On This Page – Quick Medical Summary
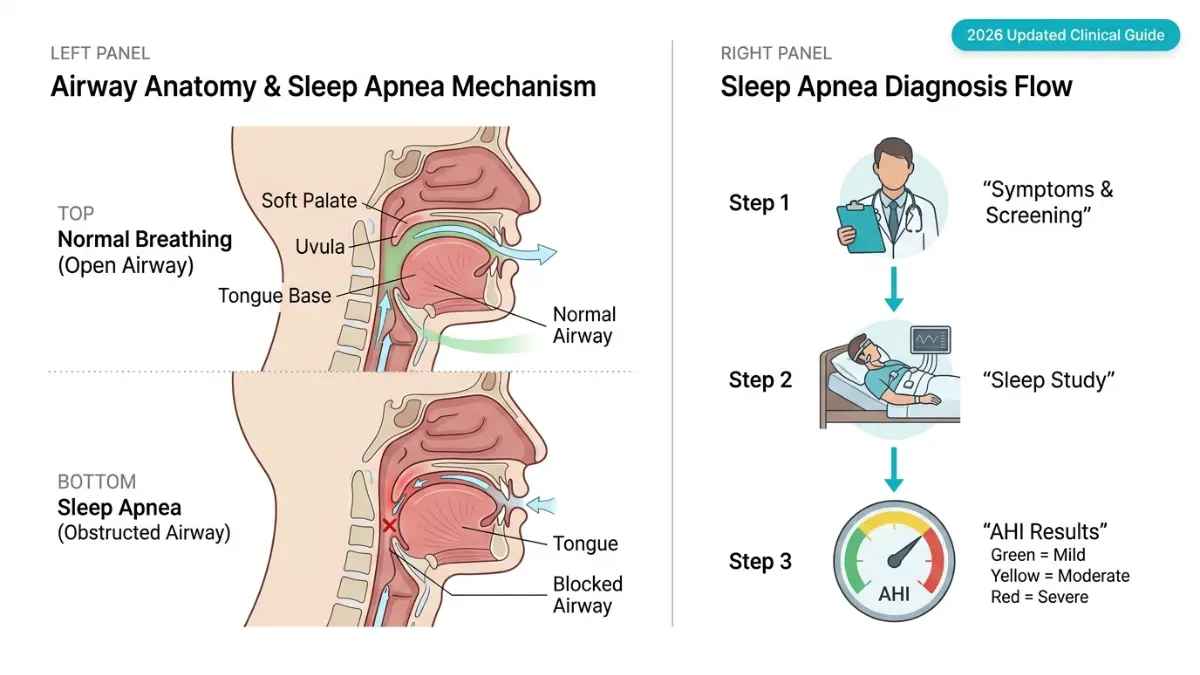
Sleep apnea is diagnosed through a sleep study — either an overnight polysomnography (PSG) in a lab or a home sleep apnea test (HSAT). A doctor confirms the diagnosis when your Apnea-Hypopnea Index (AHI) reaches 5 or more breathing disruptions per hour, combined with symptoms like loud snoring, gasping during sleep, or excessive daytime fatigue.
“My Doctor Said I Stopped Breathing 52 Times Last Night”
James, 47, a Chicago-based logistics manager, had no idea anything was wrong. His wife had complained about his snoring for years, but he dismissed it as “just snoring.” Then one night, she watched him stop breathing — completely — for nearly 20 seconds.
After a sleep study, James learned he had severe obstructive sleep apnea (OSA): 52 breathing pauses every hour.
His story is not unusual. According to research published on PMC/NCBI, up to 80% of people with moderate-to-severe sleep apnea remain undiagnosed — partly because the most obvious symptoms happen while they’re unconscious.
