On This Page – Quick Medical Summary
Sleep medications are drugs or supplements that help people fall asleep faster, stay asleep longer, or both — by altering brain chemicals that regulate the sleep-wake cycle. They range from prescription sedatives to over-the-counter antihistamines and natural supplements like melatonin. While effective for short-term use, most carry significant risks of dependence, next-day impairment, and reduced sleep quality — making safer alternatives worth serious consideration.
Why Millions of Americans Can’t Sleep (And Why They Reach for a Pill)
It’s 3 AM. Michael, a 42-year-old teacher from Ohio, has been staring at the ceiling for two hours. His mind won’t stop. He has a meeting in the morning. He reaches for the bottle of zolpidem on his nightstand — and swallows one. Again.
He’s not alone.
The scale of the problem:
- Between 30% and 40% of U.S. adults report insomnia symptoms at some point each year, according to research published in PMC
- Chronic insomnia — lasting 3+ months — affects roughly 10% of the adult population
- The economic cost of insomnia exceeds $100 billion annually in the U.S. alone, driven by lost productivity and increased healthcare use (The Lancet, 2022)
The appeal of sleep medications is obvious: take a pill, fall asleep, wake up rested. But most people who reach for a sleeping pill don’t fully understand what class of drug they’re taking, how it works on the brain, or what happens after weeks of use.
Understanding what you’re actually taking — and what your options are — could change everything. Use our Sleep Calculator to first identify exactly how much sleep your body actually needs by age and lifestyle before assuming you need medication.
If you’ve been waking up repeatedly at odd hours, our deep-dive on why you keep waking up at 3 AM every night can help you understand whether your issue is behavioral, hormonal, or medication-related.
Complete Guide to Sleep Medication Types — OTC, Prescription, and Natural
Not all sleep medications work the same way. Choosing the wrong type — or using the right type for too long — is where most people run into serious trouble.
Over-the-Counter (OTC) Sleep Aids
The most accessible sleep medications available without a prescription in the U.S. are antihistamine-based:
- Diphenhydramine (found in ZzzQuil, Unisom SleepTabs, Benadryl)
- Doxylamine succinate (found in Unisom SleepMelts, NyQuil)
Both reduce wakefulness by blocking histamine — the brain chemical that promotes alertness. They work fast, but tolerance builds within 3–5 days of consecutive use.
