On This Page – Quick Medical Summary
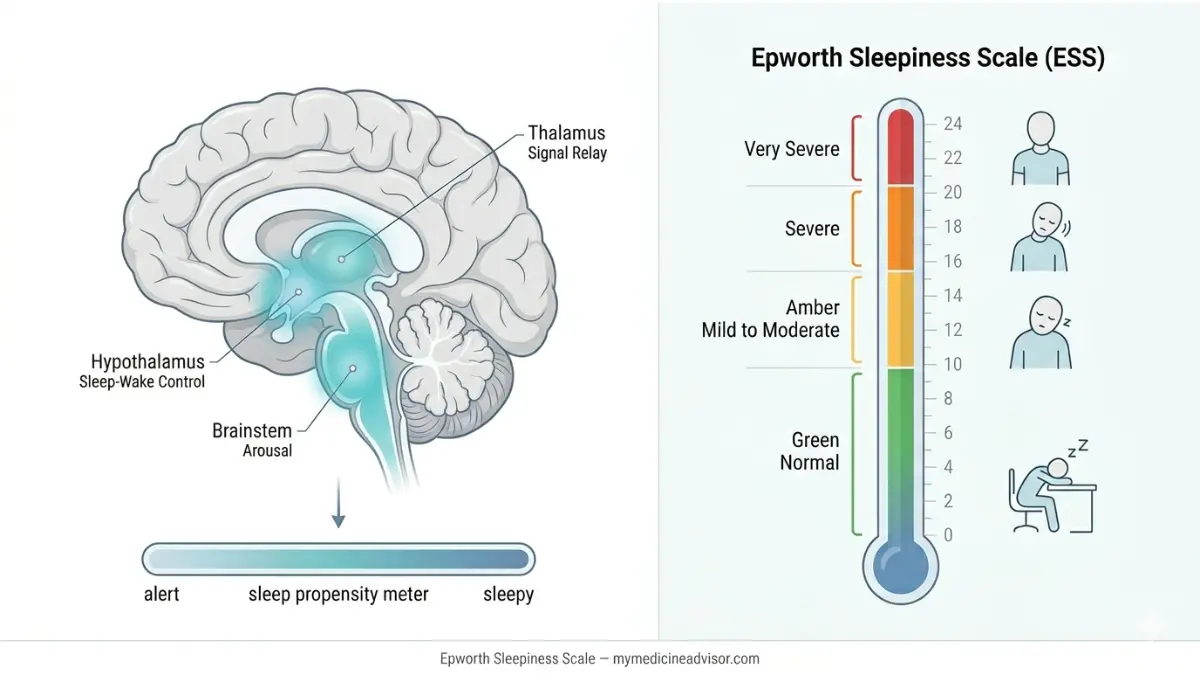
The Epworth Sleepiness Scale (ESS) is an 8-question, clinically validated questionnaire that measures your tendency to doze off during everyday activities. Scores range from 0 to 24. A score of 0–10 is normal; anything 11 or above signals excessive daytime sleepiness that warrants medical attention. If you just got your result and want to know exactly what it means — and what to do next — this guide covers everything.
What Is the Epworth Sleepiness Scale?
The Epworth Sleepiness Scale was developed in 1990 by Dr. Murray Johns at Epworth Hospital in Melbourne, Australia. It was designed as a fast, practical tool to quantify average sleep propensity — how likely a person is to fall asleep across a range of daily situations.
The test takes 2–3 minutes to complete. You rate your chance of dozing off in eight different scenarios on a scale of 0 to 3:
- 0 = Would never doze
- 1 = Slight chance of dozing
- 2 = Moderate chance of dozing
- 3 = High chance of dozing
The eight situations are deliberately chosen because they vary widely in how sleep-inducing they are — from lying down to rest (highly somniferous) to sitting in stopped traffic (low somniferous). This range is what makes the ESS diagnostically useful, not just a simple fatigue survey.
Important distinction most sites miss: The ESS measures sleep propensity (your biological drive to fall asleep) — not general tiredness or fatigue. You can feel exhausted yet score normally on the ESS, or feel reasonably alert yet score high. That’s why it matters beyond how you feel day-to-day.
