On This Page – Quick Medical Summary
What PT/INR Test Results Actually Mean (Your Numbers Decoded)
Rowan Westbrook checked his phone during lunch. His doctor’s portal showed a new lab result: “INR: 3.7.” His heart raced. Too high? Too low? Dangerous?
Here’s what you need to know immediately: PT/INR test results measure how long your blood takes to clot. A PT/INR test is critical for anyone on blood thinners like warfarin, with results typically ranging from 0.8 to 5.0 or higher. Your specific number tells doctors if your anticoagulation therapy is working correctly—or if adjustments are needed urgently.
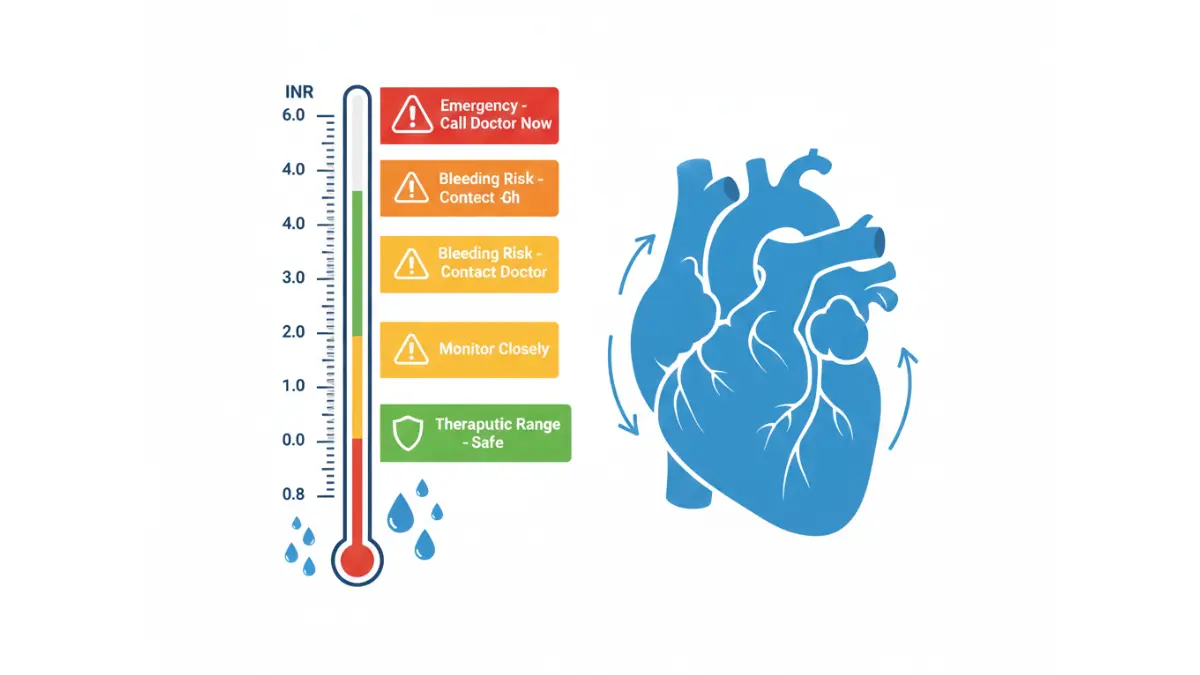
Quick INR Interpretation (2026 Standards):
| INR Range | What It Means | Action Needed |
|---|---|---|
| 0.8-1.2 | Normal (not on blood thinners) | Routine monitoring |
| 1.5-2.0 | Below therapeutic target | Contact doctor within 24-48 hours |
| 2.0-3.0 | Therapeutic for DVT, AFib, PE | Continue current dose |
| 3.0-4.0 | Therapeutic for mechanical valves | Weekly monitoring |
| 4.0-5.0 | High bleeding risk | Same-day doctor contact |
| Above 5.0 | Emergency territory | Call doctor immediately |
For Rowan, his 3.7 meant he needed same-day contact with his cardiologist—not an emergency, but requiring prompt attention.
Why Your PT/INR Results Matter Right Now:
Your INR levels directly impact bleeding and clotting risks. Too low, and dangerous blood clots can form in your legs, lungs, or brain. Too high, and internal bleeding becomes a serious concern—similar to how blood sugar readings guide diabetes management with immediate treatment implications.
