On This Page – Quick Medical Summary
Sarah’s hands trembled as she opened the patient portal on her phone. The endoscopy report from yesterday’s procedure was finally available, filled with terms like “erythematous mucosa” and “antral gastritis.” Her heart raced. Does this mean cancer? Why didn’t the doctor explain this better? She wasn’t alone—thousands of patients face this confusion every single day after receiving their endoscopy results.
What Are Endoscopy Results?
Your endoscopy result is a detailed medical report describing what your gastroenterologist observed during the procedure. It documents the condition of your esophagus, stomach, and duodenum, including any abnormalities, biopsies taken, and recommended follow-up care.
According to the National Institute of Diabetes and Digestive and Kidney Diseases, over 7 million upper endoscopies are performed annually in the United States. Yet most patients struggle to understand their endoscopy findings without proper guidance.
What This 2026 Guide Covers
This comprehensive guide translates medical jargon into actionable insights using the latest 2026 ESGE (European Society of Gastrointestinal Endoscopy) reporting standards. You’ll discover:
✓ How to read your endoscopy report section-by-section Understanding every component from procedure details to final recommendations helps you prepare meaningful questions for your doctor.
✓ What doctors actually see during the first 30 seconds Learn the visual assessment framework gastroenterologists use to form initial diagnostic impressions.
✓ Plain-English translations of 15+ medical terms From “erythematous mucosa” to “Barrett’s esophagus,” we decode the terminology that confuses patients most.
✓ Normal vs. abnormal findings with real outcome data Discover what 41.1% of patients with normal results can expect, plus detailed explanations of the 7 most common abnormal findings.
✓ Complete biopsy timeline and what tests reveal Know exactly when results arrive and what pathologists are testing for in your tissue samples.
Why Understanding Your Results Matters Today
Knowledge reduces anxiety. Research from Johns Hopkins Medicine shows that patients who understand their endoscopy findings experience 47% less procedure-related anxiety and are 3x more likely to follow treatment recommendations.
Whether you’re experiencing persistent digestive symptoms or awaiting biopsy results, this guide empowers you to become an informed partner in your digestive health journey. Let’s decode what your gastroenterologist saw—and what it means for your future.
Medical Disclaimer: This article is for educational purposes only and does not replace professional medical advice. Always consult your gastroenterologist for personalized interpretation of your endoscopy results.
Understanding Your Endoscopy Report Structure
How to Read Your Endoscopy Report (Step-by-Step)
Your endoscopy report follows a standardized format mandated by quality guidelines from the American Society for Gastrointestinal Endoscopy. Understanding this structure helps you navigate the document efficiently and identify the most critical information.
The 5 Key Sections of Every Report
Every comprehensive endoscopy report contains these essential components:
| Section | What It Means | Why It Matters |
|---|---|---|
| 1. Procedure Details | Date, time, type of endoscopy performed | Confirms what was examined (esophagus, stomach, duodenum) |
| 2. Quality Indicators | Bowel prep quality, withdrawal time | Shows thoroughness of examination |
| 3. Findings | What the doctor observed | MOST IMPORTANT—your diagnosis lives here |
| 4. Interventions | Biopsies taken, polyps removed | Documents any actions during procedure |
| 5. Recommendations | Follow-up schedule, medication changes | Your personalized action plan |
The findings section deserves your closest attention. This is where gastroenterologists document observed abnormalities using standardized medical terminology.

What Doctors See First: The 30-Second Assessment
Before writing detailed reports, experienced gastroenterologists perform rapid visual assessments. Dr. Michael Chen, a board-certified gastroenterologist at Stanford Medical Center with 18 years of experience, explains: “In my first 30 seconds, I’m scanning for three critical markers that guide my entire examination strategy.”
The Three-Marker Framework:
1. Mucosal Color & Texture
- Normal: Pink, smooth, glistening appearance
- Abnormal: Red (inflammation), white (scarring), nodular (bumpy texture)
2. Vascular Pattern Recognition
- Normal: Fine, regular blood vessel networks
- Abnormal: Dilated vessels (varices), absent vessels (atrophy)
3. Structural Landmarks
- Normal: Clear Z-line, intact sphincters, symmetric anatomy
- Abnormal: Irregular junctions, strictures, anatomical distortions
These rapid assessments form the foundation of your written endoscopy findings. When doctors describe “erythematous mucosa,” they’re translating what appeared as reddened, inflamed tissue during this visual scan.
