On This Page – Quick Medical Summary
If you have heard that an mRNA vaccine for pancreatic cancer is showing promise, the honest answer is this: the science is real and encouraging, but the vaccine is still experimental and available only through clinical trials — not yet as an approved treatment.
What you need next depends on where you are. If you or a loved one was recently diagnosed, the sections on who the trials are for and how to ask about them matter most. If surgery has already happened and you worry about recurrence, the trial-status and access sections speak directly to you. If you are comparing experimental options, the data and limitations sections show what the evidence does and does not prove. And if a headline brought you here, the sections on what the results mean — and what this vaccine is not — will help you read the news accurately.
This article explains the leading pancreatic cancer mRNA vaccine, what its trials have found, where the research stands now, and the concrete step to take with your care team.
ℹ️ Medical Disclaimer: This article is general health education, not medical advice, and does not diagnose disease, recommend treatment, or replace care from your own clinicians. Decisions about pancreatic cancer diagnosis, surgery, chemotherapy, medication, insurance, and clinical trial participation depend on details only your treating team can assess. Discuss any treatment or trial question with a board-certified medical or surgical oncologist before acting.
What an mRNA cancer vaccine is and how it works
An mRNA cancer vaccine is a treatment for people who already have cancer, not a shot to prevent it. The leading candidate for pancreatic cancer is autogene cevumeran (also called BNT122), developed by BioNTech and Genentech, a member of the Roche Group.
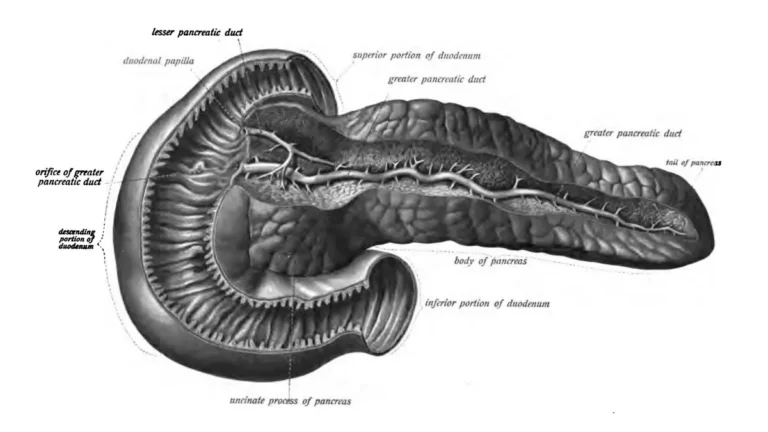
How autogene cevumeran is made from your tumor
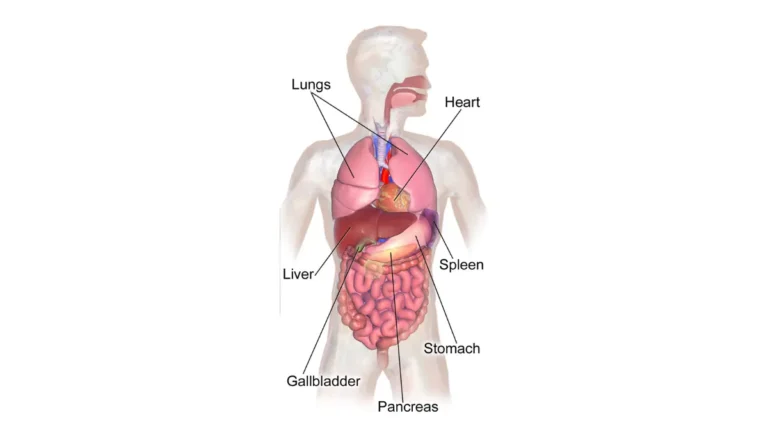
Unlike an off-the-shelf vaccine, this one is built individually for each person. After surgeons remove the tumor, it is genetically sequenced to find neoantigens — abnormal proteins unique to that patient’s cancer. A custom vaccine is then manufactured to teach the immune system to recognize those specific markers.
