On This Page – Quick Medical Summary
Cognitive behavioral therapy for insomnia (CBT-I) is the #1 doctor-recommended, non-drug treatment for chronic insomnia. Delivered over 6–8 sessions, CBT-I rewires the sleep-destroying thought patterns and behaviors that keep you awake — producing results equal to sleeping pills, with no dependency, no side effects, and improvements that continue for years after treatment ends.
What Is Cognitive Behavioral Therapy for Insomnia (CBT-I)?
Marcus had been lying awake every night for eight months. It was always the same pattern — he’d get into bed at 10:30 PM, stare at the ceiling until 2:00 AM, then wake up at 5:30 feeling wrecked. His doctor prescribed Ambien. It worked for two weeks. Then it stopped working completely, and Marcus was back where he started — except now he was also worried about becoming dependent on medication.
What Marcus needed wasn’t another pill. He needed cognitive behavioral therapy for insomnia (CBT-I) — the most evidence-backed sleep treatment in medicine.
What Is CBT-I, Exactly?
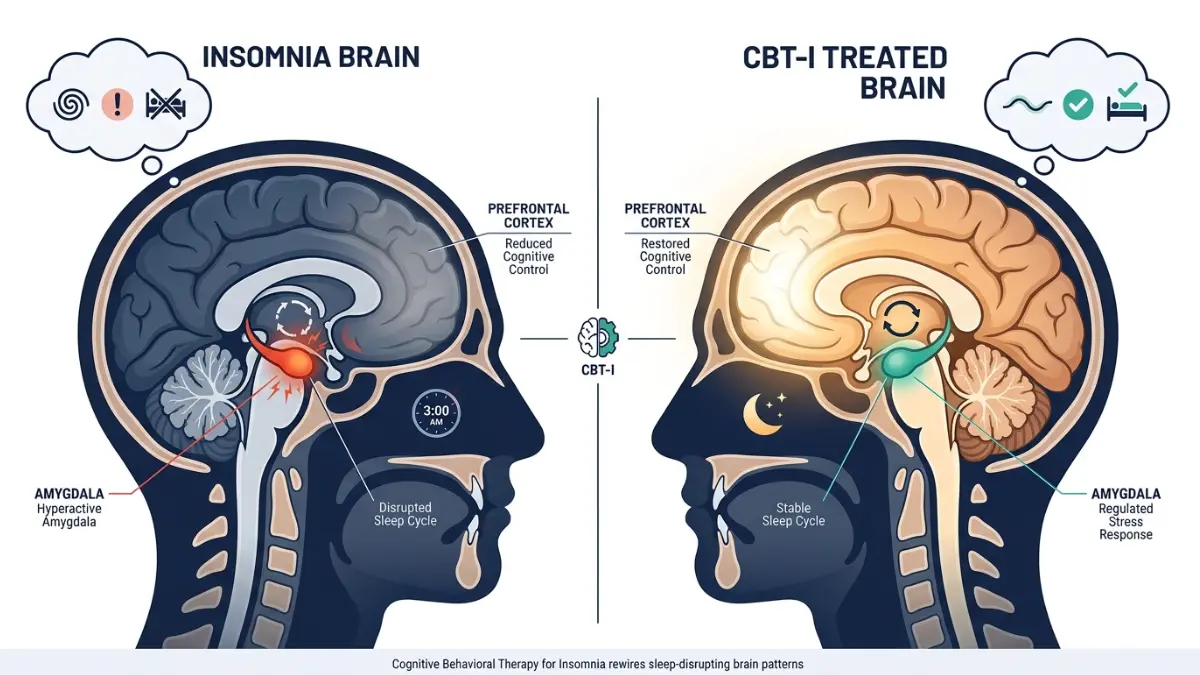
Cognitive behavioral therapy for insomnia is a structured, short-term treatment that identifies and changes the thoughts and behaviors perpetuating chronic insomnia. Unlike sleeping pills, which mask symptoms, CBT-I corrects the underlying mechanisms driving your sleeplessness.
The National Heart, Lung, and Blood Institute describes CBT-I as a 6 to 8-week treatment plan recommended as the first-line option for long-term insomnia — before any medication is considered.