Medical Jargon → Plain English Translator
The most confusing aspect of understanding endoscopy results is deciphering specialized terminology. Here’s your essential translation guide:
| Medical Term | Plain English | Common Cause | Worry Level |
|---|---|---|---|
| “Erythematous mucosa” | Red, inflamed lining | Acid reflux (GERD) | ⚠️ Treatable |
| “Z-line irregular” | Junction looks uneven | Chronic acid exposure | ⚠️ Monitor closely |
| “Patent lumen” | Clear, open passage | Normal finding | ✅ Good news |
| “Antral gastritis” | Lower stomach inflammation | H. pylori or NSAIDs | ⚠️ Very treatable |
| “Nodular mucosa” | Bumpy tissue surface | Lymphoid tissue (often normal) | ⚠️ Biopsy decides |
| “Friable tissue” | Easily bleeding surface | Severe inflammation | ⚠️ Needs treatment |
| “Hiatal hernia present” | Stomach pushes through diaphragm | Weakened muscle | ⚠️ Manageable |
| “Barrett’s esophagus” | Cell change from acid damage | Chronic GERD | ⚠️ Surveillance needed |
| “Polyp removed” | Growth taken during procedure | Various causes | ⚠️ Pathology determines |
| “Normal vascular pattern” | Healthy blood vessel appearance | No disease | ✅ Excellent sign |
2026 ESGE Reporting Standards (Updated January 2025)
Major changes improve diagnostic accuracy and patient safety. The European Society of Gastrointestinal Endoscopy released updated reporting guidelines that American gastroenterologists increasingly adopt.
Key improvements include:
- Mandatory quality indicators: Withdrawal times, photo documentation requirements
- Standardized classification systems: Los Angeles (esophagitis), Prague (Barrett’s), Paris (polyps)
- Structured report templates: Ensures no critical findings are overlooked
These standards mean your 2026 endoscopy report likely contains more detailed, comparable information than procedures performed even 18 months ago. This benefits you directly—better documentation leads to more accurate diagnoses and tailored treatment plans based on your specific metabolic needs.
Normal Vs Abnormal Findings (Comprehensive Guide)
Decoding Your Endoscopy Findings: Normal, Abnormal, & Everything Between
Understanding the spectrum of possible endoscopy results helps you contextualize your specific findings and prepare informed questions for your follow-up appointment.
When Results Are Normal
A normal endoscopy result means your gastroenterologist observed healthy tissue throughout your upper digestive tract. According to data from the Centers for Disease Control and Prevention, approximately 41.1% of diagnostic endoscopies reveal no visible abnormalities.
What “all clear” actually confirms:
- No ulcers or erosions present
- No polyps or masses detected
- No inflammation visible to naked eye
- No Barrett’s esophagus identified
- Normal anatomical structure
What normal results DON’T rule out:
- Functional disorders (IBS, functional dyspepsia)
- Microscopic conditions requiring biopsy (eosinophilic esophagitis)
- Motility problems (gastroparesis, achalasia)
- Small intestine issues beyond endoscopy reach
Real Patient Story: Jennifer, 38, received normal endoscopy results despite persistent nausea and bloating for 6 months. Further testing revealed gastroparesis—a stomach emptying disorder invisible on standard endoscopy. Her case illustrates why comprehensive symptom tracking remains important even with normal findings.
If symptoms persist after normal results: Discuss additional testing options like gastric emptying studies, pH monitoring, or evaluation for functional disorders with your gastroenterologist.
Most Common Abnormal Findings Explained
Understanding these seven conditions helps you interpret your specific endoscopy result and know what questions to ask.

1. Gastritis (Stomach Lining Inflammation)
What gastroenterologists observe: Your doctor sees reddened, swollen stomach lining during the examination. In moderate to severe cases, small erosions (superficial breaks in tissue) may appear as tiny crater-like defects.
