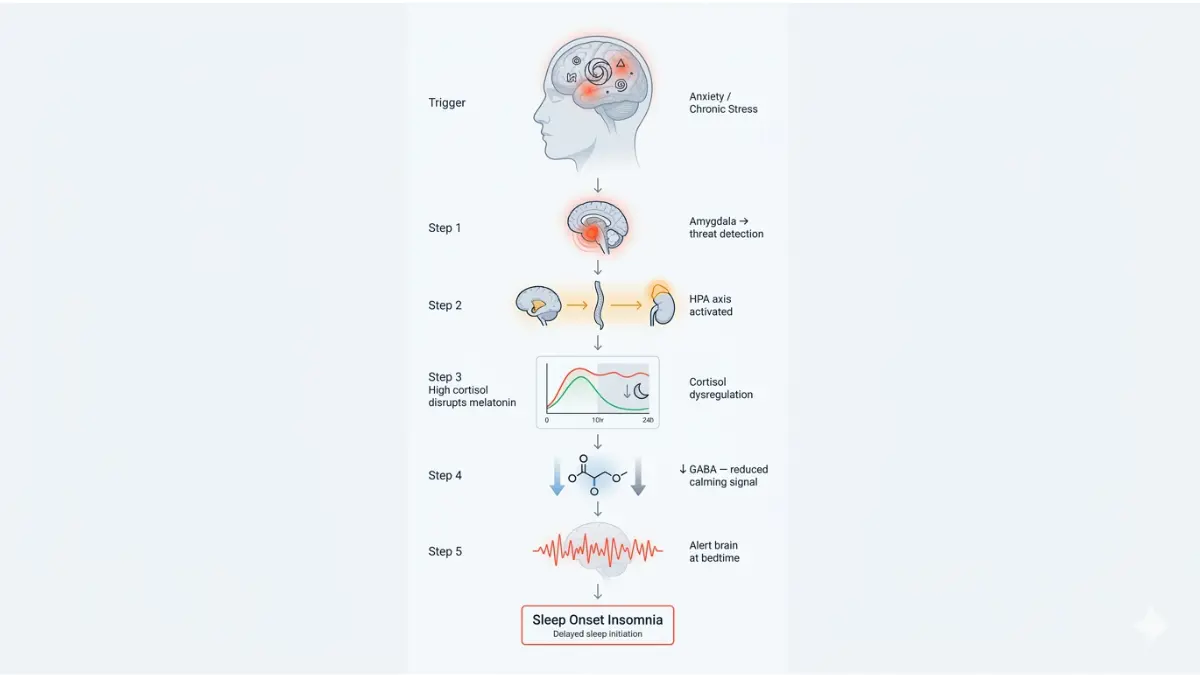
Anxiety triggers your body’s fight-or-flight response — a survival mechanism controlled by the amygdala. When you’re anxious, your brain signals the adrenal glands to release cortisol and adrenaline, hormones designed to keep you alert and ready for danger.
The problem? Your brain cannot distinguish between a real threat and a worried thought at 11pm.
The bidirectional relationship means that anxiety and sleep deprivation can be self-reinforcing — worrying causes poor sleep, while further sleep difficulties cause greater anxiety.
GABA Disruption: The Missing Sleep Chemical
Your brain uses a neurotransmitter called GABA (gamma-aminobutyric acid) to slow neural activity and allow sleep onset. Chronic anxiety dysregulates GABA pathways, meaning the brain’s natural “off switch” stops working effectively.
Research published in Frontiers in Psychiatry confirms that insomnia and anxiety share a pathogenetic mechanism — hyperarousal caused by dysregulation of neurotransmitter systems including cholinergic and GABAergic mechanisms.
This is why anxious people often describe lying in bed feeling physically exhausted but mentally “wired.”
Which Anxiety Disorders Cause the Worst Sleep Problems?
| Anxiety Disorder | Primary Sleep Problem | Severity |
|---|---|---|
| Generalized Anxiety (GAD) | Difficulty falling asleep, racing thoughts | High |
| PTSD | Nightmares, hypervigilance, frequent waking | Very High |
| Panic Disorder | Nocturnal panic attacks, fear of sleep | Severe |
| OCD | Intrusive thoughts delaying sleep onset | High |
| Social Anxiety | Pre-event rumination, early waking | Moderate |
In several studies, over 90% of people with PTSD associated with military combat have reported symptoms of insomnia.
