On This Page – Quick Medical Summary
A pancreatic cancer diagnosis lands hard, and the days before your first specialist visit can blur together with fear and unanswered questions. This guide gives you the questions to ask — and the plain-language context to use them — so you walk in prepared and leave with answers you actually understand.
How you use it depends on where you are right now:
- Just diagnosed and waiting for your first appointment? Begin with how to prepare, then the diagnosis and treatment questions.
- A caregiver or family member? The preparation and supportive-care sections will help you advocate and plan.
- Already weighing treatment paths? Skip ahead to treatment options, testing, and second opinions.
Whatever brought you here, the aim is the same: to help you become an informed partner in your own care. For the bigger picture of the disease, see our full guide to pancreatic cancer. None of this replaces your medical team — it helps you talk with them.
ℹ️ Medical Disclaimer: This article is general education, not medical advice for your specific situation. Decisions about pancreatic cancer diagnosis, staging, treatment, medication, surgery, and genetic testing must be made with your own board-certified oncology team. Survival statistics here are population averages and cannot predict any individual’s outcome. Always consult your oncologist, surgeon, or genetic counselor before acting on anything you read.
How to prepare for your first pancreatic cancer appointment
Walking in organized turns an overwhelming appointment into a working conversation, and a few steps beforehand change how much you understand and remember.
Confirm who you’ll see and what to bring
Find out which specialist you’re meeting. A medical oncologist plans systemic treatment like chemotherapy; a surgical oncologist or hepatobiliary surgeon assesses whether surgery is possible; a gastroenterologist may have run your initial workup. Bring a photo ID, insurance card, a current medication list, and any imaging discs or pathology reports you can collect.
Gather your records and your history
Request copies of your CT or MRI scans, biopsy results, and recent bloodwork in advance — your team will want them, and having them speeds planning. Write down your personal and family history of cancer, since that shapes testing recommendations. Knowing the tests used to diagnose pancreatic cancer helps you ask for the right ones.
Bring someone and capture the answers
Bring a trusted companion to listen and take notes — two sets of ears catch more than one. Ask whether you may record the conversation, and write your questions down beforehand so nothing slips away in the moment.
✅ Patient Action: Before the visit, call the office to confirm exactly which specialist you’re seeing and whether your scans and pathology have arrived — and if not, ask how to get them there in time.
Questions to ask about your diagnosis and stage
The first questions pin down exactly what you’re dealing with: what type and stage you have, and whether your tumor can be removed.
Stage vs. resectable: the distinction that drives treatment
Ask your team to explain your diagnosis in plain terms. Most pancreatic cancers are pancreatic adenocarcinoma, the most common exocrine type, though less common forms behave differently. Stage describes how far the cancer has spread; resectability describes whether surgery can remove it — and treatment is planned around resectability, not the stage number alone.
🔬 How It Works: Surgeons classify tumors as resectable (removable), borderline resectable (close to major blood vessels), unresectable/locally advanced (not removable), or metastatic (spread to distant organs). A small tumor can still be borderline resectable if it sits against a key artery — which is why this label, set by your surgeon, guides the plan. See resectable versus unresectable pancreatic cancer and how pancreatic cancer is staged.
What the survival statistics do and don’t mean
If you’ve searched survival rates, read them carefully and ask how your own situation compares.
📊 Clinical Data Point: Five-year relative survival is about 43.6% for localized pancreatic cancer, 17.0% for regional, and 3.4% for distant disease, with an overall rate of 13.7% — Source: NCI SEER, cases diagnosed 2016–2022. These are averages from people diagnosed years ago and cannot predict one person’s outcome.
✅ Patient Action: Ask your surgical oncologist or hepatobiliary surgeon: “Is my tumor resectable, borderline resectable, or unresectable — and what specifically would change that classification?”
Questions to ask about your treatment options
Once you understand your diagnosis, the next questions are about what can be done — learning the realistic options and the goal behind them, not deciding anything alone.
