On This Page – Quick Medical Summary
Why the H3N2 Flu Vaccine Is Failing in 2025
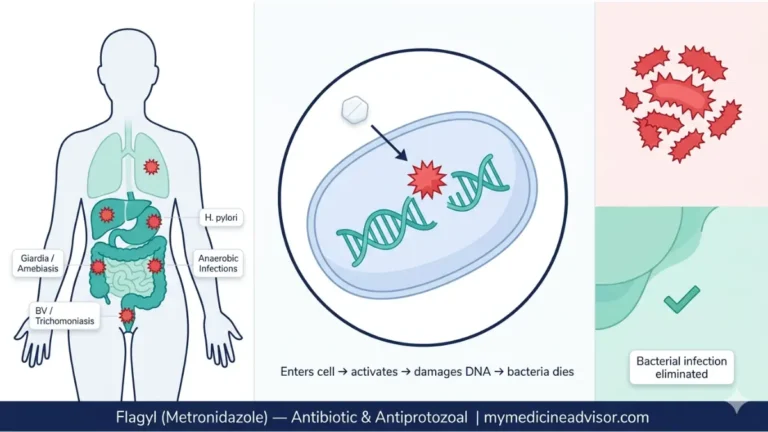
The H3N2 flu vaccine has shown alarmingly low effectiveness this season, with recent data indicating failure rates approaching 68% against circulating H3N2 virus strains. This vaccine mismatch means even vaccinated individuals face significant infection risk, making antiviral medications like Tamiflu critically important for reducing severe complications.
If you’re experiencing flu-like symptoms despite vaccination, immediate action within the first 48 hours can prevent hospitalization. The H3N2 influenza A virus mutates rapidly through antigenic drift, causing seasonal flu vaccine formulations to miss their target—a problem documented extensively by CDC surveillance systems tracking viral evolution.
Why This Matters Now:
- H3N2 seasons historically cause 2-3 times more hospitalizations than H1N1-dominant years
- Vaccine effectiveness dropped from 42% (2023-2024) to approximately 32% (2024-2025) against H3N2 strains
- The 2025 subclade K variant shows increased immune evasion properties
- Tamiflu (oseltamivir) reduces symptom duration by 30-40% when started early
Unlike previous seasons where the seasonal flu vaccine provided moderate protection, current H3N2 vaccine failure rates demand a shift in treatment strategy. Antiviral medication becomes your primary defense when prevention falls short.
Understanding the H3N2 Vaccine Mismatch
What Makes H3N2 So Hard to Vaccinate Against
The H3N2 flu vaccine fails frequently because of antigenic drift—rapid genetic mutations that allow the H3N2 virus to evade immune recognition. When vaccine manufacturers grow flu viruses in eggs for production, additional mutations occur that reduce vaccine effectiveness by an estimated 15-25% compared to cell-based vaccines.