People with insomnia are 20 times more likely to develop panic disorder compared to normal sleepers — one of the starkest statistics in sleep medicine.
What This Means For You: If you struggle to fall asleep due to a racing mind, circling worries, or a sense of dread about tomorrow — anxiety-driven hyperarousal is the likely culprit. For deeper context on what’s happening neurologically, read our guide on what adrenaline actually does to your body.
How Depression Causes Sleep Problems — And Why It’s Different
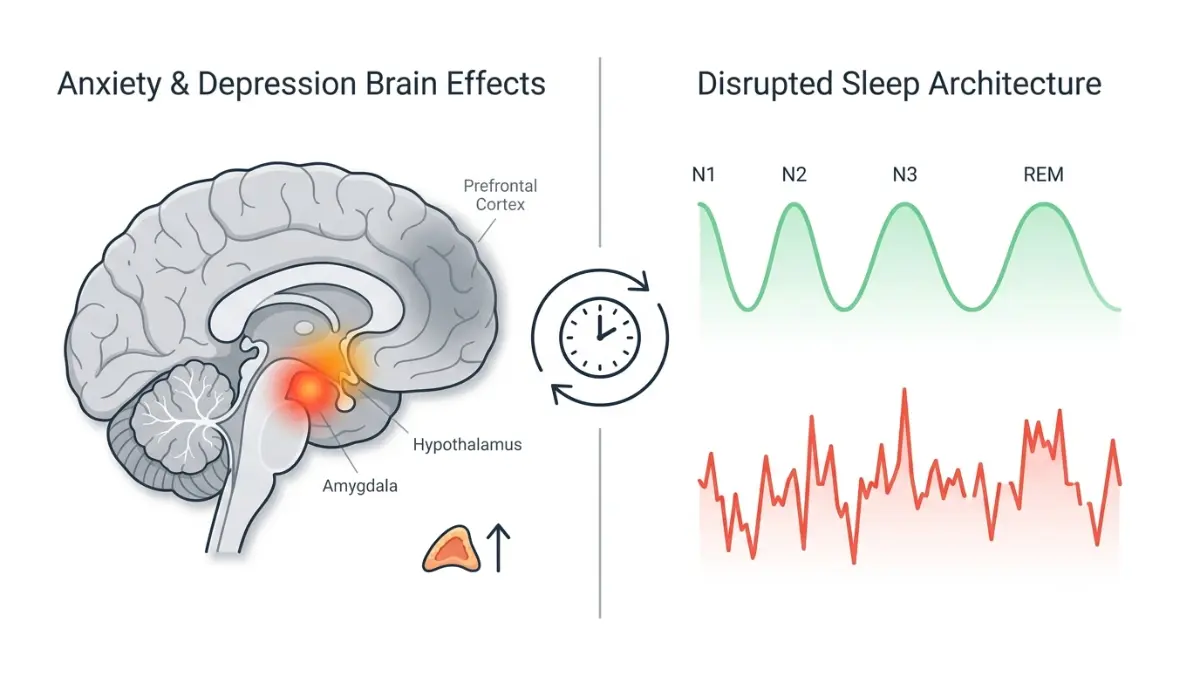
Depression Attacks Your Sleep Architecture
While anxiety primarily prevents sleep onset, depression does something more insidious — it dismantles the structure of sleep itself.
Depression disrupts REM sleep (Rapid Eye Movement sleep), the stage responsible for emotional processing and memory consolidation. It also shortens slow-wave deep sleep, the most physically restorative stage. The result is sleep that is technically present but not restoring you.
Among people with depression, 75% have trouble falling asleep or staying asleep. And people with insomnia face a tenfold higher risk of developing depression than those who sleep well.
Depression Can Cause Both Too Little AND Too Much Sleep
This surprises many people. Depression doesn’t always mean insomnia. It can cause hypersomnia — sleeping 10–12 hours yet still feeling exhausted. Both patterns stem from the same serotonin and dopamine dysregulation disrupting the circadian rhythm. To understand how your internal body clock controls this process, see our detailed guide on what circadian rhythm is and how it works.