According to the CDC’s anticoagulation monitoring data, approximately 2-3 million Americans take warfarin, making PT/INR one of the most frequently ordered blood tests in the United States. Understanding what your specific number means can prevent life-threatening complications.
What you’ll learn in the next 4 minutes:
- Exact interpretation of every INR number from 1.5 to 5.0
- When to call your doctor versus when to go to the ER
- Why your INR fluctuates and how to stabilize it
- 2026 home monitoring options and their accuracy
Understanding The Science
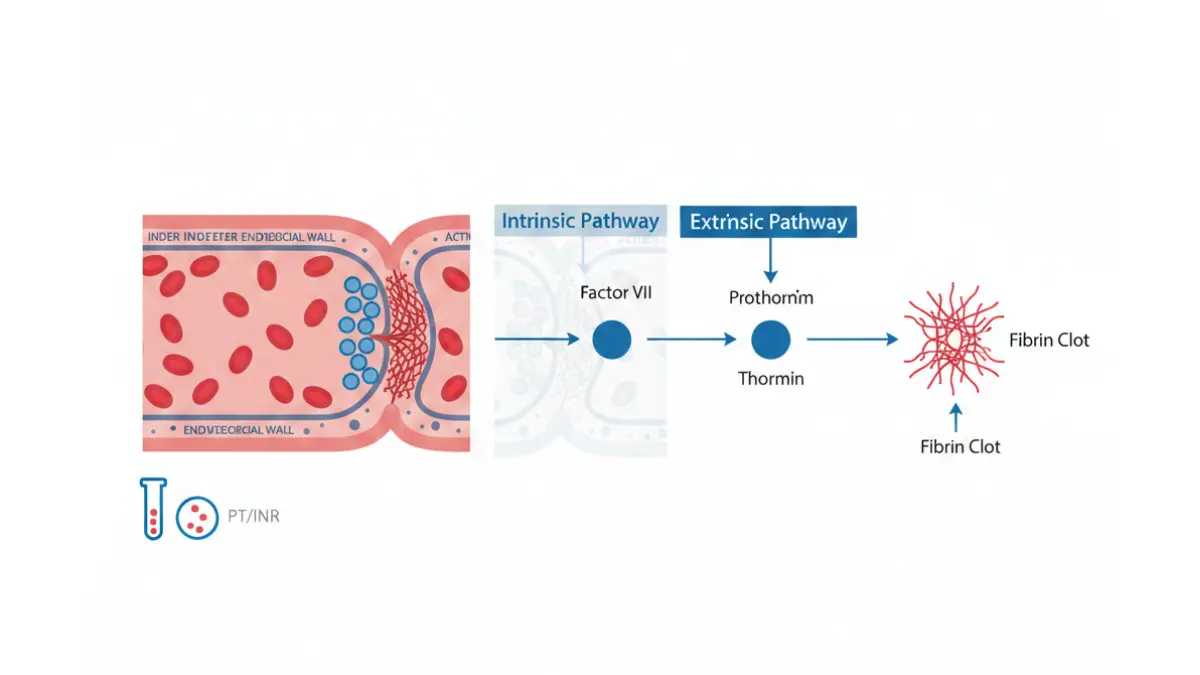
How PT/INR Testing Works (The Blood Clotting Process Explained)
What Is Prothrombin Time? (The 13-Second Standard)
Prothrombin time measures how many seconds your blood takes to form a clot. Normal PT ranges from 11 to 13.5 seconds for people not taking anticoagulants. When you take warfarin or similar medications, your PT intentionally increases—making your blood clot more slowly to prevent dangerous clots.
Think of blood clotting like a construction team building a wall. Normally, the team works at full speed (11-13 seconds). Blood thinners slow down the crew, taking 20-40 seconds or longer to complete the same wall. This delay prevents unwanted “construction” (clots) in the wrong places.
Why INR Was Created (International Standardization)
Different labs use different testing reagents, making PT results vary between facilities. The International Normalized Ratio (INR) was introduced in 1983 to standardize results globally. Your INR of 2.5 in New York means the same as an INR of 2.5 in London—crucial for consistent anticoagulation monitoring.