Critical warning: A large-scale study published in JAMA Internal Medicine found that long-term use of anticholinergic drugs like diphenhydramine is linked to a 54% higher risk of developing dementia, as these drugs block acetylcholine, a key memory and cognition chemical. The Johns Hopkins Medicine sleep aid guide explicitly flags this risk.
Prescription Sleep Medications — 5 Major Classes
| Class | Common Examples | How It Works | Dependence Risk | Best Suited For |
|---|---|---|---|---|
| Benzodiazepines | Temazepam, Triazolam | Enhances GABA (calms brain) | High | Short-term acute insomnia |
| Z-Drugs | Zolpidem (Ambien), Eszopiclone (Lunesta), Zaleplon (Sonata) | Targets GABA-A receptors | Medium | Sleep onset + maintenance |
| Orexin Antagonists (DORAs) | Suvorexant (Belsomra), Lemborexant (Dayvigo), Daridorexant (Quviviq) | Blocks wakefulness signals | Lower | Sleep maintenance insomnia |
| Melatonin Receptor Agonists | Ramelteon (Rozerem) | Mimics natural melatonin | Very Low | Circadian rhythm disorders |
| Sedating Antidepressants | Trazodone, Doxepin (Silenor) | Serotonin/histamine modulation | Variable | Insomnia with comorbid depression |
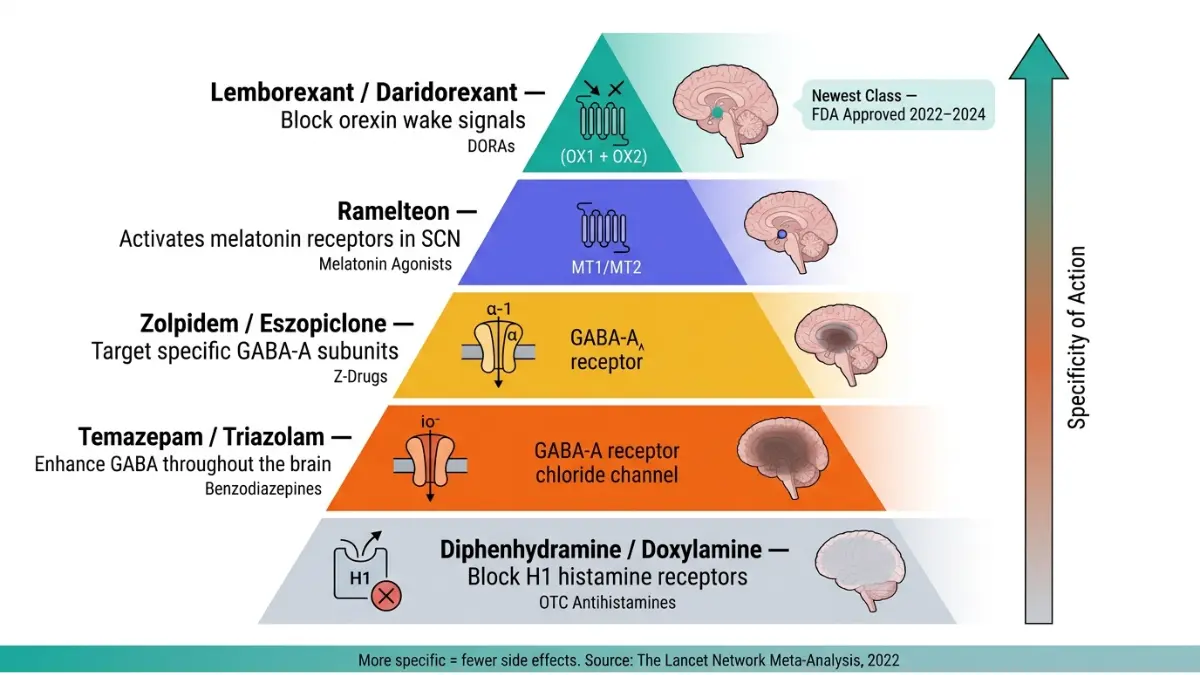
2026 Update — DORAs Are Now the Safest Prescription Class: Dual orexin receptor antagonists (DORAs) — including lemborexant and daridorexant — represent the newest FDA-approved class for insomnia. Unlike benzodiazepines that sedate the entire brain, DORAs work by specifically blocking the brain’s wakefulness signal (orexin), allowing natural sleep without disrupting REM or deep sleep stages. A 2022 landmark network meta-analysis in The Lancet — covering 170 randomized trials and 36 drug comparisons — found lemborexant and eszopiclone had the most favorable efficacy and tolerability profiles among all reviewed medications.
Natural Supplements for Sleep
| Supplement | Evidence Level | Typical Dose | Side Effects |
|---|---|---|---|
| Melatonin | Moderate | 0.5–3 mg | Minimal; avoid high doses |
| Magnesium Glycinate | Moderate | 200–400 mg | Very rare GI upset |
| L-Theanine | Low-Moderate | 100–200 mg | None reported |
| Valerian Root | Low-Moderate | 300–600 mg | Rare headache |
Important: “Natural” does not mean risk-free. Melatonin supplements can interact with blood thinners, diabetes medications, and immunosuppressants. If you’re on multiple medications, use our Pill Identifier tool to cross-check what you’re already taking before adding any supplement.
Real Risks of Sleep Medications Nobody Warns You About
This is the section your doctor may not have time to cover — and the one that could save you from years of harm.