Why Sleep Apnea Goes Undetected for Years
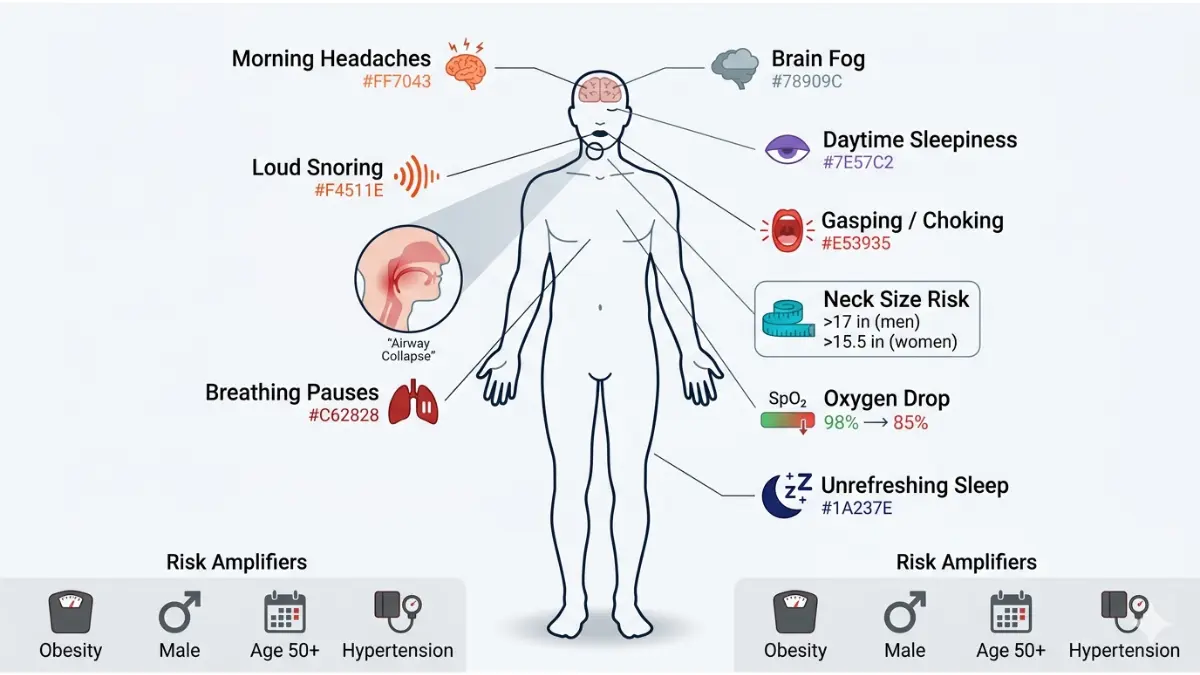
Most people don’t realize they stop breathing in their sleep. They only notice the downstream effects: morning headaches, brain fog, exhaustion that no amount of sleep fixes.
If you recognize yourself in any of these warning signs, it’s time to talk to your doctor:
- Loud snoring or gasping sounds witnessed by a partner or family member
- Excessive daytime sleepiness — falling asleep during meetings, driving, or watching TV
- Morning headaches occurring 3+ times per week
- Waking up choking or gasping during the night
- Unrefreshing sleep — you sleep 8 hours and still feel exhausted
- Neck circumference over 17 inches (men) or 15.5 inches (women) — a key physical risk marker
- Frequent nighttime urination — a lesser-known OSA symptom
You can run a quick health check using our Symptom Checker if you’re unsure whether your symptoms warrant a doctor visit. And if you’re always tired regardless of how many hours you sleep, our guide on always feeling tired no matter how much sleep you get explains what conditions could be behind that exhaustion.
What This Means For You: If you have 2 or more of these symptoms, don’t wait. Sleep apnea is linked to hypertension, stroke, atrial fibrillation, and type 2 diabetes. Early diagnosis changes outcomes dramatically.
Before the Sleep Lab — How Doctors Screen You First
Most patients don’t walk into a sleep lab on day one. There’s a structured pre-diagnostic phase that determines whether a sleep study is even needed.
Step 1: The Clinical Interview
Your doctor will ask about your sleep history, snoring frequency, witnessed breathing pauses, and daytime function. They’ll also review your medical history for conditions that raise OSA risk:
- Obesity (BMI over 30 — check yours with our BMI Calculator)
- Hypertension
- Type 2 diabetes
- Atrial fibrillation
- Hypothyroidism
- PCOS
- History of stroke
Step 2: Physical Examination
Your doctor will assess:
- Neck circumference
- Jaw and airway anatomy (retrognathia, enlarged tonsils)
- Body weight and BMI
- Blood pressure
Step 3: The STOP-Bang Questionnaire
The STOP-Bang is the most widely used clinical screening tool for OSA. It’s an 8-question yes/no survey based on the most reliable risk factors.
