On This Page – Quick Medical Summary
Quick Answer: Exfoliating removes dead skin cells from the skin’s surface, supporting cell turnover and radiance. But done incorrectly — too often, with the wrong method, or on the wrong skin type — it destroys your skin barrier, triggers breakouts, and accelerates skin aging. Most Americans are making at least one critical exfoliation mistake right now.
What Is Exfoliating — And Why Most Americans Do It Wrong
Marcus, 31, came to his dermatologist frustrated. He’d been using a glycolic acid toner every morning and a physical scrub every evening — convinced more was better. Within three weeks, his skin was red, burning, and breaking out worse than ever. His skin barrier was destroyed. His dermatologist had a one-word diagnosis: over-exfoliation.
This scenario plays out in dermatology offices across the United States every single week.
What exfoliating actually does:
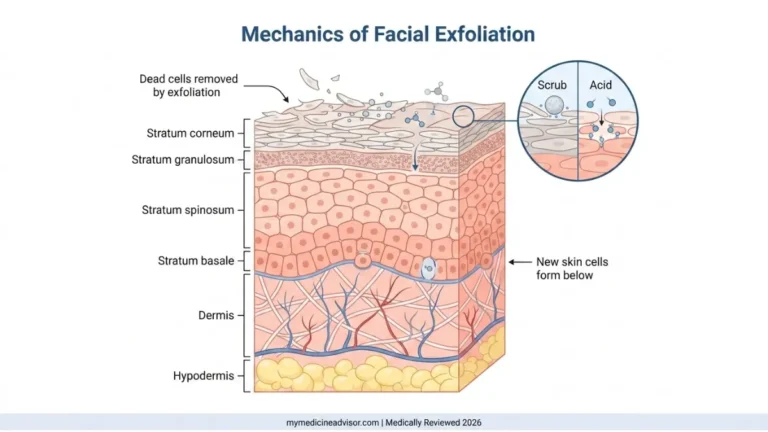
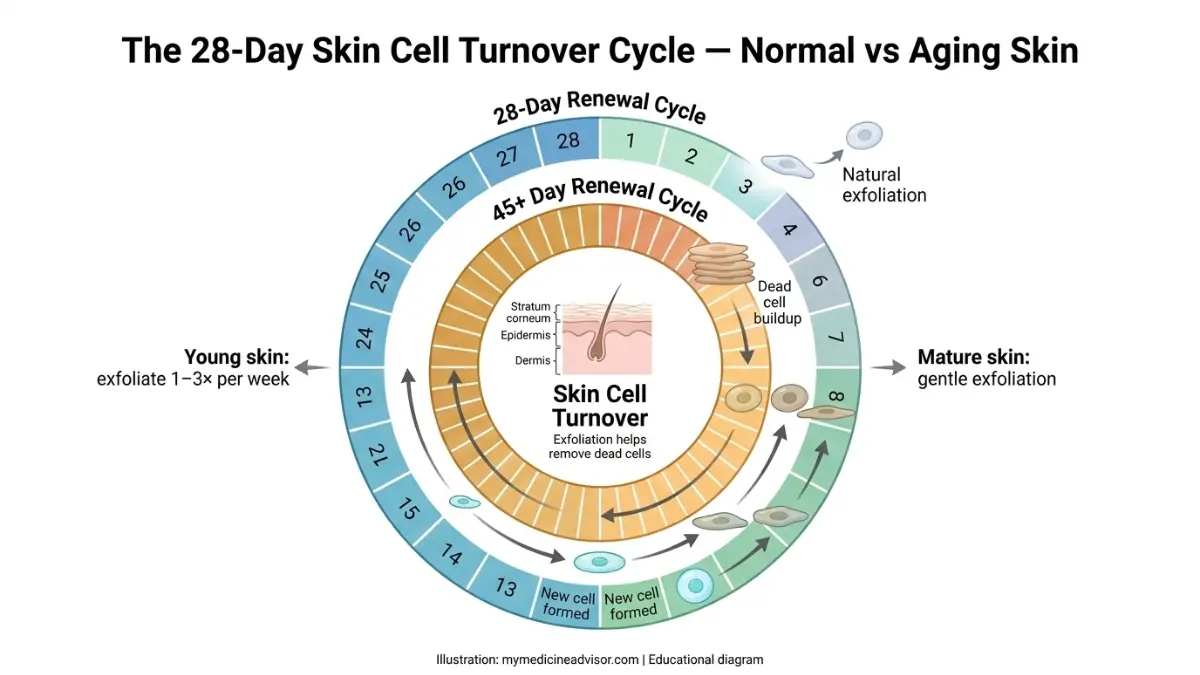
Exfoliating is the process of removing dead skin cells from the outermost layer of your skin — the stratum corneum, which is made up of 10 to 30 layers of dead cells. Your skin naturally sheds these cells every 28 days in younger adults. That cycle slows to 45 or more days as you age.
When this shedding process becomes sluggish — due to age, environmental stress, or hormones — dead cells build up on the surface. The result: dull, uneven skin tone, clogged pores, and reduced absorption of your moisturizers and serums.
Exfoliating helps accelerate this natural renewal. According to the American Academy of Dermatology, proper exfoliation can leave skin looking brighter and improve the effectiveness of topical skincare products by enhancing absorption.