Dependence and Rebound Insomnia
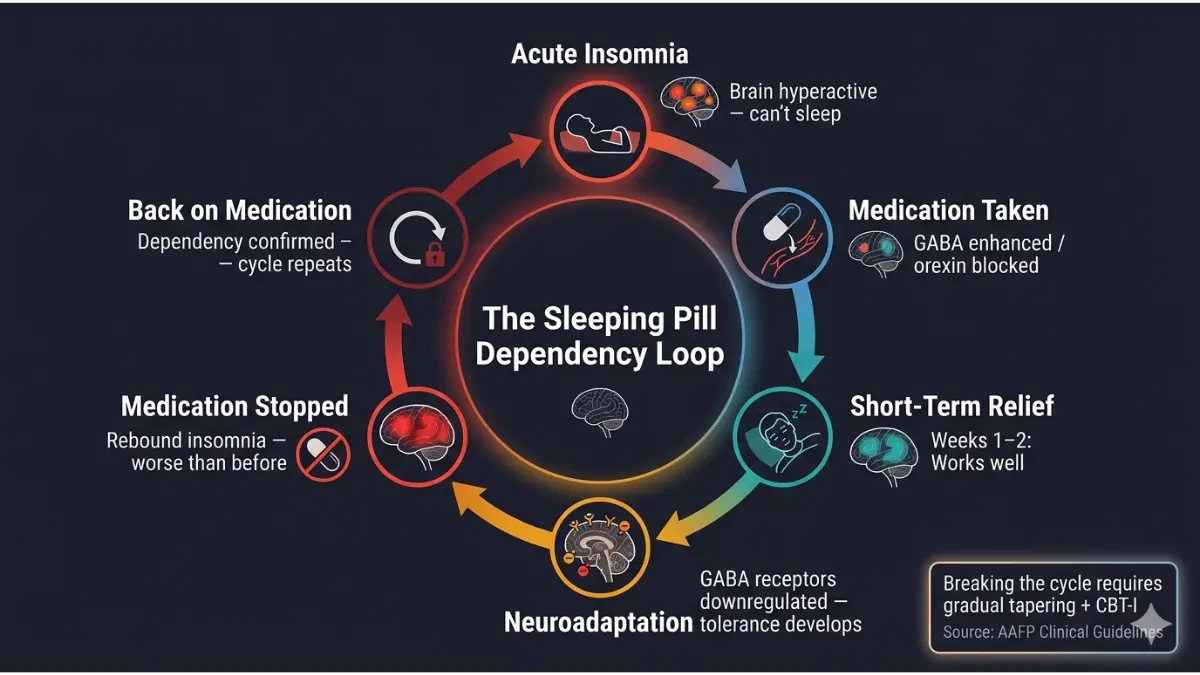
Many sleep medications create a dependency cycle that’s deeply misunderstood by patients. Here’s how it works:
- You take a sleeping pill for a few weeks
- Your brain adjusts — it stops producing its own natural sleep signals
- When you try to stop, sleep gets worse than before you started
- You assume you still need the medication
This is called rebound insomnia, and it affects a significant portion of people who stop benzodiazepines or Z-drugs. According to the American Academy of Family Physicians (AAFP), between 15% and 40% of long-term benzodiazepine users report severe withdrawal symptoms upon stopping, including anxiety, tremors, and in rare cases, seizures.
Never stop benzodiazepines or Z-drugs cold turkey. Always taper slowly under medical guidance.
Parasomnia — The Side Effect That Can Be Life-Threatening
Z-drugs like zolpidem carry a rare but documented risk of parasomnia: dangerous behaviors performed while partially asleep with no memory afterward.
Documented cases include:
- Sleepwalking — wandering through the house or outdoors
- Sleep-driving — operating a vehicle with no recollection
- Sleep-eating — consuming food, often in large quantities
The FDA issued a Black Box Warning — its strongest possible warning — for zolpidem products specifically because of these behaviors. In response, the FDA also lowered the recommended dose for women, who metabolize zolpidem more slowly and experience higher rates of next-morning impairment.
