On This Page – Quick Medical Summary
Kevin, a 41-year-old teacher from Ohio, slept eight hours every night. Yet every afternoon, he’d fight to stay awake mid-lesson — sometimes losing the battle entirely. His colleagues thought he was lazy. His doctor eventually diagnosed him with obstructive sleep apnea. Kevin isn’t unusual. Millions of Americans experience exactly this, and most never get answers.
Excessive daytime sleepiness (EDS) is not ordinary tiredness. It is a persistent, often overwhelming urge to sleep during waking hours — even after a full night’s rest. According to a 2025 clinical review, EDS affects an estimated 33% of Americans on a daily basis, making it one of the most underreported health conditions in primary care.
This guide covers every symptom, every cause, and every red flag you need to know — including exactly when excessive daytime sleepiness becomes a medical emergency.
What Is Excessive Daytime Sleepiness — And How Is It Different From Normal Fatigue?
Most people feel tired after a bad night’s sleep. Excessive daytime sleepiness is different. It is defined as an inability to stay awake and alert during the day on a sustained basis — occurring almost every day for at least three months — despite apparently adequate or even extended nighttime sleep.
The critical distinction most articles miss:
| Feature | Normal Fatigue | Excessive Daytime Sleepiness |
|---|---|---|
| Can stay awake if needed | Yes | Often no |
| Napping provides relief | Usually | Often not |
| Occurs despite full sleep | No | Yes |
| Affects driving safety | Rarely | Frequently |
| Persists for months | No | Yes |
Fatigue means you feel drained and sluggish but can stay awake. EDS means your body physically pulls you toward sleep at inappropriate times — during meetings, meals, or even while driving.
This distinction matters enormously. If you are always tired no matter how much sleep you get, it may point to a specific underlying condition that requires investigation — not just more rest.
Key Takeaway: Excessive daytime sleepiness is a medical symptom, not a character flaw or lifestyle choice.
10 Symptoms of Excessive Daytime Sleepiness Most Americans Ignore
Daytime sleepiness exists on a spectrum. Recognising where you fall on that spectrum is the first step toward getting real answers.
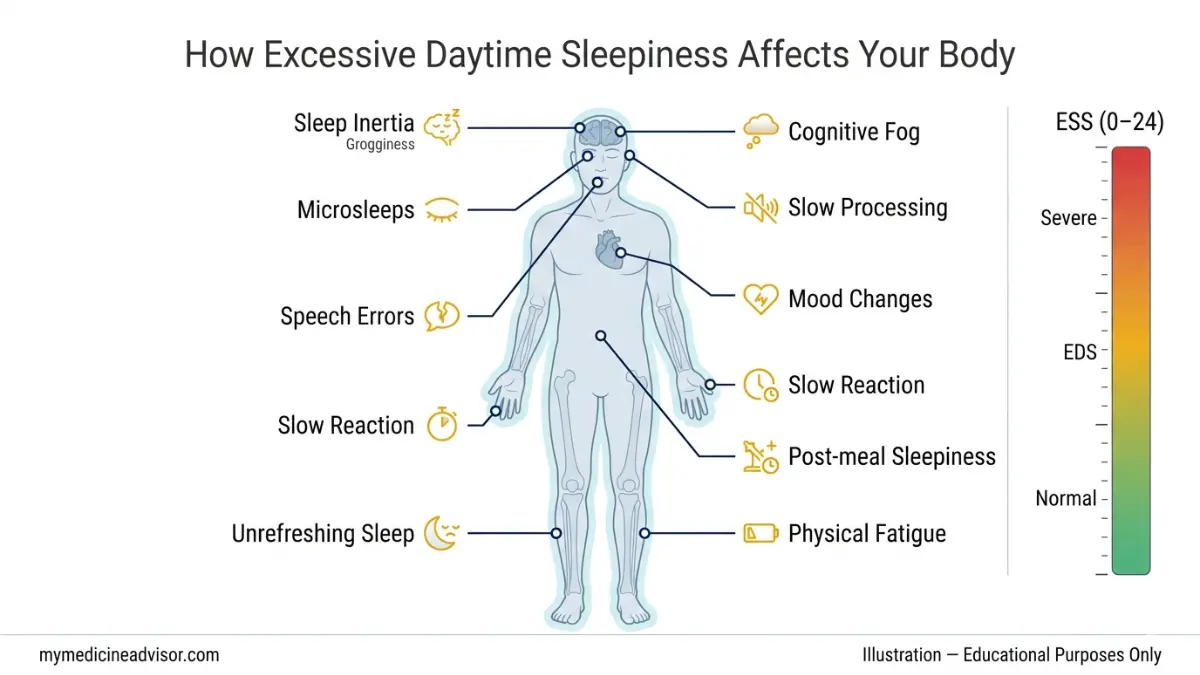
The 10 most clinically significant symptoms of EDS:
- Uncontrollable sleep episodes — falling asleep without intending to, even mid-conversation
- Persistent drowsiness — feeling sleepy throughout the day regardless of how much you slept
- Sleep inertia — severe grogginess and confusion lasting 30+ minutes after waking
- Microsleeps — brief (2–30 second) episodes of sleep you may not notice, especially dangerous while driving
- Non-refreshing naps — sleeping during the day and waking up equally or more tired
- Cognitive fog — difficulty concentrating, recalling words, or making decisions
