On This Page – Quick Medical Summary
Bariatric Surgery: Cost, Types & If You Qualify
Maria, a 42-year-old teacher from Ohio, struggled with obesity for 15 years despite trying every diet imaginable. After undergoing gastric bypass surgery in January 2024, she lost 78 pounds within nine months and reversed her type 2 diabetes completely. Bariatric surgery is a metabolic procedure that alters your digestive system to promote significant weight loss—typically 50-80% of excess body weight—and can cost between $12,000 to $35,000 depending on the procedure type and insurance coverage. The four primary types include gastric bypass, sleeve gastrectomy, gastric band, and duodenal switch, with qualification typically requiring a BMI of 40+ or BMI 35+ with serious obesity-related health conditions.
Why Bariatric Surgery Matters Now
More than 40% of American adults currently live with obesity, according to the latest Centers for Disease Control and Prevention data, yet fewer than 1% of eligible candidates undergo weight loss surgery annually. The reality is harsh: traditional diet and exercise programs fail long-term for 95% of people with severe obesity due to complex metabolic factors beyond willpower. Bariatric surgery addresses these biological mechanisms by reducing stomach capacity, altering hunger hormones, and in some procedures, decreasing nutrient absorption. Beyond weight loss, metabolic surgery resolves type 2 diabetes in 80% of patients, eliminates sleep apnea in 85% of cases, and significantly reduces cardiovascular disease risk.
Understanding your baseline is critical—use our free BMI Calculator to determine if you fall within the qualification range (BMI 35-40+ typically required). Coupling this with a Body Fat percentage calculator provides a comprehensive picture of your metabolic health status.
What You’ll Learn in This Guide
This evidence-based guide delivers everything you need to make an informed bariatric surgery decision:
- Complete procedure breakdown: Gastric bypass vs. sleeve gastrectomy vs. gastric band—which delivers the best outcomes for your situation
- 100% transparent cost analysis: Self-pay pricing, insurance coverage requirements, Medicare guidelines, and hidden expenses
- Qualification roadmap: BMI thresholds, comorbidity requirements, and the 6-month pre-approval process explained
- Real recovery timelines: What the first 6 weeks actually look like, plus long-term lifestyle changes
- Risk assessment: Complication rates, nutritional deficiencies, and how to minimize adverse outcomes
- Expert selection criteria: Finding MBSAQIP-accredited surgeons with proven track records
Medical Disclaimer: This article provides educational information about bariatric surgery options and should not replace personalized medical advice. Always consult with board-certified bariatric surgeons and your healthcare team before making treatment decisions. Individual results vary based on numerous factors including age, starting BMI, procedure type, and adherence to post-surgical protocols.
Types of Bariatric Surgery: Which Procedure Is Right for You?
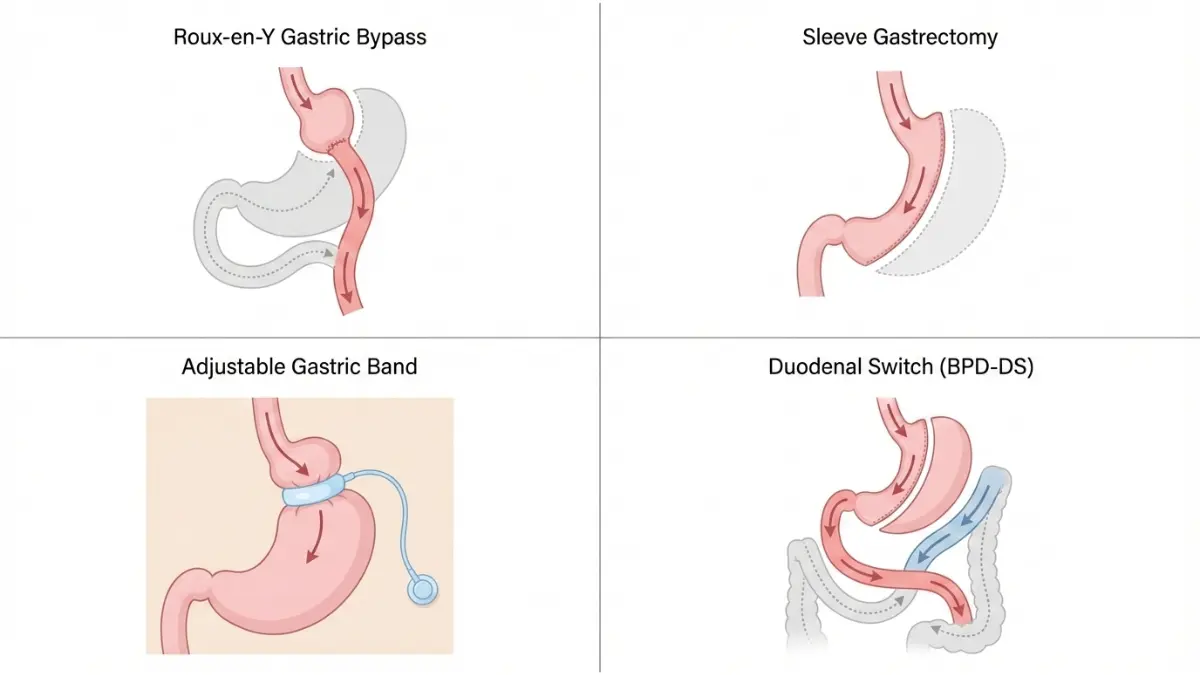
Choosing among the different types of bariatric surgery requires understanding how each procedure works, what results to expect, and which option aligns with your health profile. The American Society for Metabolic and Bariatric Surgery updated their clinical guidelines in 2022 to reflect evolving surgical techniques and long-term outcome data, with sleeve gastrectomy now representing 60% of all weight loss surgery procedures performed in the United States. Each bariatric surgery type offers distinct advantages and tradeoffs in terms of weight loss potential, complication rates, and lifestyle impact.