If you’re unsure whether you’re meeting your sleep needs, our free Sleep Calculator can help you assess how much sleep your body actually requires each night — a useful companion step before interpreting your ESS result.
A modified pediatric version — the ESS-CHAD — exists for children and adolescents, with adjusted language and scenarios. The standard adult ESS (1997 version) is used for most people 18 and older.
The Complete Epworth Sleepiness Scale Score Breakdown
Your total score is the sum of all eight responses, ranging from 0 to 24. Here is the definitive score interpretation table — including real mean ESS scores by condition from Dr. Johns’ original 1991 validation study, data that no major competitor presents to patients:
ESS Score Interpretation Table
| ESS Score | Category | Clinical Meaning | Your Next Step |
|---|---|---|---|
| 0–5 | Low-normal | Very low daytime sleepiness | No action needed; maintain healthy sleep habits |
| 6–10 | Higher-normal | Normal range for healthy adults | Monitor; review sleep schedule if closer to 10 |
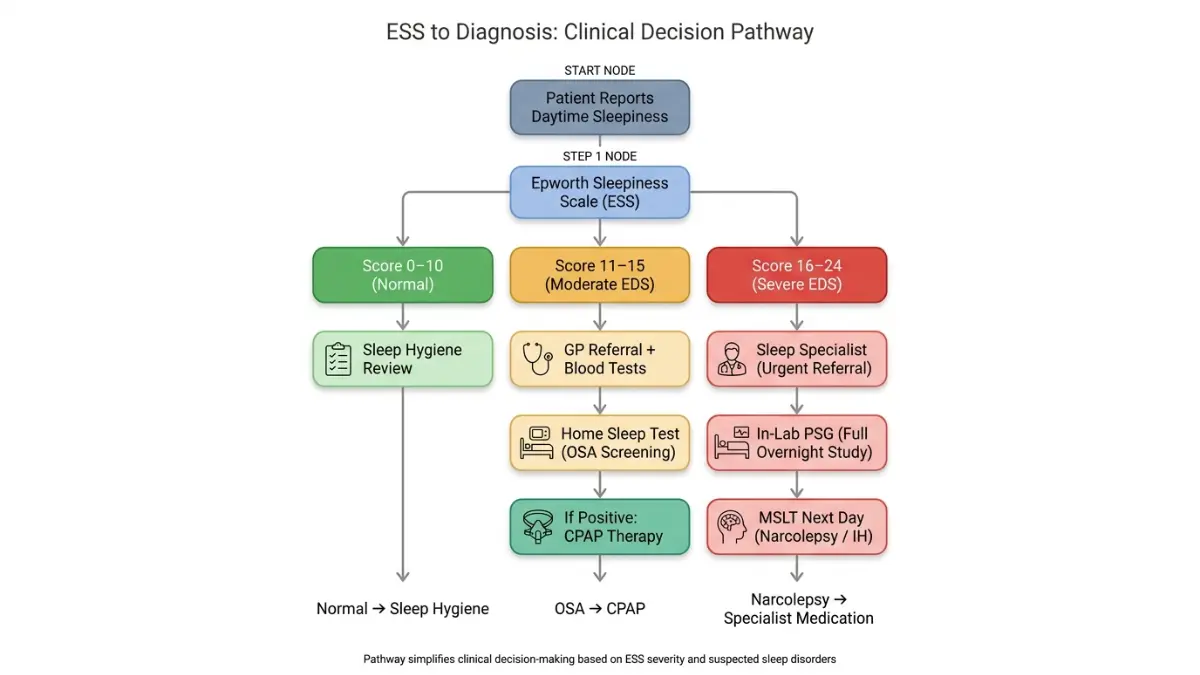
| 11–15 | Mild–Moderate EDS | Possible sleep debt, mild OSA, or medication effect | Book a GP appointment; bring your score |
| 16–20 | Severe EDS | Likely significant sleep disorder (OSA, hypersomnia) | Urgent sleep specialist referral required |
| 21–24 | Very Severe EDS | High probability of narcolepsy or severe OSA | Seek specialist evaluation immediately |