- Mood changes — increased irritability, emotional blunting, or depressive episodes
- Falling asleep in low-stimulation settings — waiting rooms, church, passenger seat of a car
- Performance decline — dropping grades, missed deadlines, increased workplace errors
- Automatic behaviour — completing tasks on “autopilot” with no memory of doing so
Notice 3 or more of these happening most days? This is not normal tiredness. Use our Symptom Checker to document your symptoms before your next appointment — it gives your doctor a far clearer clinical picture than “I’ve been tired lately.”
It is also worth reviewing our guide on the warning signs of a sleep disorder to understand whether your pattern of symptoms points toward a specific diagnosis.
What This Means For You: The more symptoms on this list that apply to you daily, the more urgently you need a sleep evaluation — not a second coffee.
The Epworth Sleepiness Scale — Score Yourself Right Now
The Epworth Sleepiness Scale (ESS) is the gold-standard clinical tool used by sleep specialists across the USA, UK, Canada, and Australia to quantify excessive daytime sleepiness. Developed in 1990 by Dr. Murray Johns at Epworth Hospital, Melbourne, it takes under three minutes to complete.
How it works: Rate how likely you are to doze off in each of these 8 situations, from 0 (never) to 3 (high chance):
- Sitting and reading
- Watching TV
- Sitting inactive in a public place (meeting, theatre)
- As a car passenger for one hour
- Lying down to rest in the afternoon
- Sitting and talking to someone
- Sitting quietly after lunch (no alcohol)
- Stopped briefly in traffic while driving
Add up your score. Here is what it means:
| ESS Score | Interpretation | Recommended Action |
|---|---|---|
| 0–10 | Normal daytime sleepiness | Monitor; focus on sleep hygiene |
| 11–15 | Excessive daytime sleepiness | See your primary care physician within 2–4 weeks |
| 16–24 | Severe EDS — probable sleep disorder | Seek urgent sleep specialist referral |
An ESS score above 10 indicates clinical excessive daytime sleepiness. A score of 16 or higher is strongly associated with serious conditions including narcolepsy and severe obstructive sleep apnea, according to the American Academy of Sleep Medicine.
Real case: Marcus, 52, from Texas, took the ESS and scored 19. He had assumed his constant sleepiness was “just getting older.” His sleep study revealed he was stopping breathing 44 times per hour. Six months of CPAP therapy later, his ESS score dropped to 6.
To better understand how much sleep your body actually needs, use our Sleep Calculator — it calculates your optimal sleep window based on age and sleep cycle science.
What Causes Excessive Daytime Sleepiness? From Common to Critical
EDS has dozens of possible causes. Understanding them — and their severity — is what separates a manageable lifestyle fix from a condition needing urgent treatment.