The 2026 clinical reality:
A 2024 survey by the International Dermal Institute found that 68% of U.S. dermatologists treated patients in the past year for adverse skin reactions — including contact dermatitis, barrier damage, and severe purging — directly linked to at-home exfoliation products or viral techniques popularized on social media.
The problem isn’t exfoliating itself. It’s that most people exfoliate too aggressively, too frequently, and with the wrong products for their skin type.
If you’re experiencing unusual skin reactions after your routine, our free Symptom Checker can help you assess whether your skin may be responding to barrier stress.
The 3 Types of Exfoliation — What Dermatologists Actually Prefer in 2026
Not all exfoliation is equal. Understanding the three primary methods is the single most important step in getting exfoliating right.
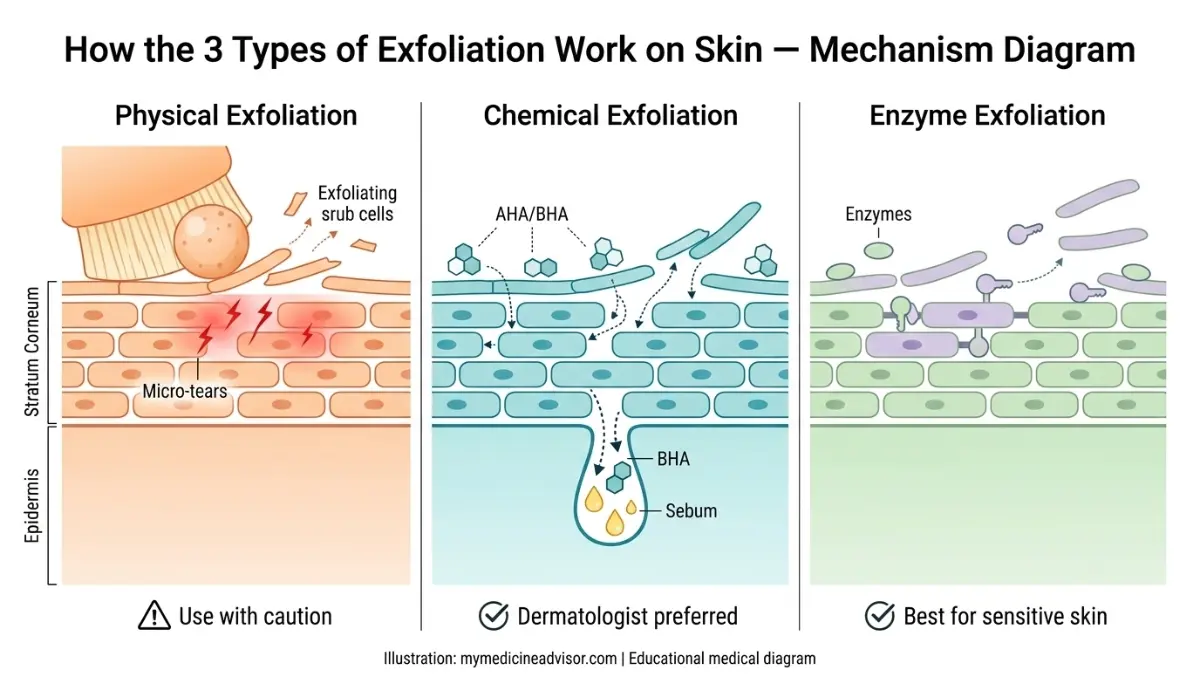
Physical Exfoliation — The Most Overused Method
Physical (mechanical) exfoliation uses a tool or abrasive substance to manually scrub away dead skin cells. This includes face scrubs, loofahs, cleansing brushes, and washcloths.
Who it’s right for: People with oily, thick skin only.
The critical warning most guides skip:
Physical scrubs with jagged or uneven particles — including popular sugar and walnut scrubs — can create microscopic tears in the skin. These micro-abrasions trigger an inflammatory response, worsen hyperpigmentation in darker skin tones, and can introduce bacteria into open micro-wounds, worsening acne.
The AAD explicitly advises that those with sensitive, dry, or acne-prone skin should avoid mechanical exfoliation entirely and opt for chemical alternatives instead.
Chemical Exfoliation — AHAs, BHAs, and PHAs
Chemical exfoliants use acids to dissolve the bonds between dead skin cells, allowing them to shed more effectively. This is currently the dermatologist-preferred category.