Surgery, chemo, and radiation: what may be on the table
Your team may discuss:
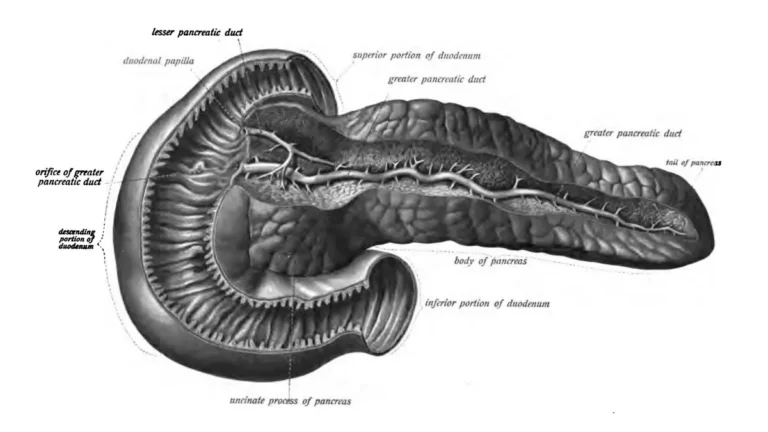
- Surgery when the tumor is resectable — a Whipple procedure (pancreaticoduodenectomy) for tumors in the head of the pancreas, or a distal pancreatectomy for the body or tail.
- Chemotherapy such as FOLFIRINOX or gemcitabine with nab-paclitaxel, sometimes given before surgery (neoadjuvant) or after it (adjuvant).
- Radiation therapy, used in certain situations alongside other treatments.
Ask which apply to you and why. Our overview of pancreatic cancer treatment options and what Whipple recovery involves can help you prepare follow-up questions.
Curative vs. control: ask about the goal
🩺 Physician Note: A question many people miss is the goal of treatment. Guidance frames pancreatic cancer treatment as either curative-intent (aiming to remove the cancer) or focused on controlling disease and easing symptoms. Knowing which your team is pursuing — and the planned sequence — changes how you weigh every option.
✅ Patient Action: Ask your medical oncologist: “Is the goal of my treatment to remove the cancer or to control it, what’s the recommended order of treatments, and am I a candidate for surgery now or later?” You can read more in the NCI’s patient treatment overview.
Questions to ask about genetic and biomarker testing
This is the set of questions most easily overlooked — and one of the most important. Testing your genes and your tumor can shape which treatments and trials are open to you.
Why germline genetic testing is recommended for everyone
National guidelines (NCCN) recommend germline genetic testing for every patient diagnosed with pancreatic adenocarcinoma, regardless of family history, because inherited mutations turn up even in people with no family history of cancer. Results can affect your treatment, your eligibility for clinical trials, and your relatives’ awareness of their own risk. Ask whether you’ve been referred for testing and genetic counseling — our guide to genetic testing for pancreatic cancer explains more.
Molecular profiling and what CA 19-9 means
🔬 How It Works: Tumor (somatic) molecular profiling examines the cancer’s own genes for targetable changes that may match a specific therapy or trial — especially recommended in advanced disease. CA 19-9 is a blood marker used mainly to track the disease over time, not to diagnose it alone; some people don’t produce it, so a single number rarely tells the whole story. Learn what CA 19-9 means.
✅ Patient Action: Ask your oncologist or a genetic counselor: “Should I have germline genetic testing and tumor molecular profiling, and could the results open up targeted treatments or a pancreatic cancer clinical trial?”
Questions about your care team and second opinions
You’re allowed to ask who’s treating you and where — and a second opinion is a normal, expected part of cancer care, not a betrayal of your team.
Why a second opinion is normal and welcomed
Getting a second opinion is common and won’t offend a good oncologist; many encourage it, and it rarely causes harmful delay. It can confirm your plan or surface an option you hadn’t heard, which is especially valuable if your diagnosis is complex or surgery is on the table.
Asking about experience and where to be treated
Experience matters in pancreatic cancer. Research has linked higher surgical and hospital volume to better outcomes after pancreatic surgery, so it’s fair to ask about a center’s track record. Ask whether your case is reviewed by a multidisciplinary team or tumor board, where specialists plan together.
🩺 Physician Note: Balancing experience against timing is real — you want a skilled team, but you also don’t want a long search to cause a harmful delay. A reasonable approach is to ask your current team whether a brief second opinion at a high-volume center would change anything before treatment begins.
✅ Patient Action: Ask any prospective center: “How many pancreatic cancer cases and Whipple procedures does this team handle each year, and will my case be reviewed by a tumor board?”
Questions about symptoms, support, and what to report right away
The last questions are about living through treatment — comfort, support, and knowing when to call. These matter as much as the medical plan.
Comfort, nutrition, and emotional support
Ask about palliative care (also called supportive care) early — it eases symptoms alongside treatment and isn’t only for end of life. Ask about pain control, including ways to manage pancreatic cancer pain, and whether you should see an oncology dietitian, since weight loss and digestion problems are common. Ask what emotional support — counseling, social work, support groups — is available to you and your family.