Lifestyle Causes (Start Here)
The most common and most reversible causes:
- Chronic sleep deprivation — the #1 cause; most U.S. adults need 7–9 hours but average 6.5
- Irregular sleep schedules — inconsistent bedtimes disrupt your body’s circadian rhythm, making quality sleep impossible
- Blue light exposure — screens suppress melatonin production, delaying sleep onset
- Alcohol — acts as a sedative but fragments deep sleep stages, leaving you unrefreshed
- Sedating medications — antihistamines, antidepressants, muscle relaxants, and antipsychotics
- Caffeine dependency — disrupts sleep architecture when consumed after 2pm
- Physical inactivity — regular exercise is proven to improve daytime alertness and reduce time to sleep onset
Understanding how your sleep stages work is essential here — poor lifestyle choices specifically suppress slow-wave and REM sleep, which are the stages responsible for restoration.
Medical & Sleep Disorder Causes
These require clinical diagnosis:
Obstructive Sleep Apnea (OSA) The single most dangerous and most undertreated cause of EDS. In OSA, the airway collapses repeatedly during sleep, fragmenting it without the person waking fully. An estimated 26–32% of U.S. adults are at risk. Obesity is a major risk factor — if your BMI is elevated, checking your BMI Calculator is a practical first step in assessing your OSA risk.
Narcolepsy A neurological disorder where the brain loses control of the sleep-wake cycle. People with narcolepsy experience sudden “sleep attacks” — uncontrollable sleep onset regardless of activity. It often remains undiagnosed for 8–10 years.
Idiopathic Hypersomnia Sleeping 11 or more hours yet waking exhausted, with severe sleep inertia. Unlike narcolepsy, naps provide no relief. According to the National Institutes of Health, this condition is significantly underdiagnosed.
Restless Legs Syndrome (RLS) Uncomfortable sensations in the legs at night create fragmented sleep, leading directly to EDS the following day.
Circadian Rhythm Disorders Shift workers, frequent travellers, and night-owl chronotypes face misalignment between their internal clock and external schedule. This is addressed in detail in our circadian rhythm guide.

Hidden Medical Triggers (What Top Competitors Miss)
These are the causes that most online articles completely overlook:
- Hypothyroidism — an underactive thyroid slows metabolism, causing profound fatigue and EDS; explore our deep-dive on hypothyroidism symptoms
- Anaemia (iron deficiency) — reduced oxygen delivery to the brain causes unrelenting sleepiness
- Depression — can manifest as hypersomnia, not just insomnia; see our depression guide
- Diabetes / blood sugar dysregulation — post-meal glucose spikes and crashes trigger acute sleepiness episodes
- Kidney or liver disease — organ dysfunction releases toxins that impair wakefulness
- Neurological conditions — Parkinson’s disease, multiple sclerosis, and TBI all list EDS as a primary symptom
- Vitamin D deficiency — now linked to sleep quality disruption in multiple 2024–2025 studies
The Cause-Severity Matrix — No Competitor Shows You This:
| Cause | EDS Severity | Reversible? | Urgency |
|---|---|---|---|
| Sleep deprivation | Mild–Moderate | ✅ Yes | Low |
| Hypothyroidism | Mild–Moderate | ✅ Yes | Moderate |
| Depression | Moderate | ✅ With treatment | Moderate |
| OSA | Moderate–Severe | ✅ With CPAP | High |
| Narcolepsy | Severe | ⚠️ Managed only | High |
| Idiopathic Hypersomnia | Severe | ⚠️ Partially | High |
| CNS/Neurological cause | Severe | Depends | Urgent |
When to Worry — Red Flags and How Doctors Diagnose EDS
This is the section that no major competitor fully covers — and the #1 reason people search this topic.
🔴 Red Flag Symptoms: See a Doctor Urgently
Do not wait for your next annual check-up if you experience any of the following:
- Falling asleep while driving or in genuinely dangerous situations
- Cataplexy — sudden, brief muscle weakness triggered by strong emotions (laughing, surprise); this is a hallmark of narcolepsy
- Hypnagogic hallucinations — vivid, often frightening hallucinations when falling asleep or waking
- EDS that developed suddenly over days or weeks rather than gradually
- Snoring + gasping + morning headaches — the classic OSA triad
- ESS score above 16
- Sleepiness alongside rapid unexplained weight gain (thyroid/metabolic cause)
- Unrefreshing sleep persisting for more than 3 months despite good sleep hygiene
Critical Safety Fact: Research published in Mayo Clinic Proceedings found that EDS in patients with obstructive sleep apnea was linked to significantly higher rates of major adverse cardiovascular events. This is not a quality-of-life issue only — it carries real mortality risk.