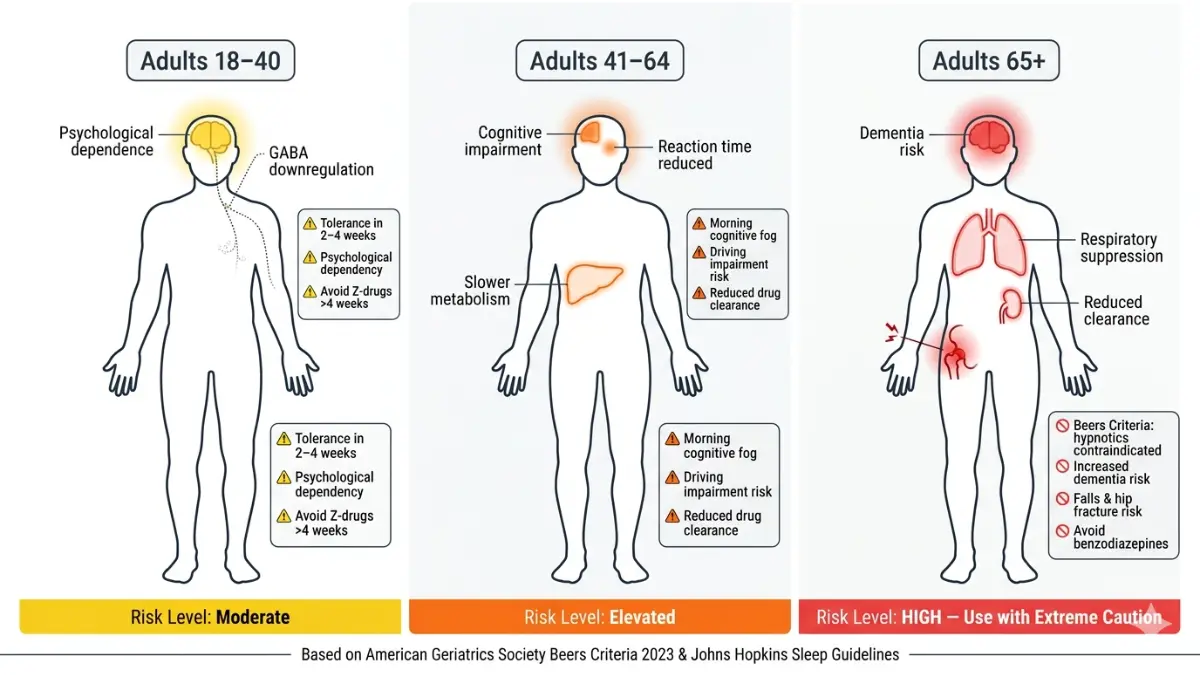
Age-Stratified Risk Table — Who Is Most Vulnerable
| Age Group | Primary Risk | Specific Warning |
|---|---|---|
| 18–40 | Tolerance & psychological dependence | Avoid Z-drugs for more than 2–4 weeks |
| 41–64 | Next-day cognitive impairment, driving risk | Do not drive the morning after taking long-acting sleep meds |
| 65+ | Falls, hip fractures, dementia | OTC antihistamines + benzodiazepines are high-risk per Beers Criteria |
The American Geriatrics Society Beers Criteria explicitly identifies most prescription hypnotics as potentially inappropriate for adults over 65 due to falls, fractures, and cognitive decline risk.
Dangerous Drug Interactions
- Opioids + sleeping pills = potentially fatal respiratory depression. The FDA has formally warned that combining opioids with any CNS depressant (including Z-drugs) can cause breathing to slow or stop entirely
- Alcohol + sleep medications = amplified sedation, dramatically increased overdose risk
- SSRIs/SNRIs + trazodone = serotonin syndrome risk at higher doses
If you suspect your current prescriptions might be contributing to your sleep problems rather than solving them, read our article on medications that cause insomnia — a commonly missed root cause.
Who Should — and Absolutely Should Not — Take Sleep Medications
Not everyone with a sleep problem needs a pill. And for certain people, sleep medications pose risks that outweigh any benefit.