Asking about prognosis on your terms
You decide how much detail you want. It’s valid to ask “What does this mean for my future?” — or to say you’d rather not discuss numbers right now. Tell your team your preference so they can meet you where you are.
⚠️ Clinical Warning: Contact your care team promptly if you notice new or worsening jaundice (yellow skin or eyes), fever or chills, uncontrolled pain, persistent vomiting or an inability to keep fluids down, or leg swelling with sudden shortness of breath (a possible blood clot). These can signal complications that need quick attention.
✅ Patient Action: Ask your team: “Which symptoms should make me call you right away, and can I be referred now for palliative care and nutrition support alongside my treatment?”
Common questions after a pancreatic cancer diagnosis
1. What questions should I ask my doctor after a pancreatic cancer diagnosis?
After a newly diagnosed pancreatic cancer, ask what type and stage you have, whether the tumor is resectable, what treatments and goals are recommended, whether you need genetic and tumor testing, and how to reach your team. Bring the questions written down, and discuss the specifics with your oncology team.
2. How do I prepare for my first pancreatic cancer appointment?
Confirm which specialist you’re seeing, gather your scans, pathology, bloodwork, and medication list, and note your personal and family cancer history. Bring a companion to take notes and ask whether you can record the visit. Preparing this way helps you absorb and remember a difficult conversation.
3. What’s the difference between a medical oncologist and a surgical oncologist?
A medical oncologist plans and oversees systemic treatments like chemotherapy, while a surgical oncologist or hepatobiliary surgeon evaluates whether your tumor can be removed and performs the operation. Many people see both as part of a multidisciplinary team. Ask who is coordinating your overall care.
4. Should I get a second opinion for pancreatic cancer?
Yes — a second opinion is common and won’t offend a good team; many oncologists encourage it, and it rarely causes harmful delay. It can confirm your plan or reveal another option, which is especially valuable if surgery is being considered. Ask your team whether a second opinion would change anything.
5. What does resectable vs. unresectable pancreatic cancer mean?
Resectable means the tumor can be removed with surgery; unresectable (locally advanced) means it cannot, often because it involves major blood vessels. Borderline resectable sits between, and metastatic means it has spread to distant organs. Your surgeon sets this classification, and it drives your plan. Confirm your category with your team.
6. Should I get genetic testing if I have pancreatic cancer?
National guidelines recommend germline genetic testing for everyone diagnosed with pancreatic adenocarcinoma, regardless of family history, because inherited mutations appear even without one. Results can affect your treatment, trial eligibility, and your relatives’ risk awareness. Ask your oncologist or a genetic counselor whether testing has been ordered for you.
7. What is CA 19-9 and what does my number mean?
CA 19-9 is a blood marker used mainly to track pancreatic cancer over time and monitor response to treatment, not to diagnose it on its own. Some people don’t produce it, so one value rarely tells the whole story. Ask your oncologist how to interpret your specific result.
8. What treatment options will be discussed at my first visit?
Your team may discuss surgery (such as a Whipple procedure) when the tumor is resectable, chemotherapy like FOLFIRINOX or gemcitabine with nab-paclitaxel, and radiation in some cases, given before or after surgery. Which apply depends on your stage and resectability. Ask your oncologist which options fit your situation and why.
9. Should I ask about clinical trials right away?
Yes — ask about clinical trials early, not only after standard options. Trials can offer newer approaches, and tumor molecular profiling may match you to one. For someone newly diagnosed with pancreatic cancer, raising this at the first visit keeps every door open. Ask your oncologist which trials you may qualify for.
10. How do I ask about my prognosis — or choose not to know?
You control how much you hear. You can ask directly, “What does this mean for my future?”, or tell your team you’d prefer not to discuss numbers right now. Both choices are valid. Let your oncologist know your preference so the conversation matches what you actually want.
11. What symptoms should I report to my cancer care team right away?
Contact your team promptly for new or worsening jaundice, fever or chills, uncontrolled pain, persistent vomiting, or leg swelling with sudden breathlessness that may signal a blood clot. These can mean complications needing quick care. Ask your team in advance which symptoms warrant an urgent call.
Walking into your first visit with confidence
No one absorbs all of this at once, and you don’t have to. Print the questions that matter most to you, bring them to your appointment, and let your team fill in the rest.
You’ve just become an informed partner in your own care — someone who walks in with questions instead of only fear. Keep the people you trust close, take notes, and ask anything you don’t understand until it’s clear. Remember that the survival figures you may have read are population averages, not a verdict on your life. Your situation is yours, and your team is there to guide you through it one step at a time.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.