The National Heart, Lung, and Blood Institute explains that INR calculations account for laboratory variations, giving doctors a reliable number for warfarin dosing decisions.
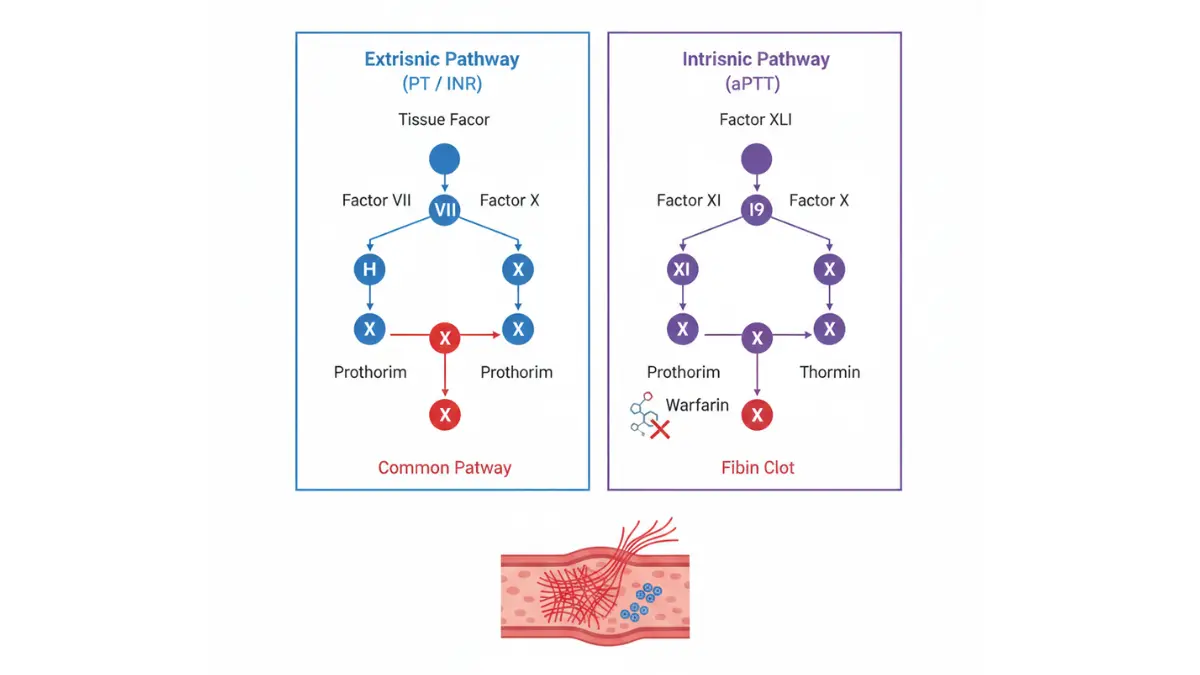
PT vs INR vs aPTT: Key Differences
| Test | What It Measures | Primary Use | Normal Range |
|---|---|---|---|
| PT | Extrinsic clotting pathway | Warfarin monitoring | 11-13.5 seconds |
| INR | Standardized PT ratio | Warfarin dosing | 0.8-1.2 (no meds) |
| aPTT | Intrinsic clotting pathway | Heparin monitoring | 25-35 seconds |
2026 Testing Technology Update:
Point-of-care INR devices now achieve 95-97% accuracy compared to laboratory testing, according to FDA validation data. Devices like CoaguChek and Alere deliver results in 60-90 seconds from a fingerstick sample—revolutionizing home anticoagulation management for patients requiring frequent monitoring.
Understanding these differences helps you interpret results from coagulation test panels that often include multiple clotting measurements beyond just PT/INR values.
Interpreting Your Specific Results
What Your PT/INR Numbers Mean (Range-by-Range Breakdown)
INR 0.8-1.2: Not on Blood Thinners (Normal Baseline)
This range represents normal blood clotting for individuals not taking anticoagulants. Your blood clots at the expected speed, providing natural protection against excessive bleeding while preventing unwanted clot formation.
What to do: Routine annual checkups. No immediate action needed unless testing was ordered for specific clotting concerns.