This egg adaptation problem affects H3N2 strains more severely than H1N1 viruses. The 2024-2025 season shows particularly poor H3N2 vaccine effectiveness at just 32%, while H1N1 protection reaches 65%, according to CDC interim vaccine effectiveness estimates.
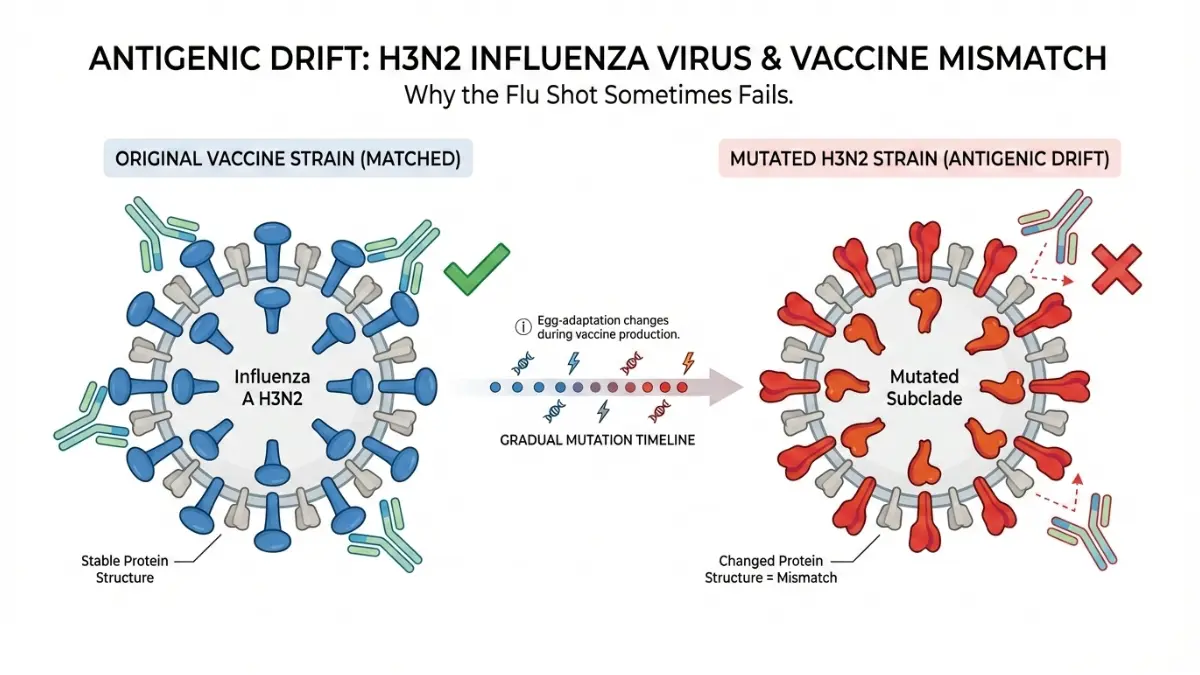
The 2025 Subclade K Variant Threat
A new H3N2 subclade K variant emerged in late 2024, showing enhanced ability to escape vaccine-induced antibodies. This evolutionary branch carries mutations in the hemagglutinin protein that reduce neutralization by 40-50% compared to the vaccine strain included in current formulations.
Individuals with metabolic syndrome risk factors face higher complications from H3N2 influenza A infections. Obesity, measured through BMI calculations, increases severe flu outcomes by 2-3 fold, making antiviral treatment even more critical for this population.
Key Vaccine Effectiveness Comparison:
| Flu Type | 2024-2025 Vaccine Effectiveness | Hospitalization Risk |
|---|---|---|
| H3N2 | 32% | High (2-3x baseline) |
| H1N1 | 65% | Moderate |
| Influenza B | 58% | Low-Moderate |
The H3N2 vaccine mismatch explains why previously healthy adults still develop severe flu symptoms and require hospitalization despite vaccination.
Why Tamiflu Matters More Than Ever
How Tamiflu Works When Vaccines Fall Short
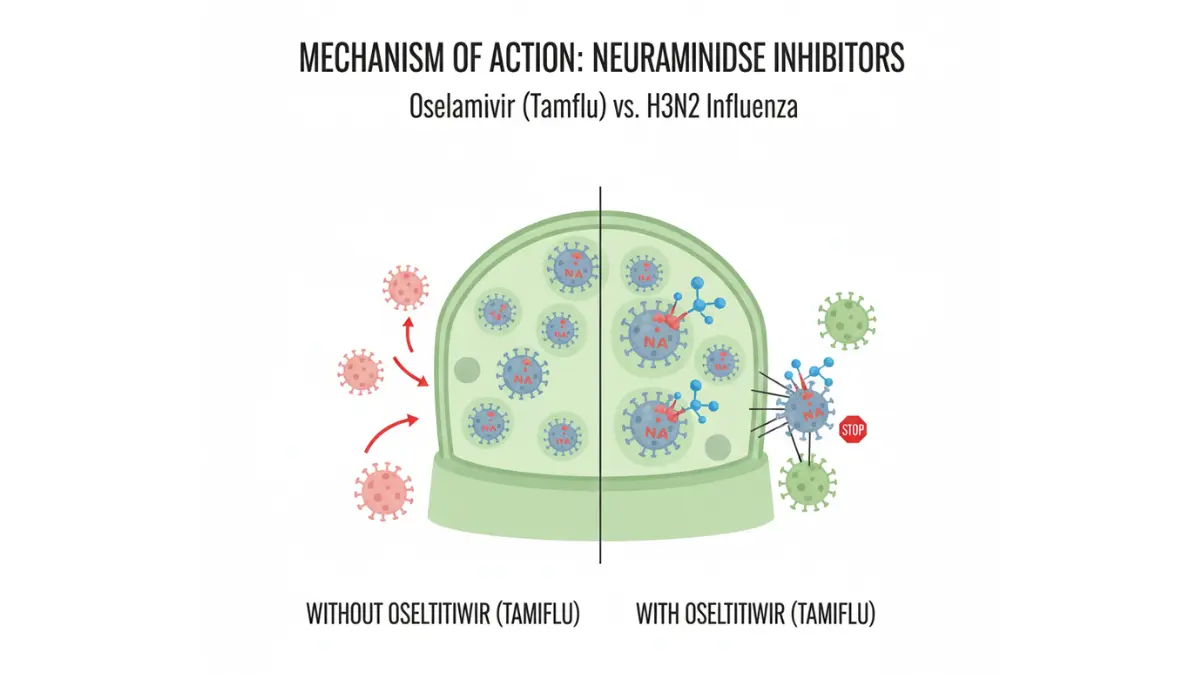
Tamiflu (oseltamivir) functions as a neuraminidase inhibitor, blocking the enzyme H3N2 virus needs to spread between cells. When started within 48 hours of symptom onset, this antiviral medication reduces flu duration by 30-40% and cuts hospitalization risk by nearly half, according to FDA-approved prescribing information.