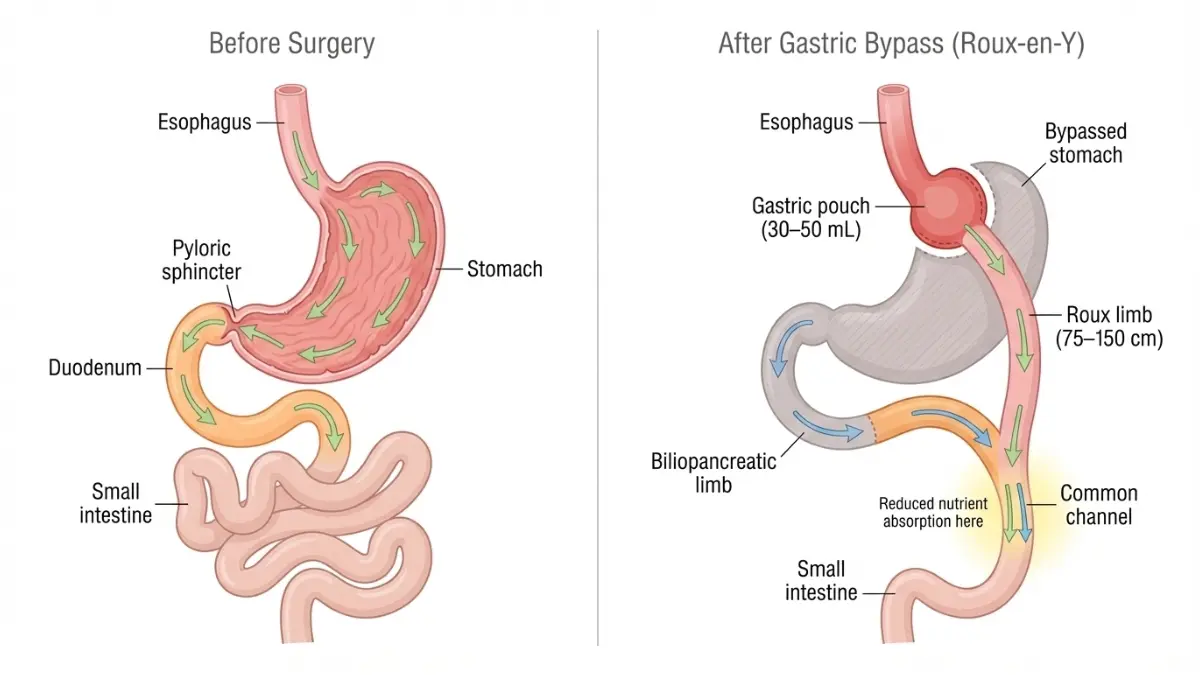
Roux-en-Y Gastric Bypass (RYGB)
The Roux-en-Y gastric bypass creates a small stomach pouch (about the size of an egg) and reroutes a portion of the small intestine to this new pouch, bypassing most of the stomach and the first section of the small intestine. This dual mechanism—restricting food intake and reducing nutrient absorption—produces exceptional metabolic changes beyond simple calorie reduction.
Weight loss outcomes are substantial: patients typically lose 60-80% of their excess body weight within 18-24 months, with research from the National Institutes of Health showing sustained weight loss of 50-60% excess weight at the 10-year mark. Gastric bypass delivers superior diabetes remission rates, with 80-85% of type 2 diabetes patients achieving complete resolution without medication within the first year.
Best candidates for Roux-en-Y gastric bypass include individuals with severe gastroesophageal reflux disease (GERD), BMI above 50, or metabolic syndrome requiring maximum intervention. The procedure requires 2-3 days of hospitalization, with most patients returning to desk jobs within 2-3 weeks.
What This Means For You: If you struggle with uncontrolled diabetes or severe obesity (BMI 45+), gastric bypass offers the highest probability of remission, but requires lifelong commitment to vitamin supplementation and dietary restrictions.
Sleeve Gastrectomy (Gastric Sleeve Surgery)
Sleeve gastrectomy permanently removes approximately 80% of the stomach, leaving a narrow tube or “sleeve” about the size and shape of a banana. Unlike gastric bypass, this procedure doesn’t reroute intestines, making it technically simpler with shorter operative time—averaging 47 minutes compared to 68 minutes for bypass surgery.
Weight loss outcomes reach 50-70% of excess body weight within 12-18 months, with a Portland State University meta-analysis reporting 58.3% excess weight loss maintained at five years. The procedure removes the portion of stomach that produces ghrelin (the hunger hormone), significantly reducing appetite without malabsorption issues.
Safety profile gives sleeve gastrectomy an advantage: comparative studies from NIH researchers found sleeve patients experienced fewer complications (6.6% vs 9.6%), lower mortality rates, and reduced emergency department visits compared to gastric bypass patients at two years post-surgery. Hospital stays average 1-2 days, with most patients resuming normal activities within 10-14 days.
Best for patients with BMI 35-45, those seeking a simpler procedure with faster recovery, or individuals concerned about long-term nutritional deficiencies. However, irreversibility is crucial to understand—there’s no way to restore the removed stomach tissue. Tracking your progress with a Weight Loss Calculator helps set realistic expectations for your specific starting BMI.
What This Means For You: Sleeve gastrectomy offers an excellent balance of effectiveness and safety, particularly for first-time bariatric patients without severe diabetes complications.
Adjustable Gastric Band (Lap-Band)
The adjustable gastric band places an inflatable silicone ring around the upper stomach, creating a small pouch that limits food intake. While minimally invasive and reversible, this procedure has fallen from favor—comprising less than 1% of bariatric surgeries performed in 2024 compared to 35% in 2011.
Weight loss results are modest: patients lose 40-50% of excess weight, with significantly higher failure rates (30-40%) requiring band removal or conversion to another procedure within 10 years. The band can be adjusted by adding or removing saline through a port placed under the skin, allowing customization over time.
Advantages include complete reversibility, no stomach cutting or stapling, and lowest immediate surgical risk. Disadvantages encompass frequent adjustments (every 4-6 weeks initially), band slippage (5-10% of patients), port complications, and lower long-term effectiveness compared to sleeve or bypass options.
Still recommended for patients with BMI 30-35 who want a reversible option, cannot tolerate more invasive surgery due to medical conditions, or strongly prefer avoiding permanent anatomical changes.