INR 1.5-2.0: Below Therapeutic Range (Subtherapeutic)
If you’re taking warfarin for conditions like deep vein thrombosis or atrial fibrillation, this range indicates inadequate anticoagulation. Your blood is clotting faster than intended, increasing stroke and clot risks.
Real Case: Jennifer Martinez’s INR dropped to 1.7 after starting a vitamin K-rich diet. Her hematologist increased her warfarin dose from 5mg to 6mg daily, retesting in five days until her INR stabilized at 2.4.
Action steps:
- Contact your doctor within 24 hours
- Don’t double-dose without medical guidance
- Avoid vitamin K-rich foods temporarily
- Retest in 3-5 days after dose adjustment
INR 2.0-3.0: Therapeutic for Most Conditions
This is the target range for 85% of patients on warfarin therapy, including those with DVT, pulmonary embolism, and non-valvular atrial fibrillation. You’re achieving the perfect balance—preventing clots without excessive bleeding risk.
Condition-Specific Targets:
| Condition | Target INR | Monitoring Frequency |
|---|---|---|
| DVT/PE (first 3 months) | 2.0-3.0 | Weekly initially |
| Atrial Fibrillation | 2.0-3.0 | Monthly when stable |
| Recurrent DVT | 2.5-3.5 | Every 2-4 weeks |
Action steps:
- Continue current warfarin dose
- Maintain consistent vitamin K intake
- Monthly INR checks if stable for 3+ months
- Report unusual bleeding or bruising
INR 3.0-4.0: Higher Therapeutic Range (Mechanical Heart Valves)
Patients with mechanical heart valves require higher anticoagulation due to increased thrombotic risk from artificial valve surfaces. According to American Heart Association 2026 guidelines, bileaflet mechanical aortic valves typically target INR 2.5-3.5, while mitral valves need 3.0-4.0.
Action steps:
- Weekly monitoring recommended
- Watch for bleeding symptoms (gum bleeding, easy bruising, blood in urine)
- Notify doctor of any new medications
- Use soft-bristled toothbrush
INR 4.0-5.0: Bleeding Risk Territory (Warning Zone)
Your blood is clotting significantly slower than intended. While not always an emergency, this range requires same-day medical evaluation.
Warning symptoms at this range:
- Nosebleeds lasting >10 minutes
- Blood in urine (pink or red)
- Dark/tarry stools
- Unusual bruising from minor bumps
- Prolonged bleeding from cuts
Real Case: David Chen’s INR jumped to 4.6 after starting antibiotics for a dental infection. His cardiologist held one warfarin dose, reduced his weekly total by 10%, and had him retest in 48 hours. His INR returned to 2.8 within a week.
INR Above 5.0: Emergency Protocol
Immediate actions:
- Call your doctor’s emergency line or cardiology service
- Don’t take today’s warfarin dose until instructed
- Avoid activities with fall/injury risk
- Go to ER if experiencing active bleeding, severe headache, or abdominal pain
The National Institutes of Health vitamin K reversal protocol guides emergency management, with oral vitamin K (1-2.5mg) typically reversing INR within 12-24 hours for non-bleeding patients.
If you’re experiencing concerning symptoms, use our Symptom Checker to assess severity while contacting medical help.
