On This Page – Quick Medical Summary
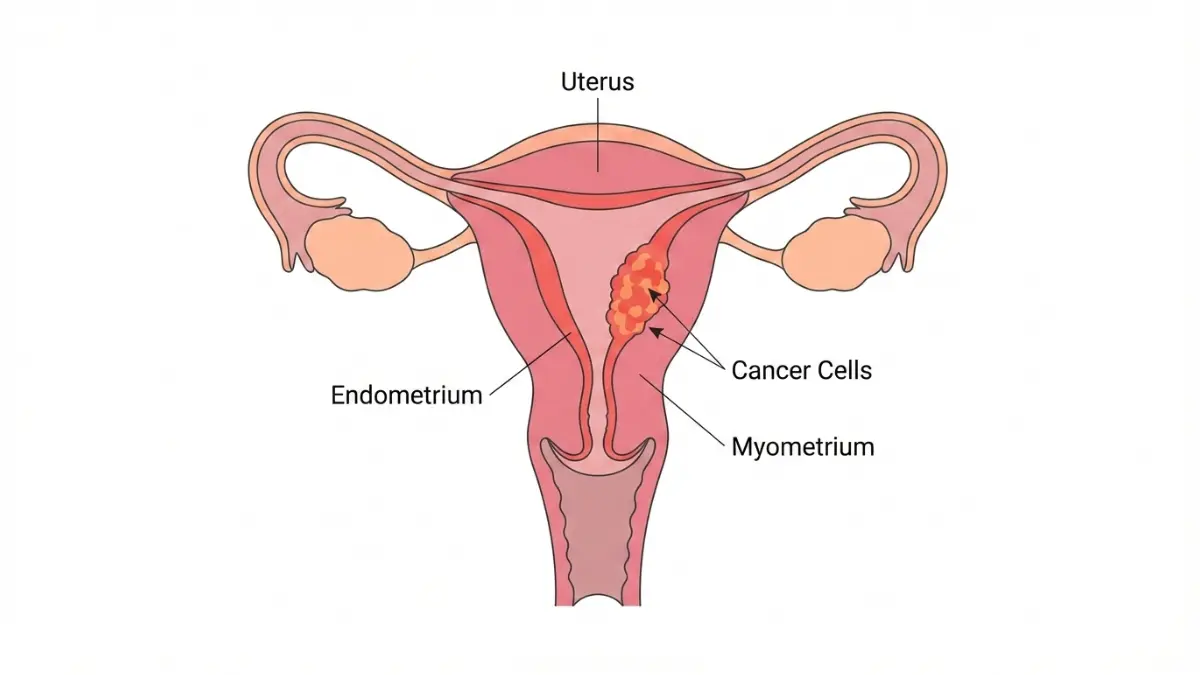
What Every Woman Needs to Know About Uterine Cancer in 2026
Michelle, a 58-year-old marketing director from Chicago, dismissed her light spotting as “just hormones adjusting.” Six months later, she faced a stage 2 uterine cancer diagnosis. “I thought bleeding after menopause meant my periods were coming back,” she recalls. “I never imagined cancer.”
Michelle’s story isn’t unique. In 2026, an estimated 69,120 American women will be diagnosed with uterine cancer, making it the most common gynecologic malignancy in the United States. More alarming: incidence rates have been rising 0.7% annually since 2013, with mortality climbing even faster at 1.6% per year.
The tragedy? Most women miss the early warning signs.
Unlike ovarian cancer, which often hides until advanced stages, uterine cancer announces itself through symptoms—particularly abnormal bleeding. Yet women routinely dismiss these red flags as “normal aging,” perimenopause, or “just heavy periods.” The average diagnosis age has dropped from 64 to 61 years, meaning younger women are increasingly at risk.
Here’s what makes this disease both terrifying and hopeful: when caught early, the 5-year survival rate is 95%. The difference between life-threatening illness and complete recovery often hinges on recognizing 11 specific warning signs that women consistently overlook.