Duodenal Switch / BPD-DS
The biliopancreatic diversion with duodenal switch combines a sleeve gastrectomy with extensive intestinal rerouting, bypassing approximately 75% of the small intestine. This complex procedure delivers the highest weight loss potential—70-80% of excess body weight—but carries significantly elevated complication risks.
Reserved exclusively for patients with BMI 50+ or super-obesity (BMI 60+) when other procedures prove insufficient. The duodenal switch produces severe malabsorption, requiring aggressive vitamin supplementation protocols and creating the highest risk of protein malnutrition, with 30-40% of patients developing nutritional complications requiring medical intervention.
Recovery extends 4-6 weeks, with longer hospital stays (3-5 days) and higher costs ($30,000-$45,000 average). Only highly specialized bariatric centers perform this procedure, limiting availability.
Emerging Metabolic Surgery Procedures
SADI-S (Single Anastomosis Duodeno-Ileal Bypass) represents a simplified version of the duodenal switch, requiring only one intestinal connection instead of two. Early research suggests comparable weight loss with potentially lower complication rates, though long-term data remains limited as of 2025.
Endoscopic sleeve gastroplasty offers a non-surgical alternative using an endoscope inserted through the mouth to place sutures that reduce stomach size by approximately 70%. This outpatient procedure costs $8,000-$15,000 but isn’t covered by most insurance plans. Weight loss averages 15-20% of total body weight—significantly less than surgical options—with higher weight regain rates.
Gastric Bypass vs Sleeve Gastrectomy: Side-by-Side Comparison
| Feature | Gastric Bypass (RYGB) | Sleeve Gastrectomy | Gastric Band |
|---|---|---|---|
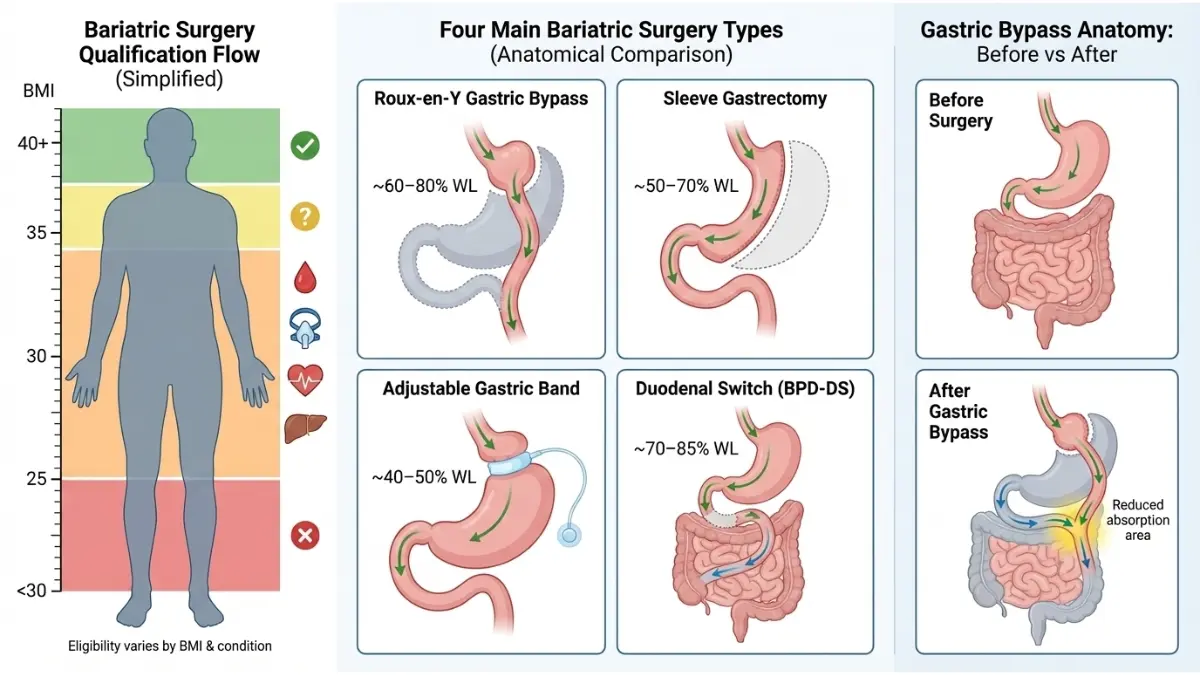
| Excess Weight Loss (1 year) | 60-80% | 50-70% | 40-50% |
| Hospital Stay | 2-3 days | 1-2 days | Outpatient/1 day |
| Average Surgery Time | 60-90 minutes | 45-60 minutes | 30-45 minutes |
| Reversibility | Very difficult | Irreversible | Yes |
| Diabetes Remission Rate | 80-85% | 60-70% | 40-50% |
| Nutrient Malabsorption | High (lifelong supplements required) | Minimal | None |
| 2-Year Complication Rate | 9.6% | 6.6% | 3-5% |
| Revision Surgery Rate (5 years) | 5-8% | 8-12% | 25-35% |
| Average Total Cost | $23,000-$35,000 | $15,000-$25,000 | $10,000-$18,000 |
Understanding your baseline metabolic rate helps predict outcomes—use our BMR Calculator to determine your body’s calorie-burning capacity before and after bariatric surgery planning.
Bariatric Surgery Costs & Insurance Coverage
How Much Does Bariatric Surgery Cost? (2025 Pricing Breakdown)
Sarah from Cincinnati thought bariatric surgery would bankrupt her family—initial quotes ranged from $28,000 to $35,000 for gastric bypass. After verifying her insurance coverage and meeting pre-authorization requirements, her out-of-pocket expense totaled just $3,800. Understanding the true cost of bariatric surgery requires looking beyond sticker prices to insurance coverage policies, Medicare requirements, financing options, and long-term economic benefits that often offset initial expenses within 3-5 years through reduced medication costs and improved health outcomes.
Self-Pay Bariatric Surgery Costs
The average bariatric surgery cost varies dramatically by procedure type, geographic location, and facility accreditation status. Sleeve gastrectomy typically costs $12,000-$25,000 for self-pay patients, making it the most affordable major weight loss surgery option. Gastric bypass surgery costs range from $20,000-$35,000, with prices highest in Northeast and West Coast metropolitan areas. Gastric band procedures, though declining in popularity, cost $8,000-$18,000, while the complex duodenal switch can exceed $40,000 at specialized centers.