Warfarin & Medication Management
Managing Your PT/INR on Blood Thinners (Warfarin & Beyond)
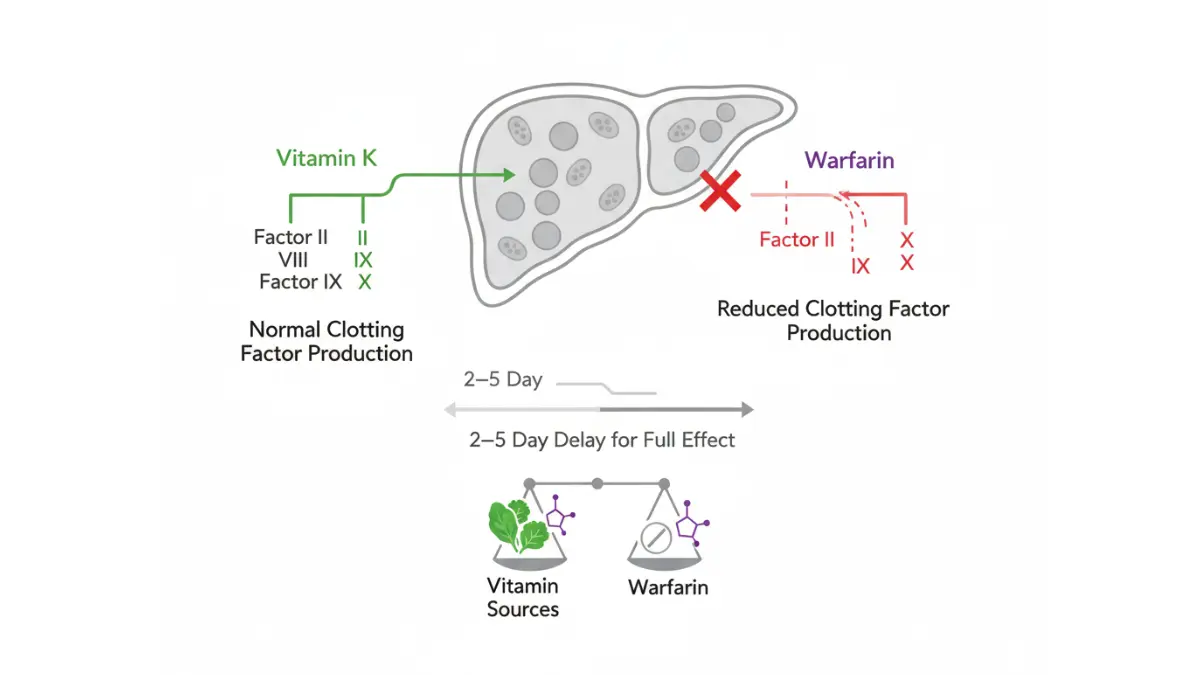
How Warfarin Affects Your INR (Dose-Response Timeline)
Warfarin doesn’t work immediately. After a dose change, your INR typically responds on this timeline:
INR Change Timeline:
- Day 1-2: Minimal to no change in INR
- Day 3-4: Peak dose effect begins showing
- Day 5-7: Full effect visible, INR stabilizes
- Day 8-14: Steady state achieved
This delay happens because warfarin blocks vitamin K-dependent clotting factor production in your liver, but existing clotting factors remain active for 2-5 days.
Why Your INR Fluctuates (10 Common Causes)
Understanding fluctuation triggers helps maintain stable PT/INR levels:
1. Dietary Changes:
- Sudden increase in leafy greens (vitamin K)
- Alcohol consumption variations
- Grapefruit juice (affects warfarin metabolism)
2. New Medications: Antibiotics are the #1 culprit for unexpected INR changes. The FDA drug interaction database lists 200+ medications affecting warfarin.
3. Illness or Infection:
- Fever increases metabolism
- Diarrhea/vomiting affects absorption
- Liver disease alters warfarin processing
4. Consistency Issues: Missing doses or taking double doses creates unpredictable swings.
Drug Interactions That Impact INR (Critical List)
Medications That RAISE INR (Bleeding Risk):
- Antibiotics: Ciprofloxacin, metronidazole, sulfamethoxazole
- Pain relievers: Aspirin, NSAIDs, acetaminophen (high doses)
- Antifungals: Fluconazole, ketoconazole
- Heart medications: Amiodarone, propafenone
- Antidepressants: SSRIs, particularly fluoxetine
Medications That LOWER INR (Clot Risk):
- Vitamin K supplements
- Cholestyramine (binds warfarin)
- Carbamazepine (increases metabolism)
- Rifampin (antibiotic)
- St. John’s Wort (herbal supplement)
If you’ve been prescribed new medications, verify them using our Pill Identifier and discuss warfarin interactions with your pharmacist immediately.
Vitamin K and INR: The Food Factor
The USDA nutrient database shows vitamin K content varies dramatically:
High Vitamin K Foods (>100mcg per serving):
- Kale: 1,062mcg per cup
- Spinach: 888mcg per cup
- Collard greens: 836mcg per cup
The key: Consistency matters more than avoidance. Eating spinach three times weekly is fine—just don’t suddenly eliminate or triple your intake.
DOACs vs Warfarin: 2026 Comparison
Direct oral anticoagulants (DOACs) like apixaban, rivaroxaban, and dabigatran don’t require INR monitoring. However, warfarin remains preferred for mechanical heart valves and costs significantly less—$4-15 monthly versus $400-600 for DOACs without insurance.