Anxiety vs. Depression: How Sleep Problems Differ
This is the comparison no competitor has ever published — and it’s the most clinically useful table you’ll find on this topic:
| Factor | Anxiety Sleep Problems | Depression Sleep Problems |
|---|---|---|
| Sleep onset | Very difficult (racing thoughts) | Variable — may fall asleep easily |
| Night wakings | Occasional | Frequent, especially 3–5am |
| Early morning waking | Rare | Very common (classic sign) |
| Total sleep time | Reduced | Reduced OR excessive |
| REM sleep | Disrupted by hyperarousal | Significantly shortened early in night |
| Dream quality | Anxiety dreams, worry themes | Negative, hopeless themes |
| Morning feeling | Fatigued but tense | Flat, empty, heavy |
| Daytime pattern | Restless fatigue | Deep exhaustion, no motivation |
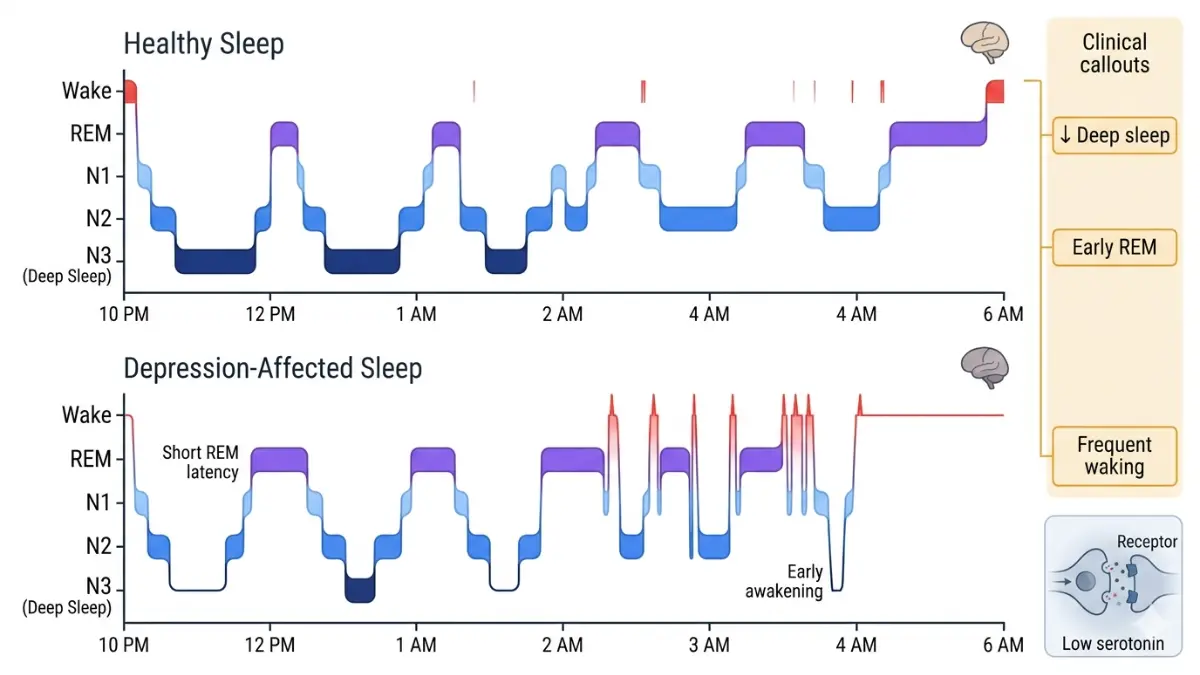
Duke Health psychiatrist Dr. Dan G. Blazer puts it precisely: “Chronic anxiety often prevents a person from falling asleep, but once they do fall asleep, they sleep soundly. The depressed may fall asleep without that much difficulty but then sleep lightly and awaken frequently during the night, especially toward the end of the night.”
Not sure if it’s anxiety, depression, or something else causing your sleep problems? Use our free Symptom Checker for a structured self-assessment.
For a deeper breakdown of sleep stages and what happens during each one, visit our guide on sleep stages explained.
The Vicious Cycle — When Sleep Problems Become Their Own Problem
Sleep Deprivation Is Now an Independent Risk Factor
For decades, sleep problems were treated as a symptom of anxiety and depression — address the mental health condition and the sleep would follow. That model is now outdated.
Research now confirms that sleep disturbance is no longer an epiphenomenon of depression but a predictive prodromal symptom — meaning poor sleep can precede and trigger depression, not just follow it.