Hidden expenses significantly impact total bariatric surgery cost calculations. Pre-operative testing (including cardiac workup, sleep studies, nutritional assessments) adds $1,500-$3,000. Post-surgery vitamin supplementation costs $100-$200 monthly for life, totaling $1,200-$2,400 annually. Follow-up appointments, potential complications, and eventual plastic surgery for excess skin removal (typically $15,000-$30,000 and rarely covered by insurance) must factor into long-term financial planning.
Regional cost variations are substantial: bariatric surgery in Texas or Florida averages 20-30% less than comparable procedures in New York or California. Medical tourism to Mexico or Costa Rica offers sleeve gastrectomy for $4,000-$7,000, though patients sacrifice domestic follow-up care and legal recourse if complications arise. Use our Ideal Weight Calculator to project your target weight and estimate the total journey costs based on your starting point.
Insurance Coverage for Bariatric Surgery
Approximately 95% of private insurance companies maintain defined pre-authorization policies for weight loss surgery, with 92% covering procedures for patients with BMI 40+ or BMI 35+ with qualifying comorbidities. The insurance approval process typically requires:
- Six-month supervised medical weight management program: Documented monthly visits with physician, showing diet and exercise compliance attempts
- BMI documentation: At least two measurements separated by 30+ days showing sustained eligibility
- Psychological evaluation: Screening for eating disorders, depression, and realistic expectations
- Nutritional counseling: Pre-operative education on lifelong dietary changes
- Comorbidity documentation: Medical records proving conditions like type 2 diabetes, sleep apnea, or cardiovascular disease
- Letter of medical necessity: Physician statement explaining why bariatric surgery is medically appropriate
After meeting these requirements, typical out-of-pocket costs with private insurance range $2,500-$7,000, covering deductibles and coinsurance. Insurance coverage rates vary by plan type—research from the University of Pennsylvania found PPO and fee-for-service plans approve bariatric surgery at significantly higher rates than HMO plans, which impose stricter pre-authorization requirements and network limitations.
The pre-authorization timeline averages 4-6 months for private insurance, though expedited approvals occasionally occur within 8-12 weeks for patients with severe comorbidities. Appeal processes succeed in 30-40% of initial denials when patients provide comprehensive medical documentation and specialist letters supporting medical necessity.
Medicare Bariatric Surgery Coverage
Medicare covers bariatric surgery including gastric bypass, sleeve gastrectomy, and laparoscopic gastric band procedures for beneficiaries meeting strict eligibility criteria. Patients must have BMI 35+ with at least one obesity-related comorbidity and receive surgery at a Medicare-approved facility with MBSAQIP (Metabolic and Bariatric Surgery Accreditation and Quality Improvement Program) accreditation.
Medicare beneficiaries typically pay: 20% coinsurance after meeting the Part B annual deductible ($240 in 2025), resulting in out-of-pocket costs of $2,000-$5,000 for the complete surgical episode. Hospital stay costs fall under Medicare Part A, requiring the inpatient deductible ($1,632 in 2025) for stays under 60 days. Dual-eligible beneficiaries (qualifying for both Medicare and Medicaid) often face minimal or zero cost-sharing, significantly improving access to weight loss surgery for lower-income seniors.
Medicare requires more extensive documentation than private insurers, including detailed medical history spanning 2+ years showing failed weight loss attempts, comprehensive comorbidity documentation, and psychological clearance. The approval timeline extends 6-9 months from initial consultation to surgery date.
Financing Options & Long-Term Value
Payment plans and financing make bariatric surgery accessible even without insurance coverage. Many hospital systems offer 12-48 month interest-free payment plans with no credit check required. Medical credit cards like CareCredit provide 6-24 month promotional periods, though interest rates exceed 25% APR after promotional periods expire. Health Savings Accounts (HSA) and Flexible Spending Accounts (FSA) cover bariatric surgery as qualified medical expenses, allowing pre-tax dollar utilization.
Cost-effectiveness analyses consistently demonstrate bariatric surgery’s long-term economic value. A Jefferson University study found gastric bypass cost-effective at both 5-year ($27,799 per quality-adjusted life year) and 10-year ($957 per QALY) time horizons, well below the $50,000 willingness-to-pay threshold used in healthcare economics. Obesity-related healthcare costs average $3,500-$5,500 annually, while type 2 diabetes medications alone cost $500-$800 monthly—expenses largely eliminated post-surgery for most patients.
Tax deductibility applies to bariatric surgery costs exceeding 7.5% of adjusted gross income, potentially recovering 22-37% of expenses through federal tax deductions. Planning your nutritional strategy post-surgery with a Calorie Deficit Calculator helps maximize results and ensure your investment delivers optimal health returns.
Who Qualifies For Bariatric Surgery?
Do You Qualify for Bariatric Surgery? (BMI Requirements & Criteria)
Tom had a BMI of 34.5—technically below standard bariatric surgery qualification thresholds—but his uncontrolled type 2 diabetes, severe sleep apnea, and documented 8-year struggle with obesity led his insurance company to approve gastric sleeve surgery under expanded metabolic surgery criteria. Understanding bariatric surgery qualification involves far more than a simple BMI calculation; it requires comprehensive evaluation of obesity-related health conditions, documented weight loss attempts, psychological readiness, and insurance-specific requirements that vary significantly between carriers.
BMI Requirements for Bariatric Surgery
The National Institute of Diabetes and Digestive and Kidney Diseases established criteria in 1991 that remain the foundation for bariatric surgery qualification: adults with BMI 40+ qualify regardless of comorbidities, while those with BMI 35-39.9 become eligible when accompanied by at least one major obesity-related health condition. Recent guidelines expanded access for patients with BMI 30-34.9 who have uncontrolled type 2 diabetes despite maximum medical therapy, recognizing metabolic surgery’s unique ability to achieve diabetes remission in this population.