This isn’t another generic symptom list. This is a comprehensive, evidence-based guide built on 2026 medical research, National Cancer Institute data, and real patient experiences. You’ll learn exactly what symptoms demand immediate attention, how uterine cancer manifests differently at various ages, and when “wait and see” becomes dangerous.
What you’ll discover:
- The 11 warning signs 90% of women dismiss
- Age-specific symptom patterns (under 45, 45-55, over 55)
- The 24-hour rule for emergency symptoms
- How to differentiate cancer from fibroids, endometriosis, and perimenopause
- Your personal risk profile and prevention strategies
Why should you read this today? Because 69% of uterine cancers are diagnosed at localized stage when treatment is most effective, but only if women recognize symptoms early. Using our Symptom Checker alongside this guide can help you assess your personal risk and determine if you need immediate evaluation.
Every woman deserves to know what her body is telling her. Let’s decode those signals together.
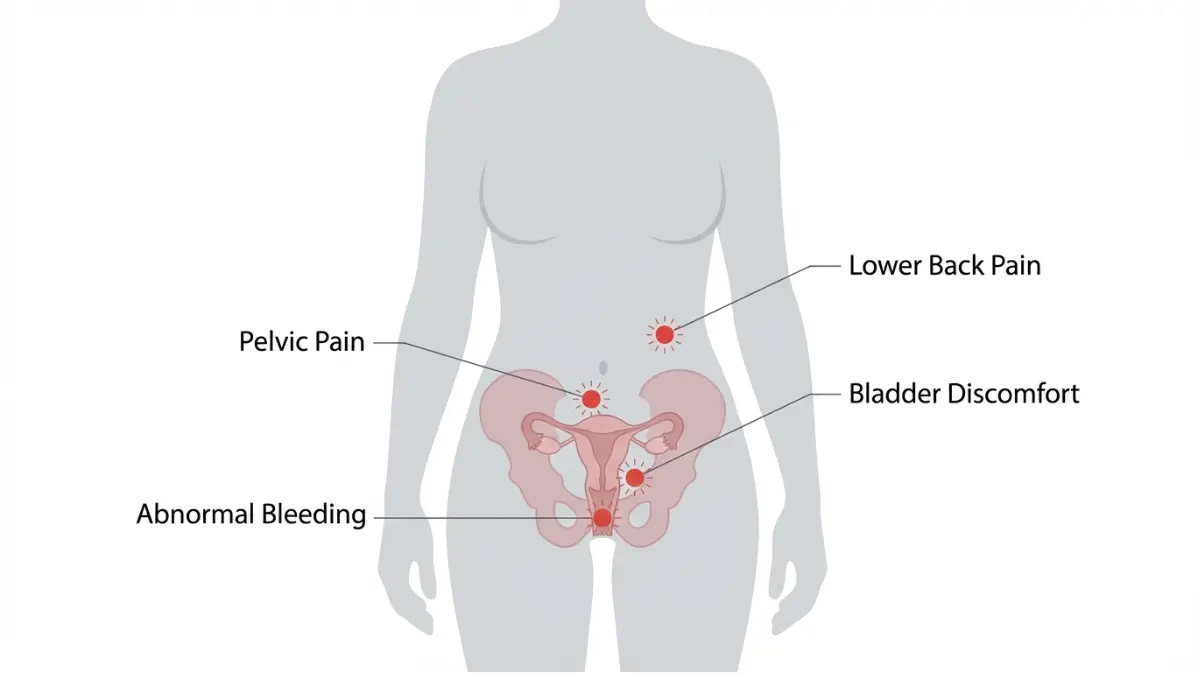
11 Uterine Cancer Symptoms Most Women Miss
Why Women Overlook These Signs
Ninety percent of uterine cancer patients experience abnormal bleeding, yet countless women delay seeking care. According to CDC surveillance data, the median time from first symptom to diagnosis is 3-6 months—a delay that can mean the difference between stage 1 and stage 3 disease.
The problem isn’t ignorance; it’s normalization. Women are conditioned to accept irregular bleeding, cramping, and discharge as “just part of being female.” But your body speaks a specific language when cancer develops, and learning that language could save your life.