Similar to how HbA1c monitoring tracks long-term diabetes control, consistent PT/INR testing ensures your anticoagulation stays in the therapeutic window.
Home Monitoring & Lifestyle
PT/INR Home Testing & Daily Life Management
Home INR Monitors: Accuracy & Cost (2026 Devices)
Point-of-care testing has transformed anticoagulation management. The Centers for Medicare & Medicaid Services now covers home INR monitoring for 90% of warfarin patients who meet training requirements.
2026 Device Comparison:
| Device | Accuracy vs Lab | Cost Per Test | Medicare Coverage |
|---|---|---|---|
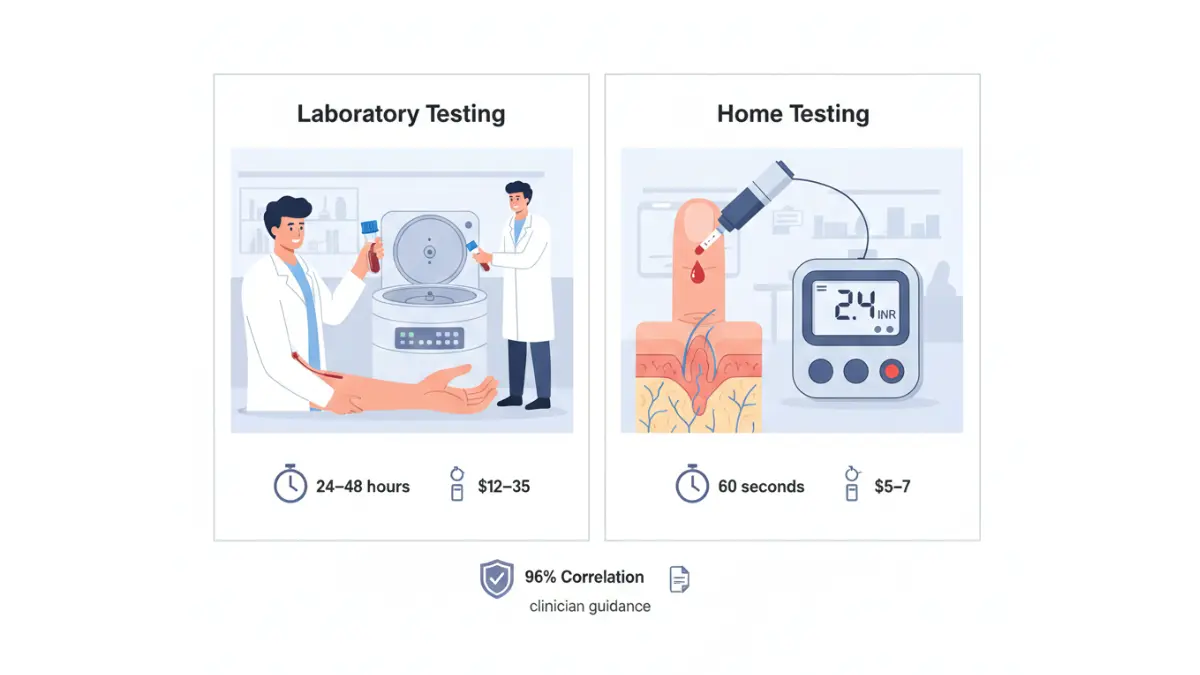
| CoaguChek XS Plus | 96.8% correlation | $5-7 | Yes, 100% |
| Alere INRatio2 | 95.3% correlation | $4-6 | Yes, 100% |
| Laboratory Draw | 100% (gold standard) | $12-35 | Yes, variable |
Home monitoring benefits:
- Test weekly without clinic visits
- Catch fluctuations 5-7 days earlier
- Results in 60 seconds
- Reduce stroke risk by 40% versus monthly lab testing
Testing Frequency by Condition
Your diagnosis determines monitoring schedules:
Initiation Phase (First 3 months):
- Weekly testing until stable
- After each dose adjustment, retest in 5-7 days
- Document results in a log
Maintenance Phase (After stabilization):
- Monthly testing if INR stable for 3+ months
- Every 2 weeks for higher-risk conditions
- Weekly for recent medication changes
Travel with Warfarin: What You Need to Know
8-Point Travel Protocol:
- Pack extra warfarin (7 days beyond trip length)
- Carry medication in original bottles
- Bring INR testing supplies if using home monitor
- TSA allows testing strips—keep in carry-on
- Adjust for time zones >3 hours (consult doctor)
- Pack medical alert card listing INR target
- Research anticoagulation clinics at destination
- Avoid alcohol excess on flights
According to Mayo Clinic travel medicine guidelines, dehydration during flights can temporarily affect INR—maintain hydration similar to recommendations from our Water Intake Calculator.