Calculate your current BMI using our BMI Calculator to determine baseline eligibility—the tool provides instant classification (normal, overweight, obese class I/II/III) with specific bariatric surgery qualification guidance. Important note: BMI thresholds adjust for certain populations, with research published in BMC Public Health demonstrating Asian individuals face equivalent obesity-related mortality risks at BMI 27.5-32.5, leading many centers to lower qualification thresholds to BMI 27.5+ with comorbidities for East Asian, South Asian, and Pacific Islander patients.
Adolescent bariatric surgery qualification requires BMI ≥120% of the 95th percentile for age and sex (typically BMI 35+ for teens) plus at least one severe comorbidity like type 2 diabetes or severe sleep apnea. Pediatric patients also need demonstrated maturity to understand lifelong lifestyle changes and family commitment to post-surgical support.
Obesity-Related Conditions That Strengthen Qualification
Insurance companies prioritize specific comorbidities when evaluating bariatric surgery qualification, with type 2 diabetes carrying the most weight in approval decisions. Major qualifying conditions include:
- Type 2 diabetes mellitus: Hemoglobin A1C ≥7.0% despite medication compliance, particularly with BMI 30-39.9 range
- Obstructive sleep apnea: Documented by sleep study (AHI ≥15), especially if requiring CPAP therapy
- Cardiovascular disease: Including coronary artery disease, history of myocardial infarction (learn more about silent heart attack warning signs), or congestive heart failure
- Hypertension: Blood pressure ≥140/90 mmHg requiring multiple medications
- Non-alcoholic fatty liver disease (NAFLD): With documented liver enzyme elevation or biopsy-confirmed steatohepatitis
- Severe joint disease: Debilitating osteoarthritis limiting mobility and quality of life
- Gastroesophageal reflux disease (GERD): Requiring daily proton pump inhibitors
- Polycystic ovary syndrome (PCOS): With associated metabolic complications and infertility (explore symptoms at PCOS guide)
A comprehensive NIH review found bariatric surgery achieves 74% diabetes remission rates, 54% hypertension resolution, and 94% sleep apnea improvement within two years post-surgery, making these comorbidities particularly compelling in qualification discussions.
Psychological and Behavioral Requirements
Mental health evaluation represents a non-negotiable component of bariatric surgery qualification. Psychological screening assesses:
- Absence of active eating disorders: Binge eating disorder, bulimia, or anorexia requiring treatment before surgical consideration
- Mental health stability: Controlled depression, anxiety, or other psychiatric conditions (if struggling with anxiety, review natural anxiety reduction strategies)
- Realistic expectations: Understanding that surgery is a tool requiring lifelong dietary and behavioral changes
- Social support system: Family or friend network capable of providing post-operative assistance
- Substance abuse history: No active alcohol or drug abuse; minimum 6-12 months sobriety if prior history
Documented weight loss attempts through supervised medical programs must demonstrate genuine effort, even if unsuccessful. Most insurers require 6 consecutive months of physician-supervised weight management with monthly documentation showing attendance, weight tracking, dietary counseling, and exercise recommendations. This requirement proves particularly frustrating for patients but serves insurance purposes in demonstrating medical necessity.
Smoking cessation is mandatory at virtually all bariatric surgery centers, with nicotine testing performed pre-operatively. Patients must quit smoking at least 6-8 weeks before surgery due to significantly elevated complication risks including wound healing problems, pneumonia, and blood clots.
The Pre-Approval Process Timeline
Month 1-2: Initial bariatric surgery consultation includes comprehensive medical history, physical examination, BMI documentation, and review of weight loss history. Insurance verification determines coverage details, out-of-pocket costs, and specific pre-authorization requirements. Baseline laboratory testing (complete metabolic panel, lipid profile, hemoglobin A1C, vitamin levels) establishes pre-operative health status. Nutritionist appointment begins education on post-surgical dietary progression and supplement requirements—calculate your optimal post-surgery macronutrient needs with our Macro Calculator.
Month 2-6: The mandated supervised weight loss program requires monthly physician visits documenting weight, dietary compliance, physical activity, and behavior modification attempts. Even if no weight loss occurs, consistent attendance and genuine effort documentation satisfies insurance requirements. Concurrent specialists visits address specific health issues—sleep medicine for apnea evaluation, cardiology for cardiac clearance if indicated, endocrinology for diabetes optimization.
Month 4-6: Psychological evaluation with licensed mental health professional trained in bariatric assessment typically occurs mid-process. The comprehensive interview assesses eating behaviors, psychiatric history, support systems, and readiness for life-altering surgery. Clearance requires demonstrated understanding of post-surgical requirements and realistic expectations.
Month 6-7: Final surgical consultation reviews all accumulated documentation, confirms continued BMI eligibility, and submits comprehensive insurance pre-authorization packet including physician letters of medical necessity, complete medical records, supervised weight loss documentation, psychological clearance, and specialist evaluations. Insurance review takes 2-4 weeks, with appeal processes adding 3-6 weeks if initial denial occurs.
Month 7-8: Upon insurance approval, pre-operative testing including upper GI imaging, chest X-ray, EKG, and final laboratory work occurs within 30 days of surgery. Scheduling accommodates patient availability and surgeon schedule. Many programs require 1-2 week pre-operative liquid diet to reduce liver size and improve surgical safety.
Self-pay advantages: Patients bypassing insurance can complete the process in 4-8 weeks, attending informational seminars, completing required evaluations, and scheduling surgery rapidly without mandated waiting periods.
Quick Qualification Assessment
| Your Situation | Qualification Status | Next Step |
|---|---|---|
| BMI 40+, no other health issues | ✅ Strong candidate | Schedule consultation at accredited center |
| BMI 35-39.9 + diabetes, hypertension, or sleep apnea | ✅ Strong candidate | Verify insurance coverage, start documentation |
| BMI 30-34.9 + uncontrolled diabetes (A1C >7%) | ✅ Possible candidate (metabolic surgery criteria) | Consult bariatric specialist about metabolic surgery |
| BMI 30-34.9, well-controlled diabetes | ⚠️ Unlikely to qualify | Focus on medical weight management first |
| BMI <30, any conditions | ❌ Not eligible | Consider non-surgical interventions |
Bariatric Surgery Recovery, Risks & Life After Surgery
Bariatric Surgery Recovery Timeline & Long-Term Life Changes
Maria returned to her teaching job just 12 days after sleeve gastrectomy, but her genuine transformation unfolded over the next 18 months as she learned to navigate tiny meal portions, aggressive vitamin supplementation, and unexpected emotional challenges accompanying 92-pound weight loss. Bariatric surgery recovery extends far beyond the initial 4-6 weeks of physical healing; it represents a permanent lifestyle restructuring requiring daily protein prioritization, lifelong nutritional supplementation, consistent exercise habits, and psychological adaptation to dramatic body changes and social relationship shifts.
