On This Page – Quick Medical Summary
What a high creatinine result actually means
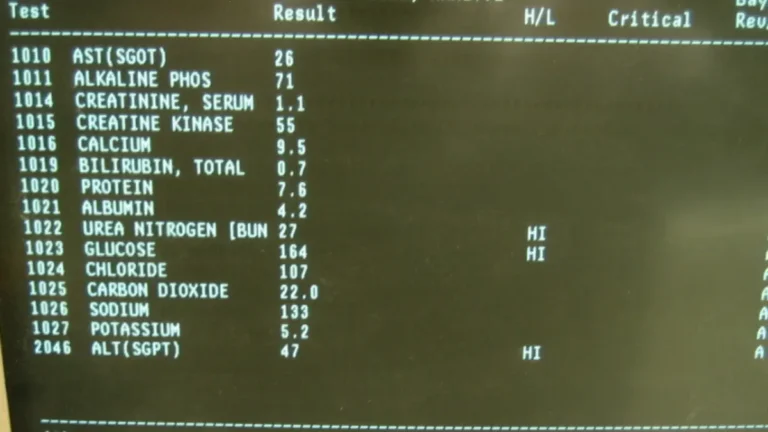
Seeing “creatinine — HIGH” on a blood test is unsettling, because it pattern-matches to kidney failure in most people’s minds. In the large majority of cases, a single mildly high reading is not that emergency — but it is worth understanding. Find your situation:
- Feel fine, just saw the flag → read what counts as high and the harmless causes below.
- You lift, eat high protein, or take creatine → the “false alarm” section is for you.
- Diabetes, high blood pressure, older, or one kidney → focus on the kidney-related causes and next steps.
- New swelling, very little urine, or breathless → read the red-flag section now and seek care.
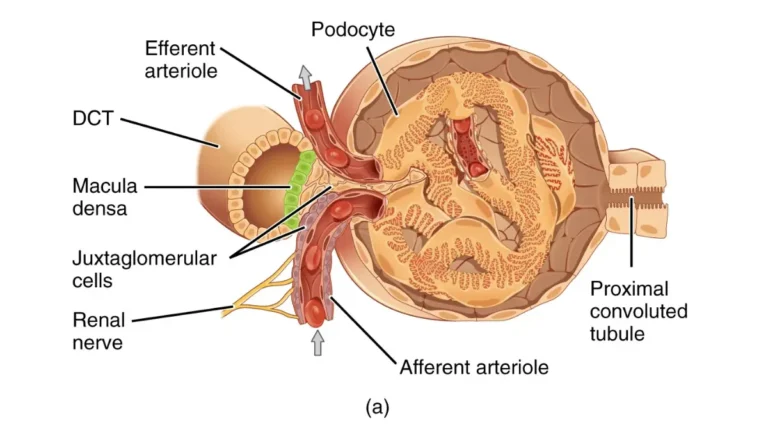
Creatinine is a waste product your muscles make around the clock, and healthy kidneys filter it into your urine, per MedlinePlus. Because it comes from muscle and leaves through the kidneys, your level reflects both how much muscle you carry and how well your kidneys filter.
ℹ️ Medical Disclaimer: This article is general health education, not a diagnosis, treatment plan, or medication guidance, and not a substitute for individual care. Creatinine results and any decisions about medications, procedures, or insurance should be reviewed with a licensed clinician — a primary care physician or a nephrologist. If you have the emergency symptoms described below, seek urgent care or call your local emergency number.
What counts as high, and why the raw number can mislead
There is no single universal cutoff, because normal creatinine depends on who you are. As a general guide, MedlinePlus puts a typical serum creatinine at about 0.7–1.3 mg/dL for men and 0.5–0.95 mg/dL for women. Women tend to run lower mainly because they carry less muscle on average, not because their kidneys work less well.
📊 Clinical Data Point: Typical serum creatinine — roughly 0.7–1.3 mg/dL (men) and 0.5–0.95 mg/dL (women). Source: MedlinePlus (U.S. National Library of Medicine). Always read your result against the reference range printed on your own lab report, which each lab sets itself.
The more useful number sits right beside it: your eGFR, or estimated glomerular filtration rate, which your lab calculates from your creatinine, age, and sex using the current race-free 2021 CKD-EPI equation supported by NIDDK. A normal adult eGFR is usually above 90. Because creatinine production rises with muscle mass, a muscular 30-year-old and a frail 80-year-old can share the same creatinine number while having very different kidney function — so clinicians read the two together.
That is the lesson most competing articles skip: one value out of range is a prompt to look closer, not a verdict. See how creatinine fits with your other panel values in the guide to the normal ranges for a comprehensive metabolic panel, and read more in the NIH’s guidance on estimating kidney function.
Harmless and temporary reasons creatinine goes up
Many high creatinine results have nothing to do with kidney damage. Muscle mass is the first factor: more muscle means more creatinine produced daily, so athletes often sit at the high end with healthy kidneys.
