On This Page – Quick Medical Summary
Hearing the name of a chemotherapy regimen for the first time — FOLFIRINOX, gemcitabine — can feel like being handed a decision you never trained for. Both are standard, guideline-recommended treatments for pancreatic cancer, and the honest answer to “which is better” is that it depends on your fitness and your situation, not on a single survival number.
Where you are right now shapes which part of this guide matters most. If you were just diagnosed and are weighing a first treatment, the comparison of effectiveness and side effects below is for you. If you are mainly worried about how hard treatment will be, the side-effect and quality-of-life section speaks to that directly. If you have already had surgery and are deciding on follow-up chemotherapy, the post-surgery section is yours. And if you are a caregiver, the warning-signs section will help you know when to act.
This guide compares the two treatments using verified trial data, then explains how oncologists actually choose between them. You can see where both fit within the full range of pancreatic cancer treatment options in our wider guide.
ℹ️ Medical Disclaimer: This article explains pancreatic cancer treatments, survival statistics, chemotherapy regimens, and warning symptoms for general educational purposes only. It does not diagnose disease, recommend a specific treatment or medication, or replace professional care. Treatment decisions depend on details only your own team can assess. Consult a board-certified medical oncologist before making or changing any treatment decision.
What FOLFIRINOX and gemcitabine actually are
The first thing to understand is what each treatment is made of, because the two differ sharply in intensity.
FOLFIRINOX: a four-drug combination
FOLFIRINOX is a combination of four chemotherapy drugs — oxaliplatin, irinotecan, leucovorin, and fluorouracil (5-FU) — given together by infusion, usually on a two-week cycle. Because it combines four agents, it is more intensive and tends to cause more side effects than a single drug.

Adapted from Wikimedia Commons Chemotherapy iv.jpg, licensed under public domain.
🔬 How It Works: Each drug in FOLFIRINOX interferes with rapidly dividing cancer cells in a different way — some block the cell’s ability to copy its DNA, another damages DNA directly, and another disrupts the repair process. Combining them attacks the cancer on several fronts at once, which is part of why the regimen is both more effective and harder on the body.
Gemcitabine: alone or paired with another drug
Gemcitabine is a single chemotherapy drug. On its own it is gentler, but for patients well enough to tolerate more, it is usually paired with nab-paclitaxel (albumin-bound paclitaxel) to make it more effective. This distinction matters: gemcitabine alone and gemcitabine-plus-nab-paclitaxel are not the same treatment, and much of the confusion patients feel comes from this single point. Gemcitabine given by itself is now used mainly for people who are older or more frail. The National Cancer Institute’s overview of pancreatic cancer treatment covers where each regimen fits.
Is FOLFIRINOX or gemcitabine stronger?
The clearest head-to-head evidence comes from a trial called PRODIGE 4/ACCORD 11, published in the New England Journal of Medicine in 2011.
The PRODIGE 4 trial, head-to-head
In that trial of 342 patients — all with good performance status — median overall survival averaged 11.1 months with FOLFIRINOX versus 6.8 months with gemcitabine. Progression-free survival (time before the cancer grew again) was 6.4 versus 3.3 months, and tumors shrank meaningfully in 31.6% of FOLFIRINOX patients versus 9.4% of those on gemcitabine.
📊 Clinical Data Point: Median overall survival was 11.1 months with FOLFIRINOX vs 6.8 months with gemcitabine (hazard ratio 0.57) — Source: Conroy et al., New England Journal of Medicine, 2011 (PRODIGE 4/ACCORD 11).
Why the numbers need context
That gap is real, but it is not the choice most patients actually face. The trial compared FOLFIRINOX to gemcitabine alone — not to today’s gemcitabine-plus-nab-paclitaxel, which reached roughly 8.5 months in a separate trial. The FOLFIRINOX patients were also specifically the fit ones. Survival figures describe groups, not individuals, and outcomes shift with stage; our guide to how each stage shapes the outlook explains why.