CBT-I works by targeting what sleep scientists call the 3P Model of Insomnia:
| Factor | What It Means | Example |
|---|---|---|
| Predisposing | Your biological vulnerability to insomnia | Family history, anxiety tendency |
| Precipitating | The event that triggered your insomnia | Job loss, bereavement, illness |
| Perpetuating | The habits keeping insomnia alive right now | Spending 10 hours in bed, daytime napping, clock-watching |
CBT-I focuses exclusively on perpetuating factors — the habits and beliefs you can actually change. This is why it works when the stressor that first caused your sleep problems has long since passed, yet insomnia persists.
How Is CBT-I Different from Regular CBT?
This is a question most competitor sites completely ignore. Standard CBT addresses broad thought patterns across life situations. CBT-I is a highly specialized protocol — laser-focused on sleep cognitions, sleep-specific behaviors, and the physiological arousal cycle that locks insomnia in place. A therapist trained in general CBT is not automatically qualified to deliver CBT-I.
What This Means For You: If you’ve been struggling with insomnia for more than 3 months — difficulty falling asleep, staying asleep, or waking too early at least 3 nights per week — you have chronic insomnia, and CBT-I is your clinically recommended first step. Before your first session, use our Sleep Calculator to establish your baseline sleep window — this data is invaluable for your therapist.
The 5 Core CBT-I Techniques — And What Happens Each Session
This is what separates CBT-I from every other sleep advice you’ve read. It isn’t a single technique. It’s a precisely sequenced combination of methods tailored to your specific insomnia pattern.
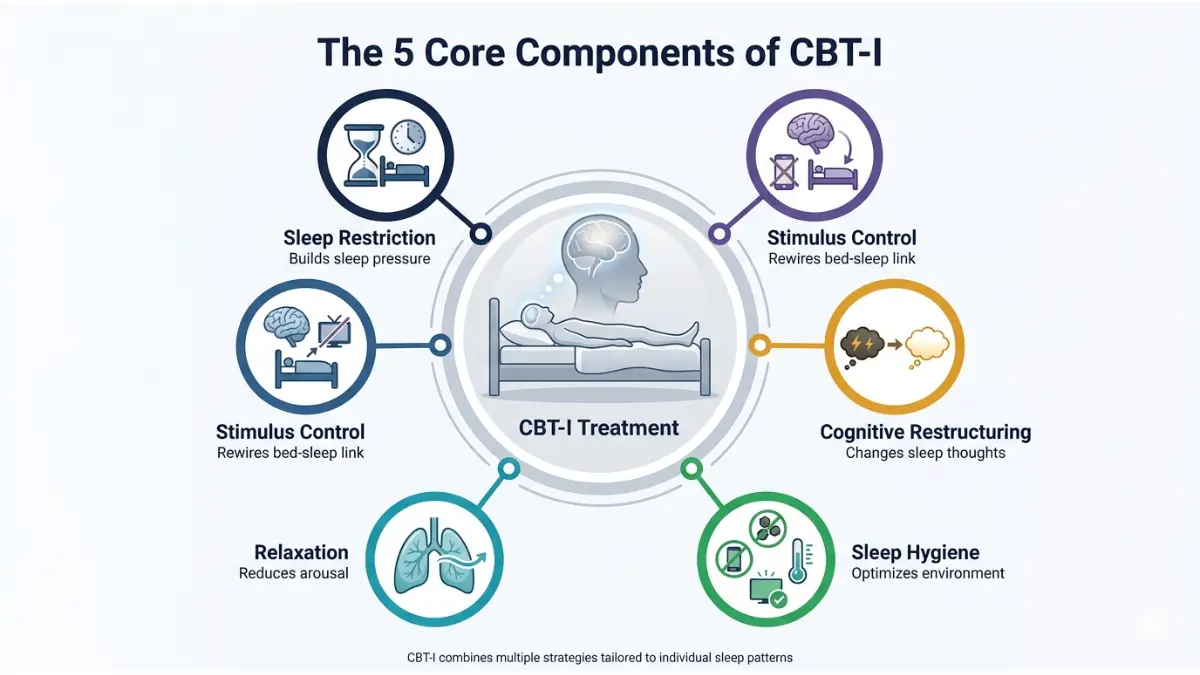
The 5 Techniques Explained
1. Sleep Restriction Therapy (SRT)
This is the hardest — and most powerful — component of CBT-I.