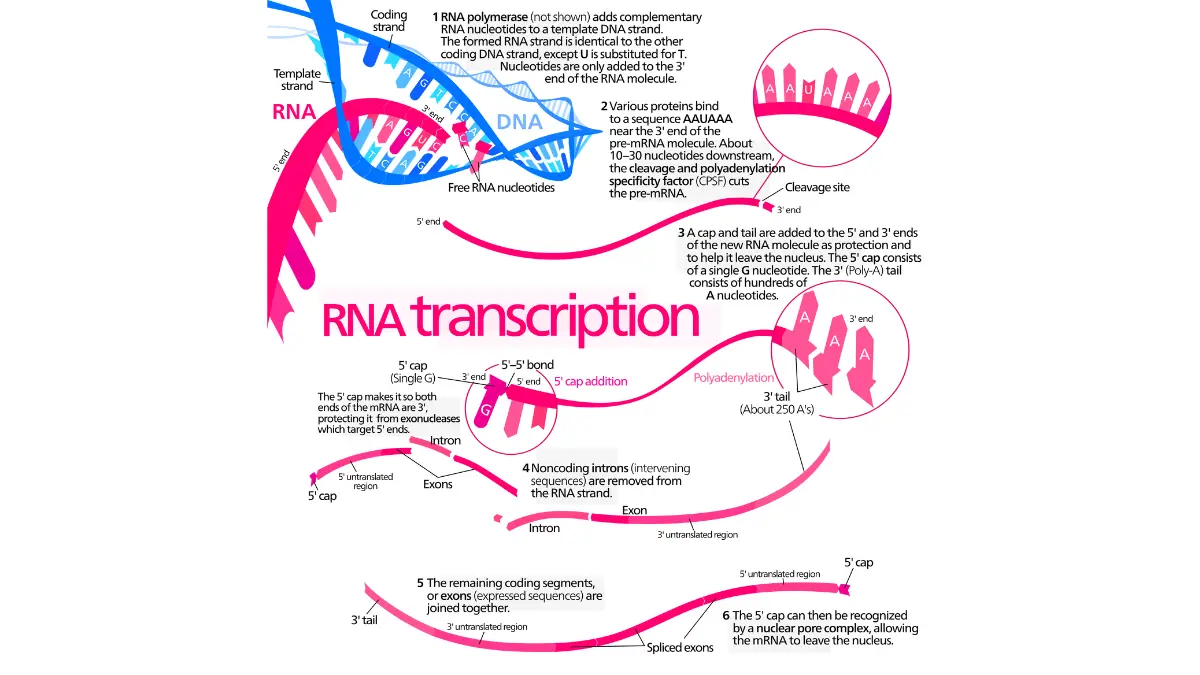
🔬 How It Works: The vaccine delivers mRNA instructions that prompt the body to make copies of the tumor’s neoantigens. This trains immune cells called T cells to find and destroy cancer cells carrying those markers — including hidden cells too small to show on a scan.
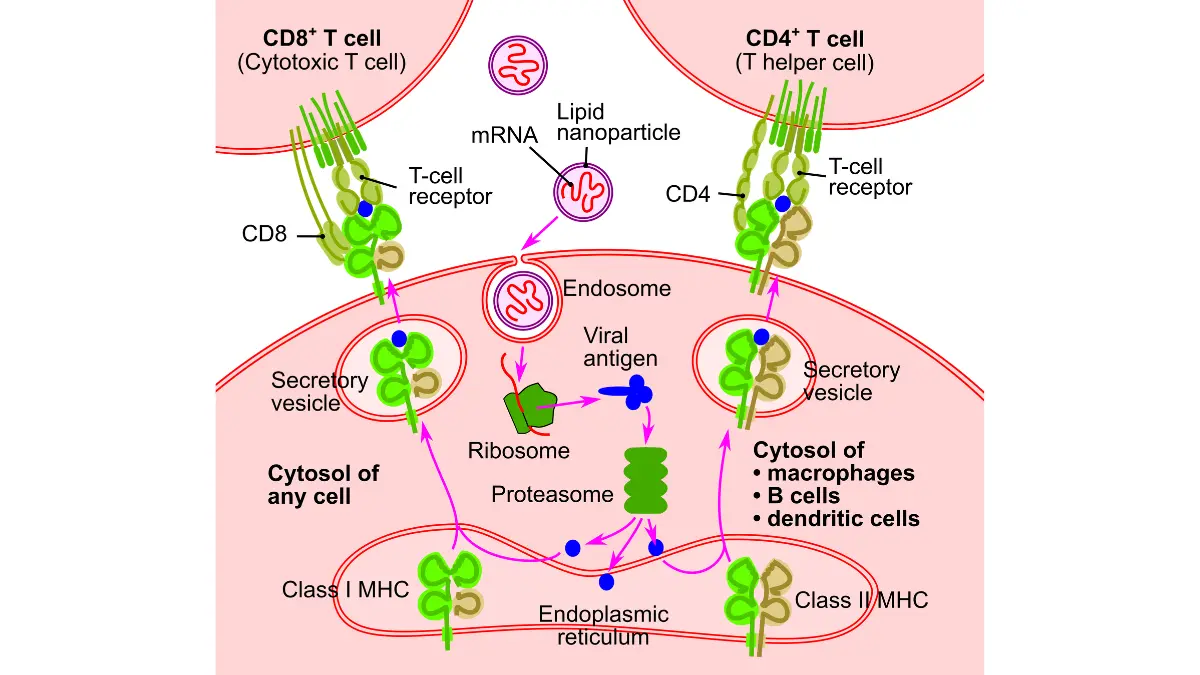
Adapted from Wikimedia Commons RNA vaccine-en, licensed under CC BY-SA 3.0.