Creatine supplements raise serum creatinine as a normal byproduct, not a sign of harm — in a 12-week controlled trial, resistance-trained people on a high-protein diet took creatine while researchers measured true kidney filtration, and kidney function did not change. A high-protein diet, especially cooked red meat, can also raise creatinine by roughly 0.1–0.8 mg/dL (about 10–50% above baseline) without kidney damage, per peer-reviewed literature.
🔬 How It Works: Creatine stored in muscle steadily converts into creatinine, and your creatine pool grows when you supplement or eat lots of protein. More creatine in means more creatinine out — the two are chemically linked. Because eGFR is calculated from creatinine, a bigger creatine pool can make eGFR look lower even when filtration is completely normal.
Dehydration temporarily reduces blood flow to the kidneys and raises creatinine, usually reversing with rehydration. And certain drugs — including the antibiotic trimethoprim and the acid-reducer cimetidine — raise serum creatinine simply by blocking its secretion in the kidney tubule, without damaging the kidney. When the picture is unclear, clinicians can order cystatin C, a marker unaffected by muscle mass.
✅ Patient Action: Before you retest, tell your clinician if you take creatine, eat very high protein, started a new medication, or were dehydrated on test day, and ask: “Could this explain my result, or should we recheck and consider a cystatin C test?” To gauge the effect, estimate your daily water needs or check a sensible daily protein target; the creatine evidence is in a controlled trial that measured true kidney filtration.
When high creatinine points to a kidney problem
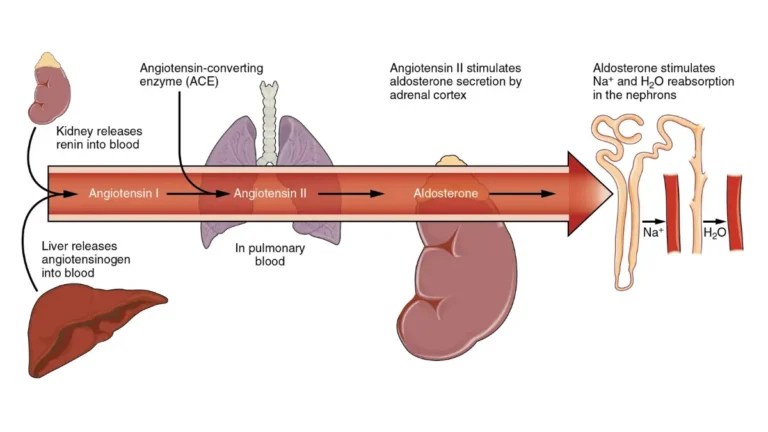
Sometimes a high creatinine does signal that the kidneys need attention, and clinicians sort the causes into three groups. Reduced blood flow is the most common — from dehydration, blood loss, heart failure, severe infection, or drugs like NSAIDs and ACE inhibitors. Direct kidney damage comes from acute tubular necrosis, inflammation of the kidney’s filters, or nephrotoxic medications. Blockage of urine flow comes from kidney stones, an enlarged prostate, or a tumor.
Timing is the other distinction. Acute kidney injury develops over hours to days, while chronic kidney disease means reduced filtration or damage persisting three months or more, per NIDDK and the National Kidney Foundation. An eGFR below 60 for three months, or above 60 with signs of damage such as protein in the urine, is how chronic kidney disease is defined.
🩺 Physician Note: A common point of confusion is that one high creatinine cannot, by itself, reveal whether a problem is acute or chronic. Clinicians rely on your trend — comparing today’s value to previous results — which is why an old baseline result is so valuable.
According to the CDC, diabetes and high blood pressure are the leading causes of kidney failure, together accounting for about two of every three new cases.
✅ Patient Action: If you have diabetes, high blood pressure, or take NSAIDs regularly, ask: “Is this acute or chronic, what’s driving it, and should I see a nephrologist?” Review how creatinine pairs with its companion marker in the guide to your BUN and creatinine kidney markers.
When to worry: red flags that need urgent care
This is the clearest line in the article. Most single, mild creatinine elevations without symptoms call for a recheck rather than an emergency visit — but a specific set of symptoms alongside a high result can signal acute kidney injury and should not wait.
⚠️ Clinical Warning: Seek urgent care if a high creatinine comes with any of these, which the National Kidney Foundation lists as signs of acute kidney injury: passing very little or no urine; new swelling in the legs, ankles, feet, or around the eyes; shortness of breath; chest pain or pressure; confusion; or severe fatigue. These can reflect dangerous fluid or electrolyte buildup and need same-day evaluation, not home monitoring. If symptoms come on suddenly or worsen quickly, treat it as an emergency.
One reason these are urgent is that failing kidneys can let potassium climb, and high potassium can affect the heart — see how that marker behaves in the guide to high potassium and your kidneys. When kidneys can’t clear extra fluid, it backs up into the legs and lungs, which is why swelling plus breathlessness is a combination to take seriously. If your result is mildly high and you feel well, a planned recheck — not the emergency room — is usually right.
✅ Patient Action: If you have any red-flag symptom, seek urgent care or call your local emergency number today — do not wait to retest. If you feel well but want to think through non-emergency symptoms, check kidney-related symptoms, remembering it is an educational tool, not a substitute for care.