✅ Sleep Medications May Be Appropriate For:
- Adults with acute short-term insomnia (travel, grief, post-surgical recovery)
- Shift workers managing circadian disruption (short-term, lowest effective dose)
- Patients with comorbid depression where sedating antidepressants treat both conditions simultaneously
❌ High-Risk Groups Who Should Avoid or Use With Extreme Caution:
- Pregnant or breastfeeding women — Benzodiazepines are classified as Category D/X (proven fetal risk). Per Mayo Clinic’s prescribing guidelines, sleeping pills are generally not safe during pregnancy
- People with obstructive sleep apnea — Sedatives suppress respiratory drive, worsening nighttime breathing; if you haven’t been evaluated, read our guide on how sleep apnea is diagnosed
- Adults 65 and older — Most sleeping pills are flagged by Beers Criteria
- Anyone with a history of substance use disorder — Dependency risk is significantly elevated
- People with liver or kidney disease — Clearance is impaired; standard doses become overdose-level doses
- Anyone taking opioid pain medications — The combination carries a documented risk of fatal respiratory depression
Safer Alternatives to Sleep Medications That Actually Work
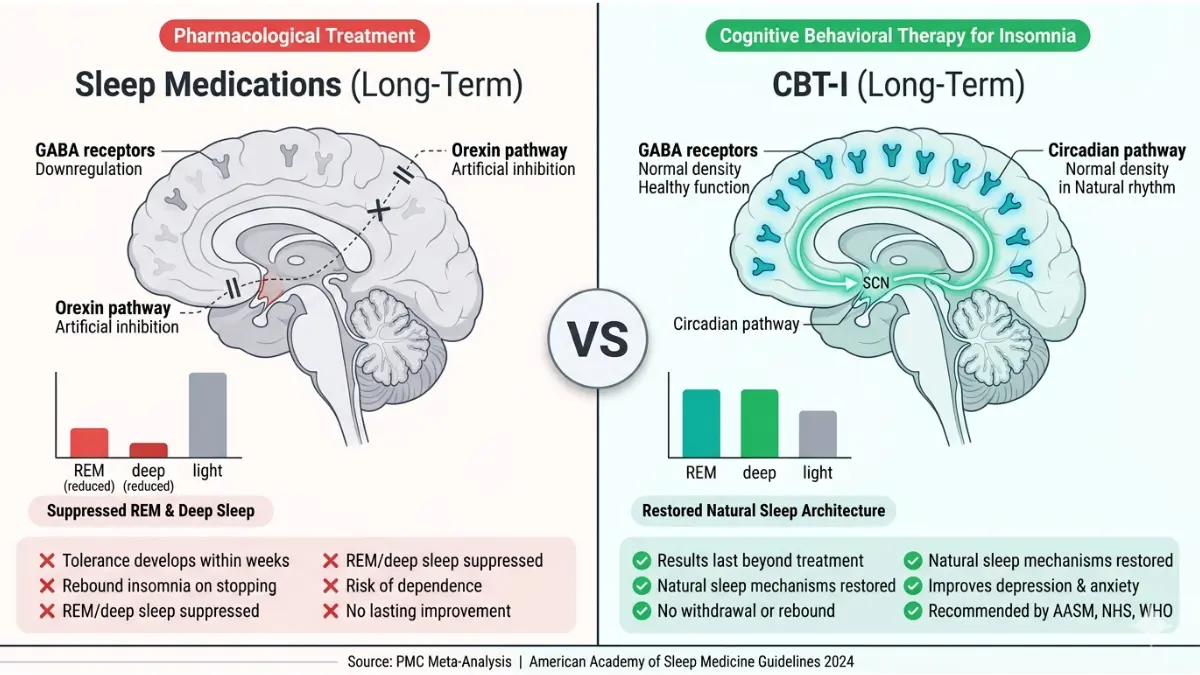
This is where the real transformation happens — and where competitors almost always fall short. The scientific evidence in 2026 is unambiguous: for chronic insomnia, behavioral therapies outperform medications in long-term outcomes, with zero side effects.
CBT-I — The Gold Standard Non-Drug Treatment
Cognitive Behavioral Therapy for Insomnia (CBT-I) is now the first-line treatment recommended by every major sleep medicine body worldwide — the American Academy of Sleep Medicine (AASM), the NHS (UK), and the Canadian Sleep Society.
According to PMC research, CBT-I produces results equivalent to sleep medication for short-term outcomes, and significantly superior results long-term — with no side effects and no rebound insomnia.