| Letter | Question |
|---|---|
| S — Snoring | Do you snore loudly? |
| T — Tired | Are you often tired or sleepy during the day? |
| O — Observed | Has anyone seen you stop breathing during sleep? |
| P — Pressure | Do you have or are you being treated for high blood pressure? |
| B — BMI | Is your BMI greater than 35? |
| A — Age | Are you older than 50? |
| N — Neck | Is your neck circumference greater than 16 inches? |
| G — Gender | Are you male? |
Scoring:
- 0–2: Low risk of OSA
- 3–4: Intermediate risk
- 5–8: High risk — sleep study strongly recommended
The Critical Limitation No Competitor Tells You
Here’s what most health websites won’t say: approximately 60% of people who score high on STOP-Bang do NOT actually have OSA. The tool has high sensitivity but low specificity — meaning it catches most real cases but also flags many people who don’t have the condition.
A STOP-Bang score does not diagnose sleep apnea. It only tells your doctor whether to order a sleep study.
A 2025 modification published in PeerJ (PMC) showed that for patients with BMI below 35, adjusting the cutoffs for age (≥40), BMI (≥23), and neck circumference (≥35 cm) significantly improved sensitivity — reaching 93% accuracy at a score of 3.
What This Means For You: If your STOP-Bang score is high, don’t panic. It’s a starting point, not a verdict. A confirmed diagnosis requires an objective sleep test.
The Two Ways Sleep Apnea Is Officially Diagnosed
Once your doctor decides you need testing, there are two paths. Which one you take depends on your health history, symptoms, and risk profile.
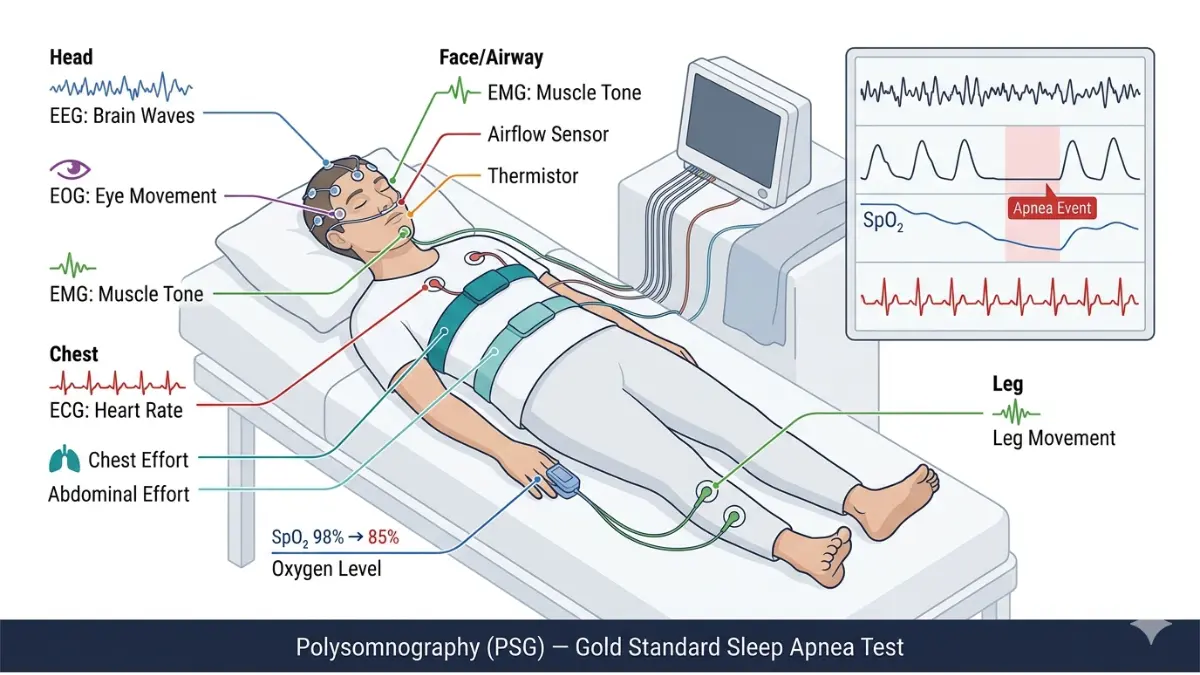
Path 1: In-Lab Polysomnography (PSG) — The Gold Standard
Polysomnography is the most comprehensive sleep test available. You spend one night in a sleep clinic while trained technologists monitor your body across 7 biological channels simultaneously.