What your doctor will do after a high creatinine result
A high creatinine starts a process, not a diagnosis. The first move is often simply to repeat the test and check your eGFR trend, because a single value can be thrown off by hydration, diet, or a recent hard workout.
From there, clinicians commonly add targeted tests. A urine albumin-to-creatinine ratio checks for protein leaking into the urine, an early sign of damage that NIDDK recommends for a fuller assessment. Where muscle mass complicates the reading, a cystatin C test can refine the estimate, and a kidney ultrasound can look for stones or blockage.
✅ Patient Action: Before your visit, gather previous blood-test results and list your medications and supplements, then ask: “Should we recheck this, test my urine for protein, or check cystatin C given my muscle mass?” See the wider picture in the guide to how to read your full CMP results. Bringing prior results matters, because your trend tells your clinician more than any single value.
How common is kidney disease, and why early detection matters
Putting your result in context helps replace fear with perspective. Kidney disease is common and usually silent early on, which is exactly why a routine blood test is often what catches it.
📊 Clinical Data Point: About 14% of U.S. adults — roughly 37 million people — are estimated to have chronic kidney disease, and most don’t know it; even among those with severely reduced kidney function who aren’t on dialysis, around 40% are unaware. Source: CDC national kidney disease report (updated 2026).
Those numbers can read as alarming, but the takeaway is encouraging: because early kidney disease rarely causes symptoms, a flagged creatinine is useful information that gives you and your clinician a head start, and there is more that can be done when issues are found early. If you have diabetes, high blood pressure, or a family history, ask your clinician whether you should have regular kidney checks — an eGFR and a urine albumin test. Explore the data through the CDC’s national kidney disease data.
High creatinine: frequently asked questions
1. What is the main cause of high creatinine?
The most common cause of persistently high creatinine is reduced kidney filtration, but harmless factors like high muscle mass, creatine, a high-protein diet, or dehydration often explain it. Have any persistent elevation checked by your clinician.
2. Can dehydration cause high creatinine?
Yes. Dehydration reduces blood flow to the kidneys and temporarily raises serum creatinine, usually reversing once you rehydrate. This is one reason clinicians often repeat the test. Mention it to your clinician before retesting.
3. Should I worry about slightly high creatinine?
Usually a single, mildly high creatinine without symptoms is not an emergency and needs a recheck, not urgent care. Worry more if it persists across tests or comes with red-flag symptoms your clinician should evaluate.
4. Do creatine supplements raise creatinine?
Yes, creatine raises serum creatinine as a normal byproduct without harming the kidneys; a 12-week controlled trial found no change in true kidney function. Tell your clinician you take it, since it can make eGFR look lower.
5. Does a high-protein diet raise creatinine?
Yes. A high-protein diet, especially cooked red meat, can raise serum creatinine by roughly 0.1 to 0.8 mg/dL without kidney damage — enough to trigger a false alarm. Mention your diet to your clinician before retesting.
6. What creatinine level is dangerous?
There is no universal “dangerous” number, because normal creatinine depends on muscle mass, age, and sex. Clinicians judge it by your eGFR, your trend, and any symptoms; a high result with red-flag symptoms needs urgent evaluation.
7. Can high creatinine be reversed?
It depends on the cause. Elevations from dehydration, supplements, diet, or acute kidney injury are often reversible, while chronic kidney disease usually is not fully reversible but can be slowed. Only your clinician can determine which applies.
8. What are the symptoms of high creatinine?
Early on there are often none, which is why it is usually caught on a blood test. Significantly reduced kidney function may cause swelling, fatigue, reduced urine output, nausea, or shortness of breath. Report these to your clinician.
9. What tests are done after a high creatinine result?
Clinicians usually repeat the creatinine test, check your eGFR trend, and add a urine albumin-to-creatinine test for protein; some order cystatin C or a kidney ultrasound. Bring prior results, since your trend matters more than one value.
10. Does high creatinine always mean kidney disease?
No. Muscle mass, creatine, a high-protein diet, dehydration, and certain medications can all raise it without kidney damage. A persistent elevation, however, should be evaluated by your clinician.
11. When should I see a doctor about high creatinine?
See your clinician promptly for any persistent elevation, or urgently if you have red-flag symptoms such as very low urine output, new swelling, breathlessness, chest pain, or confusion. For a mild, symptom-free elevation, a planned recheck is usually appropriate.
The bottom line on a high creatinine result
A high creatinine sounds like a crisis, but for most people it is a signal to look closer rather than a diagnosis. The number rises for plenty of harmless reasons — muscle, creatine, protein, dehydration, and certain medications — and for kidney-related ones too, which is why context, your trend, and your symptoms matter more than a single value.
Understand your result, watch for the red flags, and follow up. Share this number and any symptoms with your clinician, bring prior results so they can see the trend, and ask whether a recheck or a urine test is the right next step. You can also review what other flagged values mean in the guide to what abnormal CMP results can mean.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.