The three acid families:
| Acid Type | Examples | Best For | How It Works |
|---|---|---|---|
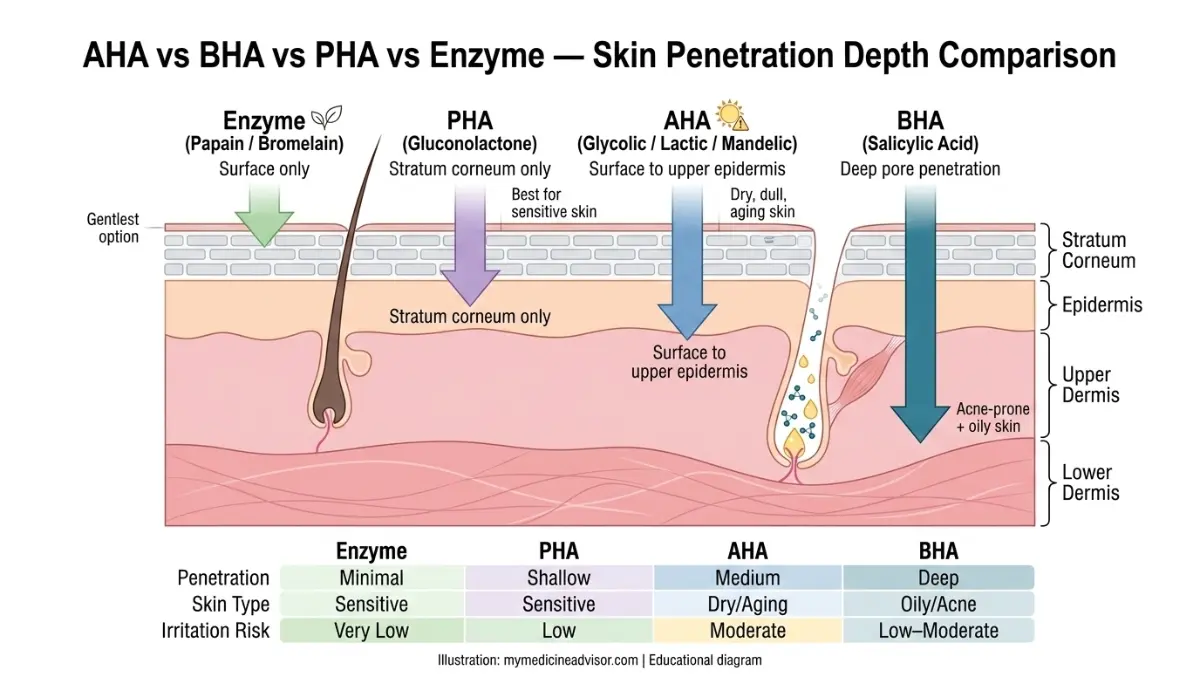
| AHA (Alpha Hydroxy Acid) | Glycolic, lactic, mandelic | Dry, dull, aging skin | Dissolves dead cells on the surface |
| BHA (Beta Hydroxy Acid) | Salicylic acid | Acne-prone, oily skin | Oil-soluble; penetrates pores |
| PHA (Polyhydroxy Acid) | Gluconolactone | Sensitive, reactive skin | Gentle, larger molecule, slower acting |
For home use, board-certified dermatologists recommend concentrations of 5–10% for AHAs and 1–2% for BHAs. Anything stronger should be administered by a licensed professional.
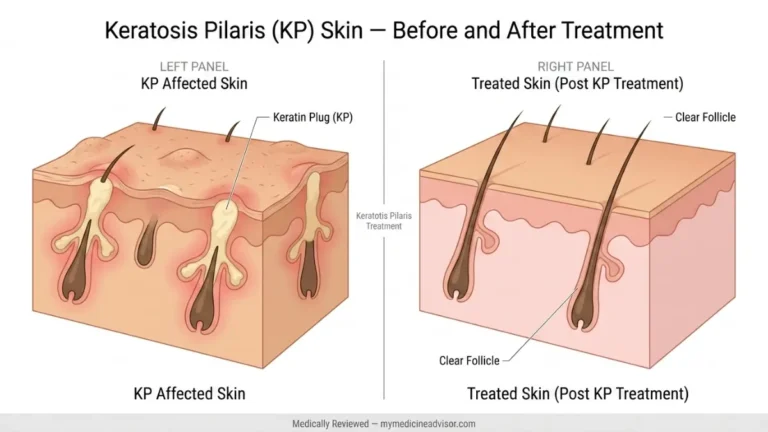
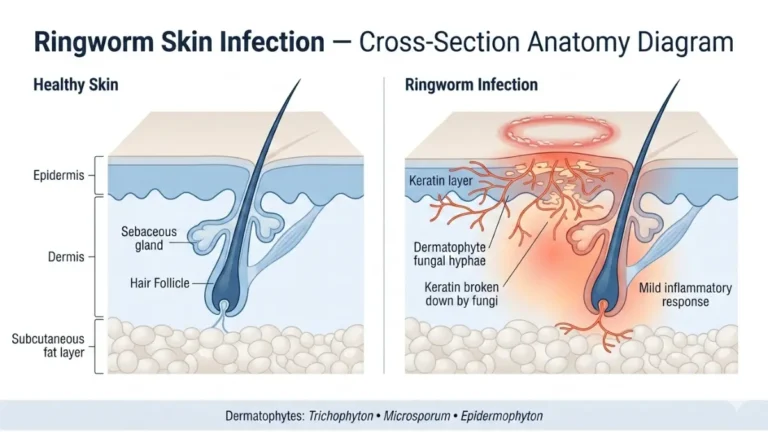
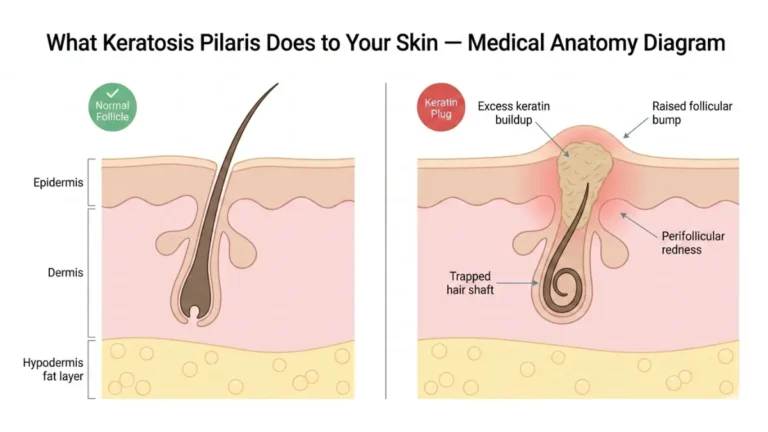
If you’re managing a condition like keratosis pilaris, our detailed guide on KP treatment covers how chemical exfoliation specifically addresses this common skin texture concern.