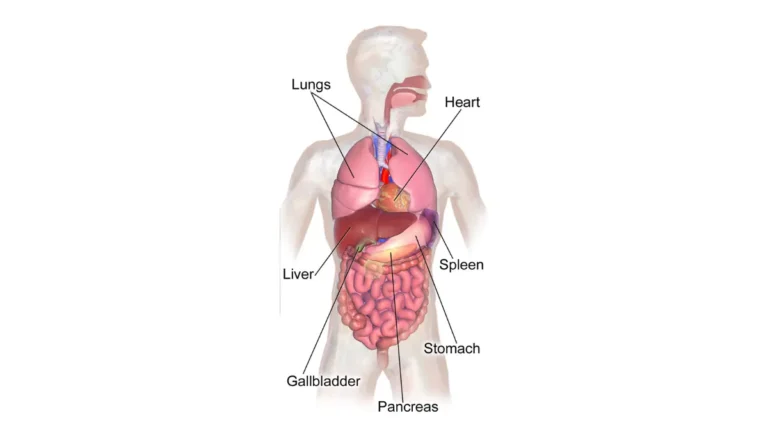
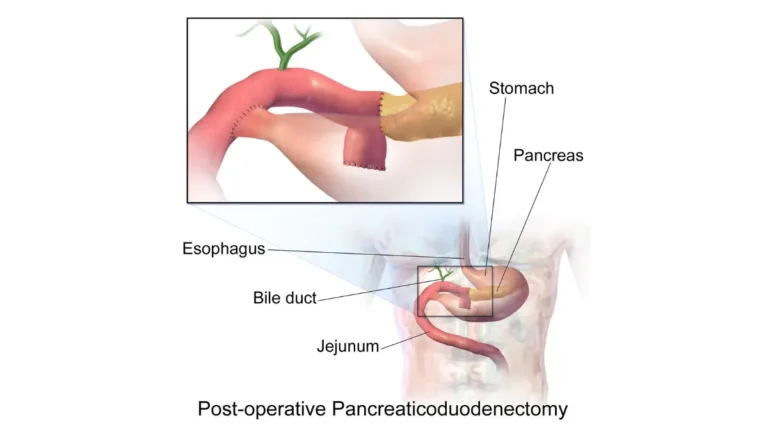
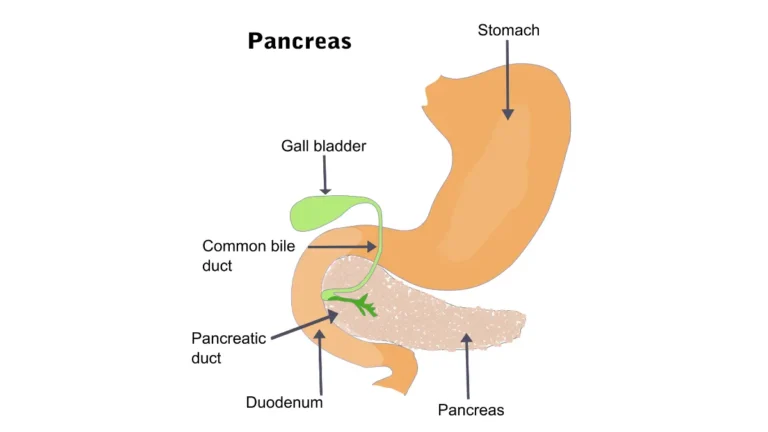
Adapted from Wikimedia Commons Abdomal organs body.svg, licensed under [CC BY-SA 3.0]
How oncologists choose between them
The decision turns less on the headline numbers and more on how well a person is functioning day to day.
Performance status is the deciding factor
Doctors use a scale called ECOG performance status, where 0 means fully active and higher numbers mean more limited. Current NCCN guidance (2025) maps treatment to fitness. For good performance status (ECOG 0–1), preferred first-line options are FOLFIRINOX or modified FOLFIRINOX, gemcitabine plus nab-paclitaxel, and a newer regimen called NALIRIFOX. For reduced fitness (ECOG 2), gemcitabine plus nab-paclitaxel is preferred, and gemcitabine alone is used when someone is more frail.
🩺 Physician Note: FOLFIRINOX is generally considered too demanding for older or frailer patients, and the median age at pancreatic cancer diagnosis is about 71. Choosing a gemcitabine-based regimen for a less-fit person is the guideline-consistent decision — not a lesser or “giving-up” option.