What PSG Measures:
| Channel | What It Detects |
|---|---|
| EEG (electroencephalogram) | Brain wave activity and sleep stages |
| EOG (electrooculogram) | Eye movements (REM detection) |
| EMG (electromyogram) | Muscle activity and limb movements |
| ECG (electrocardiogram) | Heart rhythm and rate |
| Nasal/oral airflow sensors | Breathing cessation events |
| Chest/abdominal bands | Respiratory effort |
| Pulse oximeter | Blood oxygen saturation (SpO₂) |
According to AASM clinical guidelines (PMC), PSG is strongly recommended — not optional — for patients with:
- Significant cardiorespiratory disease
- Neuromuscular conditions
- Suspected central sleep apnea
- Chronic opioid use
- History of stroke
- Severe insomnia
Split-Night Protocol: In many US sleep labs, if your PSG shows clear OSA in the first half of the night, the second half is used for CPAP pressure titration — saving you a second visit.
For a deeper breakdown of what happens during a sleep study, read our detailed guide on sleep study and polysomnography.
Path 2: Home Sleep Apnea Test (HSAT) — Convenient, But With Limits
A Home Sleep Apnea Test lets you sleep in your own bed while a small wearable device records key respiratory data. It’s more convenient and costs less than a lab study.
Important limitation: HSAT devices do not record EEG signals. This means they cannot measure actual sleep stages — they estimate sleep from movement and breathing patterns. This causes HASTs to frequently underestimate OSA severity compared to PSG.
HSAT is appropriate for:
- Healthy adults with a high pre-test probability of moderate-to-severe OSA
- No significant cardiac, pulmonary, or neurological comorbidities
- No other suspected sleep disorders (narcolepsy, parasomnias, PLMD)
Monitor Type Comparison Table — Unique to This Guide
| Monitor Type | Setting | EEG Included? | Channels | Best Used For |
|---|---|---|---|---|
| Type I (PSG) | Sleep lab | ✅ Yes | Full (7+) | Gold standard, complex cases |
| Type II | Home | ✅ Yes | Full | High-risk mobile patients |
| Type III (HSAT) | Home | ❌ No | 4+ respiratory | Uncomplicated moderate-severe OSA |
| Type IV | Home | ❌ No | 1–2 channels | Screening only — not diagnostic |
What This Means For You: Don’t choose your test type based on convenience alone. If your doctor recommends in-lab PSG, there’s a clinical reason. A home test that returns negative results in a high-risk patient should always be followed up with PSG.
What Your AHI Score Actually Means — Decoded
After your sleep test, your results hinge on one critical number: the Apnea-Hypopnea Index (AHI).
AHI = total number of apneas + hypopneas ÷ hours of sleep