Why it is given with surgery, chemotherapy, and a checkpoint inhibitor
The vaccine does not replace standard care. In the trials it is added after surgery, alongside the chemotherapy regimen used for pancreatic cancer and atezolizumab, a checkpoint inhibitor that helps the immune system work against cancer. The aim is to lower the chance the cancer returns, not to shrink an existing tumor.
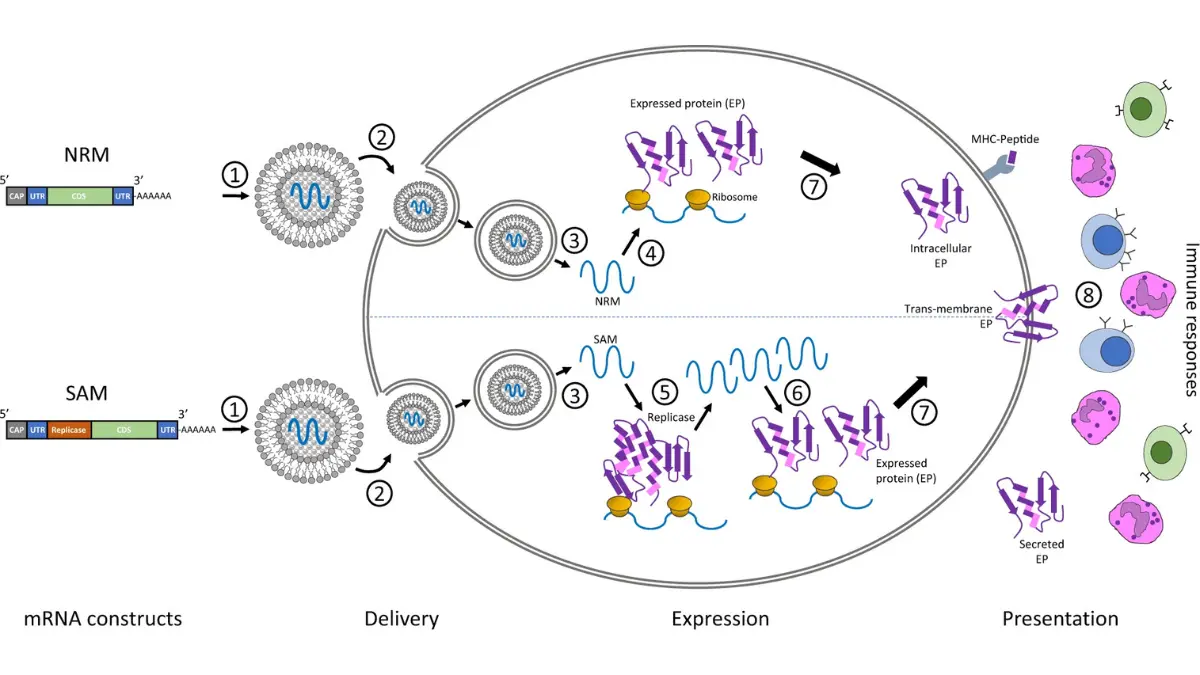
Adapted from Wikimedia Commons 41541 2020 159 Fig1 HTML, licensed under CC BY 4.0.
What the trial data actually shows so far
The results behind the headlines come from one small early study, and reading them accurately matters more than reading them hopefully. The Phase 1 trial enrolled just 16 patients with surgically removed pancreatic cancer at Memorial Sloan Kettering, led by surgeon-scientist Vinod Balachandran, MD, and was designed mainly to test safety and immune response, as documented in the Phase 1 study record.
The Phase 1 results in plain numbers
Half of the patients responded to the vaccine; half did not. The most striking finding came years later.