The 5 components of CBT-I:
- Sleep Restriction — Temporarily limit time in bed to build sleep pressure
- Stimulus Control — Reassociate the bed with sleep only (no phones, no reading in bed)
- Cognitive Restructuring — Replace catastrophic sleep thoughts with realistic ones
- Sleep Hygiene — Behavioral habits that support natural sleep architecture
- Relaxation Training — Progressive muscle relaxation, diaphragmatic breathing
Can’t access a therapist? The FDA-cleared Somryst® app delivers CBT-I digitally via smartphone, approved for adults 22+ with chronic insomnia. Some U.S. insurers now cover it. Find a certified CBT-I therapist through sleepeducation.org (AASM-certified sleep centers).
Evidence-Ranked Alternatives: Quick Reference
| Alternative | Evidence Level | Time to Effect | Side Effects |
|---|---|---|---|
| CBT-I | ⭐⭐⭐⭐⭐ Highest (Gold Standard) | 2–4 weeks | None |
| Sleep Restriction Therapy | ⭐⭐⭐⭐ High | 1–2 weeks | Short-term daytime fatigue |
| Melatonin (0.5–3 mg) | ⭐⭐⭐ Moderate | 1–2 weeks | Minimal |
| Magnesium Glycinate | ⭐⭐⭐ Moderate | 2–3 weeks | Rare GI upset |
| Mindfulness Meditation | ⭐⭐⭐ Moderate | 2–4 weeks | None |
| Valerian Root | ⭐⭐ Low-Moderate | Inconsistent | Rare headache |
Non-Negotiable Sleep Hygiene Rules (2026 Evidence-Based)
- Fix your wake time first — A consistent wake time (even weekends) is the single most powerful circadian anchor
- Keep your room at 65–68°F (18–20°C) — Core body temperature drop is necessary for sleep onset
- Cut all screens 60 minutes before bed — Blue light suppresses melatonin production by up to 50%
- Stop caffeine by 2 PM — Caffeine’s half-life is 5–7 hours, meaning half is still in your system at bedtime; our full breakdown is in does caffeine disrupt sleep?
- Stabilize your meal timing — Irregular eating disrupts circadian rhythm; use our Intermittent Fasting Calculator to align meals with your natural sleep-wake cycle
How to Safely Stop Taking Sleep Medications
If you’ve been taking prescription sleep aids for weeks or months, quitting abruptly is dangerous and almost guaranteed to fail.
Safe tapering protocol:
- Reduce dose by 25% every two weeks — no faster
- Simultaneously start CBT-I techniques to rebuild natural sleep
- Work with your prescribing physician throughout the process
- Expect some disrupted nights during the taper — this is normal, not failure
For anyone whose insomnia stems from anxiety or depression — both common drivers — also read our related guides on what causes insomnia and whether depression can cause sleep problems.
Expert Panel Consensus — What Doctors Across 4 Countries Recommend in 2026
The global medical community has reached a clear consensus on sleep medications in 2026. Here is what evidence-based guidelines from four Tier 1 countries now state:
🇺🇸 United States — American Academy of Sleep Medicine (AASM): The AASM’s clinical practice guideline — published in the Journal of Clinical Sleep Medicine and available via aasm.org — recommends against benzodiazepines as a first-line treatment and strongly endorses CBT-I before any pharmacological intervention for chronic insomnia.
🇬🇧 United Kingdom — NICE Guidelines: The UK’s National Institute for Health and Care Excellence (NICE CG73) specifies that hypnotic medications should only be prescribed at the lowest effective dose, for the shortest possible duration, and only after sleep hygiene and psychological interventions have been tried.
🇦🇺 Australia — Sleep Health Foundation: The Sleep Health Foundation of Australia emphasizes that sleeping pills are not a cure for insomnia and should never be used as a first or long-term response. Behavioral approaches are strongly prioritized.
🇨🇦 Canada — Canadian Sleep Society: The Canadian Sleep Society recommends against benzodiazepines as first-line for any patient group, citing high dependency risk and the availability of superior behavioral alternatives.