EDS is also linked to motor vehicle accidents at a rate comparable to driving while legally intoxicated. If you are falling asleep at the wheel, this is a medical emergency — not a caffeine deficiency.
How Doctors Diagnose Excessive Daytime Sleepiness
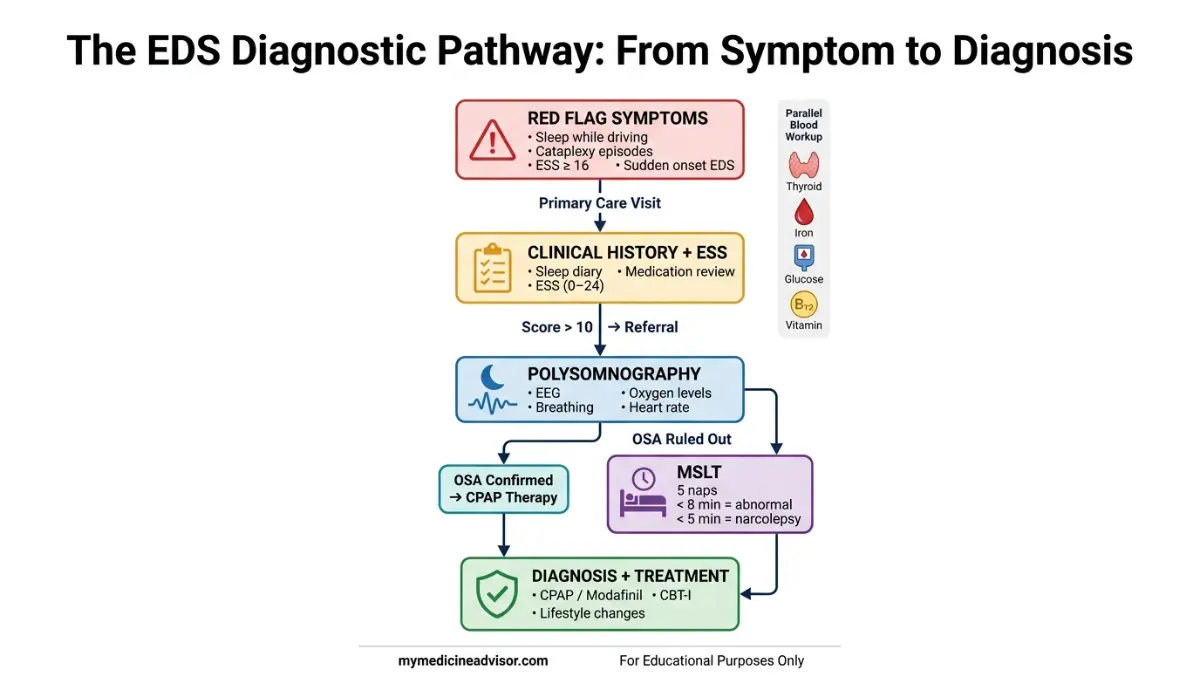
A sleep specialist will typically use a stepwise approach:
Step 1 — Clinical History + ESS Score Your doctor will ask about symptom duration, sleep schedule, medications, and lifestyle. The ESS quantifies severity.
Step 2 — Sleep Diary You log sleep and wake times, nap frequency, and daytime function for 2–4 weeks. This reveals patterns invisible to a single clinic visit.
Step 3 — Polysomnography (Overnight Sleep Study) The definitive test for sleep-disordered breathing. Conducted in a sleep lab or, increasingly, at home. Measures brain waves, oxygen levels, breathing, and heart rate simultaneously.
Step 4 — Multiple Sleep Latency Test (MSLT) Measures how quickly you fall asleep in a quiet room — conducted 5 times across a single day at 2-hour intervals. The faster you fall asleep, the more severe your EDS. Falling asleep in under 8 minutes is clinically significant. Under 5 minutes suggests narcolepsy.