It tells you how many times per hour your breathing fully stopped (apnea) or significantly reduced (hypopnea) during the night.
AHI Severity Classification
| AHI Score | Severity | Events Per Hour | Clinical Impact |
|---|---|---|---|
| < 5 | Normal | Fewer than 5 | Minimal disruption |
| 5–14 | Mild OSA | 5–14 | Daytime fatigue, reduced concentration |
| 15–29 | Moderate OSA | 15–29 | Oxygen drops, cardiovascular strain begins |
| ≥ 30 | Severe OSA | 30 or more | Serious hypoxemia, elevated stroke and heart attack risk |
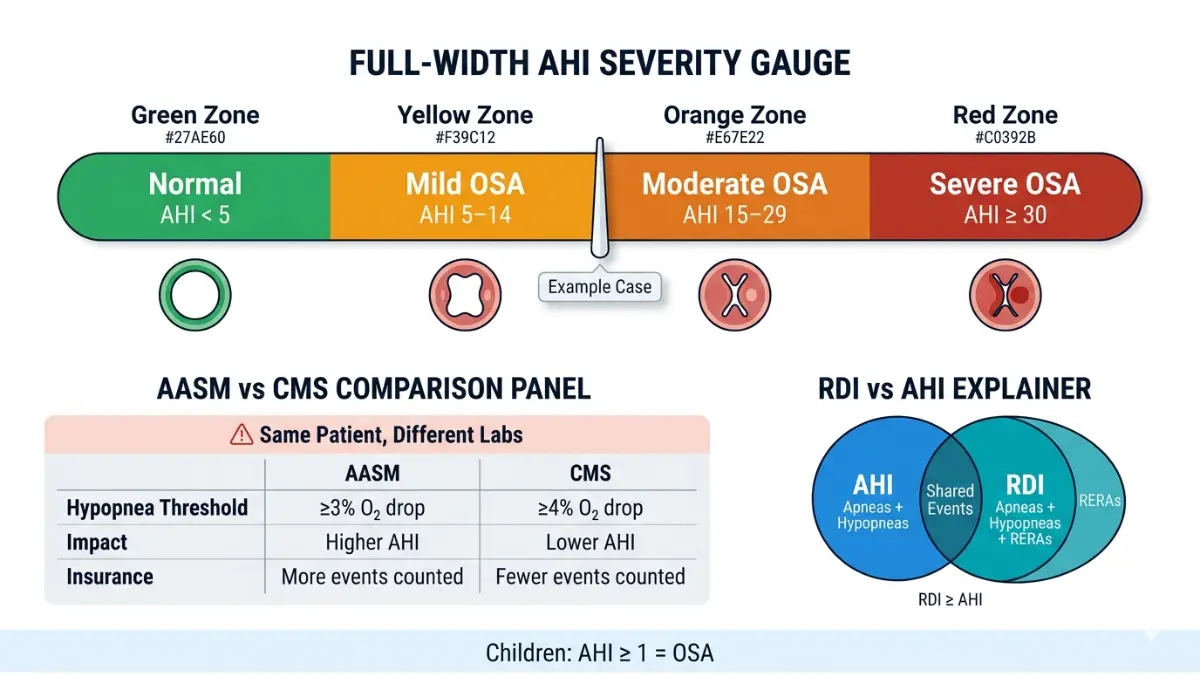
The AHI Discrepancy Most Patients Never Learn About
Here’s a critical fact that no major competitor article explains:
Your AHI score can differ between labs — even on the same night of data.
- AASM criteria defines a hypopnea as a ≥30% drop in airflow + ≥3% oxygen desaturation
- CMS (Medicare/insurance) criteria requires ≥4% desaturation for the same event to count
This single 1% difference means the same patient can have an AHI of 18 at one lab and 11 at another — and potentially not qualify for insurance-covered CPAP under the stricter CMS standard.
If your results are borderline, always ask your sleep physician which scoring criteria your lab used.
RDI vs. AHI — They Are Not the Same
The Respiratory Disturbance Index (RDI) includes respiratory effort-related arousals (RERAs) in addition to full apneas and hypopneas. RDI is almost always higher than AHI. Some patients with normal AHI still have significant OSA-related symptoms because their RDI is elevated.
Pediatric vs. Adult Thresholds
In children, the diagnostic threshold is AHI ≥ 1 event per hour — compared to ≥5 in adults. Parents should not assume that a child’s results are being evaluated using the same scale.
What This Means For You: An AHI of 6 in an adult with no symptoms may be managed conservatively. An AHI of 6 in a child is a confirmed OSA diagnosis requiring treatment. Always ask your doctor which criteria apply to your specific case.
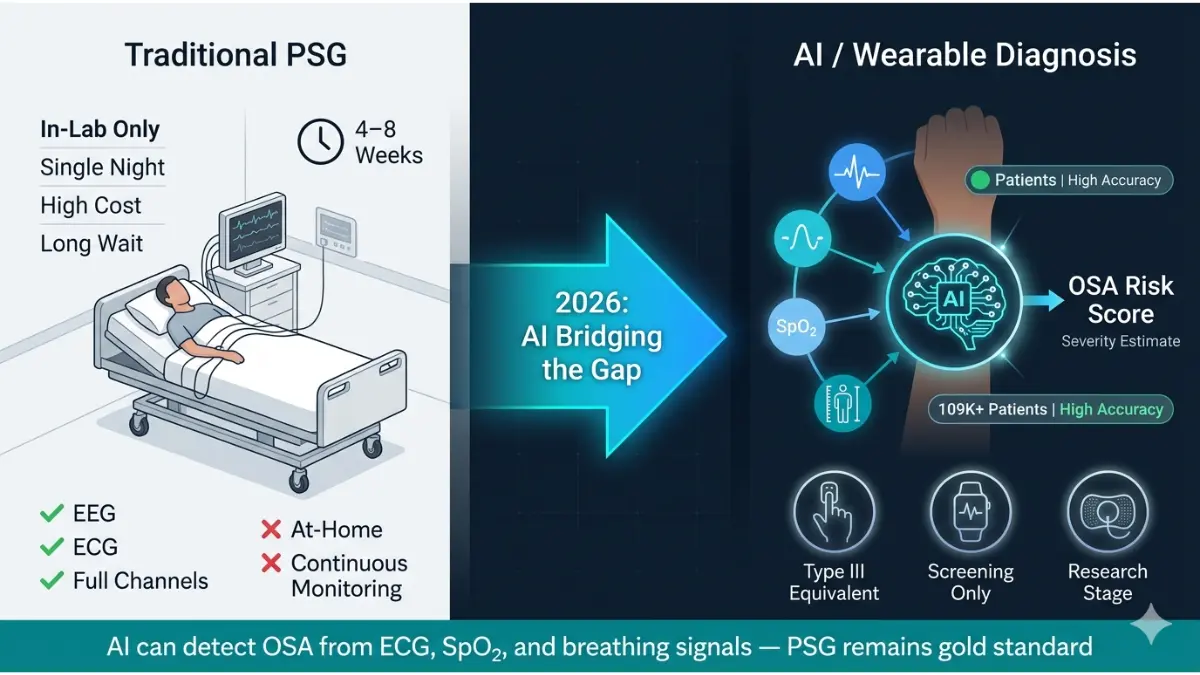
The 2026 Frontier — AI Diagnosis, Wearables & What’s Changing
The biggest gap in every competitor article on sleep apnea diagnosis is this: they don’t tell you what’s happening right now.
The Scale of the Crisis
According to PMC research, the annual economic burden of undiagnosed sleep apnea in the United States alone was estimated at $150 billion — and that figure is from 2015. The number is substantially higher today.
OSA affects an estimated 26% of American adults aged 30–70, yet the vast majority remain undiagnosed and untreated.
AI Is Reshaping How Sleep Apnea Gets Detected