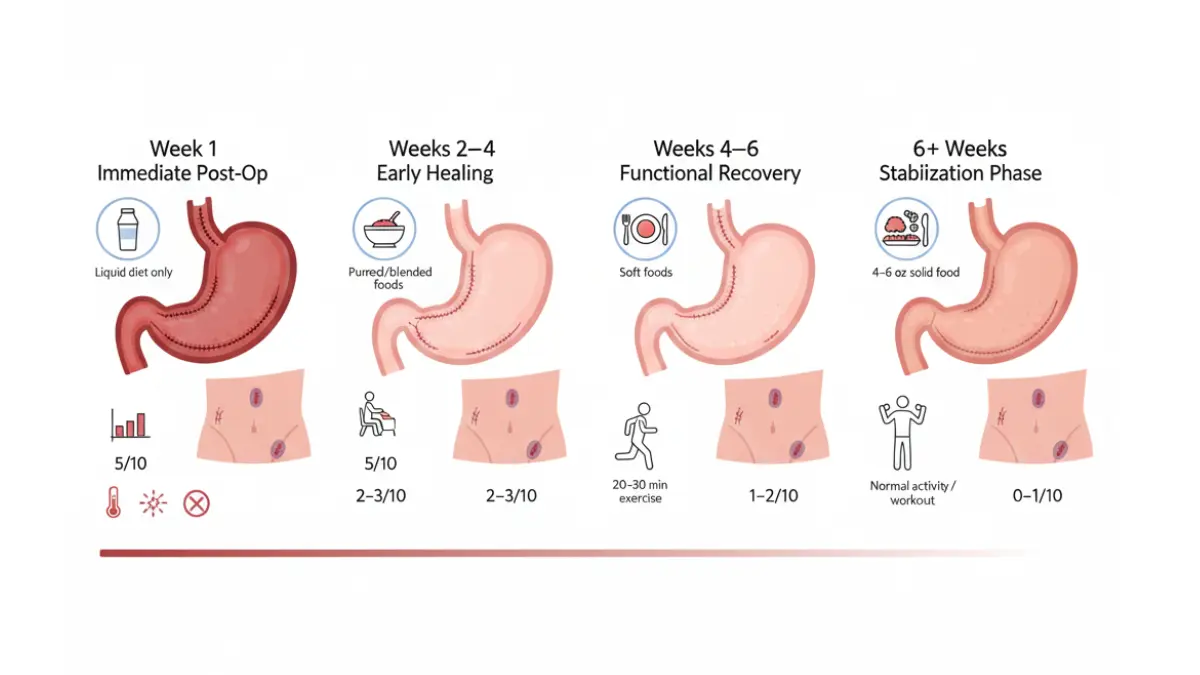
Immediate Recovery Timeline (First 6 Weeks)
Week 1 post-surgery involves hospital monitoring for 1-3 days depending on procedure complexity (gastric bypass requires longer observation than sleeve gastrectomy). Pain levels typically register 3-5 out of 10 with medication, managed through prescribed opioids transitioned to over-the-counter options by day 4-5. The liquid-only diet phase includes protein shakes (minimum 60-80g daily protein), clear broths, sugar-free beverages, and sugar-free gelatin totaling 400-600 calories. Walking begins immediately—patients must walk 5-10 minutes every 2 hours while awake to prevent dangerous blood clots including pulmonary embolism, which represents the most serious early mortality risk.
Weeks 2-4 introduce pureed foods including blended proteins (Greek yogurt, cottage cheese, scrambled eggs), mashed vegetables, and smooth nut butters. Portion sizes remain 2-4 tablespoons per meal, consumed over 20-30 minutes with thorough chewing critical to prevent “foaming” (excessive saliva production) or vomiting. Most patients return to sedentary work within 2-3 weeks, while physically demanding jobs require 4-6 week recovery. Calculate your optimal protein distribution using our Protein Intake Calculator to ensure adequate nutrition during restricted calorie phases.
Weeks 4-6 transition to soft solid foods including ground meats, tender cooked vegetables, soft fruits, and well-cooked whole grains. Meal portions expand to 4-6 ounces consumed over 30 minutes. Exercise progression reaches 20-30 minutes daily of low-impact activities (walking, stationary cycling, swimming). Adequate hydration becomes easier as swelling subsides—aim for 64+ ounces daily between meals using a Water Intake Calculator for personalized targets. NCBI medical literature documents that most acute complications (anastomotic leaks, strictures, bleeding) manifest within this 6-week window, requiring immediate medical attention if severe abdominal pain, fever, or inability to tolerate liquids develops.
Long-Term Weight Loss Expectations & Plateaus
Months 1-6 represent rapid weight loss phase with gastric bypass patients losing 60-70% of excess body weight and sleeve gastrectomy patients achieving 50-60% loss. Common experiences include hair thinning (temporary, resolves by month 9-12), fatigue despite improved cardiovascular fitness, cold intolerance, and emotional volatility as hormones and neurotransmitters adjust. Weight loss averages 10-20 pounds monthly during this phase, though individual variation is substantial based on starting BMI, age, gender, and exercise compliance.
Months 6-18 bring continued steady loss with velocity slowing to 4-8 pounds monthly. Weight loss plateaus lasting 3-6 weeks are physiologically normal as metabolism adjusts and body composition changes. Most patients reach 75-80% of total expected excess weight loss by month 12-14. Skin laxity becomes apparent, particularly in abdomen, arms, thighs, and breast tissue, prompting some patients to pursue plastic surgery (typically delayed until 18-24 months post-bariatric surgery to ensure weight stabilization).