- Your therapist calculates how many hours you’re actually sleeping (not lying in bed)
- You are given a strict “sleep window” — typically 5–6 hours initially
- This builds up sleep pressure (the biological drive for sleep) rapidly
- As your sleep efficiency improves, your window is gradually extended
- Most patients see dramatic improvement within 2–3 weeks of beginning sleep restriction
⚡ Key Insight: Sleep restriction causes temporary tiredness in week 1. This is expected and necessary. Patients who quit at this stage miss the most powerful part of the treatment.
2. Stimulus Control Therapy
Over time, insomniacs unconsciously train their brains to associate the bedroom with wakefulness and anxiety. Stimulus control reverses this conditioning.
The core rules:
- Go to bed only when genuinely sleepy
- Use the bed only for sleep (and sex) — no phones, no TV, no reading
- If awake for more than 20 minutes, get out of bed and return only when sleepy
- Maintain a fixed wake time — even on weekends
3. Cognitive Restructuring
Chronic insomnia generates catastrophic thinking that makes the problem worse. Examples your therapist will identify and challenge:
- “If I don’t get 8 hours, tomorrow will be ruined”
- “I’ve never been a good sleeper — this is permanent”
- “I’ll get sick if I keep sleeping this badly”
Your CBT-I therapist uses structured questioning to test whether these beliefs are accurate — and replaces them with evidence-based, sleep-promoting thoughts.
4. Sleep Hygiene Education
This covers the environmental and lifestyle factors that directly affect sleep quality:
- Caffeine: Avoid within 6 hours of bedtime (caffeine has a 5–7 hour half-life)
- Alcohol: Disrupts REM sleep even if it helps you fall asleep initially — see our detailed guide on how caffeine disrupts sleep
- Light: Dim screens at least 1 hour before bed; blackout curtains help significantly
- Exercise: Regular physical activity improves sleep quality — but avoid intense workouts within 3 hours of bedtime
5. Relaxation Training
Teaches your nervous system to downregulate before bed, including:
- Progressive muscle relaxation (PMR)
- Diaphragmatic breathing
- Guided imagery
- Mindfulness meditation
Session-by-Session CBT-I Outline
| Session | Focus |
|---|---|
| 1 | Sleep diary review, insomnia assessment, sleep education, 3P model explained |
| 2 | Introduce sleep restriction therapy, set initial sleep window |
| 3 | Stimulus control rules, review sleep diary progress |
| 4 | Cognitive restructuring — identify and challenge sleep-blocking beliefs |
| 5 | Relaxation training, refine sleep window based on progress |
| 6 | Relapse prevention, maintenance strategies, exit planning |
| 7–8 | (If needed) Address residual issues, comorbidities, or poor adherence |
What This Means For You: You don’t need all 5 techniques at maximum intensity. Your therapist selects the combination most relevant to your specific insomnia pattern. If you’re unsure whether your symptoms meet the threshold for insomnia disorder, use our Symptom Checker before your first appointment.