Step 5 — Blood Tests Thyroid panel (TSH, T3, T4), full blood count, ferritin, B12, blood glucose, and vitamin D are commonly ordered to rule out metabolic causes.
Who Is Most at Risk in the USA?
- Adults aged 17–24 (peak EDS prevalence in young adults)
- Shift workers — nurses, long-haul truck drivers, emergency responders
- Adults with obesity (OSA risk is substantially elevated)
- Pregnant women — sleep architecture changes dramatically in each trimester; use our Pregnancy Weight Gain Calculator to track related health markers
- People with depression, anxiety, or bipolar disorder
- Anyone taking multiple medications (polypharmacy)
How to Treat Excessive Daytime Sleepiness — From Today’s Fixes to Clinical Options
Treatment is entirely cause-dependent. Here is the most comprehensive breakdown available.
Step 1: Start With Sleep Hygiene
For lifestyle-driven EDS, these changes work — but must be sustained:
- Lock in a consistent sleep/wake time — even weekends; this is the single most effective circadian reset
- Restrict caffeine after 2pm — caffeine has a 5–7 hour half-life
- No alcohol within 3 hours of bedtime — it fragments REM sleep
- Strategic napping: 10–20 minutes maximum, before 3pm only; longer naps worsen night-time sleep quality
- Increase physical activity — even a 20-minute walk reduces time to sleep onset and improves slow-wave sleep depth. Use our Heart Rate Zone Calculator to find your optimal low-intensity exercise zone for sleep benefits
- Reduce screen time 60–90 minutes before bed — blue light suppresses melatonin by up to 50%
The CDC’s sleep health guidelines recommend adults obtain 7–9 hours per night as a foundation for addressing daytime sleepiness.
Step 2: Treat the Underlying Condition
| Diagnosis | Primary Treatment | Medication (When Needed) |
|---|---|---|
| OSA | CPAP therapy | Modafinil for residual EDS |
| Narcolepsy | Scheduled naps + behavioural therapy | Sodium oxybate, Pitolisant (Wakix) |
| Idiopathic Hypersomnia | Extended sleep + sleep hygiene | Modafinil, Armodafinil |
| Hypothyroidism | Levothyroxine (thyroid hormone replacement) | — |
| Anaemia | Iron supplementation | — |
| Depression | CBT + antidepressant therapy | Per psychiatrist |
| Shift Work Disorder | Light therapy + timed melatonin | Modafinil (FDA-approved for shift work) |
| Circadian Rhythm Disorder | Chronotherapy + structured schedule | Melatonin, light therapy |