Year 2+ transitions to maintenance phase where 10-15% weight regain is statistically normal and doesn’t indicate failure. Research from the University of Miami tracked patients for 14+ years, finding sustained 31.3% total body weight loss with maintained remission of diabetes, hypertension, and sleep apnea in over 90% of compliant patients. Weight maintenance requires vigilance—patients who regain significant weight often cite return to high-calorie beverages (soda, juice, alcohol), grazing behavior replacing structured meals, and decreased exercise consistency.
Bariatric Surgery Risks & Complications
Short-term surgical complications occur in 5-15% of bariatric surgery cases depending on procedure type and surgeon experience. Comprehensive NIH analysis identifies the most significant early risks as anastomotic leaks (1-5% of cases, most serious complication requiring immediate reoperation), bleeding requiring transfusion (1-3%), pulmonary embolism (<1% with preventive blood thinners), and surgical site infection (2-4%). Mortality risk remains extremely low at 0.1-0.5%—lower than gallbladder removal or hip replacement surgery.
Long-term nutritional deficiencies affect 30-50% of bariatric surgery patients who don’t maintain lifelong supplementation protocols. Iron deficiency develops in 20-35% (particularly menstruating women), vitamin B12 deficiency in 15-30% (causing neurologic symptoms if untreated), calcium and vitamin D deficiency in 25-50% (increasing osteoporosis risk), and thiamine deficiency in severe cases causing Wernicke encephalopathy. Quarterly laboratory monitoring for the first 2 years, then annual testing, enables early detection and correction.
Dumping syndrome affects 20-30% of gastric bypass patients when consuming high-sugar foods that rapidly empty into the small intestine, causing severe nausea, cramping, diarrhea, rapid heartbeat, and sweating within 30 minutes of eating. While distressing, many patients view dumping syndrome as a helpful deterrent against poor food choices. Late dumping (reactive hypoglycemia occurring 2-3 hours post-meal) develops in 5-10% of Roux-en-Y patients, sometimes requiring medication management.
Additional long-term risks include gallstones (10-20% develop within first year due to rapid weight loss, often treated preventively with ursodiol), internal hernias (3-5% of gastric bypass patients), marginal ulcers (1-16% near surgical connections), and incisional hernias (10-20%). Alcohol sensitivity increases dramatically post-surgery—blood alcohol levels spike higher and faster, creating addiction vulnerability even in patients with no prior alcohol issues.
Life After Bariatric Surgery: Permanent Changes
Dietary restrictions become permanent lifestyle. Meal capacity remains 4-8 ounces per sitting forever. Protein must comprise 60-80 grams daily (prioritized at each meal before carbohydrates). High-fiber foods require careful chewing to prevent blockages. Carbonated beverages may cause discomfort and stomach stretching. Alcohol requires extreme caution due to altered metabolism and addiction risk. Vitamin supplementation costs $50-$100 monthly and continues for life without exception.
Exercise requirements mandate 150+ minutes weekly of moderate activity to maintain weight loss and prevent muscle loss. Strength training becomes crucial after age 40 to combat sarcopenia (age-related muscle loss accelerated by rapid weight reduction). Many successful long-term patients exercise 300+ minutes weekly, recognizing that metabolic advantage from surgery diminishes over time.
Follow-up care demands include quarterly bariatric surgeon visits year 1, semi-annual visits year 2, then annual lifelong monitoring. Annual comprehensive laboratory panels screen for nutritional deficiencies. Support groups provide accountability and community—70% of successful long-term patients attend regularly. Mental health counseling addresses body image concerns, relationship changes (divorce rates increase 10-40% post-bariatric surgery), and adjustment challenges.
Pregnancy planning requires 12-18 month delay post-surgery to ensure nutritional stability and weight stabilization. Gestational monitoring intensifies for bariatric patients, though outcomes generally remain excellent with appropriate prenatal vitamin optimization and earlier introduction of iron supplementation to prevent anemia.
Choosing The Best Bariatric Surgery & Finding Qualified Surgeons
How to Choose the Best Bariatric Surgery Option & Find Qualified Surgeons
Jennifer’s surgeon recommended gastric bypass based on her BMI of 48 and severe diabetes, but after thorough consultation discussing her active lifestyle, fear of malabsorption complications, and willingness to accept slightly lower diabetes remission rates, they collaboratively chose sleeve gastrectomy—a decision she calls “the best choice I ever made” three years later. Selecting between gastric bypass vs sleeve gastrectomy (or other bariatric surgery options) requires honest evaluation of your health priorities, lifestyle preferences, complication tolerance, and long-term commitment level, guided by experienced surgeons who practice shared decision-making rather than one-size-fits-all recommendations.
Deciding Between Gastric Bypass vs Sleeve
Choose Roux-en-Y gastric bypass if your primary goals include maximum diabetes remission (80-85% success rate), you have severe GERD requiring daily medication, your BMI exceeds 50 requiring aggressive intervention, or you’re willing to accept higher malabsorption risks and stricter lifelong vitamin protocols in exchange for superior metabolic benefits. Gastric bypass delivers 10-15% greater excess weight loss than sleeve but demands more intensive nutritional monitoring and carries elevated dumping syndrome risk.
Choose sleeve gastrectomy if you have BMI 35-45 range, prefer simpler surgery with faster recovery (1-2 day hospitalization vs 2-3 days), want to minimize malabsorption and nutritional complications, or prioritize safety over maximum weight loss potential. Sleeve’s 6.6% complication rate versus bypass’s 9.6% rate makes it ideal for first-time bariatric patients without severe metabolic disease requiring urgent intervention.
Choose gastric banding only if you have BMI 30-35 with limited comorbidities, strongly prefer reversible procedures, cannot tolerate permanent anatomical changes due to religious or personal beliefs, or have medical contraindications to more invasive surgery. Accept that 30-40% of bands require removal within 10 years and weight loss averages 40-50% excess weight versus 60-80% with bypass.