A 2025 systematic review published in PMC analyzed 65 studies involving 109,046 patients and found that AI-powered diagnostic algorithms consistently exceeded traditional screening tools in accuracy, sensitivity, and specificity.
AI systems are now able to identify OSA risk from:
- ECG signals — cardiac rhythm irregularities that correlate with apnea events
- Respiratory sound analysis — microphone-based snore pattern recognition
- Peripheral oximetry data — oxygen desaturation curves analyzed by machine learning
- Anthropometric data — BMI, age, neck circumference processed through logistic regression
The American Academy of Sleep Medicine has formally called for diagnostic methods that move beyond AHI alone — incorporating demographic, comorbidity, and symptom data for more accurate screening.
What About Smartwatches and Wearables?
Several FDA-cleared consumer devices now offer respiratory tracking and blood oxygen monitoring, including the Apple Watch, Fitbit, and Withings ScanWatch. The WatchPAT device — a clinical-grade wearable using peripheral arterial tonometry — is used as a Type III-equivalent HSAT in accredited US sleep centers.
What these devices can do:
- Track blood oxygen levels during sleep
- Detect irregular breathing patterns
- Flag potential disruptions for physician review
What they cannot do:
- Confirm a clinical OSA diagnosis
- Replace a PSG or accredited HSAT
- Determine OSA severity or guide CPAP pressure settings
If your wearable or smartwatch is flagging breathing irregularities during sleep, treat that as a strong signal to speak with a sleep specialist — not as a diagnosis. You may also want to review the warning signs of a sleep disorder to better understand what symptoms to bring to your appointment.
What This Means For You: AI-assisted tools are promising, but as of 2026, a PSG or accredited HSAT remains the only path to an official OSA diagnosis recognized by the AASM and covered by US insurance providers.
After Your Diagnosis — Severity, Next Steps & When to Act Today
A confirmed OSA diagnosis is the start of a treatment journey, not the end of a diagnostic one. What happens next depends on your AHI severity, symptoms, and overall health.
Treatment Pathway by Severity
Mild OSA (AHI 5–14):
- Positional therapy (sleeping on your side reduces AHI by up to 50% in position-dependent cases)
- Weight loss — a 10% reduction in body weight produces a meaningful decrease in AHI (Canadian Thoracic Society, per PMC)
- Oral appliances (mandibular advancement devices)
- Reduced alcohol and sedative use, particularly before sleep
Since obesity is the single largest modifiable risk factor for OSA, use our Weight Loss Calculator to set a realistic target and our BMR Calculator to understand your baseline caloric needs.