Enzyme Exfoliation — The 2026 Dermatologist-Preferred Method (Zero Competitors Cover This)
Enzyme exfoliants use naturally derived proteins — primarily papain (from papaya) and bromelain (from pineapple) — to break down the keratin protein in dead skin cells. They dissolve the cellular “glue” without using acid.
Why it’s surging in 2026:
- Zero acid irritation
- Safe for rosacea, eczema, and barrier-compromised skin
- Suitable for patients who have failed AHA and BHA trials
- Dermatologists in 2026 are increasingly recommending enzyme + PHA combinations as a first-line at-home option for sensitive patients
Research published in the Journal of Cosmetic Dermatology confirms that enzyme-based formulas produce equivalent dead cell removal to low-concentration AHAs with significantly lower irritation rates in sensitive skin populations.
How Often Should You Exfoliate? The 2026 Frequency Guide
This is the most-searched question about exfoliating — and the most poorly answered by every major competitor.
Direct answer: For most people, exfoliating 1 to 3 times per week is clinically appropriate. Daily exfoliation is almost never safe for at-home use and is a primary driver of skin barrier damage seen in U.S. dermatology practices in 2026.
Exfoliation Frequency by Skin Type
| Skin Type | Recommended Frequency | Best Exfoliant | Avoid |
|---|---|---|---|
| Sensitive | Once every 7–10 days | PHA or enzyme | AHAs, physical scrubs |
| Dry / Dehydrated | Once per week | Low % lactic acid (5–8%) | Glycolic acid, physical |
| Normal / Combination | Twice per week | Lactic or mandelic acid | Daily use |
| Oily / Acne-Prone | 2–3x per week | 2% BHA (salicylic acid) | Layering multiple actives |
| Mature Skin (45+) | Once per week | Gentle lactic acid | Physical scrubs |
| Darker Skin Tones | Max once per week | PHA or enzyme | Glycolic acid (PIH risk) |
Morning vs. Night — When Should You Exfoliate?
Timing matters more than most people realize:
- AHAs (glycolic, lactic, mandelic): Night use only. AHAs increase photosensitivity for 48–72 hours after application. Skipping SPF the next morning after AHA use significantly increases UV damage risk.
- BHAs (salicylic acid): Morning or night is acceptable; less photosensitizing than AHAs.
- Physical exfoliants: Morning only; never layer with retinoids or acids.
Always apply broad-spectrum SPF 30 or higher the following morning after any exfoliating treatment. Research indexed on PubMed (NIH) confirms that AHA use without sun protection significantly increases UV-induced skin damage.
The Skin Cycling Method — 2026’s Most Clinically Endorsed Protocol
Skin cycling was developed to prevent the over-exfoliation epidemic currently seen in U.S. dermatology:
- Night 1: Exfoliate
- Night 2: Retinoid
- Night 3–4: Recovery (barrier repair only — no actives)
This four-night rotation ensures your skin barrier has adequate time to recover between active ingredient exposures. It’s the protocol most commonly recommended by U.S. board-certified dermatologists in 2026.
What This Means For You: If you are currently using a retinoid or benzoyl peroxide, you must reduce your exfoliation frequency immediately. Combining these on the same night is the #1 cause of chemical burns from at-home skincare.
8 Warning Signs You’re Over-Exfoliating — And Damaging Your Skin Barrier
This is the section your skin desperately needs you to read.