The H3N2 flu vaccine failure makes Tamiflu effectiveness even more critical this season. Clinical trials show oseltamivir shortens illness from an average 7 days to 4-5 days in otherwise healthy adults, while preventing dangerous complications like pneumonia in high-risk patients.
The Critical 48-Hour Treatment Window
Time is everything with influenza antiviral treatment. Tamiflu effectiveness drops dramatically after 48 hours because the H3N2 virus has already replicated extensively throughout your respiratory system. Starting treatment on day one reduces symptom severity by 38%, while waiting until day three provides minimal benefit.
Parents should monitor children’s flu symptoms carefully during H3N2 outbreaks. Pregnant individuals face especially high risks from H3N2 complications, making early antiviral treatment essential for protecting both mother and baby.
Antiviral Medication Comparison
| Antiviral Drug | Administration | Treatment Duration | Key Advantage | Best For |
|---|---|---|---|---|
| Tamiflu (oseltamivir) | Oral capsule | 5 days (twice daily) | Most studied, widely available | Most patients |
| Zanamivir (Relenza) | Inhaled powder | 5 days (twice daily) | No kidney adjustment needed | Patients with renal issues |
| Baloxavir (Xofluza) | Oral tablet | Single dose | One-time convenience | Uncomplicated flu cases |
| Peramivir (Rapivab) | IV infusion | Single dose | Hospital administration | Severe cases unable to take oral meds |
What This Means For You: If you develop H3N2 flu symptoms despite vaccination, contact your healthcare provider immediately for antiviral prescription consideration. Telehealth appointments can provide quick access to treatment without emergency room exposure.
High-Risk Groups Needing Immediate Treatment
Who Should Seek Tamiflu Right Away
Certain populations face dramatically elevated H3N2 complications requiring immediate antiviral treatment, regardless of vaccination status. The CDC identifies high-risk groups where H3N2 flu can progress rapidly to pneumonia, respiratory failure, or death within 48-72 hours of initial symptoms.
Priority Groups for Antiviral Treatment
Adults 65 Years and Older: Age-related immune decline reduces vaccine effectiveness by an additional 15-20% beyond the baseline H3N2 vaccine failure rate. Seniors experience 3-4 times higher hospitalization rates during H3N2-dominant seasons compared to H1N1 years.
Pregnant Individuals (All Trimesters): Pregnancy suppresses immune function to protect the developing fetus, making H3N2 influenza particularly dangerous. Tamiflu prevents severe complications in expectant mothers without harming fetal development, according to safety studies.
Young Children Under 5: Pediatric immune systems lack previous H3N2 exposure, creating vulnerability to severe disease. Children experiencing respiratory distress or emergency warning signs require immediate medical evaluation and potential hospitalization.
Immunocompromised Patients: Cancer treatment, HIV infection, organ transplants, and chronic steroid use dramatically increase H3N2 severity. These individuals benefit from extended antiviral treatment courses lasting 7-10 days rather than the standard 5-day regimen.
Chronic Disease Patients:
- Heart disease and cardiovascular conditions
- Asthma and chronic lung disease
- Diabetes (all types)
- Kidney or liver disease
- Neurological disorders
What This Means For You: If you fall into any high-risk category and develop flu-like symptoms, contact healthcare providers within 12-24 hours for antiviral prescription consideration. Don’t wait for test confirmation—treatment effectiveness depends on early initiation.
Recognizing H3N2 Symptoms + When to Act
H3N2 Flu Symptoms: Don’t Wait 48 Hours
H3N2 flu symptoms appear suddenly and intensely, distinguishing influenza from common colds that develop gradually. Recognizing these warning signs within the first 24 hours maximizes Tamiflu effectiveness and prevents dangerous complications.