Signs 1-4: Bleeding-Related Symptoms
1. Postmenopausal Bleeding (Even One Drop Matters)
Any vaginal bleeding after you’ve stopped having periods for 12 consecutive months is abnormal. Period.
“I spotted for just two days—barely enough to need a panty liner,” says Jennifer, diagnosed at 62. “I almost didn’t mention it to my doctor.” That “insignificant” spotting was stage 1 endometrial cancer.
Research from the American College of Obstetricians and Gynecologists confirms that 90% of postmenopausal women with endometrial cancer present with vaginal bleeding. The color varies—pink, brown, or bright red—but the rule remains: one dab of blood after menopause requires immediate evaluation.
2. Unusually Heavy Periods (Premenopausal Warning)
Heavy menstrual bleeding affects 15-25% of premenopausal women with uterine cancer. But how heavy is too heavy?
Red flags include:
- Soaking through a pad or tampon every 1-2 hours
- Passing blood clots larger than a quarter
- Bleeding lasting longer than 7 days
- Needing to change protection during the night
“My periods were always heavy, so I didn’t think much of it,” recalls Destiny, diagnosed at 43. “When I started bleeding through overnight pads in 3 hours, I finally went in.” Many women with obesity-related hormonal imbalances attribute heavy bleeding to their weight rather than recognizing it as a cancer symptom—making tools like our BMI Calculator crucial for understanding your overall risk profile.
3. Bleeding Between Periods (The Spotting Women Ignore)
Intermenstrual bleeding—spotting between regular periods—affects approximately 30% of premenopausal women with uterine cancer. This symptom is particularly insidious because women often dismiss it as “breakthrough bleeding” or ovulation spotting.
What to watch for:
- Pink or brown discharge mid-cycle
- Light spotting for 2-3 days between periods
- Irregular bleeding patterns developing over 2+ months
The challenge: distinguishing cancer from common causes like hormonal contraception side effects, polyps, or stress. When spotting persists for three consecutive cycles or increases in frequency, evaluation becomes essential.
4. Bleeding After Sex (Post-Intercourse Spotting)
Post-coital bleeding occurs in 10-15% of uterine cancer cases, though it’s more commonly associated with cervical issues. The bleeding typically appears immediately or within hours after intercourse.
“I assumed my husband and I were just being too rough,” admits Patricia, 56. “After the third time, my gynecologist ordered an ultrasound.” The National Institutes of Health emphasizes that any persistent post-coital bleeding in women over 40 warrants endometrial evaluation.
Signs 5-7: Discharge & Pain Symptoms
5. Watery or Blood-Tinged Discharge
Fifty percent of endometrial cancer patients report abnormal vaginal discharge before diagnosis. This discharge differs from normal variations:
Cancer-related discharge characteristics:
- Watery consistency (sometimes described as “thin” or “runny”)
- Pink, brown, or blood-streaked appearance
- Foul or unusual odor
- Persistent despite treatment for infections
“The discharge was constant—like a slow leak I couldn’t control,” describes Tamara, 61. “It wasn’t painful or itchy, just always there.” This symptom often coincides with tumor necrosis (tissue breakdown), producing the characteristic odor that distinguishes it from bacterial vaginosis or other infections.
6. Pelvic Pain or Pressure (The Cramping That Won’t Stop)
Persistent pelvic discomfort affects 20-30% of women with uterine cancer, particularly as the disease advances. This pain differs markedly from menstrual cramping.