Where NALIRIFOX and genetic testing fit
NALIRIFOX (liposomal irinotecan with oxaliplatin and 5-FU/leucovorin) is an FDA-approved first-line option from the NAPOLI-3 trial. Guidelines also recommend germline genetic testing for everyone with metastatic pancreatic cancer, because BRCA1, BRCA2, or PALB2 mutations favor platinum-based regimens like FOLFIRINOX. You can review inherited risk factors with our genetic risk tool.
✅ Patient Action: Ask your medical oncologist: “Given my performance status and overall health, why is this regimen the right fit for me — and have I had germline genetic testing?”
Side effects and quality of life: the real trade-off
The real trade-off is tolerability. FOLFIRINOX is more effective on average, but it asks more of the body.
FOLFIRINOX: more effective, more demanding
Severe (grade 3/4) side effects were markedly higher with FOLFIRINOX than gemcitabine in the PRODIGE 4 trial: neutropenia (low white blood cells) in about 46% versus 19%, febrile neutropenia in 5.4% versus 0.6%, severe diarrhea in 12.7% versus 1.2%, and severe nerve-related symptoms in roughly 9% versus none. More than 40% of FOLFIRINOX patients needed growth-factor support to protect their white blood cells.
⚠️ Clinical Warning: Febrile neutropenia — a fever during chemotherapy when white blood cells are low — can signal a dangerous infection and is treated as a medical emergency. It was several times more common with FOLFIRINOX than gemcitabine, which is one reason fitness matters when choosing it.
What the quality-of-life data showed
The picture is not simply “harsher equals worse.” The trial’s quality-of-life analysis found that FOLFIRINOX patients went longer before a definitive decline in quality of life than gemcitabine patients, despite the rougher early side effects. Side effects are monitored and managed actively throughout treatment; our guide to managing chemotherapy side effects covers what that looks like.
✅ Patient Action: Ask your oncology team: “Which side effects are most likely with my regimen, and exactly how will you prevent and treat them?”
Which is used after pancreatic cancer surgery?
For people whose tumor was removed surgically, the comparison shifts to the adjuvant (after-surgery) setting — and here the FOLFIRINOX advantage is even larger. Whether surgery is an option depends on whether a tumor is resectable or unresectable.
The PRODIGE 24 trial: after-surgery results
In the PRODIGE 24 trial, adjuvant modified FOLFIRINOX produced median overall survival of 54.4 months versus 35.0 months for gemcitabine; five-year results confirmed the benefit at 53.5 versus 35.5 months. Disease-free survival was 21.6 versus 12.8 months.
📊 Clinical Data Point: After surgery, adjuvant modified FOLFIRINOX reached a median overall survival of 54.4 months vs 35.0 months with gemcitabine — Source: Conroy et al., NEJM 2018; five-year update, JAMA Oncology 2022 (PRODIGE 24/CCTG PA.6).
What modified FOLFIRINOX means
“Modified” FOLFIRINOX uses an adjusted, gentler version of the regimen. As in the metastatic setting, it is reserved for patients fit enough to tolerate it: severe side effects occurred in about 76% of the modified-FOLFIRINOX group versus 52% on gemcitabine. Timing also matters, and depends on recovery from surgery — our guide to recovery after pancreatic cancer surgery explains what that involves.
Warning signs to take seriously during chemotherapy
Whichever regimen you or a loved one receives, certain symptoms during treatment need prompt attention rather than waiting.
Call your oncology team promptly if…
- A fever develops, which can be a sign of infection when white blood cells are low
- Diarrhea becomes severe or persistent, raising the risk of dehydration
- There are signs of infection such as chills, a sore throat, or a new cough
When to seek emergency care
Seek emergency care for a high fever with shaking chills, signs of significant dehydration (dizziness, very little urine, confusion), or difficulty breathing. These are general signs — follow the specific instructions and temperature thresholds your own care team gave you, and use the after-hours number they provided rather than waiting for the next scheduled visit.
Frequently asked questions about FOLFIRINOX vs. gemcitabine
1. Is FOLFIRINOX or gemcitabine stronger?
In the PRODIGE 4 trial, FOLFIRINOX produced longer survival than gemcitabine alone (about 11.1 versus 6.8 months). But that comparator was gemcitabine by itself, and FOLFIRINOX suits only fitter patients. Your oncologist can say which is right for your case.