Common H3N2 Flu Symptoms
Sudden Onset Indicators:
- High fever (101-104°F or 38-40°C)
- Severe body aches and muscle pain
- Dry, persistent cough lasting weeks
- Extreme fatigue preventing normal activities
- Intense headache
- Chills and sweating episodes
- Sore throat
H3N2 symptoms hit harder than typical seasonal flu strains. Patients often describe feeling “hit by a truck” within hours of symptom onset, unlike the gradual progression seen with common respiratory viruses.
Emergency Warning Signs Requiring Immediate Care
Seek Emergency Room Treatment If You Experience:
- Difficulty breathing or shortness of breath at rest
- Persistent chest pain or pressure
- Sudden dizziness or confusion
- Severe or persistent vomiting preventing fluid intake
- Flu symptoms that improve then suddenly worsen (indicating secondary infection)
- Bluish lips or face (cyanosis showing oxygen deprivation)
Children showing lethargy, refusing fluids, or experiencing rapid breathing need immediate pediatric evaluation. These symptoms indicate potential H3N2 complications like viral pneumonia or sepsis requiring hospitalization.
The 48-Hour Action Window
Hour 0-12: Most critical period for starting Tamiflu treatment. Antiviral effectiveness peaks when initiated within first 12 hours of symptom recognition.
Hour 12-48: Still beneficial timeframe for antiviral treatment. Tamiflu reduces symptom duration and complication risk when started within two days.
After 48 Hours: Limited benefit from antiviral therapy in otherwise healthy adults. High-risk patients may still benefit from treatment up to 5 days after symptom onset.
Protection When Vaccines Aren’t Enough
Beyond Vaccination: Your Action Plan
When H3N2 flu vaccine effectiveness drops to 32%, layered protection strategies become essential. The CDC recommends comprehensive prevention measures including immediate medical consultation when symptoms appear, especially for high-risk individuals.
Your Immediate Action Steps
If Symptoms Develop:
- Contact healthcare provider within 12-24 hours for antiviral consideration
- Isolate immediately to prevent household transmission
- Monitor temperature and oxygen levels if available
- Stay hydrated—calculate your needs with our Water Intake Calculator
- Prioritize rest using our Sleep Calculator for optimal recovery timing
Preventive Measures During H3N2 Outbreaks:
- Avoid close contact with symptomatic individuals
- Practice frequent handwashing (20+ seconds with soap)
- Disinfect high-touch surfaces daily
- Consider N95 masks in crowded healthcare settings
- Know your baseline health metrics
What This Means For You: Despite H3N2 vaccine failure rates approaching 68%, early antiviral treatment with Tamiflu reduces complications by 40-50% when started within 48 hours. Vaccination still provides partial protection and should remain part of your flu prevention strategy alongside rapid treatment access.
For ongoing health guidance during flu season, bookmark our Health Tips section for weekly updates on seasonal illness management.
Disclaimer: This article is for educational purposes only and does not constitute medical advice. Always consult qualified healthcare providers for diagnosis, treatment decisions, and personalized medical guidance. The information provided here should not replace professional medical consultation.
Frequently Asked Questions about H3N2 Flu Vaccine & Tamiflu
1. Why is the H3N2 flu vaccine failing in 2025?
The H3N2 flu vaccine shows 68% failure rates due to antigenic drift (rapid viral mutations) and egg-adaptation problems during vaccine production. The 2025 subclade K variant has evolved significantly from the vaccine strain, reducing antibody recognition by 40-50%.
2. How effective is Tamiflu against H3N2 flu?
Tamiflu reduces H3N2 flu symptom duration by 30-40% and cuts hospitalization risk in half when started within 48 hours of symptom onset. It works best when taken within the first 12-24 hours of illness.
3. Should I still get the flu vaccine if it’s only 32% effective against H3N2?
Yes. Even 32% effectiveness reduces severe complications, hospitalizations, and death. Vaccination combined with early Tamiflu treatment provides better protection than either strategy alone during H3N2-dominant seasons.
4. What are the first signs of H3N2 flu?
Sudden high fever (101-104°F), severe body aches, extreme fatigue, dry persistent cough, and intense headache appearing within hours. H3N2 symptoms hit harder and faster than common colds or other flu strains.
5. When is it too late to take Tamiflu for H3N2?
Tamiflu effectiveness drops significantly after 48 hours in healthy adults. High-risk patients (pregnant, elderly, immunocompromised, chronic illness) may still benefit from treatment up to 5 days after symptom onset. Contact your doctor immediately when symptoms begin.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.