Distinguishing features:
- Constant dull ache rather than cyclical cramping
- Feeling of fullness or pressure in the lower abdomen
- Pain that doesn’t respond to typical menstrual cramp remedies
- Radiating discomfort to the lower back or legs
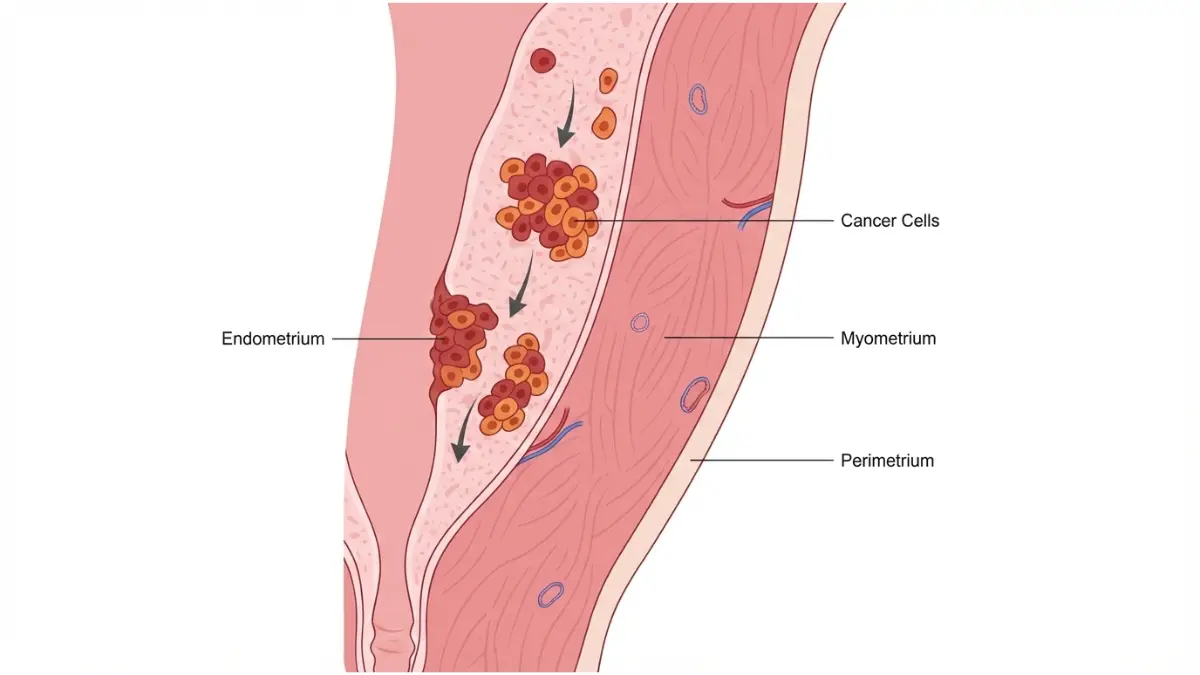
The pain results from tumor growth stretching the uterine wall or invading surrounding tissues. Women often describe it as “something pressing from inside” or “a weight that won’t shift.”
7. Pain During Intercourse (Dyspareunia)
Deep pelvic pain during or after sex occurs more frequently with advanced uterine cancer. The discomfort stems from:
- Direct tumor involvement of pelvic structures
- Uterine enlargement causing pressure
- Inflammation of surrounding tissues
This symptom often accompanies other warning signs, rarely appearing in isolation. If you’re experiencing multiple symptoms, our comprehensive Symptom Checker can help you assess whether immediate medical evaluation is necessary.
Signs 8-11: Systemic & Subtle Symptoms
8. Unexplained Weight Loss (Without Trying)
Unintentional weight loss exceeding 10 pounds over 1-2 months appears in advanced-stage disease. This cancer-related weight loss differs from intentional dieting:
- Occurs despite normal or increased appetite
- Accompanied by fatigue and weakness
- Often coincides with other symptoms
“I’d been trying to lose weight for years,” says Rhonda, 59. “When I finally did, without changing anything, I should have been suspicious.”
9. Persistent Bloating (Abdomen Feels Full)
Abdominal distention from uterine cancer presents as:
- Constant bloating unrelated to menstrual cycle
- Visible abdominal swelling
- Feeling of fullness after eating small amounts
- Clothing fitting tighter around the waist
This symptom typically indicates tumor growth or fluid accumulation (ascites) in more advanced cases.