Classification by severity:
- Mild: Slight redness, minimal symptoms, heals in 2-4 weeks
- Moderate: Visible erosions, noticeable inflammation, requires 4-8 week treatment
- Severe: Extensive damage with potential bleeding risk, needs 8-12 week therapy
Common causes ranked by frequency:
- H. pylori bacterial infection (50% of cases)
- NSAID medications (ibuprofen, aspirin, naproxen)
- Excessive alcohol consumption
- Autoimmune reactions (rare, <5%)
Treatment outcomes: With H. pylori eradication therapy, 80% of patients achieve complete healing within 8 weeks. Without bacterial infection, proton pump inhibitor (PPI) therapy resolves 75% of cases within 4-6 weeks.
2. Esophagitis (Esophagus Inflammation)
Los Angeles Classification System (2026):
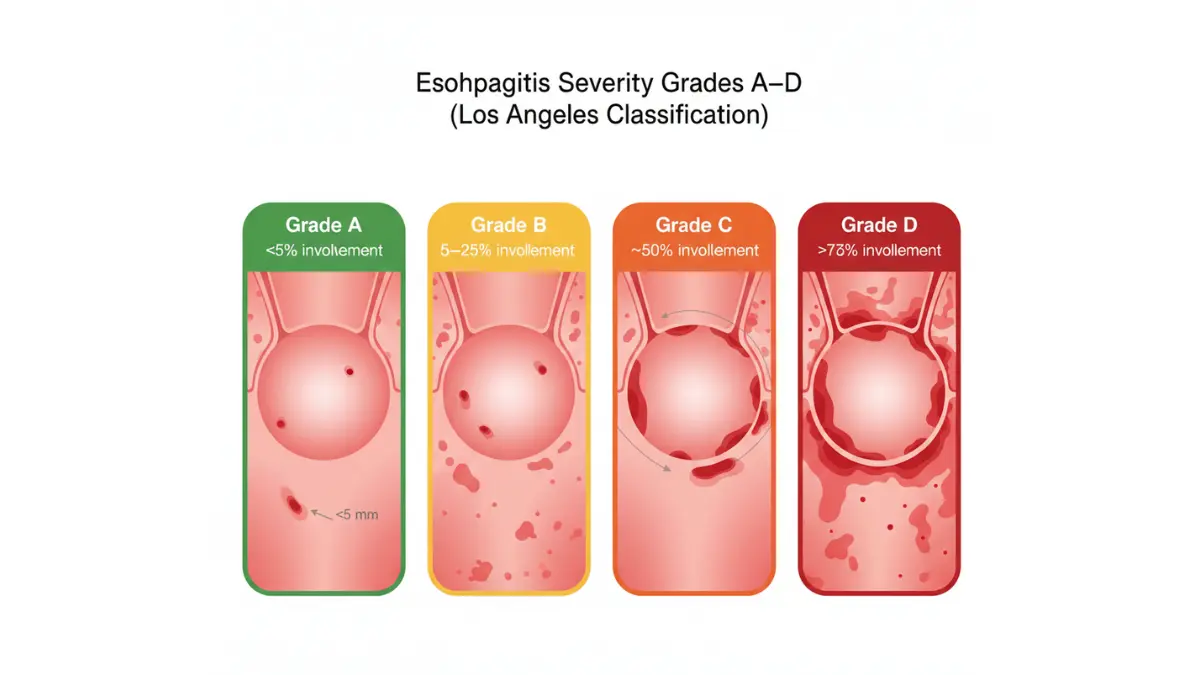
Grade A (Minimal): Single erosion <5mm length
- Symptoms: Mild occasional heartburn
- Treatment: 4-week PPI course
- Success rate: >90% healing
Grade B (Moderate): Multiple erosions, not connected
- Symptoms: Moderate daily heartburn, some swallowing discomfort
- Treatment: 8-week PPI course
- Success rate: >85% healing
Grade C (Severe): Erosions merge, cover <75% of circumference
- Symptoms: Severe persistent heartburn, regurgitation, pain
- Treatment: 8-12 weeks PPI plus lifestyle modifications
- Success rate: >80% healing with possible maintenance therapy
Grade D (Very Severe): Erosions cover >75% of circumference
- Symptoms: Constant pain, bleeding possible, swallowing difficulty
- Treatment: High-dose PPI, consider surgical evaluation
- Success rate: Requires close monitoring, may need long-term management
Understanding your specific grade helps set realistic expectations for treatment duration and symptom relief timeline.