What the Original Study Data Shows
In the original Johns 1991 validation study published via Harvard Medical School’s Division of Sleep Medicine, mean ESS scores by condition were:
| Condition | Mean ESS Score |
|---|---|
| Normal healthy adults | 5.9 |
| Simple snorers (no disorder) | 6.5 |
| Periodic limb movement disorder | 9.2 |
| Obstructive sleep apnea (OSA) | 11.7 |
| Narcolepsy | 17.5 |
| Idiopathic hypersomnia | 17.9 |
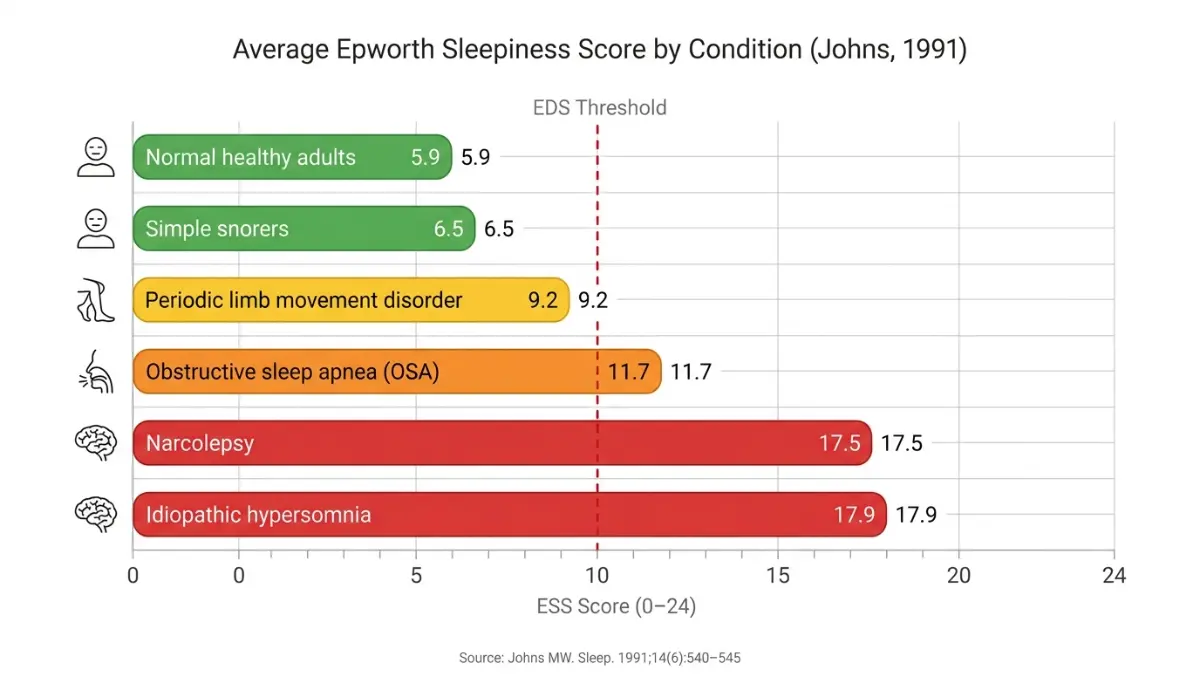
What this means for you: If you scored between 11 and 15, your ESS is statistically consistent with an OSA diagnosis. A score of 16 or above places you in the range associated with narcolepsy or severe sleep disorders.
🔴 Score ≥16 Warning: According to the official Epworth Sleepiness Scale guidelines, scores above 15 suggest very high average sleep propensity across most circumstances. People with scores this high should not rely on the ESS alone for driving fitness assessments — confirmatory testing is essential.
If you’re concerned about how your result connects to broader symptoms, our Symptom Checker can help you identify whether your daytime sleepiness may be part of a wider pattern worth investigating.
What Causes a High Epworth Sleepiness Score?
A high ESS score is a symptom signal, not a diagnosis. Multiple conditions and factors can drive your score above 10.