10. Urinary Changes (Frequent or Painful Urination)
Bladder symptoms emerge when tumors press against the bladder or invade adjacent tissues:
- Urgent need to urinate frequently
- Difficulty fully emptying the bladder
- Painful urination without infection
- Stress incontinence developing suddenly
11. Fatigue That Won’t Improve
Cancer-related fatigue differs from normal tiredness. It’s overwhelming exhaustion that:
- Doesn’t improve with rest
- Interferes with daily activities
- Stems from anemia caused by chronic bleeding
- Accompanied by weakness and difficulty concentrating
What This Means For You
If you experience 2+ of these symptoms persistently for more than 2 weeks, schedule a gynecologist appointment within one week.
Emergency symptoms requiring 24-hour evaluation:
- Heavy bleeding (soaking pad hourly for 2+ hours)
- Severe pelvic pain with fever
- Sudden onset intense abdominal pain
- Any postmenopausal bleeding with clots
How Uterine Cancer Symptoms Differ by Age (2026 Research)
Age dramatically influences how uterine cancer presents, often determining whether women recognize symptoms as concerning or dismiss them as “normal for my age.”

Under 45: Pre-Menopausal Presentations
Fifteen to twenty-five percent of uterine cancer cases occur before menopause, challenging the misconception that this is exclusively a post-menopausal disease. The National Cancer Institute reports the average diagnosis age has decreased to 61 years, with increasing incidence in women under 45.
Why diagnosis is harder in younger women:
Pre-menopausal women often have irregular cycles due to polycystic ovary syndrome (PCOS), endometriosis, or hormonal imbalances. When cancer symptoms emerge, they’re indistinguishable from pre-existing menstrual irregularities.
“I’d had irregular periods my entire adult life because of PCOS,” explains Jasmine, diagnosed at 39. “When bleeding got worse, I blamed it on stress and age.” Her obesity—a known risk factor for both PCOS and uterine cancer—complicated the clinical picture further.
Red flags in younger women:
- Sudden worsening of previously stable irregular periods
- Bleeding patterns changing dramatically within 2-3 months
- Heavy bleeding accompanied by unexplained weight loss
- Persistent bleeding despite hormonal treatments
Women under 45 with obesity should particularly monitor for symptoms, as excess body weight significantly increases risk. Maintaining awareness of your baseline weight using tools like our Ideal Weight Calculator can help you recognize concerning changes early.
Ages 45-55: Perimenopause Confusion
This represents the diagnostic danger zone where cancer symptoms perfectly mimic normal menopausal transition.
The overlap problem:
| Perimenopause Symptoms | Uterine Cancer Symptoms |
|---|---|
| Irregular bleeding patterns | Irregular bleeding patterns |
| Heavy periods | Heavy periods |
| Spotting between periods | Intermenstrual bleeding |
| Hot flashes, mood changes | May occur with or without |
“Every symptom I had was ‘explained’ by perimenopause,” recalls Denise, 52. “My doctor and I both missed it for eight months.” Research from Johns Hopkins Medicine indicates this age group experiences the longest diagnostic delays.
Critical distinction: Perimenopause symptoms fluctuate monthly with hormonal changes. Cancer symptoms progressively worsen over weeks to months. Additionally, cancer-related discharge often has a foul odor, unlike perimenopause discharge.
Over 55: Post-Menopausal Red Flags
Post-menopausal women should operate under one ironclad rule: any bleeding is abnormal.
“I’d been period-free for three years when I spotted for two days,” says Carolyn, 67. “I knew immediately something was wrong.” Her prompt action led to stage 1 diagnosis with excellent prognosis.
Why this age has better detection rates:
The symptom is unambiguous. Unlike younger women who must differentiate cancer from normal menstrual variations, post-menopausal bleeding has no benign explanation. This clarity accounts for the 69% of cases diagnosed at localized stage.
Important exception: Women on hormone replacement therapy may experience some bleeding. However, the American Cancer Society emphasizes that even HRT users should report any unexpected bleeding patterns to their healthcare provider immediately.
The 2026 data shows a concerning trend: while diagnosis rates remain highest in the 55-64 age group, rising obesity rates are shifting the disease younger, making age-appropriate vigilance essential across all demographics.