“Across every major sleep medicine body worldwide — AASM, NICE, the Canadian Sleep Society, and the Sleep Health Foundation of Australia — the 2026 consensus is identical: behavioral therapy first, medication only when necessary, and never indefinitely.” — Synthesized from published clinical practice guidelines, reviewed by Dr. Omar Hassan, MD
What this means for you: If your doctor’s first response to insomnia is a prescription pad, that is no longer considered best practice. You are fully within your rights to ask: “Should I try CBT-I first?”
If you’ve noticed signs beyond insomnia — excessive daytime sleepiness, morning fatigue regardless of sleep duration, or irregular breathing during sleep — these may indicate a sleep disorder requiring formal evaluation. Use our Symptom Checker to organize your symptoms before your next medical appointment, and explore our guide on warning signs of a sleep disorder for a deeper overview.
For those concerned about Xanax or benzodiazepine use specifically, our article on Xanax risks doctors warn about covers dependency and withdrawal in detail.
Frequently Asked Questions About Sleep Medications
1. What are the most common types of sleep medications?
The main categories are: OTC antihistamines (diphenhydramine, doxylamine), prescription Z-drugs (zolpidem, eszopiclone), benzodiazepines (temazepam), orexin antagonists/DORAs (lemborexant, daridorexant), melatonin agonists (ramelteon), and sedating antidepressants (trazodone, doxepin).
2. Are sleeping pills safe for long-term use?
No. Most prescription sleep medications carry risks of tolerance, dependence, cognitive impairment, and rebound insomnia with extended use. Long-term use should only occur under close physician supervision.
3. What is the safest prescription sleep medication available in 2026?
DORAs (lemborexant, daridorexant) currently have the most favorable safety profile. A 2022 Lancet network meta-analysis ranked lemborexant among the best for efficacy, acceptability, and tolerability across all drug classes studied.
4. Can I take sleeping pills every night?
Clinical guidelines recommend no more than 2–4 weeks of continuous use for most hypnotics. Nightly use beyond this window substantially increases the risk of dependence and cognitive side effects.
5. What happens when you stop taking sleeping pills suddenly?
Withdrawal can cause rebound insomnia, heightened anxiety, irritability, and — with benzodiazepines — seizures in severe cases. Always taper gradually under medical guidance rather than stopping abruptly.
6. Are OTC sleep aids like Benadryl safe?
For the occasional sleepless night, yes. For regular use, no. Long-term use of diphenhydramine has been linked to a 54% higher dementia risk, per research in JAMA Internal Medicine.
7. What is the best natural alternative to sleeping pills?
CBT-I is the gold standard — it is more effective than any drug for long-term chronic insomnia with no side effects. Low-dose melatonin (0.5–3 mg) and consistent sleep hygiene are the best evidence-based supplements.
8. Do sleep medications affect REM sleep?
Yes. Most benzodiazepines and Z-drugs suppress both deep (slow-wave) and REM sleep stages. You may sleep longer but feel less restored because the most restorative sleep stages are being chemically shortened. Read our full breakdown of sleep stages explained.
9. Which sleep medications are dangerous for adults over 65?
Benzodiazepines, Z-drugs, and OTC antihistamines are all flagged by the American Geriatrics Society Beers Criteria as potentially inappropriate for adults over 65 due to fall risk, hip fractures, and cognitive decline.
10. Can melatonin replace prescription sleep medications?
For mild sleep onset issues (jet lag, shift work, mild circadian disruption), yes — low-dose melatonin is effective and safe. For moderate-to-severe chronic insomnia, it cannot replace behavioral treatment or more targeted pharmacotherapy, but it is a reasonable first step.
11. Is CBT-I really better than sleeping pills?
For chronic insomnia, the research is conclusive: CBT-I produces equivalent short-term results and significantly superior long-term outcomes compared to sleeping pills — with no side effects, no withdrawal, and no rebound insomnia. It is the recommended first-line treatment by every major sleep medicine authority in the U.S., UK, Canada, and Australia.
Medically reviewed by Dr. Omar Hassan, MD (Internal Medicine & Sleep Disorders) and Dr. Sara Fernandez, PharmD (Pharmacology). For the latest sleep health research, visit the CDC Sleep and Sleep Disorders resource center or explore all our evidence-based health guides at mymedicineadvisor.com.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.