Sleep Disorders
These are the most common causes of elevated Epworth sleepiness scores:
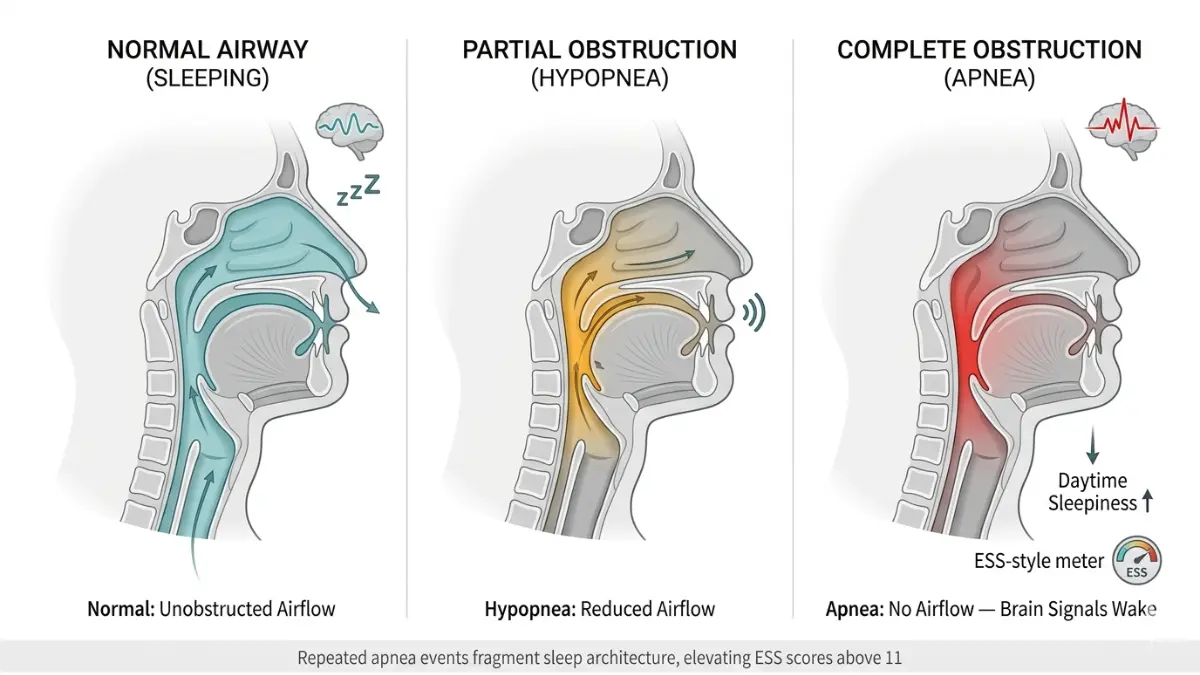
- Obstructive sleep apnea (OSA): Breathing repeatedly stops during sleep, fragmenting rest. Mean ESS of 11.7 in diagnosed patients. Learn more about how sleep apnea is diagnosed and what the testing process involves.
- Narcolepsy: A neurological disorder causing uncontrollable sleep attacks. ESS scores of 17–24 are common. High specificity (100%) and sensitivity (93.5%) for narcolepsy detection.
- Idiopathic hypersomnia: Excessive sleepiness even after adequate, quality sleep — mean ESS of 17.9.
- Restless legs syndrome / PLMD: Involuntary limb movements disrupting sleep architecture. Mean ESS around 9.2.
You can review the warning signs of a sleep disorder to see how daytime sleepiness fits into the broader clinical picture.