The 24-Hour Rule – When Uterine Cancer Symptoms Require Urgent Care
Not all symptoms demand immediate emergency care, but knowing which ones do could save your life. This evidence-based framework helps you distinguish between “schedule an appointment” and “go to the ER now.”
Emergency Symptoms (Seek Care Within 24 Hours)
Heavy, uncontrolled bleeding: Soaking through a pad or tampon every hour for 2+ consecutive hours represents a medical emergency. This blood loss can rapidly lead to dangerous anemia requiring transfusion.
Severe pelvic pain with fever: The combination suggests possible infection, tumor necrosis, or uterine perforation. According to CDC emergency guidelines, fever above 100.4°F with significant pelvic pain requires immediate evaluation.
Postmenopausal bleeding with large clots: While any post-menopausal bleeding warrants evaluation, passing clots larger than a quarter or experiencing continuous bleeding suggests advanced disease requiring urgent assessment.
Sudden onset severe abdominal pain: Sharp, intense pain that prevents normal activities could indicate tumor rupture, torsion, or other complications.
Checklist for emergency evaluation:
- ✓ Bleeding requiring pad change every 60 minutes
- ✓ Dizziness or fainting with bleeding
- ✓ Fever (>100.4°F) with pelvic pain
- ✓ Severe pain unrelieved by over-the-counter medication
- ✓ Passing clots larger than a golf ball
Urgent (Schedule Within 1 Week)
These symptoms don’t require emergency care but shouldn’t wait for your annual exam.
Any postmenopausal spotting: Even minimal bleeding—just enough to see on toilet paper—demands evaluation within one week. The National Comprehensive Cancer Network guidelines recommend endometrial biopsy for all postmenopausal bleeding.
Bleeding between periods for 2+ consecutive cycles: Persistent intermenstrual bleeding in pre-menopausal women requires investigation, especially if patterns worsen.
Persistent pelvic pain exceeding 2 weeks: Chronic pain lasting beyond normal menstrual patterns warrants gynecologic evaluation.
Foul-smelling vaginal discharge: Unusual odor accompanied by other symptoms increases cancer suspicion.
Non-Urgent (Schedule Within 2-4 Weeks)
Heavy periods with consistent pattern: If you’ve always had heavy periods without recent changes, schedule a routine evaluation rather than emergency care.
Chronic fatigue with other symptoms: When fatigue accompanies multiple warning signs, evaluation is necessary but not emergent.
Strong family history concerns: Women with Lynch syndrome or family history of gynecologic cancers should proactively discuss screening with their healthcare provider. Our Genetic Risk Assessment Tool can help you evaluate your hereditary risk profile.