Moderate OSA (AHI 15–29):
- CPAP (Continuous Positive Airway Pressure) — the frontline treatment
- Oral appliances as an alternative for CPAP-intolerant patients
- Lifestyle modification as a complement, not a replacement
Severe OSA (AHI ≥ 30):
- CPAP is mandatory
- Referral to cardiology if hypertension, atrial fibrillation, or heart failure is present
- Surgical evaluation for patients with significant anatomical obstruction
- Bariatric surgery consideration for morbidly obese patients (AASM-supported)
See a Doctor This Week If You:
- Have been told you stop breathing during sleep
- Wake up gasping or choking regularly
- Fall asleep involuntarily during the day
- Have uncontrolled hypertension despite medication
- Are experiencing excessive daytime sleepiness that affects your work or driving safety
- Have a bed partner who refuses to sleep in the same room due to your snoring
For context on how poor sleep compounds into larger health issues, read our article on what causes insomnia and explore sleep disorders: symptoms and causes.
The NHLBI (National Heart, Lung, and Blood Institute) provides authoritative patient resources on OSA risk, diagnosis, and treatment options for US patients.
⚕️ Medical Disclaimer: This article is for educational purposes only and does not constitute medical advice, diagnosis, or treatment. Always consult a board-certified physician or AASM-accredited sleep specialist for a proper evaluation and individualized care plan.
Frequently Asked Questions — Sleep Apnea Diagnosis
1. What tests are done to diagnose sleep apnea?
The two main tests are polysomnography (PSG), an overnight in-lab sleep study, and a Home Sleep Apnea Test (HSAT). PSG is the gold standard and measures brain waves, breathing, oxygen levels, and heart activity simultaneously. HSAT measures respiratory data only, without sleep staging.
2. Can you diagnose sleep apnea at home?
A Home Sleep Apnea Test (HSAT) can confirm OSA in uncomplicated adult patients with a high pre-test probability. However, it cannot replace in-lab PSG for patients with complex medical conditions, suspected central sleep apnea, or other sleep disorders.
3. What is a normal AHI score?
An AHI below 5 events per hour is considered normal for adults. Fewer than 5 breathing disruptions per hour indicates no clinically significant sleep-disordered breathing.
4. What AHI score confirms sleep apnea?
An AHI of 5 or more per hour — combined with symptoms such as daytime sleepiness or witnessed apneas — confirms obstructive sleep apnea in adults. Without symptoms, an AHI of 15 or more is sufficient for diagnosis.
5. How accurate is a home sleep apnea test?
HSAT is moderately accurate for uncomplicated OSA but tends to underestimate AHI severity because it records respiratory data without confirmed sleep time. A negative or inconclusive HSAT result in a high-risk patient must be followed by in-lab PSG.
6. What happens during a polysomnography sleep study?
You arrive at a sleep clinic in the evening and sleep in a private room while sensors track your brain activity, eye movements, muscle tone, heart rhythm, airflow, respiratory effort, and blood oxygen. A trained sleep technologist monitors the data in real time throughout the night.
7. Can a smartwatch diagnose sleep apnea in 2026?
No. While FDA-cleared wearables can track oxygen levels and flag breathing irregularities, no consumer device is currently approved to diagnose sleep apnea. They may serve as useful screening flags to prompt a clinical evaluation.
8. What is the STOP-Bang questionnaire?
STOP-Bang is an 8-question clinical screening tool that estimates your risk of OSA based on snoring, daytime tiredness, witnessed apnea, blood pressure, BMI, age, neck size, and gender. A score of 5–8 indicates high risk, but it cannot diagnose sleep apnea on its own.
9. Can children be diagnosed with sleep apnea the same way as adults?
The testing method is similar, but the diagnostic threshold is different. In children, an AHI of 1 or more events per hour confirms OSA — compared to 5 or more in adults. Pediatric sleep apnea often presents differently and requires specialist evaluation.
10. How long does it take to get a sleep apnea diagnosis?
The timeline varies. An initial GP referral takes 1–4 weeks. A sleep study appointment may take 2–8 weeks depending on your location and whether you opt for in-lab or home testing. Results interpretation typically takes 1–2 weeks after the study.
11. What is the difference between AHI and RDI?
AHI counts only apneas and hypopneas per hour. RDI (Respiratory Disturbance Index) also includes respiratory effort-related arousals (RERAs), making it a broader measure. RDI is always equal to or higher than AHI — some patients with a normal AHI still have elevated RDI and significant symptoms.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.