📊 Clinical Data Point: Of the 16 patients, 8 developed a vaccine-induced immune response. At six-year follow-up reported in 2026, 7 of those 8 responders were still alive, compared with 2 of the 8 non-responders. — Source: data presented at the AACR Annual Meeting 2026 (Balachandran et al.).
For context, survival depends heavily on the stage at diagnosis, and pancreatic cancer remains one of the hardest cancers to treat.
📊 Clinical Data Point: Overall 5-year relative survival for pancreatic cancer is about 13% across all stages, rising to roughly 44% when the cancer is found early and still confined to the pancreas. — Source: NCI SEER and American Cancer Society, 2026.
Why these results are promising but not proof
Three facts keep this in perspective: only 16 people were studied, only half responded, and the survival difference is a within-trial correlation in a handful of selected patients — not proof the vaccine extends life across the wider population. A larger randomized trial is needed before anyone can say the benefit is real.
Where the research stands now
A single small study cannot establish that a treatment works, which is why the program has moved into a larger, controlled trial. That study — a randomized Phase 2 trial known as IMCODE003 — is enrolling now.
The Phase 2 trial now enrolling
It is testing whether adding autogene cevumeran to standard treatment lowers recurrence better than standard treatment for pancreatic cancer alone.
| Detail | Current status |
|---|---|
| Candidate | Autogene cevumeran (BNT122) |
| Trial | Phase 2, randomized (IMCODE003) |
| Sponsor | Genentech with BioNTech |
| Who can join | ~260 patients with surgically removed pancreatic cancer |
| Key detail | Enrolling in the U.S. and expanding globally; results expected ~2028–2029 |
Source: ClinicalTrials.gov record (NCT05968326) and trial sponsor information, 2026.
FDA status and a realistic timeline
The vaccine is not FDA approved and cannot be prescribed outside a trial. Definitive answers about whether it improves survival are years away, with key results from the Phase 2 study expected around 2028–2029. Timelines in cancer research frequently shift, so no availability date is confirmed.
Could this be an option for you?
For most people searching today, the honest answer is “probably not yet” — but everyone has a clear next step worth taking. The current trials are open to people whose pancreatic cancer is operable and has been, or can be, surgically removed.
Who the current trials are for
The vaccine is being studied in the adjuvant setting, meaning after surgery, so eligibility starts with whether a tumor can be surgically removed. People with advanced or widely spread disease are generally not candidates for these specific trials, and surgery to remove the tumor is the gateway your team decides on.
✅ Patient Action: At your next appointment, ask a medical or surgical oncologist: “Is my cancer potentially operable, and am I a candidate for an mRNA neoantigen vaccine trial or another clinical trial after surgery?” Bring the trial identifier (NCT05968326) to the conversation.
Because inherited mutations such as BRCA can affect pancreatic cancer care, it can help to understand your inherited risk factors before treatment planning — though no tool determines trial eligibility.
⚠️ Clinical Warning: Be cautious of clinics advertising “cancer vaccines” outside registered clinical trials. Legitimate mRNA cancer vaccines are available only through trials listed on ClinicalTrials.gov, and delaying proven treatment to pursue an unverified product can be dangerous.
What this vaccine is not
Holding on to accurate hope means being clear about the limits of what has been shown. This is genuinely promising science, but several things are not yet true.
Not yet a proven or available treatment
It is not approved, not a cure, and not available outside a clinical trial. It is designed to reduce the chance of recurrence after surgery — not to replace surgery or chemotherapy, and not to remove an existing tumor. The evidence so far is a 16-person Phase 1 study plus an ongoing Phase 2 trial, which is encouraging but not definitive.
Adapted from Wikimedia Commons MRNA, licensed under CC BY-SA 3.0.
What the Phase 1 safety data showed
On safety, the early signal was reassuring.
📊 Clinical Data Point: In the Phase 1 trial, the vaccine was generally well tolerated; one patient had a vaccine-related grade 3 fever and high blood pressure, with no other serious vaccine-related side effects reported. — Source: published Phase 1 results (Nature, 2023) and conference reporting.
These are early findings in a small group, so the full safety picture will become clearer as the larger trial reports its results.
Where mRNA cancer vaccines are heading
This single vaccine is part of a fast-moving field rather than a one-off experiment. The same personalized, neoantigen-targeting approach is being tested across several cancers, which is why researchers are watching it closely.