2. What’s the difference between FOLFIRINOX and gemcitabine?
FOLFIRINOX combines four chemotherapy drugs given together, making it more intensive. Gemcitabine is a single drug, gentler on its own and often paired with nab-paclitaxel for fitter patients. The main difference is intensity and how many drugs are involved.
3. Why would a doctor choose gemcitabine over FOLFIRINOX?
Often because of fitness. FOLFIRINOX is demanding, so for older or frailer patients a gemcitabine-based regimen is the guideline-consistent choice — not a downgrade. Performance status is the main deciding factor. Ask your oncologist why your regimen fits you.
4. What are the main side-effect differences?
FOLFIRINOX causes more severe side effects than gemcitabine, including higher rates of low white blood cells (neutropenia), febrile neutropenia, severe diarrhea, and nerve symptoms. Gemcitabine is generally gentler. Side effects are monitored and managed, so ask your team how.
5. How long do people live on each treatment?
In PRODIGE 4, median survival was about 11.1 months with FOLFIRINOX versus 6.8 with gemcitabine alone. These are group averages from one trial, not individual predictions, and outcomes vary by stage and fitness. Discuss your specific outlook with your oncologist.
6. Is gemcitabine alone still used?
Yes. Gemcitabine on its own is now used mainly for patients who are older or more frail and cannot tolerate more intensive combinations. Fitter patients usually receive it combined with nab-paclitaxel, or receive FOLFIRINOX instead.
7. What is modified FOLFIRINOX?
Modified FOLFIRINOX is an adjusted, gentler version of the four-drug regimen, designed to reduce side effects while keeping effectiveness. It is the version studied after pancreatic cancer surgery in the PRODIGE 24 trial. Your oncologist decides whether it suits you.
8. Which treatment is used after pancreatic cancer surgery?
After surgical removal, modified FOLFIRINOX showed longer survival than gemcitabine in the PRODIGE 24 trial (about 54.4 versus 35.0 months), for patients fit enough to tolerate it. The choice still depends on recovery and fitness. Discuss timing with your oncologist.
9. What is NALIRIFOX and how does it compare?
NALIRIFOX is an FDA-approved first-line option using liposomal irinotecan with oxaliplatin and 5-FU/leucovorin. It is a preferred choice for fit patients alongside FOLFIRINOX and gemcitabine-plus-nab-paclitaxel. Your oncologist can explain whether it fits your situation.
10. Can you switch from gemcitabine to FOLFIRINOX?
Treatment can change based on how the cancer responds and how well side effects are tolerated. Switching regimens is a decision your oncologist makes using scans and your overall condition — it is not something to adjust on your own.
11. Does FOLFIRINOX cure pancreatic cancer?
FOLFIRINOX can extend survival and, after surgery, lower the chance of return — but the trials measured longer survival, not a guaranteed cure. Whether long-term remission is possible depends on stage and whether the tumor can be removed. Discuss your case with your oncologist.
The bottom line — and your next conversation
Both FOLFIRINOX and gemcitabine-based treatments are legitimate, guideline-recommended options for pancreatic cancer. FOLFIRINOX is more effective on average and the standard choice for fitter patients, while a gemcitabine-based regimen can be the right — and sometimes the stronger — choice for someone who is older or more frail. The decision rests on fitness and treatment setting, not on a single number.
The most useful next step is an informed conversation with your medical oncologist. Bring your questions about performance status, side effects, genetic testing, and which setting applies to you, so the recommendation you receive is one you understand and trust.
About this content
This medical content is prepared through a structured publishing workflow with expert writing, clinical review and editorial quality checks.

Board Certifications: Internal Medicine (2005); Medical Oncology (2008); Hematology (2009) Experience: 20 years | Location: Houston, Texas Education: BS Biology, Duke University (1999); MD, Baylor College of Medicine…

Board Certifications: Internal Medicine (2010); Clinical Pharmacology (2013) Experience: 15 years | Location: San Francisco, California Education: BS Molecular Biology, Caltech (2000); MD/PhD, UCSF School of Medicine (2007);…

Board Certifications: Preventive Medicine (2010); Public Health & General Preventive Medicine (2010) Experience: 15 years | Location: Washington, DC Education: BA Public Policy, Georgetown University (2001); MD, George…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.