In one major study of 10,000 adults, people with insomnia were five times more likely to develop depression. The same study found insomnia is a reliable predictor of virtually all anxiety disorder subtypes.
How the Vicious Cycle Works
Anxiety/Depression
↓
Poor Sleep Quality
↓
Impaired Emotional Regulation
↓
Increased Anxiety & Depressive Symptoms
↓
Even Worse Sleep
↑_____________↑
Stanford researchers describe it clearly: the issues compound and amplify each other, resulting in a vicious cycle where mental health problems exacerbate sleep problems, which further exacerbate sleep disruptions.
2025 Self-Check: Is Your Sleep Problem Linked to Anxiety or Depression?
Use this quick self-assessment table. If you identify with 3 or more signs in either column, discuss this with your doctor.
| # | Sign | More Likely Anxiety | More Likely Depression |
|---|---|---|---|
| 1 | Can’t fall asleep | ✅ | — |
| 2 | Wake at 3–5am, can’t return to sleep | — | ✅ |
| 3 | Racing thoughts at bedtime | ✅ | — |
| 4 | Sleep 9+ hours but still exhausted | — | ✅ |
| 5 | Dread going to bed | ✅ | — |
| 6 | No interest in things that used to help you sleep | — | ✅ |
| 7 | Physical tension (clenched jaw, tight chest) in bed | ✅ | — |
James, a 41-year-old IT manager in Chicago, had been waking at 4:15am for six months before his doctor connected it to a depressive episode — not his work stress. The correct diagnosis changed his entire treatment path.
If you regularly wake in the night and want to understand the neurological reasons, read our detailed article on waking up at 3am every night — causes and solutions.
Evidence-Based Treatments That Break the Cycle
CBT-I: The Gold Standard for Both Conditions
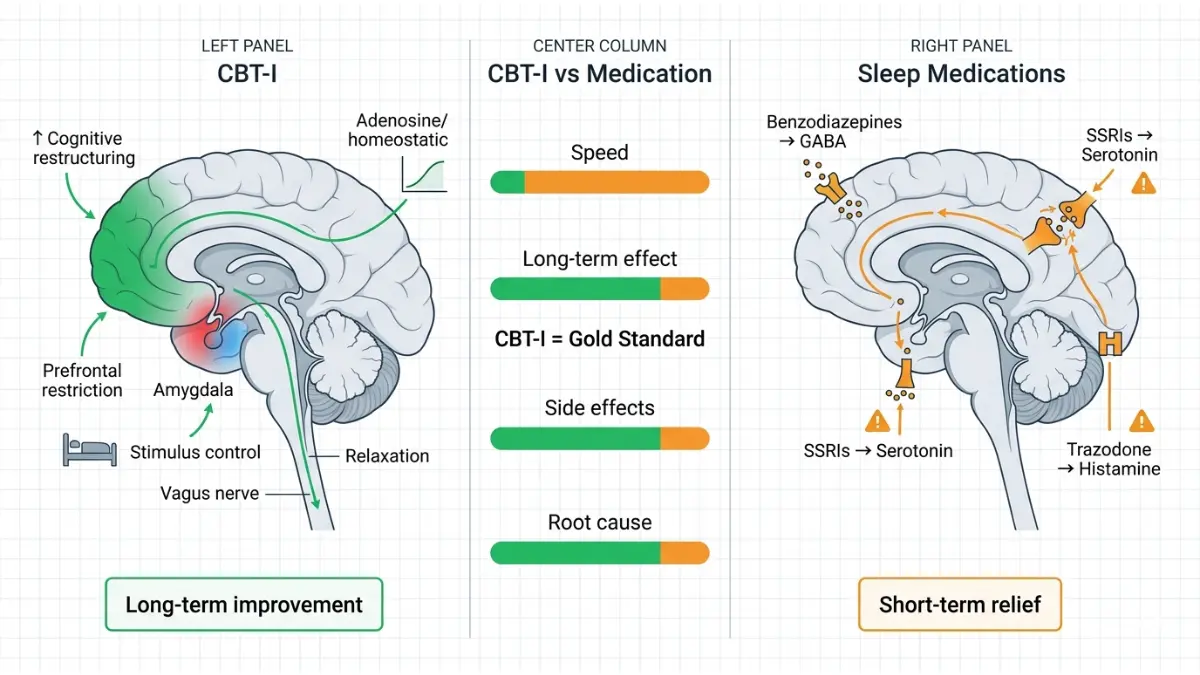
Cognitive Behavioral Therapy for Insomnia (CBT-I) is now the first-line treatment recommended by the American College of Physicians — ahead of sleep medication.