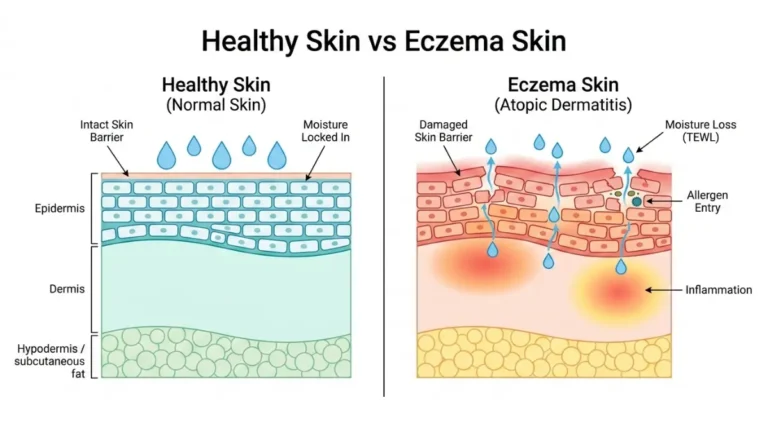
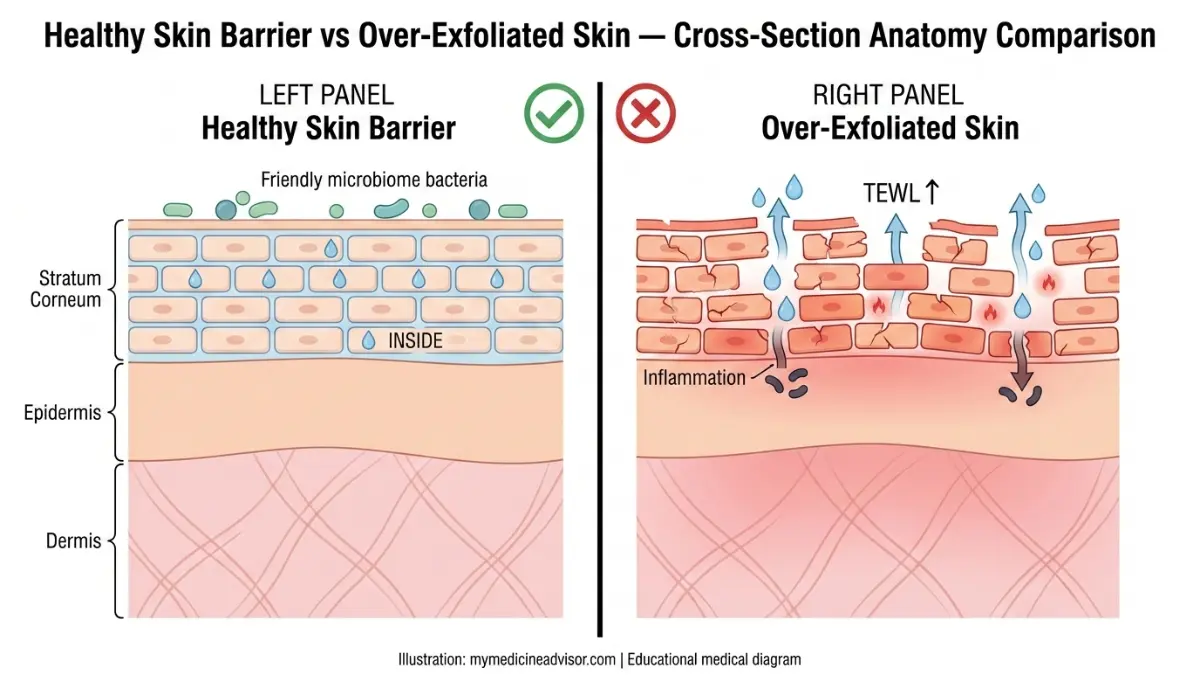
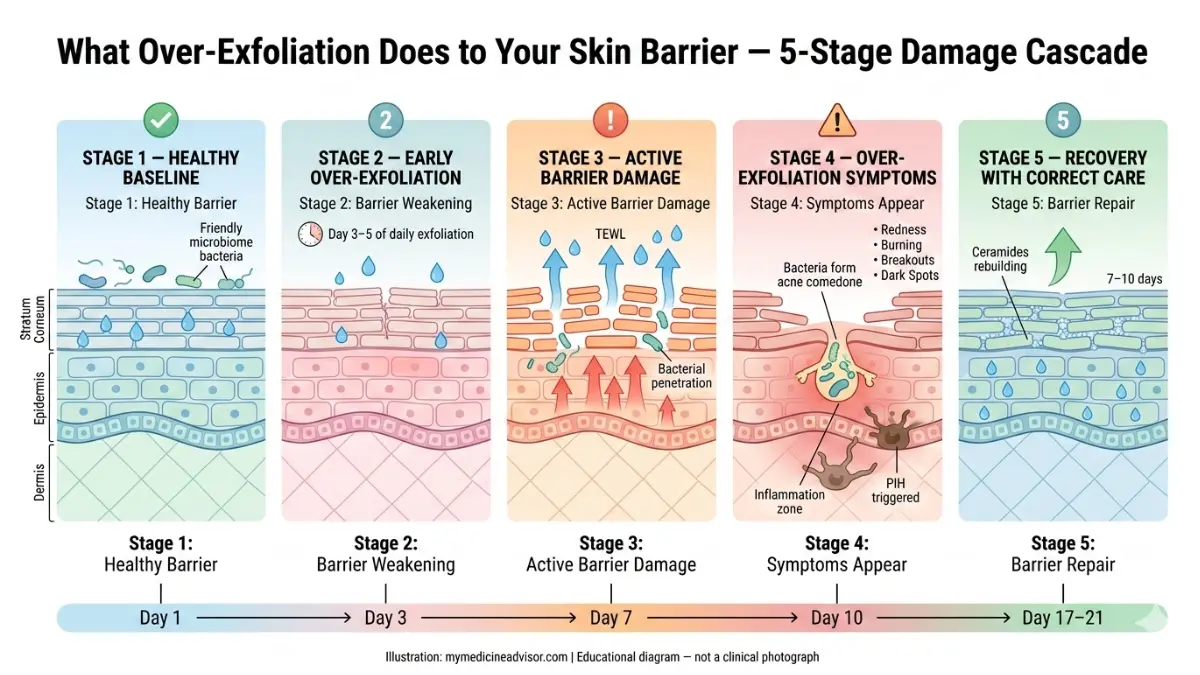
Over-exfoliating strips the stratum corneum, increases transepidermal water loss (TEWL), disrupts the skin’s microbiome, and triggers a chronic inflammatory cascade that paradoxically worsens everything you were trying to fix.