Finding the Best Bariatric Surgeon Near You
Essential surgeon qualifications include board certification in general surgery, completion of ASMBS-recognized bariatric fellowship training, performance of 100+ bariatric procedures annually (50+ for newer procedures), and hospital privileges at MBSAQIP-accredited facilities. Research from the University of Michigan demonstrates that surgeon volume directly correlates with outcomes—high-volume surgeons achieve complication rates 40% lower than low-volume practitioners.
MBSAQIP accreditation represents the gold standard for bariatric surgery centers, requiring comprehensive quality improvement programs, outcomes tracking, multidisciplinary teams (surgeon, dietitian, psychologist, exercise physiologist), and strict credentialing standards. Verify accreditation status before scheduling consultations.
Red flags during consultations include surgeons pushing specific procedures without discussing alternatives, facilities lacking dedicated bariatric programs, absence of comprehensive aftercare including support groups and nutritionist access, poor online reviews consistently mentioning post-operative abandonment, and pressure to proceed rapidly without addressing questions or concerns.
Critical Consultation Questions
Ask potential surgeons: “What is YOUR personal complication rate for this specific procedure over the past 2 years?” Expect documented rates below 5% for sleeve, below 8% for bypass. “What percentage of your patients achieve remission of diabetes/hypertension?” Compare answers against published benchmarks (80%+ diabetes remission for bypass, 60-70% for sleeve). “What does your 5-year follow-up program include?” Lifelong access to support groups, quarterly visits year one, and annual monitoring should be standard.
Revision surgery experience matters—ask how many revisional procedures the surgeon performs annually and their specific revision complication rates, which typically run 15-25% higher than primary surgeries.
Take Action: Your Next Steps
Ready to explore bariatric surgery? Follow this evidence-based roadmap:
- Verify baseline eligibility by calculating your BMI and reviewing qualifying comorbidities—most candidates have BMI 35+ with conditions like diabetes, sleep apnea, or hypertension
- Contact insurance immediately to obtain specific pre-authorization requirements, CPT codes for coverage verification (43644 for gastric bypass, 43775 for sleeve gastrectomy), and list of in-network MBSAQIP-accredited facilities
- Schedule 2-3 surgeon consultations at different accredited centers to compare approaches, philosophies, and aftercare programs before committing
- Begin documenting weight loss attempts and medical records today—insurance companies require 6-month supervised programs, so early documentation prevents delays
- Attend support group meetings (many centers allow non-patients) to hear unfiltered patient experiences about recovery, complications, and life after bariatric surgery
- Optimize current health by addressing untreated conditions, quitting smoking, and starting exercise habits that will serve you post-operatively
Bariatric surgery represents one of medicine’s most effective interventions for severe obesity and metabolic disease, but success requires informed decision-making, qualified surgical teams, and lifelong commitment to dietary and lifestyle changes.
Frequently Asked Questions About Bariatric Surgery
1. How much weight can you lose with bariatric surgery?
Most patients lose 50-80% of their excess body weight within 18-24 months. Gastric bypass typically produces 60-80% excess weight loss, while sleeve gastrectomy achieves 50-70%, depending on starting BMI and post-operative lifestyle adherence.
2. Is bariatric surgery covered by insurance?
Approximately 95% of private insurance plans cover bariatric surgery for patients with BMI 40+ or BMI 35+ with qualifying conditions like diabetes or sleep apnea. Medicare also covers bariatric procedures at MBSAQIP-accredited facilities, though pre-authorization requires 6-month supervised weight loss documentation.
3. What is the safest bariatric surgery?
Sleeve gastrectomy has the lowest complication rate at 6.6% compared to gastric bypass at 9.6%. Mortality risk for all modern bariatric procedures remains extremely low at 0.1-0.5%—safer than gallbladder removal or hip replacement surgery.
4. Can you get bariatric surgery with a BMI of 30?
Yes, if you have uncontrolled type 2 diabetes despite maximum medical therapy. Updated guidelines from 2022 expanded eligibility to BMI 30-34.9 patients with severe metabolic disease, though insurance coverage varies significantly.
5. How long does bariatric surgery take?
Sleeve gastrectomy averages 45-60 minutes, gastric bypass takes 60-90 minutes, and gastric band requires 30-45 minutes. Hospital stays range from outpatient (gastric band) to 1-2 days (sleeve) or 2-3 days (bypass).
6. What can you eat after bariatric surgery?
The first 2 weeks require liquids only (protein shakes, broth), weeks 2-4 introduce pureed foods, weeks 4-6 allow soft solids, and after 6 weeks most solid foods are tolerated in 4-6 ounce portions. Lifelong protein prioritization (60-80g daily) and vitamin supplementation remain mandatory.
7. Does bariatric surgery cure diabetes?
Gastric bypass achieves type 2 diabetes remission in 80-85% of patients, while sleeve gastrectomy produces 60-70% remission rates. Most patients discontinue diabetes medications within 3-6 months post-surgery, though long-term maintenance requires continued healthy lifestyle habits.
8. What are the long-term side effects of bariatric surgery?
Common long-term effects include nutritional deficiencies (requiring lifelong supplements), dumping syndrome in 20-30% of bypass patients, gallstones in 10-20%, and 10-15% weight regain after year 2. Permanent meal size restriction to 4-8 ounces and alcohol sensitivity also persist.
9. How painful is bariatric surgery recovery?
Most patients rate post-operative pain as 3-5 out of 10 with medication, managed through prescribed pain relievers for 3-5 days then over-the-counter options. Laparoscopic techniques cause less pain than older open surgeries, with most people returning to desk jobs within 2-3 weeks.
10. Can you gain weight back after bariatric surgery?
Yes, 10-15% weight regain is statistically normal and expected after year 2. Significant regain (20+ pounds) occurs in 20-30% of patients who return to high-calorie beverages, grazing behaviors, or decreased exercise consistency, emphasizing that surgery is a tool requiring lifelong behavioral changes.
11. What is the best age for bariatric surgery?
The ideal age range is 25-55 years when patients experience maximum benefit with lowest complication risks. Adolescents as young as 13 can qualify with BMI ≥120% of 95th percentile and severe comorbidities, while patients over 65 require more thorough cardiac and medical clearance but can still achieve excellent outcomes.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.