CBT-I works by:
- Restructuring negative beliefs about sleep (“I’ll never function without 8 hours”)
- Sleep restriction therapy — temporarily compressing sleep to build drive
- Stimulus control — retraining the brain to associate bed with sleep only
- Relaxation training — progressive muscle relaxation, breathing protocols
Stanford researchers found that CBT led to improvements in sleep which, in turn, led to lower levels of depression — and that bigger improvements in sleep correlated directly to bigger improvements in mental health outcomes.
Medication: What Helps, What Can Backfire
| Medication Type | Helps Sleep? | Risk |
|---|---|---|
| SSRIs/SNRIs (antidepressants) | Improves depression-related insomnia over time | Can initially worsen sleep in first 2 weeks |
| Benzodiazepines | Fast short-term effect | Dependency risk, worsens sleep architecture long-term |
| Trazodone | Sedating antidepressant, often prescribed off-label | Daytime drowsiness |
| Melatonin | Mild help for circadian issues | Minimal effect on anxiety/depression-driven insomnia |
| CBT-I (non-drug) | Most durable long-term improvement | Requires commitment |
Research confirms a critical clinical nuance: some antidepressants may cause or worsen sleep disturbances, and hypnotics always require consideration of drug dependence and resistance — making non-pharmacological treatments like CBT the preferred first approach.
For information on specific medications used in anxiety management, see our evidence-based guide on how to reduce anxiety naturally and our clinical overview of depression.
The AASM 2024 Sleep Hygiene Checklist
The American Academy of Sleep Medicine recommends these evidence-based habits for people whose sleep is disrupted by anxiety or depression:
- ✅ Consistent sleep/wake time — even on weekends (protects circadian rhythm)
- ✅ Cool, dark, quiet bedroom — 65–68°F is clinically optimal
- ✅ No screens 60 minutes before bed — blue light suppresses melatonin production
- ✅ Limit caffeine after 2pm — half-life of caffeine is 5–7 hours
- ✅ Avoid alcohol as a sleep aid — suppresses REM sleep and causes rebound waking
- ✅ Regular physical exercise — reduces cortisol and improves sleep architecture
- ✅ Relaxation protocol — diaphragmatic breathing, body scan, or progressive muscle relaxation
- ✅ Journaling worries before bed — externalizes anxiety and reduces cognitive arousal
Dehydration also measurably worsens sleep quality. Use our Water Intake Calculator to ensure you’re hitting your daily hydration target.
When to See a Doctor — The 5-Sign Framework
Seek professional evaluation if you experience any of the following:
- Sleep problems persisting beyond 3 weeks despite consistent sleep hygiene
- Daytime impairment — inability to concentrate, drive safely, or perform at work
- Mood symptoms accompanying sleep problems (hopelessness, persistent worry, panic attacks)
- Using alcohol or medication to fall asleep regularly
- Physical symptoms alongside poor sleep — heart palpitations, chest tightness, or weight changes
The National Institute of Mental Health (NIMH) provides a comprehensive guide on recognizing when depression requires clinical intervention.
For a full overview of sleep disorder warning signs, read our article on warning signs of a sleep disorder and our comprehensive guide on sleep disorders: symptoms and causes.
2025 Research Update — What’s New
The science on this topic moved significantly in 2024–2025:
- Nature Scientific Reports (July 2025): A network analysis of 1,571 insomnia patients found that 87.1% showed depression symptoms and 88% showed anxiety symptoms — confirming these conditions are almost universally co-occurring in sleep disorder patients.
- Stanford Medicine (August 2025): People with insomnia are 10 times more likely to have depression and 17 times more likely to have anxiety than the general population. Sleep apnea raises the risk of both conditions approximately threefold.
- “Mind After Midnight” Theory (2025): Stanford sleep researcher Dr. Jamie Zeitzer’s team found that people who go to bed late have higher risks of depression and anxiety — even when going to bed late aligns with their natural chronotype. Late-night wakefulness reduces social guardrails and amplifies negative decision-making.