Beyond pancreatic cancer
Autogene cevumeran is also in mid-stage testing for colorectal cancer, and dozens of other mRNA cancer vaccines are in trials for tumors including melanoma, lung, and breast cancer. Pancreatic cancer is an especially demanding test because its tumors have long resisted immune-based treatment.
What to watch next
The pancreatic field is advancing on several fronts at once, including other experimental treatments such as KRAS-targeted drugs. The most meaningful update for the vaccine will come when the Phase 2 trial reports, expected around 2028–2029, showing whether the early signal holds in a larger, controlled study.
Frequently asked questions about the pancreatic cancer mRNA vaccine
1. Is there an mRNA vaccine for pancreatic cancer available now?
No. A pancreatic cancer mRNA vaccine called autogene cevumeran is being tested in clinical trials, but it is experimental and not yet approved or available as standard treatment. People can access it only by enrolling in a registered trial. Ask a medical or surgical oncologist whether a trial is appropriate for your situation.
2. What is the pancreatic cancer mRNA vaccine called?
The leading candidate is autogene cevumeran, also known as BNT122, developed by BioNTech and Genentech (part of the Roche Group). It is an individualized vaccine, built from each patient’s own tumor, and is the furthest along of the mRNA vaccines being studied for pancreatic cancer.
3. How does the pancreatic cancer mRNA vaccine work?
After surgery removes the tumor, it is sequenced to find neoantigens — abnormal proteins unique to that cancer. A custom mRNA vaccine then trains the immune system’s T cells to recognize and attack remaining cancer cells carrying those markers, aiming to reduce the risk the cancer returns.
4. Did the mRNA vaccine work in the pancreatic cancer trial?
In the 16-patient Phase 1 trial, 8 patients developed an immune response. At six-year follow-up, 7 of those 8 responders were still alive versus 2 of 8 non-responders. This is an encouraging early signal, but the study was small and cannot prove the vaccine extends survival.
5. Can I get the pancreatic cancer mRNA vaccine?
Only through a clinical trial. Current trials enroll people whose pancreatic cancer is operable and has been or can be surgically removed, in the period after surgery. Eligibility is decided case by case. Ask a medical or surgical oncologist whether you qualify for a vaccine trial or another clinical trial.
6. What stage of pancreatic cancer is the vaccine for?
The current trials focus on earlier-stage, operable pancreatic cancer that can be surgically removed, giving the vaccine after surgery. People with advanced or widely spread disease are generally not candidates for these specific studies. Your oncologist can confirm whether your stage fits a trial.
7. Is the mRNA pancreatic cancer vaccine FDA approved?
No. The pancreatic cancer mRNA vaccine is investigational and has not been approved by the FDA. It cannot be prescribed outside a clinical trial, and any clinic offering a “cancer vaccine” outside a registered trial should be treated with caution.
8. When will the pancreatic cancer mRNA vaccine be available?
That depends on the ongoing randomized Phase 2 trial, with key results expected around 2028–2029. If those results confirm a meaningful benefit, further regulatory review would follow before any approval. There is no confirmed availability date, and research timelines often shift.
9. Is the pancreatic cancer mRNA vaccine safe?
In the Phase 1 trial it was generally well tolerated. One patient had a vaccine-related grade 3 fever and high blood pressure, with no other serious vaccine-related side effects reported. Because the study was small, the full safety picture will become clearer as the larger trial reports. Discuss risks with your oncologist.
10. Is the mRNA vaccine a cure for pancreatic cancer?
No. It is not a cure and is not designed to remove existing tumors. It is being studied to reduce the chance the cancer returns after surgery, alongside standard chemotherapy and immunotherapy. Whether it improves long-term survival is still being tested in a larger trial.
11. How is this different from the COVID mRNA vaccine?
Both use mRNA technology, but the purpose differs. COVID vaccines are preventive and identical for everyone. The pancreatic cancer mRNA vaccine is therapeutic and personalized — made individually from each patient’s tumor to treat existing disease by directing the immune system against that specific cancer.
The bottom line
The honest status is straightforward: a personalized mRNA vaccine for pancreatic cancer is showing real promise in early research, but it remains experimental and available only through clinical trials. The strongest signal so far comes from a small Phase 1 study, and a larger randomized trial now underway will determine whether that promise holds.
If this matters to you or someone you love, the single most useful step is a focused conversation with an oncologist about whether surgery is possible and whether a clinical trial fits your situation. For the wider picture, see how pancreatic cancer develops and is treated. Grounded hope, built on accurate information, serves patients better than headlines.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.