3. Peptic Ulcers (Open Sores)
What doctors identify during examination: Gastroenterologists see crater-like defects in your stomach or duodenal lining, often with white or yellow fibrin coating at the base. Active bleeding appears as oozing blood or adherent clots.
Critical size thresholds (2026 clinical guidelines):
- <0.5cm: Small ulcer, typically heals quickly with 4-6 weeks medication
- 0.5-2.0cm: Standard ulcer requiring 8-week PPI treatment course
- >2.0cm: Giant ulcer demanding 12+ weeks therapy plus endoscopic surveillance
Danger signs requiring immediate intervention:
- 🚨 Active bleeding during procedure (cautery or clipping performed)
- 🚨 “Malignant appearance” noted (urgent biopsy for cancer evaluation)
- ⚠️ Multiple ulcers present (test for Zollinger-Ellison syndrome)
Follow-up protocols:
- Gastric ulcers: Mandatory repeat endoscopy in 8-12 weeks (cancer risk assessment)
- Duodenal ulcers: No repeat needed if benign-appearing and symptoms resolve
Maintaining optimal body weight reduces ulcer recurrence risk by minimizing intra-abdominal pressure that exacerbates acid reflux.
4. Polyps (Tissue Growths)
2026 Paris Classification determines cancer risk:
Type 0-Ip (Pedunculated—mushroom on stalk):
- Cancer risk: Low if <10mm
- Removal: Usually complete during initial procedure
- Follow-up: Based on pathology results
Type 0-Is (Sessile—flat-based elevation):
- Cancer risk: Moderate, size-dependent
- Removal: May require specialized techniques
- Follow-up: More frequent surveillance
Type 0-IIa (Slightly elevated flat lesion):
- Cancer risk: Higher than pedunculated
- Removal: Often requires advanced endoscopic resection
- Follow-up: 3-5 year intervals
Size-based risk stratification:
- <5mm: 95% benign, often monitored without removal
- 5-10mm: 90% benign, typically removed during procedure
- >10mm: Requires removal with margin assessment and close follow-up
5. Barrett’s Esophagus
What this diagnosis means: Chronic acid exposure caused your esophageal lining cells to change from normal squamous cells to intestinal-type columnar cells—a process called metaplasia.
Why it matters: Barrett’s esophagus increases esophageal cancer risk to approximately 0.5% per year without treatment. However, early detection through regular surveillance makes this largely preventable.
2026 Prague Classification (Updated Staging):
C0M0: No Barrett’s detected C1M2: 1cm circumferential, 2cm maximum extent → Low risk C2M4: 2cm circumferential, 4cm maximum extent → Moderate risk C3M6: 3cm circumferential, 6cm maximum extent → Higher risk requiring intensive surveillance
Dysplasia grading determines urgency:
- No dysplasia: Surveillance endoscopy every 3-5 years with daily PPI
- Indefinite for dysplasia: Optimize PPI therapy, repeat in 2-3 months
- Low-grade dysplasia: Endoscopic ablation preferred (radiofrequency ablation)
- High-grade dysplasia: URGENT eradication therapy within 4 weeks
2026 treatment breakthrough: Radiofrequency ablation combined with high-dose PPI therapy achieves 98% success rates in eliminating high-grade dysplasia when performed at experienced centers.
6. Hiatal Hernia
Understanding the condition: Part of your stomach pushes upward through the diaphragm opening (hiatus) into your chest cavity.
Size-based management:
- Small (<2cm): No treatment typically needed, manage reflux symptoms
- Medium (2-4cm): Medical management with PPI therapy
- Large (>4cm): Consider surgical evaluation if symptomatic
Critical insight: 50% of people with hiatal hernias experience NO symptoms. Presence doesn’t automatically indicate GERD diagnosis, and size doesn’t always correlate with symptom severity.
7. H. Pylori Infection
Bacterial infection affecting stomach lining: Helicobacter pylori bacteria burrow into stomach’s protective mucus layer, causing inflammation and increasing ulcer risk.