On medications: Modafinil is the FDA-approved first-line wakefulness agent for EDS associated with OSA, narcolepsy, and shift work disorder. It carries a Schedule IV classification — substantially lower abuse potential than older stimulants like amphetamines. Never self-prescribe wakefulness agents. Always work with a board-certified sleep specialist.
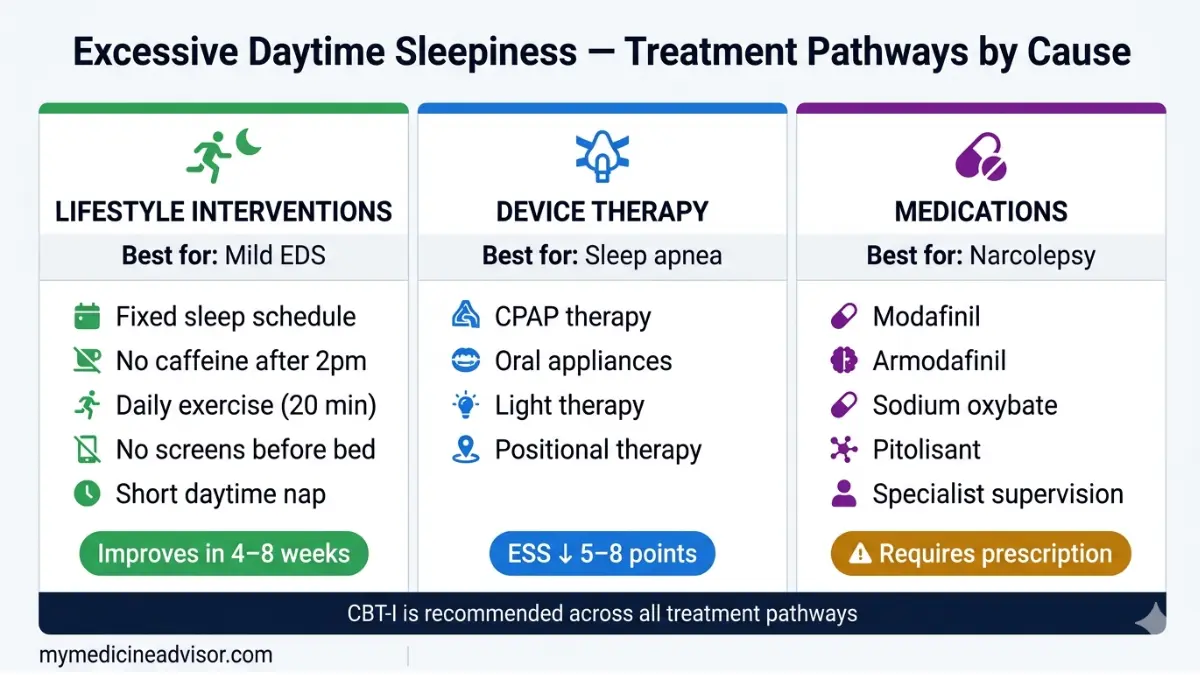
Step 3: Cognitive Behavioural Therapy for Insomnia (CBT-I)
CBT-I is the most evidence-supported non-drug treatment for sleep disorders that contribute to EDS. It restructures dysfunctional beliefs about sleep and modifies behaviours that perpetuate poor sleep. The National Institute of Neurological Disorders and Stroke recognises it as a first-line recommendation before pharmacological intervention.
What This Means For You: If you have had EDS for more than 3 months and lifestyle changes haven’t moved the needle, you likely need a sleep study — not more willpower. A single overnight polysomnography can identify or rule out the vast majority of treatable causes in one night.
Frequently Asked Questions about Excessive Daytime Sleepiness
1. What is excessive daytime sleepiness?
Excessive daytime sleepiness is a clinical condition characterised by an inability to stay awake and alert during the day, occurring persistently despite adequate or extended nighttime sleep. It is a symptom of multiple underlying conditions, not a standalone disorder.
2. How do I know if my sleepiness is a medical problem?
If it persists for more than three months, affects your ability to drive or work safely, or occurs despite getting 7–9 hours of sleep, it requires medical evaluation. An ESS score above 10 is the clinical threshold for concern.
3. Can excessive daytime sleepiness be a sign of cancer or serious illness?
In rare cases, yes. Brain tumours, neuroblastoma, and paraneoplastic syndromes can cause EDS. More commonly, EDS signals treatable conditions like OSA, hypothyroidism, or anaemia. Sudden onset EDS with no obvious cause always warrants investigation.
4. What is a concerning Epworth Sleepiness Scale score?
A score of 11 or above indicates excessive daytime sleepiness. A score of 16 or above is classified as severe and is strongly associated with narcolepsy and moderate-to-severe OSA.
5. Is it normal to feel sleepy after eating?
Mild post-meal drowsiness is normal, driven by a small insulin response and increased blood flow to the gut. Extreme sleepiness after every meal — especially lunch — can indicate blood sugar dysregulation, sleep debt, or undiagnosed sleep apnea.