Here’s what happens biologically:
When the skin barrier is compromised by excessive exfoliating, three things occur simultaneously:
- Moisture escapes faster than the skin can retain it → chronic dehydration
- Bacteria penetrate more deeply into follicles → worsened breakouts
- Melanin-producing cells (melanocytes) are stimulated by inflammation → new or worsened dark spots
The 8 Clinical Warning Signs
Watch for these signs after your current exfoliating routine:
- Persistent redness that doesn’t resolve within 24 hours — this is inflammation, not a post-exfoliation glow
- Stinging or burning when applying your regular moisturizer — classic sign of a compromised skin barrier
- Skin feels tight immediately after cleansing — TEWL signature; your barrier is failing to retain moisture
- Shiny, waxy-looking skin — over-polished stratum corneum; the protective layer has been stripped
- More breakouts, not fewer — bacteria entering through the compromised barrier
- Flaking despite heavy moisturizing — skin structurally unable to retain hydration
- Increased sun sensitivity or sunburn more easily than usual — reduced stratum corneum thickness = less UV protection
- Products that previously worked now cause stinging — your barrier is inflamed and reactive to ingredients it previously tolerated
Condition-specific risks:
- Acne-prone skin: Over-exfoliating causes deeper, more inflamed pimples — not fewer. The weakened barrier allows acne-causing bacteria to penetrate more easily.
- Rosacea: Even gentle PHA use can trigger prolonged flushing and burning in rosacea-prone patients.
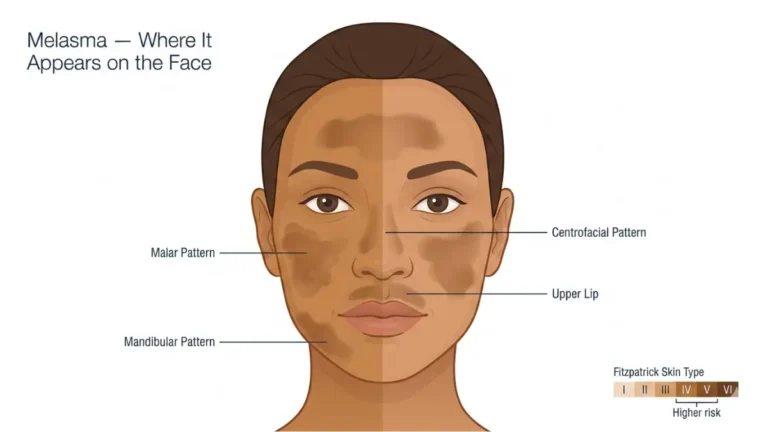
- Darker skin tones: Aggressive exfoliating is a leading trigger of post-inflammatory hyperpigmentation (PIH) — dark spots that can take months to resolve. Our comprehensive guide on melasma causes and treatment covers how PIH and melasma are managed clinically.
- Eczema: Any exfoliation during an active flare can lead to cracking, bleeding, and infection. See our dermatologist-reviewed guide on eczema treatment for barrier-safe skincare protocols.
If you’re noticing multiple symptoms from this list, use our free Symptom Checker for a structured self-assessment before your next dermatology appointment.
How to Exfoliate Correctly — The 2026 Dermatologist Protocol + Barrier Repair Plan
The 6-Step Correct Exfoliation Method
Follow this protocol for every exfoliating session:
- Cleanse first. Always exfoliate on clean, slightly damp skin. Never exfoliate over makeup, sunscreen, or dry skin.
- Apply a pea-sized amount. For chemical exfoliants: thin, even layer. For physical: gentle circular motions with fingertips only — never a scrubbing brush.
- Respect the timing. Rinse-off chemical exfoliants: 30 seconds. Leave-on formulas: follow the product instructions precisely. Physical: no more than 60 seconds of contact.
- Rinse with lukewarm water. Hot water significantly increases post-exfoliation irritation and redness.
- Apply barrier-repair moisturizer within 60 seconds. Look for ceramides, hyaluronic acid, and niacinamide. These three ingredients are clinically validated for post-exfoliation barrier recovery, as confirmed by research on PubMed (NIH).
- Apply SPF 30+ the following morning without exception. This step is non-negotiable after any AHA exfoliation.