Medical Conditions
Several systemic conditions elevate daytime sleepiness independently of sleep quality:
- Hypothyroidism — reduced metabolic rate mimics sleep deprivation
- Depression — hypersomnia is a recognized symptom in depressive disorders. See our guide on whether depression causes sleep problems
- Parkinson’s disease — dopaminergic changes disrupt sleep-wake regulation
- Cancer and chronic illness — disease burden and treatment fatigue both raise ESS scores
Medications — The Gap Every Competitor Misses
Many patients score high on the Epworth Sleepiness Scale not because of a sleep disorder, but because of what they’re taking. Medications that commonly elevate daytime sleepiness include:
- Antihistamines (diphenhydramine, hydroxyzine)
- Benzodiazepines and sleep aids
- Beta-blockers (atenolol, metoprolol)
- Antidepressants (mirtazapine, tricyclics)
- Opioid pain medications
- Antiepileptics (gabapentin, pregabalin)
Our detailed guide on medications that cause insomnia and sleep disruption covers this in depth. Always review your current medication list with your prescriber before assuming a sleep disorder is the cause.
Lifestyle Factors
- Chronic sleep deprivation — consistently sleeping fewer hours than needed
- Shift work — circadian misalignment reliably raises ESS scores
- Alcohol use — disrupts sleep architecture, especially REM sleep
- High BMI/obesity — strongly associated with OSA risk and elevated ESS
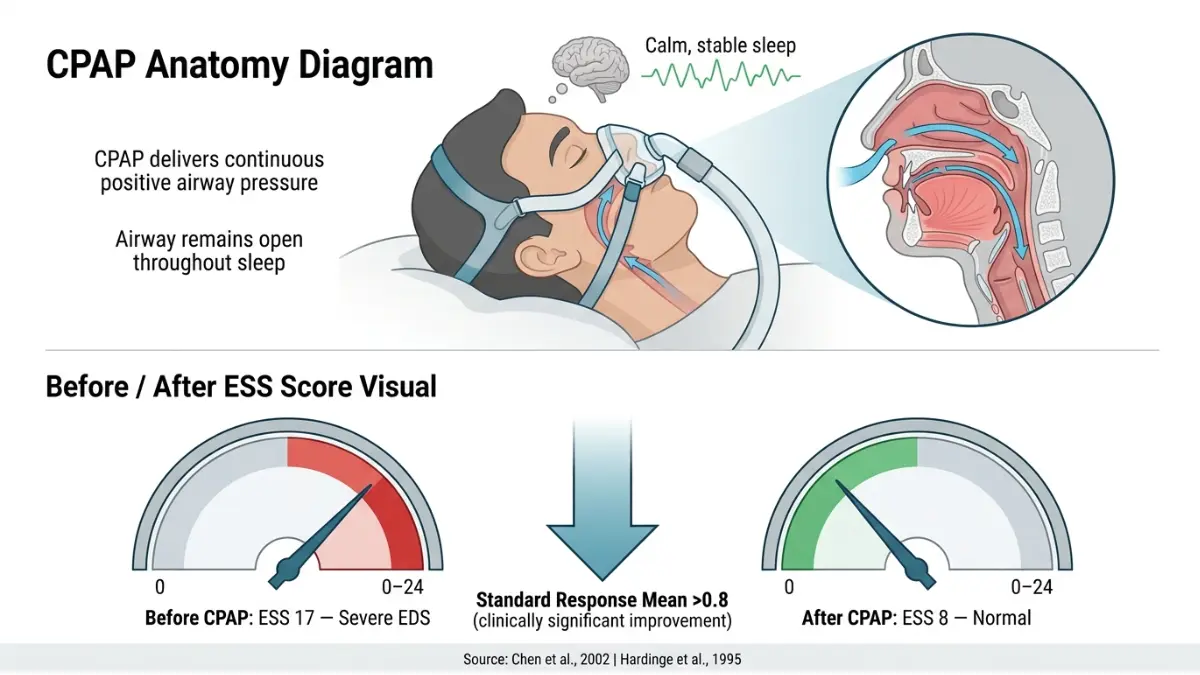
Marcus, a 44-year-old shift nurse who was “always exhausted,” scored 16 on his ESS during a routine occupational health check. He attributed it to long shifts. Polysomnography revealed moderate OSA — 23 breathing events per hour. CPAP therapy dropped his ESS to 8 within three months.
Is the Epworth Sleepiness Scale Accurate? Limitations You Must Know
The ESS is a validated and widely used clinical screening tool — but it has real limitations every patient deserves to understand.