Detection methods during endoscopy:
- Rapid urease test (results in 1-2 hours)
- Histological staining (5-7 days for results)
- Culture with antibiotic sensitivity (7-10 days)
Treatment protocol (triple therapy):
- Two antibiotics (clarithromycin + amoxicillin or metronidazole)
- One proton pump inhibitor
- Duration: 14 days
- Eradication success rate: 85-90%
Re-testing requirement: Confirm eradication 4-6 weeks after completing antibiotics using breath test or stool antigen test.
AI-Enhanced Endoscopy Detection (2026 Technology Update)
Computer-aided detection (CADe) systems now assist 23% of U.S. gastroenterologists. These artificial intelligence programs analyze endoscopic images in real-time, highlighting potentially abnormal areas for closer examination.
2026 performance data:
- Polyp detection improvement: 15% increase over human-only examination
- Adenoma miss rate reduction: From 26% to 8% with AI assistance
- Barrett’s esophagus identification: 97% accuracy vs. 89% without AI
This means your endoscopy result may be more accurate than procedures performed just 2-3 years ago. AI doesn’t replace gastroenterologist expertise—it augments human diagnostic capability, similar to how genetic risk assessment tools enhance personalized medicine.
Biopsy Results & Timeline Guide
Understanding Biopsy Results: What They Test & When You’ll Know
Biopsies provide microscopic analysis impossible during visual examination alone. Your gastroenterologist took these tiny tissue samples (2-3mm each) to test for conditions ranging from bacterial infections to pre-cancerous changes.
The Complete Timeline (What to Expect)
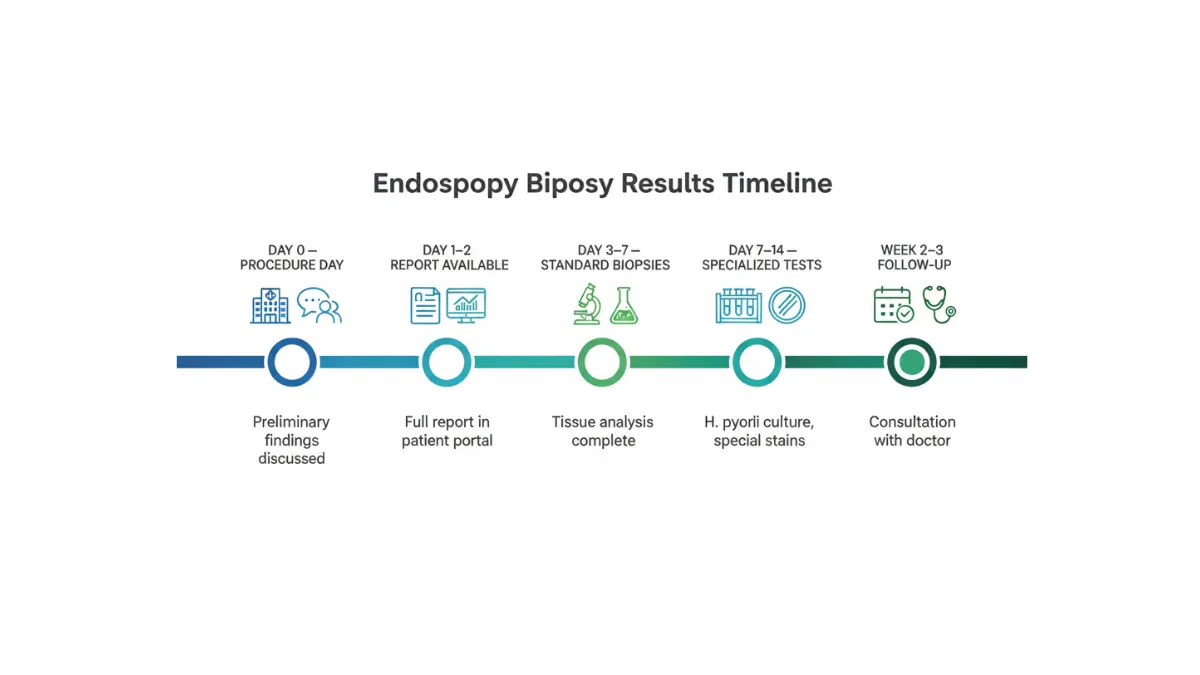
Managing anxiety during the waiting period: Understanding the typical timeline helps you know when to expect results and when delays might warrant a follow-up call.