When to Call Your Doctor (Red Flag Checklist)
Contact within 24 hours if:
- INR drops below 1.8 or rises above 4.0
- Starting any new medication or supplement
- Persistent diarrhea or vomiting >24 hours
- Planned dental work or surgery
Seek emergency care immediately for:
- Severe headache or vision changes
- Coughing up blood
- Vomiting blood or coffee-ground material
- Black, tarry stools
- Severe abdominal pain
- Major fall or head injury
Early recognition of complications, combined with consistent monitoring, reduces warfarin-related hospitalizations by 60% compared to inconsistent testing patterns.
Common PT/INR Questions Answered
1. How long does a PT/INR test take?
Laboratory tests take 5 minutes for blood draw with results in 24-48 hours. Home testing devices provide results in 60-90 seconds from fingerstick samples.
2. Can I eat before an INR test?
Yes, fasting is not required for PT/INR tests. However, maintain consistent dietary habits—don’t drastically change vitamin K intake the day before testing.
3. How often should I test my INR?
Weekly during warfarin initiation and dose changes. Monthly once stable for 3+ consecutive months. Every 2-4 weeks for high-risk conditions like recurrent DVT.
4. What raises INR quickly?
Antibiotics, NSAIDs, alcohol, sudden decrease in vitamin K intake, fever, and diarrhea can increase INR within 24-72 hours.
5. Can stress affect my INR?
Indirectly yes. Stress may alter eating patterns, medication adherence, or trigger illness—all factors that influence INR levels.
6. Is INR 4.5 dangerous?
Yes, this requires same-day medical evaluation. Bleeding risk increases significantly above 4.0. Don’t wait—contact your anticoagulation clinic or doctor immediately.
7. How fast can INR drop?
After stopping warfarin, INR typically decreases by 0.5-1.0 units daily. With vitamin K administration, INR can drop from 5.0 to 2.0 within 12-24 hours.
8. Can I drink alcohol on warfarin?
Moderate consumption (1 drink for women, 2 for men daily) is generally safe with stable INR. Binge drinking dramatically raises INR and bleeding risk.
9. What if I miss a warfarin dose?
Take it as soon as remembered if within 12 hours. If closer to next dose, skip the missed dose. Never double up. Retest INR in 5-7 days.
10. Do all blood thinners need INR monitoring?
No. Only warfarin and similar vitamin K antagonists require PT/INR testing. DOACs (apixaban, rivaroxaban, dabigatran) don’t need routine monitoring but cost significantly more.
11. When will my INR stabilize?
Most patients achieve stable INR within 4-8 weeks of starting warfarin, assuming consistent dosing, diet, and no medication changes.
What to Do After Reading This
Your 3-Step Action Plan:
- Document Your Current INR: Write down your last three results and dates. Identify any patterns or sudden changes.
- Review Your Medication List: Check the interaction sections above. Schedule a pharmacy consultation if you’re taking any medications that raise or lower INR.
- Schedule Appropriate Follow-Up:
- INR <1.8 or >4.0: Contact doctor today
- INR 1.8-2.0 or 3.5-4.0: Call within 24 hours
- INR 2.0-3.5: Continue current schedule
Helpful Resources:
- Track patterns across multiple health metrics using our Health Tips section
- Understand related test results with our CBC test guide
- Learn about clot symptoms at our blood clots resource
Medical Disclaimer: This article provides educational information about PT/INR test interpretation and is not medical advice. Always consult your healthcare provider for personalized guidance regarding anticoagulation therapy, warfarin dosing adjustments, or concerning symptoms. INR targets vary by individual condition—follow your doctor’s specific recommendations.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.