What It Does Well
- Fast and accessible: 2–3 minutes, no equipment needed
- Validated across multiple sleep disorders, primarily OSA, narcolepsy, and idiopathic hypersomnia
- Responsive to treatment: ESS scores reliably decline after CPAP therapy, stimulant treatment for narcolepsy, and other interventions — making it useful for tracking progress
Where It Falls Short
Subjective self-report: Your score reflects how you perceive your sleepiness, which can be influenced by awareness, education level, and cultural factors. Some patients with severe OSA underreport because they’ve normalized their sleepiness.
Test-retest variability: In clinical populations, ESS scores can fluctuate significantly between visits. A 2022 review published in the National Library of Medicine found notably higher intra-individual variability in clinical patients compared to the healthy subjects in Johns’ original study.
Not diagnostic alone: The ESS cannot identify which sleep disorder you have. A score of 17 could indicate narcolepsy, severe OSA, idiopathic hypersomnia, or medication effects — only further testing can distinguish these.
ESS vs. Other Sleep Tests: Quick Comparison
| Test | What It Measures | Time Required | Clinical Use |
|---|---|---|---|
| ESS | Self-reported sleep propensity | 2–3 minutes | Screening tool |
| MSLT | Objective time to fall asleep (5 naps) | Full day | Narcolepsy diagnosis |
| PSG (Polysomnography) | Full overnight sleep architecture | 8+ hours | OSA, sleep staging |
| MWT | Ability to stay awake | 4 × 40 min | Occupational/driving fitness |
The ESS is the starting point. The Multiple Sleep Latency Test (MSLT) and polysomnography are the gold standards that follow when your ESS score flags concern.
What to Do After Your Epworth Sleepiness Score Result
This is where every competitor fails you. They say “see a doctor.” We give you a tiered action protocol — exactly what to do based on your specific score.
Score 0–10: Normal Range
You’re in the healthy range. Focus on maintaining consistent sleep habits:
- Aim for 7–9 hours of sleep per night (adults)
- Keep a consistent sleep/wake schedule, including weekends
- Limit caffeine after 2 PM — understand how caffeine disrupts sleep
- If your score is 8–10, monitor it — scores in the high-normal range with symptoms like snoring or morning headaches warrant mention to your doctor
Score 11–15: Mild to Moderate Excessive Daytime Sleepiness
Book a GP appointment. Bring your written ESS responses, not just your total score — individual item scores help clinicians spot patterns.
At your appointment, ask about:
- Sleep study referral (home sleep apnea test or in-lab polysomnography)
- Medication review — could any current prescriptions be contributing?
- Mental health screening — depression and anxiety are common drivers of excessive daytime sleepiness
- Thyroid function test (TSH) — hypothyroidism is frequently missed
Score 16–24: Severe Excessive Daytime Sleepiness
Request an urgent referral to a sleep medicine specialist. Do not delay — per the CDC’s occupational health guidance on the ESS, scores at this level have serious safety implications, including elevated crash risk while driving.
Your specialist will likely order:
- In-lab polysomnography (PSG) — full overnight sleep study
- Multiple Sleep Latency Test (MSLT) — especially if narcolepsy is suspected
- Blood work: TSH, CBC, metabolic panel, HbA1c
What treatment can do: In patients with OSA, CPAP therapy consistently lowers ESS scores. Studies show a Standard Response Mean greater than 0.8 for CPAP on ESS — meaning treatment produces clinically meaningful, measurable improvement in daytime alertness.
Evidence-Based Sleep Hygiene Checklist (All Score Tiers)
- ✅ Fixed wake time 7 days a week
- ✅ Bedroom temperature 65–68°F (18–20°C)
- ✅ No screens 30–60 minutes before bed
- ✅ Avoid alcohol within 3 hours of sleep
- ✅ Regular physical activity (but not within 2 hours of bedtime)
- ✅ Consistent light exposure in the morning to anchor your circadian rhythm
Expert Perspective & Key Takeaways
Dr. Omar Hassan, Internal Medicine (mymedicineadvisor.com Expert Panel): “The Epworth Sleepiness Scale is one of the most efficient first-line tools in primary care. What patients often don’t realize is that a score doesn’t just reflect how tired they feel — it reflects a measurable biological tendency. When a patient brings in a score above 14, my clinical pathway shifts immediately toward ruling out obstructive sleep apnea and, if warranted, narcolepsy screening.”