The bottom line: Trust your instincts. If something feels wrong with your body, advocate for evaluation. Better to investigate a false alarm than delay cancer diagnosis by months.
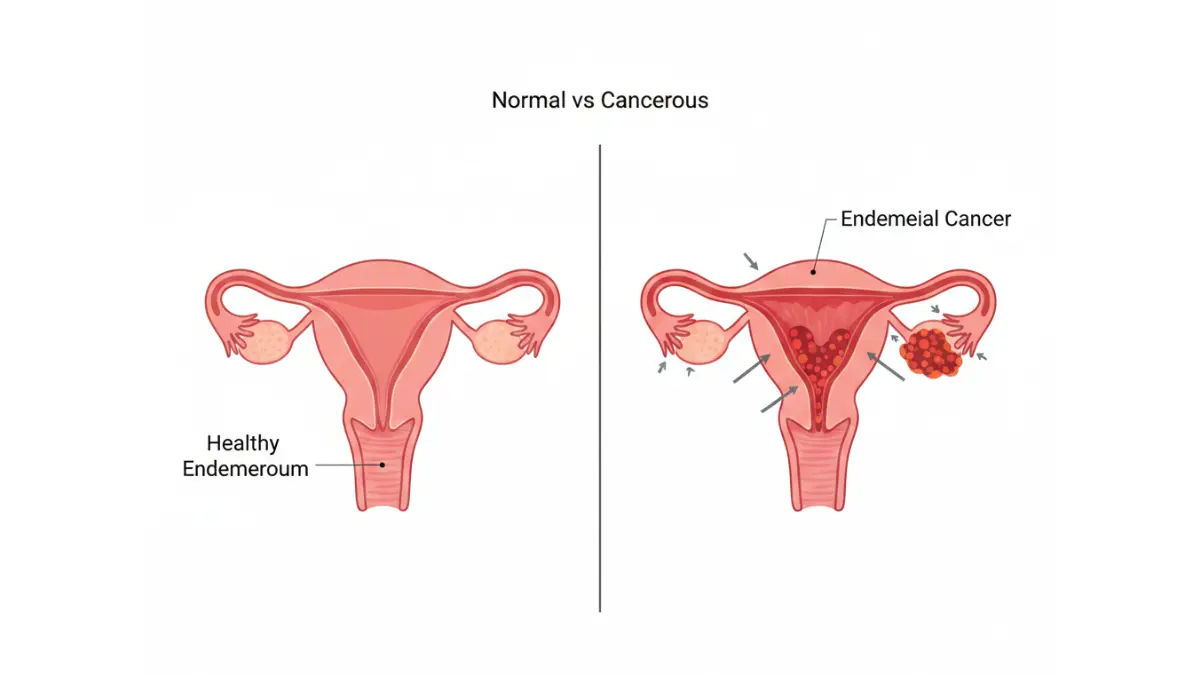
Uterine Cancer vs. Other Conditions – Know the Difference
Symptom overlap creates diagnostic confusion. Understanding key distinctions helps you communicate effectively with healthcare providers and ensures appropriate testing.
Uterine Cancer vs. Fibroids
Uterine fibroids—benign muscular tumors—affect up to 80% of women by age 50. Both conditions cause bleeding and pelvic pressure, but critical differences exist.
| Feature | Uterine Fibroids | Uterine Cancer |
|---|---|---|
| Age of onset | Typically 30s-40s | Usually 55+ (average 61) |
| Bleeding pattern | Heavy but cyclical | Progressive worsening, may be irregular |
| Pelvic pressure | Constant if large | Increases over time |
| Weight changes | Stable | Unexplained weight loss in advanced cases |
| Discharge | Normal appearance | May be watery, foul-smelling |
| Response to treatment | Improves with hormonal therapy | Symptoms persist despite treatment |
Critical point: Fibroids and cancer can coexist. “My ultrasound showed fibroids, so everyone assumed that explained my bleeding,” says Vanessa, 54. “Six months later, a biopsy revealed cancer behind the fibroids.”
Research from the American College of Obstetricians and Gynecologists emphasizes that post-menopausal women with presumed fibroids should undergo biopsy to rule out malignancy, as fibroids typically shrink after menopause while cancer grows.
Uterine Cancer vs. Endometriosis
Endometriosis causes tissue similar to uterine lining to grow outside the uterus, affecting approximately 10% of reproductive-age women.
Key differentiators:
Endometriosis produces cyclical pain that intensifies during menstruation. Cancer-related pain is typically non-cyclical and progressively worsens. Endometriosis predominantly affects women in their 20s-40s, while uterine cancer incidence peaks after 55.
“I’d lived with endometriosis for 20 years,” explains Monica, 49. “When pain became constant rather than cyclical, I knew something changed.” Her endometriosis history actually complicated diagnosis—healthcare providers initially attributed worsening symptoms to disease progression rather than investigating cancer possibility.
Diagnostic approach: Women with known endometriosis experiencing new symptom patterns—particularly bleeding after previous symptom stability or pain characteristics changing—require comprehensive re-evaluation including imaging and possible biopsy.
Uterine Cancer vs. Perimenopause
This distinction challenges even experienced clinicians because perimenopause naturally causes irregular bleeding patterns.