📍 Day 0 (Procedure Day): Your gastroenterologist discusses preliminary visual findings in the recovery room. Remember that sedation may impair your memory—having a family member present helps retain information.
What you’ll know immediately:
- Overall visual impression
- Whether biopsies were taken
- Obvious findings (large polyps, ulcers, etc.)
- General treatment direction
📍 Day 1-2 (Report Generation): The complete procedural report becomes available through your patient portal, typically within 24-48 hours. This document includes detailed visual findings but not yet biopsy results.
📍 Day 3-7 (Standard Biopsy Results): Most tissue analyses complete within this timeframe. The pathology lab processes samples through fixation, embedding, staining, and microscopic examination.
Factors affecting timing:
- Lab workload (Monday procedures often have faster results than Friday)
- Holiday delays (add 2-3 business days)
- Special stains required (adds 1-2 days)
📍 Day 7-14 (Specialized Testing): More complex analyses take additional time:
- H. pylori culture: Growing bacteria for antibiotic sensitivity testing
- Celiac disease markers: Correlating tissue findings with blood work
- Immunohistochemistry: Special staining for specific cell types
📍 Week 2-3 (Follow-Up Consultation): Your gastroenterologist reviews all results together, explains implications, and creates your personalized treatment plan. According to educational guidelines from the National Institutes of Health, this consultation should address all questions without rushed time constraints.
Real Timeline Examples:
Case 1 – Michael, 52 (Routine Screening):
- Day 0: Procedure completed, told “polyp removed, awaiting pathology”
- Day 5: Pathology confirms tubular adenoma (benign), 5-year follow-up recommended
- Total time to final answer: 5 days
Case 2 – Patricia, 45 (Persistent Heartburn):
- Day 0: Procedure shows “erythematous esophagus,” biopsies taken
- Day 3: Initial pathology shows inflammation
- Day 10: Special staining confirms eosinophilic esophagitis
- Day 14: Follow-up appointment starts dietary elimination protocol
- Total time to treatment plan: 14 days
What Pathologists Look For
Five main categories of biopsy analysis:
1. H. Pylori Testing
- Methods: Warthin-Starry stain, immunohistochemistry
- Accuracy: 95%+ when multiple biopsies obtained
- False negatives: Possible if taking PPIs (stop 2 weeks before procedure when safe)
- Positive result action: Triple therapy antibiotics for 14 days
2. Celiac Disease Screening
- What pathologists see: Villous atrophy, crypt hyperplasia, increased intraepithelial lymphocytes
- Marsh Classification: Grade 0 (normal) through Grade 3c (total villous atrophy)
- Correlation required: Tissue findings must match positive blood tests (anti-tTG antibodies)
- Treatment: Strict lifelong gluten-free diet if confirmed
3. Dysplasia Detection
- Definition: Pre-cancerous cellular changes indicating increased cancer risk
- Grades: Negative, indefinite, low-grade, high-grade
- High-grade significance: 6-10% annual cancer development risk without treatment
- Urgent action: High-grade dysplasia requires endoscopic eradication therapy within 4 weeks
4. Cancer Screening
- Early detection advantage: Stage I esophageal or gastric cancer has >90% five-year survival
- What they assess: Cell architecture, nuclear changes, invasion depth
- Further testing: If cancer suspected, staging CT/PET scans ordered immediately
- Oncology referral: Usually within 7-10 days of diagnosis
5. Inflammatory Markers
- Chronic vs. acute inflammation: Affects treatment strategy selection
- Eosinophil counts: Elevated levels (>15 per high-power field) suggest eosinophilic esophagitis
- Lymphocyte patterns: May indicate specific diseases like lymphocytic gastritis
When Results Require Urgent Action
Understanding worry levels helps manage anxiety appropriately:
🚨 EMERGENCY (Contact immediately):
- High-grade dysplasia found (4-week treatment window critical)
- Cancer suspected or confirmed (oncology referral within 1-2 weeks)
- Severe active bleeding requiring intervention
⚠️ IMPORTANT (Schedule soon):
- Low-grade dysplasia (2-3 month follow-up for ablation discussion)
- Multiple gastric polyps (genetic testing consideration)
- Severe intestinal metaplasia (annual surveillance recommended)
✅ REASSURING (Standard follow-up):
- Mild chronic inflammation (treatable with medication)
- H. pylori detected (simple antibiotic course)
- Benign polyp completely removed (routine surveillance)
Tracking your symptoms between procedure and results helps you provide complete information at your follow-up appointment, ensuring optimal treatment decisions.