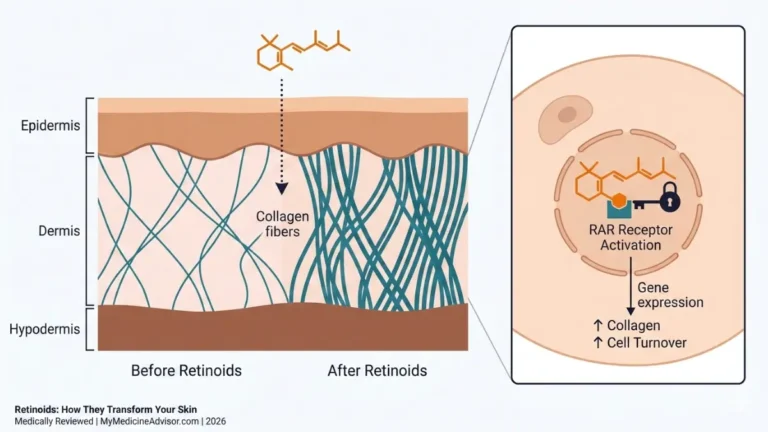
What This Means For You: Never combine same-night exfoliation with retinol or benzoyl peroxide unless explicitly directed by your dermatologist. This is the most common cause of severe at-home chemical burns seen in U.S. clinical practice. If you’re already using retinoids, read our complete retinoids guide for safe combination protocols.
The 7–10 Day Skin Barrier Repair Protocol
If you’ve already over-exfoliated, here is the evidence-backed recovery plan:
Step 1: Stop all exfoliants immediately — AHAs, BHAs, physical scrubs, retinoids, and vitamin C — for a minimum of 7 to 10 days.
Step 2: Switch to a sulfate-free, fragrance-free cleanser. Sulfates disrupt the skin’s natural pH and worsen barrier recovery.
Step 3: Apply a ceramide + niacinamide moisturizer morning and night. Ceramides are the structural lipids your barrier needs to rebuild.
Step 4: Layer hyaluronic acid serum on damp skin before your moisturizer. This maximizes moisture retention during the healing phase.
Step 5: Apply SPF 50+ every morning without exception. Over-exfoliated skin has measurably reduced UV protection.
Step 6: Avoid vitamin C, alcohol-based toners, essential oils, and fragrance until skin has fully normalized.
Step 7: Reintroduce exfoliating at half your previous frequency — with a gentler formula — only after your barrier symptoms have fully resolved.
Safe ingredient combinations for post-barrier repair:
| Combination | Timing | Clinical Benefit |
|---|---|---|
| AHA + Hyaluronic Acid | Same session | Offsets AHA-induced moisture loss |
| BHA + Niacinamide | Same session | Reduces post-exfoliation redness |
| PHA + Ceramide moisturizer | Same session | Barrier protection post-exfoliation |
| Enzyme + Aloe vera gel | Same session | Calming; safe even for rosacea skin |
Adequate daily hydration directly supports skin cell turnover and barrier recovery. Use our free Water Intake Calculator to ensure you’re hitting your daily targets — dehydration measurably slows epidermal healing.
Skin-Type Specific Exfoliation — Global Dermatologist Recommendations for 2026
Exfoliation for Acne-Prone Skin
Best choice: 2% salicylic acid (BHA), 2–3 times per week.
BHA is oil-soluble and penetrates inside the pore lining — making it clinically superior to any physical scrub for acne-prone skin. Physical exfoliation in acne-prone individuals creates micro-tears that allow Cutibacterium acnes bacteria to penetrate deeper, causing more severe inflammatory lesions.
Dr. Annie Gonzalez, MD, Board-Certified Dermatologist at Riverchase Dermatology: “Chemical exfoliation with salicylic acid is the evidence-based gold standard for acne-prone skin. Physical scrubs in active acne can worsen inflammation significantly.”
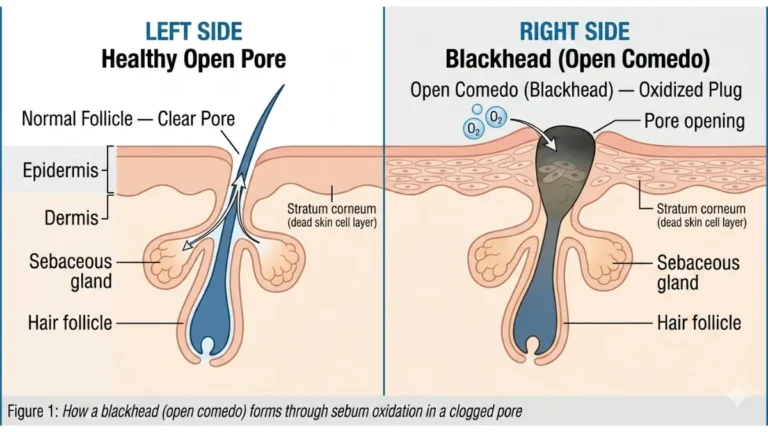
For additional acne management strategies, our guide on blackhead removal dermatologist methods covers the full clinical toolkit.
Exfoliation for Sensitive and Rosacea-Prone Skin
Best choice: PHA (gluconolactone) or enzyme exfoliant, once every 10–14 days maximum.
PHAs have a larger molecular structure than AHAs and BHAs, which means they penetrate more slowly and cause significantly less irritation. In 2026, enzyme exfoliants have become the first-line recommendation for rosacea patients because they produce zero acid-related flushing.
Avoid all AHAs, physical scrubs, and high-concentration peels in this skin type. If you’re managing eczema or rosacea alongside your exfoliation concerns, our comprehensive best eczema cream guide includes barrier-safe skincare frameworks from board-certified dermatologists.