Perimenopause characteristics:
- Bleeding varies month to month (heavy one cycle, light the next)
- Hot flashes and night sweats accompany bleeding changes
- Symptoms fluctuate with hormonal shifts
- Gradual transition over several years
Cancer characteristics:
- Bleeding steadily worsens over weeks to months
- Discharge may develop unusual odor or appearance
- Symptoms don’t correlate with hormonal cycling
- Rapid progression rather than gradual change
According to National Institutes of Health research, the critical red flag is bleeding resuming after 12+ months without periods. “I thought perimenopause was just unpredictable,” admits Helen, 51. “When bleeding returned after 14 months without periods, my doctor immediately ordered tests.”
When to insist on testing: If you’re perimenopausal with bleeding concerns, request transvaginal ultrasound and endometrial assessment. The thickness of your uterine lining measured by ultrasound helps distinguish benign changes from potential malignancy. Don’t accept “it’s just perimenopause” without objective evaluation.
Women managing weight during perimenopause can use our Calorie Deficit Calculator to maintain healthy body composition, reducing one significant uterine cancer risk factor.
Who’s at Risk for Uterine Cancer? (2026 Risk Profile)
Understanding your personal risk profile empowers proactive monitoring and prevention strategies.
Major Risk Factors You Can’t Control
Age and hormonal exposure: While the average diagnosis age is 61, risk begins rising after 45. Women who started menstruating before age 12 or entered menopause after 55 experience prolonged estrogen exposure, increasing lifetime risk. Each additional year of menstruation adds incremental risk accumulation.
Genetic predisposition: Lynch syndrome, a hereditary condition, confers 40-60% lifetime uterine cancer risk. According to the National Cancer Institute, women with this mutation should consider prophylactic hysterectomy after completing childbearing.
Racial disparities: Black women face twice the mortality rate of white women despite similar incidence rates. CDC research attributes this to:
- Later-stage diagnosis (only 56% diagnosed at localized stage vs. 71% in white women)
- Higher prevalence of aggressive non-endometrioid subtypes
- Healthcare access barriers
- Less frequent guideline-concordant diagnostic evaluation
Nulliparity: Women who’ve never been pregnant face elevated risk. Pregnancy temporarily halts menstruation and alters hormonal profiles, providing protective effects. Multiple pregnancies confer greater protection than single pregnancy.
Modifiable Risk Factors
Obesity stands as the #1 controllable risk factor. Adipose tissue produces estrogen even after menopause, continuously stimulating endometrial growth. Research from Johns Hopkins shows that obesity increases uterine cancer risk 2-4 times compared to normal weight women.
“When my oncologist told me obesity was likely the biggest contributor to my cancer, I felt both guilty and empowered,” shares Linda, 57. “Guilty for not managing my weight earlier, but empowered knowing I could reduce my risk going forward.”
Weight management tools like our BMI Calculator and Weight Loss Calculator provide practical starting points for risk reduction.
Type 2 diabetes independently increases risk by 2-fold, even after controlling for obesity. Insulin resistance and hyperinsulinemia promote endometrial proliferation.
Hormone therapy patterns matter: Estrogen-only therapy (without progesterone) dramatically increases risk. Combined hormone therapy or no hormone therapy carries lower risk.
Tamoxifen, used for breast cancer treatment, acts as an estrogen agonist in the uterus. Women taking tamoxifen require vigilant monitoring for endometrial changes.
What This Means For You
Three actions to take today:
- Calculate your baseline weight and BMI using our measurement tools—knowing your starting point enables tracking meaningful changes
- Schedule annual gynecologic exams including discussion of family history and personal risk factors
- Document your complete family cancer history spanning three generations—this information guides screening intensity and timing
Women with multiple risk factors should discuss enhanced surveillance protocols with their gynecologist, potentially including annual endometrial assessment beginning at age 40-45 rather than waiting for symptoms.
Related resources on gynecologic health can be found in our comprehensive Health Tips section, including articles on cervical cancer symptoms and ovarian cancer warning signs.
Medical Disclaimer: This article is for educational purposes only and does not replace professional medical advice, diagnosis, or treatment. Always consult your healthcare provider regarding any medical concerns. If you experience symptoms described in this article, schedule an appointment with your gynecologist for proper evaluation.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.