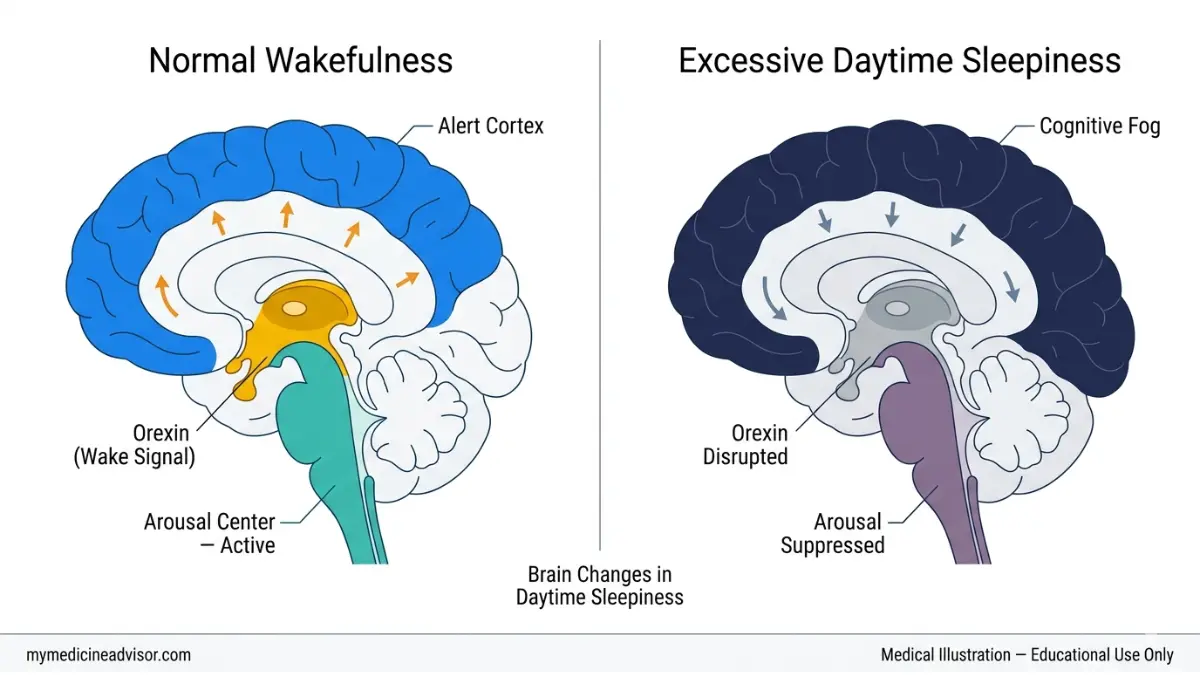
6. What is the difference between hypersomnia and narcolepsy?
Hypersomnia (idiopathic hypersomnia) involves prolonged sleep and unrefreshing naps without cataplexy or hallucinations. Narcolepsy involves sudden uncontrollable sleep attacks, often with cataplexy, and is caused by a deficiency of the brain chemical hypocretin (orexin).
7. Can anxiety or depression cause excessive daytime sleepiness?
Yes. Depression is one of the most common non-sleep-disorder causes of EDS. It can push sleep duration far beyond normal (hypersomnia subtype) while leaving sleep completely unrestorative. Anxiety fragments sleep architecture, reducing slow-wave and REM sleep.
8. What medications cause excessive daytime sleepiness?
Common culprits include benzodiazepines, antihistamines (diphenhydramine), tricyclic antidepressants, antipsychotics, muscle relaxants, opioid pain medications, and some blood pressure medications (beta-blockers). Always review your medication list with your pharmacist using our Pill Identifier tool if you are unsure what you are taking.
9. Can sleep apnea cause excessive daytime sleepiness?
Obstructive sleep apnea is the most dangerous and most common diagnosable cause of EDS. Each breathing interruption partially wakes the brain, preventing deep restorative sleep — even if the person has no memory of waking. CPAP therapy resolves EDS in the majority of OSA patients.
10. What does a sleep specialist do for EDS?
A sleep specialist reviews your full medical, medication, and sleep history, administers validated questionnaires like the ESS, and orders a polysomnography and/or MSLT to identify the precise cause. They then create a cause-specific treatment plan combining behavioural, medical, and pharmacological strategies.
11. Can excessive daytime sleepiness be treated naturally?
For lifestyle-driven EDS — yes, completely. Consistent sleep schedules, eliminating alcohol before bed, regular moderate exercise, and eliminating sedating medications often resolve EDS within 4–8 weeks. For EDS caused by OSA, narcolepsy, or hypothyroidism, natural approaches alone are insufficient — medical treatment is essential.
Related Reading From mymedicineadvisor.com:
- Sleep Disorders: Symptoms & Causes
- Waking Up at 3am Every Night — What It Means
- What Is REM Sleep and Why It Matters
- Hours of Sleep by Age — The Complete Chart
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.