Key Takeaways
- The ESS measures sleep propensity across 8 scenarios — not general fatigue or how well you slept last night
- Normal is 0–10; scores of 11+ indicate excessive daytime sleepiness requiring professional evaluation
- A score of 16+ is clinically significant — associated with severe OSA, narcolepsy, or idiopathic hypersomnia
- Medications are an underrecognized cause of elevated ESS scores — always review your drug list
- The ESS is a screening tool, not a diagnosis — polysomnography and MSLT are needed to confirm any sleep disorder
For broader sleep and health content, explore our Health & Wellness resource hub for evidence-based guides reviewed by our international expert panel.
Frequently Asked Questions: Epworth Sleepiness Scale
1. What is a normal Epworth Sleepiness Scale score?
A score of 0–10 is considered normal for healthy adults. The average in the general population is around 5.9. Scores of 6–10 remain within the normal range but may warrant monitoring if you have other symptoms like snoring.
2. What does an ESS score of 15 mean?
A score of 15 falls in the mild-to-moderate excessive daytime sleepiness range. It is consistent with the mean ESS for obstructive sleep apnea (11.7) and warrants a GP referral. A sleep study may be recommended to rule out OSA or other disorders.
3. Is a score of 11 on the Epworth Sleepiness Scale bad?
An ESS of 11 marks the threshold for excessive daytime sleepiness (EDS). It’s not an emergency, but it signals that your daytime sleepiness is above the normal range and should be evaluated by a healthcare provider.
4. What score on the Epworth Sleepiness Scale indicates sleep apnea?
There’s no single diagnostic threshold, but scores ≥11 are associated with OSA, with the mean ESS for diagnosed OSA patients being 11.7. Scores above 16 suggest more severe forms of sleep-disordered breathing. A sleep study is required for a confirmed OSA diagnosis.
5. How accurate is the Epworth Sleepiness Scale?
The ESS is a validated and reliable screening tool, not a diagnostic test. Its internal consistency (Cronbach’s alpha 0.73–0.90) is strong, but test-retest variability is higher in clinical populations than in healthy subjects. Physician-administered ESS tends to be more accurate than self-administered versions.
6. Can I take the Epworth Sleepiness Scale at home?
Yes — the ESS can be self-administered. However, a 2013 study found that physician-administered ESS produces more accurate results in OSA patients. Use home completion as a first step, then discuss your responses with your doctor.
7. What happens after a high Epworth sleepiness score?
Your doctor will review your medications, order blood tests, and likely refer you for a polysomnography (PSG) or home sleep apnea test. A Multiple Sleep Latency Test (MSLT) may follow if narcolepsy is suspected.
8. Does a high ESS score always mean a sleep disorder?
No. Medications, depression, hypothyroidism, cancer, and chronic sleep deprivation can all produce high scores without a primary sleep disorder. A thorough clinical evaluation is essential before any diagnosis is made.
9. What is the difference between the ESS and the Pittsburgh Sleep Quality Index?
The ESS measures sleep propensity (likelihood of dozing during the day). The Pittsburgh Sleep Quality Index (PSQI) measures overall sleep quality including duration, efficiency, and disturbances. They measure different constructs and are often used together in clinical assessments.
10. Can medications cause a high Epworth sleepiness score?
Yes — and this is frequently overlooked. Antihistamines, benzodiazepines, beta-blockers, opioids, and many antidepressants can significantly elevate ESS scores. Always bring a full medication list to your appointment when discussing a high ESS result.
11. Is there an Epworth Sleepiness Scale for children?
Yes. The ESS-CHAD (Children and Adolescents) is a modified version with age-appropriate language and scenarios. It is used in pediatric sleep medicine for children and adolescents when daytime sleepiness is a clinical concern.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.