Exfoliation for Darker Skin Tones — A Critically Underserved Topic
This is one of the most significant gaps in all current competitor content, and one of the most important topics for diverse U.S. skin populations.
Key clinical facts:
- Glycolic acid carries the highest risk of triggering post-inflammatory hyperpigmentation (PIH) in deeper skin tones — dark spots that can persist for 6–12 months or longer
- Mandelic acid (an AHA) is the safest acid for darker skin tones due to its larger molecular size and slower absorption rate
- PHA is the preferred first-line chemical exfoliant for Fitzpatrick skin types IV–VI
- Never use high-strength peels (>20% AHA) at home on darker skin tones without professional supervision
The American Academy of Dermatology offers specific guidance on exfoliating safely for darker skin tones at aad.org.
Exfoliation for Mature Skin (Ages 45+)
As skin ages, cell turnover slows from the 28-day cycle to 45 days or more. Paradoxically, mature skin is also thinner and more fragile — meaning it needs exfoliation more but can tolerate it far less aggressively.
Clinical guidance for 45+ skin:
- Lactic acid at 5–8% concentration, once weekly — the gold-standard AHA for mature skin. It exfoliates while simultaneously attracting moisture to the skin, making it the only AHA with a built-in hydrating effect.
- Never use physical scrubs on mature skin. The skin is thinner, collagen density is lower, and micro-tear risk is substantially higher.
- Follow every session with SPF 50+ — mature skin has reduced melanin protection and slower repair mechanisms.
What This Means For You: If you are over 45, the combination of lactic acid exfoliation at low concentration + ceramide moisturizer + daily SPF 50 is the clinical trifecta endorsed by dermatologists worldwide for maintaining skin renewal without barrier compromise.
For more on professional-grade treatments that complement a home exfoliation routine, explore our expert guide on microdermabrasion — is it worth it? and the 2026 review on facial exfoliator methods.
Frequently Asked Questions
Q1. What does exfoliating do to your skin?
Exfoliating removes dead skin cells from the stratum corneum, accelerates cell turnover, unclogs pores, and improves the absorption of moisturizers and serums. Done correctly, it produces brighter, smoother, and more even-toned skin.
Q2. How often should you exfoliate your face?
Most skin types: 1–3 times per week. Sensitive or rosacea-prone skin: once every 7–14 days. Daily exfoliation is almost never appropriate for at-home use and is a leading cause of skin barrier damage.
Q3. Is chemical or physical exfoliation better?
Chemical exfoliation is preferred by board-certified dermatologists for most skin types. Physical scrubs carry a higher risk of micro-tears, inflammation, and worsened hyperpigmentation — especially on sensitive, acne-prone, or darker skin tones.
Q4. What are the signs you’re over-exfoliating?
Persistent redness, stinging when applying moisturizer, tight skin after cleansing, shiny or waxy-looking skin, more breakouts than usual, increased sun sensitivity, and products that previously worked now causing irritation.
Q5. Can you exfoliate every day?
No. Daily exfoliation strips the skin barrier, increases transepidermal water loss, disrupts the skin’s microbiome, and triggers chronic inflammation. Dermatologists in 2026 uniformly recommend against daily at-home exfoliation.
Q6. What should you NOT do after exfoliating?
Do not apply retinol, benzoyl peroxide, vitamin C, or any other active ingredient on the same night. Do not use hot water to rinse. Do not skip SPF the following morning. Do not exfoliate again within 48 hours.
Q7. What is the best exfoliant for acne-prone skin?
2% salicylic acid (BHA) applied 2–3 times per week is the dermatologist-endorsed gold standard for acne-prone skin. It penetrates pores directly and has anti-inflammatory properties that physical scrubs lack.
Q8. How long does over-exfoliated skin take to heal?
Mild barrier damage typically resolves within 7–10 days with a simplified, barrier-focused routine. More severe damage or worsened hyperpigmentation can take 2–4 weeks or longer.
Q9. What is enzyme exfoliation?
Enzyme exfoliation uses naturally derived proteins — primarily papain (papaya) and bromelain (pineapple) — to dissolve dead skin cell bonds without using acids. It is the gentlest exfoliation method available and is becoming the 2026 first-line recommendation for sensitive, rosacea, and eczema-prone skin.
Q10. Can exfoliating cause breakouts?
Yes — and this is one of the most misunderstood outcomes in skincare. Over-exfoliating compromises the skin barrier, allowing acne-causing bacteria to penetrate more deeply and triggering inflammation. Many people mistake over-exfoliation damage for skin “purging” and exfoliate even more aggressively, worsening the cycle.
Q11. Is it safe to exfoliate during pregnancy?
Lactic acid and enzyme exfoliants are generally considered safe during pregnancy at standard over-the-counter concentrations. Salicylic acid (BHA) at high concentrations and glycolic acid peels should be avoided. Always consult your OB-GYN or dermatologist before using any active skincare ingredient during pregnancy.
Last medically reviewed: March 2026 | Sources: American Academy of Dermatology (AAD), National Institutes of Health (NIH) PubMed, International Dermal Institute, peer-reviewed research from the Journal of Cosmetic Dermatology and CosmoDerma (2025).
For personalized skin health guidance and expert-reviewed articles, explore our full health and wellness library.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.