- AASM Survey (May 2024): Over half of Americans (55%) report disrupted sleep due to depression, and nearly three-quarters report stress-related sleep disruption — rates significantly higher than pre-pandemic baselines.
The CDC’s sleep and sleep disorders resource center offers continuously updated population-level data on sleep health across the United States.
For further reading on what happens to your body when you’re always tired, see why you’re always tired no matter how much you sleep.
FAQs — Every Question Answered
1. Can anxiety cause sleep problems every night?
Yes. Chronic anxiety maintains elevated cortisol and hyperarousal state continuously, making consistent poor sleep a predictable outcome. Without intervention, the cycle tends to worsen over time rather than self-resolve.
2. Does depression make you sleep too much or too little?
Both. Depression can cause insomnia (difficulty falling or staying asleep) or hypersomnia (excessive sleep — 10+ hours with no refreshment). The type depends on the severity and subtype of depression, and both disrupt the sleep-wake cycle.
3. What type of sleep problems does anxiety cause?
Anxiety primarily causes sleep onset insomnia (difficulty falling asleep), frequent night wakings, vivid anxiety dreams, and early morning alertness due to cortisol spikes. Physical symptoms like rapid heartbeat and muscle tension also interfere with sleep.
4. How do I know if my sleep problem is from anxiety or depression?
Key distinction: Anxiety mainly prevents you from falling asleep. Depression typically lets you fall asleep but causes frequent waking or very early waking (3–5am) with a flat, empty mood. Use the self-check table in Section 3 above, and our Symptom Checker tool.
5. Can treating depression fix my sleep problems?
Partially — and not always immediately. There is evidence that lingering sleep problems in people undergoing depression treatment increase the risk of relapse into depression, which is why sleep must be treated as an independent condition alongside depression, not assumed to resolve on its own.
6. What is the best treatment for sleep problems caused by anxiety?
CBT-I (Cognitive Behavioral Therapy for Insomnia) is the gold standard. It is more effective than sleep medication in long-term studies and specifically addresses the thought patterns and behaviors that maintain anxiety-driven insomnia. The Anxiety and Depression Association of America (ADAA) provides a practitioner directory.
7. Does CBT-I work for anxiety-related insomnia?
Yes. CBT-I has a strong evidence base for both anxiety-related insomnia and depression-related insomnia. Studies show significant and durable improvements in sleep onset, total sleep time, and sleep quality — with benefits persisting at 12-month follow-up.
8. Can sleep problems cause anxiety — or is it the other way around?
Both. This is the bidirectional relationship covered throughout this article. Sleep problems can contribute to the onset and worsening of different mental health problems, including depression, anxiety, and even suicidal ideation — not just the reverse. New research treats poor sleep as an independent causal factor, not merely a symptom.
9. Why does anxiety get worse at night when trying to sleep?
Without the distractions of daytime activity, the brain defaults to worry processing mode. Cortisol also follows a natural spike pattern in early morning hours (beginning around 3–4am). Add physical stillness, darkness, and silence, and the conditions are neurologically optimized for anxiety to dominate.
10. Are sleep problems a warning sign of depression?
Yes — increasingly, clinicians treat chronic insomnia as a prodromal warning sign of depression. Research from Haukeland University Hospital found that subjects reporting insomnia in an initial survey had a significantly higher risk of developing an anxiety disorder and depression during a follow-up survey conducted 10 years later.
11. When should I see a doctor about sleep problems linked to mental health?
See a doctor if your sleep problems have persisted for 3 or more weeks, are affecting your work, relationships, or daily function, or are accompanied by persistent low mood, anxiety, panic attacks, or thoughts of self-harm. Early intervention dramatically improves outcomes for both sleep disorders and mental health conditions.
Key Takeaways
- ✅ Yes — anxiety and depression both directly cause sleep problems through distinct neurological mechanisms
- ✅ Anxiety mainly prevents falling asleep; depression mainly disrupts sleep quality and early morning waking
- ✅ Sleep problems are now an independent risk factor for developing anxiety and depression — not just a symptom
- ✅ CBT-I is the first-line treatment — more effective than medication long-term
- ✅ Sleep hygiene, consistent routines, and professional support can break the cycle
- ✅ Don’t wait — persistent sleep problems are a clinical signal worth acting on
For a comprehensive overview of what causes insomnia beyond mental health, read our related guide on what causes insomnia.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.