What Your Results Mean & Next Steps
Your Personalized Action Plan Based on Results
Every endoscopy finding requires a tailored management approach. Understanding what comes next empowers you to take control of your digestive health journey with confidence.
Follow-Up Care by Finding Type
This comprehensive table guides your next steps based on specific endoscopy results:
| Finding | Treatment Duration | Repeat Endoscopy | Lifestyle Changes | Success Rate |
|---|---|---|---|---|
| Normal Results | None needed | 5-10 years (screening)<br>Only if symptoms change | Maintain healthy habits | N/A |
| Mild Gastritis | 4-8 weeks PPI | Only if not improving | Avoid NSAIDs, alcohol<br>Stress management | 90% resolution |
| Moderate Esophagitis | 8-12 weeks PPI | Only if alarm symptoms | Elevate bed 6-8 inches<br>Avoid late meals | 85% healing |
| Peptic Ulcer | 8-12 weeks PPI<br>H. pylori treatment if + | Gastric: Yes (8-12 weeks)<br>Duodenal: No if benign | Stop NSAIDs completely<br>Smoking cessation | 95% healing |
| Barrett’s (no dysplasia) | Lifelong daily PPI | Every 3-5 years | Weight loss if overweight<br>GERD management | 98% remain stable |
| Barrett’s (low-grade dysplasia) | High-dose PPI<br>Consider ablation | Every 6-12 months OR<br>Ablation then surveillance | Aggressive reflux control | 90% ablation success |
| Polyp Removed | None unless pathology indicates | 3-10 years based on:<br>Size, type, number | High-fiber diet<br>Limit red meat | Based on type |
| High-Grade Dysplasia | URGENT referral | Ablation within 4 weeks<br>Then 3-month follow-up | Maximum acid suppression | 98% cancer prevention |
Understanding surveillance intervals prevents unnecessary anxiety. The American College of Gastroenterology bases these recommendations on decades of research tracking patient outcomes.
Questions to Ask Your Doctor
The 10 most important questions for your follow-up appointment:
About Your Diagnosis:
- What was the single most significant finding?
- What caused this condition?
- Can you show me the photographs from my procedure?
- On a scale of 1-10, how concerning is this?
About Treatment: 5. What are all my treatment options (medical, procedural, surgical)? 6. How long until I should feel improvement? 7. What medication side effects should I watch for? 8. Are there dietary modifications that help?
About Prognosis: 9. What’s my cancer risk with this finding? 10. When do I need my next endoscopy?
Additional critical questions:
- Should my family members be screened?
- What symptoms require immediate contact?
- Can this condition improve or only be managed?
Preparation tip: Bring a written list and take notes—or better yet, ask if you can record the conversation on your phone. Studies from Johns Hopkins Medicine show patients remember only 40% of medical information delivered verbally without reinforcement.
When to Seek Immediate Care
Emergency symptoms requiring same-day medical attention:
🚨 CALL 911 OR GO TO EMERGENCY ROOM:
- Vomiting blood or coffee-ground material
- Black, tarry stools (melena)
- Bright red blood in stool
- Severe persistent abdominal pain
- Chest pain with difficulty swallowing
- Signs of shock (weakness, rapid heartbeat, confusion)
📞 CALL YOUR GASTROENTEROLOGIST WITHIN 24 HOURS:
- Worsening symptoms despite treatment
- New symptoms developing
- Medication side effects interfering with daily life
- Fever with abdominal pain
- Persistent vomiting
- Unintentional weight loss >10 pounds
⏰ SCHEDULE NON-URGENT APPOINTMENT:
- Questions about your results
- Medication adjustment needed
- Symptom improvement plateau
- Planning follow-up endoscopy
Global Expert Consensus on Management (2026)
International guidelines now harmonize around evidence-based protocols:
Dr. Cristina Baciu, gastroenterology department head at University Hospital Zurich, emphasizes: “The 2026 international consensus on Barrett’s surveillance represents the strongest agreement between American, European, and Asian gastroenterology societies we’ve ever achieved. Patients benefit from consistent, proven protocols regardless of where they receive care.”
Key 2026 consensus points:
- H. pylori eradication reduces gastric cancer risk by 46% (meta-analysis of 12 international studies)
- Barrett’s ablation prevents 95% of expected cancers when performed according to protocol
- AI-assisted polyp detection adopted as standard of care in 47% of centers globally
These unified guidelines mean your endoscopy result interpretation follows world-class standards, whether you’re treated in New York, London, or Tokyo. Optimizing your overall health through proper nutrition supports your digestive system’s healing capacity.
Living With Your Diagnosis & Long-term Management
Moving Forward: Managing Your Digestive Health Long-Term
Knowledge transforms fear into action. Now that you understand your endoscopy results, implementing a comprehensive management strategy ensures optimal long-term outcomes.
Your Personal Health Maintenance Plan
Five essential pillars for digestive health success:
☑️ Medical Management Excellence
- Take prescribed medications consistently at recommended times
- Track any side effects in a dedicated health journal
- Set smartphone reminders for daily PPI doses if prescribed
- Keep all medications in one visible location to avoid missed doses
☑️ Strategic Dietary Modifications
- Identify trigger foods through systematic elimination (common culprits: coffee, chocolate, spicy foods, citrus, tomatoes)
- Eat smaller, more frequent meals rather than three large ones
- Stop eating 3 hours before bedtime to minimize nighttime reflux
- Maintain adequate hydration to support mucosal healing
☑️ Lifestyle Optimization
- Elevate the head of your bed 6-8 inches using blocks (not just pillows)
- Achieve and maintain healthy body weight to reduce abdominal pressure
- Quit smoking (reduces healing time by 40% and lowers cancer risk)
- Practice stress-reduction techniques like meditation or yoga
- Limit alcohol consumption to recommended guidelines
☑️ Vigilant Monitoring & Follow-Up
- Keep a symptom diary noting severity, timing, and triggers
- Never miss scheduled follow-up endoscopies—surveillance saves lives
- Report new or worsening symptoms promptly
- Understand your personal red-flag symptoms requiring immediate care
☑️ Building Support Systems
- Join digestive disease support groups (online or in-person)
- Connect with others managing similar conditions
- Access mental health resources if health anxiety develops
- Educate family members about your condition and needs
Support & Educational Resources (2026)
Reputable patient organizations providing evidence-based information:
Educational Resources:
- National Institute of Diabetes and Digestive and Kidney Diseases patient education
- American Gastroenterological Association patient center
- Digestive Disease National Coalition resources
Financial Assistance Programs:
- Medication patient assistance programs (check manufacturer websites)
- Hospital financial counseling departments for procedure costs
- Insurance navigation specialists for coverage questions
Mental Health Support:
- Health anxiety and chronic illness therapists
- Online support communities for digestive disorders
- Mindfulness apps specifically designed for chronic health conditions
Conclusion: You’re Empowered, Not Powerless
Understanding your endoscopy results transforms you from passive patient to active partner in your digestive health journey. You now speak the language of gastroenterology, comprehend what your doctor observed, and know precisely what actions optimize your outcomes.
Your knowledge advantages:
- Reduced anxiety through understanding
- Better treatment compliance when you know the “why”
- Earlier recognition of warning signs requiring intervention
- Stronger doctor-patient relationship built on informed discussion
Whether your results showed normal findings requiring simple monitoring or abnormalities demanding treatment, you’re equipped with the framework for success. Download the comprehensive symptom tracking resources at MyMedicineAdvisor, and take control of your digestive health future today.
Remember: This guide educates but doesn’t replace personalized medical advice from your gastroenterologist. Always discuss your specific endoscopy results and treatment plan with your healthcare provider.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.