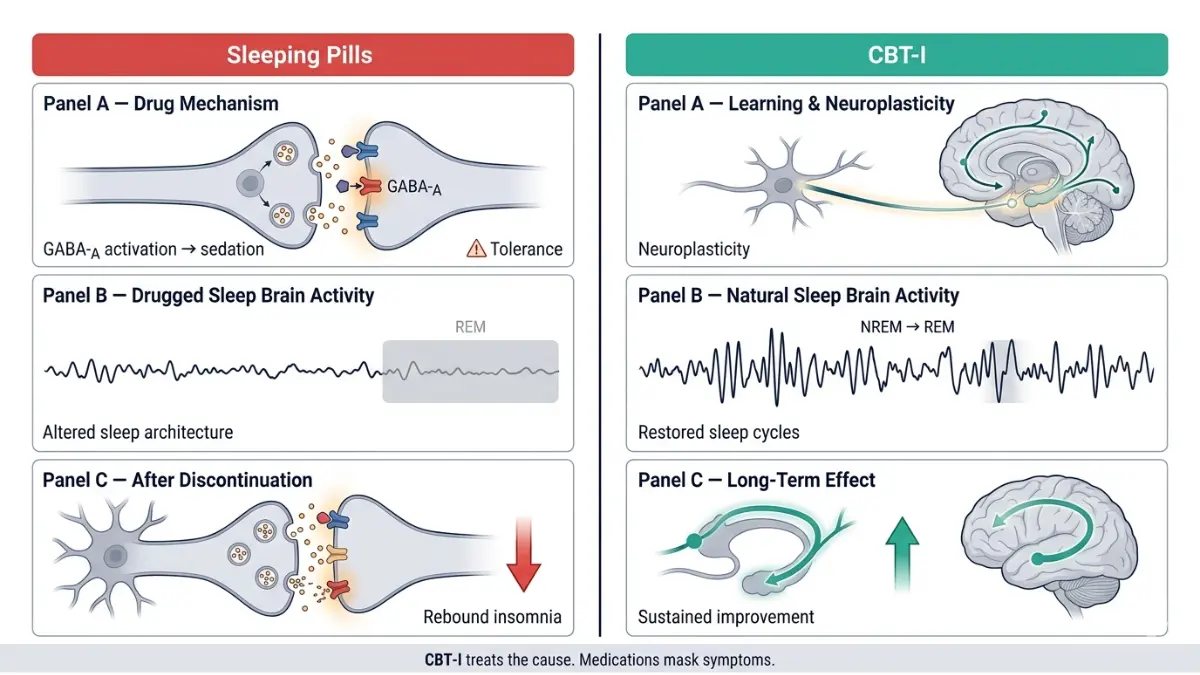
CBT-I vs. Sleeping Pills — What the 2026 Evidence Actually Shows
This is the conversation most primary care doctors aren’t having with their patients. According to CDC data, 50–70 million Americans suffer from sleep disorders — yet prescription sleep medications remain the most commonly dispensed treatment, despite not being the recommended first-line option.
Here’s what the science shows when you compare them directly:
Head-to-Head Comparison Table
| Factor | CBT-I | Sleeping Pills (Zolpidem, Eszopiclone, etc.) |
|---|---|---|
| First-line recommendation | ✅ AASM, NHS, NICE, ACP | ❌ Second-line |
| Works long-term (1–3 years) | ✅ Yes — sleep continues improving | ❌ No — effectiveness declines with use |
| Side effects | ✅ Minimal (temporary tiredness in week 1) | ❌ Dependence, amnesia, next-day drowsiness, fall risk |
| Stops working after treatment | ✅ No — skills are permanent | ❌ Yes — insomnia returns when stopped |
| Insurance/Medicare coverage (2026) | ✅ Expanding — CMS now reimburses FDA-cleared digital CBT-I | ✅ Typically covered |
| Available via app | ✅ Yes — FDA-cleared digital options | N/A |
| Suitable for older adults | ✅ Yes — preferred over pills in 65+ | ⚠️ Higher fall/cognitive risk |
The Numbers Don’t Lie
A landmark meta-analysis of 20 randomized controlled trials found CBT-I produced:
- 19-minute reduction in time to fall asleep
- 26-minute reduction in nighttime wakefulness
- 10% improvement in sleep efficiency
More impressively, a 2025 review of 49 randomized controlled trials involving over 20,000 participants confirmed that even fully digital CBT-I programs deliver moderate-to-large effects on insomnia severity — a finding that’s reshaping how American health systems are delivering insomnia care.
The 2026 Game-Changer: In 2025, the Centers for Medicare & Medicaid Services (CMS) established national reimbursement codes for FDA-cleared digital cognitive behavioral therapy for insomnia. This is the first time a digital mental health treatment has received this level of coverage — a significant policy shift that no major competitor article has covered.
💊 What This Means For You: If your doctor immediately reached for their prescription pad when you mentioned sleep problems, ask specifically about CBT-I first. Our guide on sleep medications explains exactly which drugs are prescribed, their risks, and when medication is appropriate alongside CBT-I rather than instead of it.
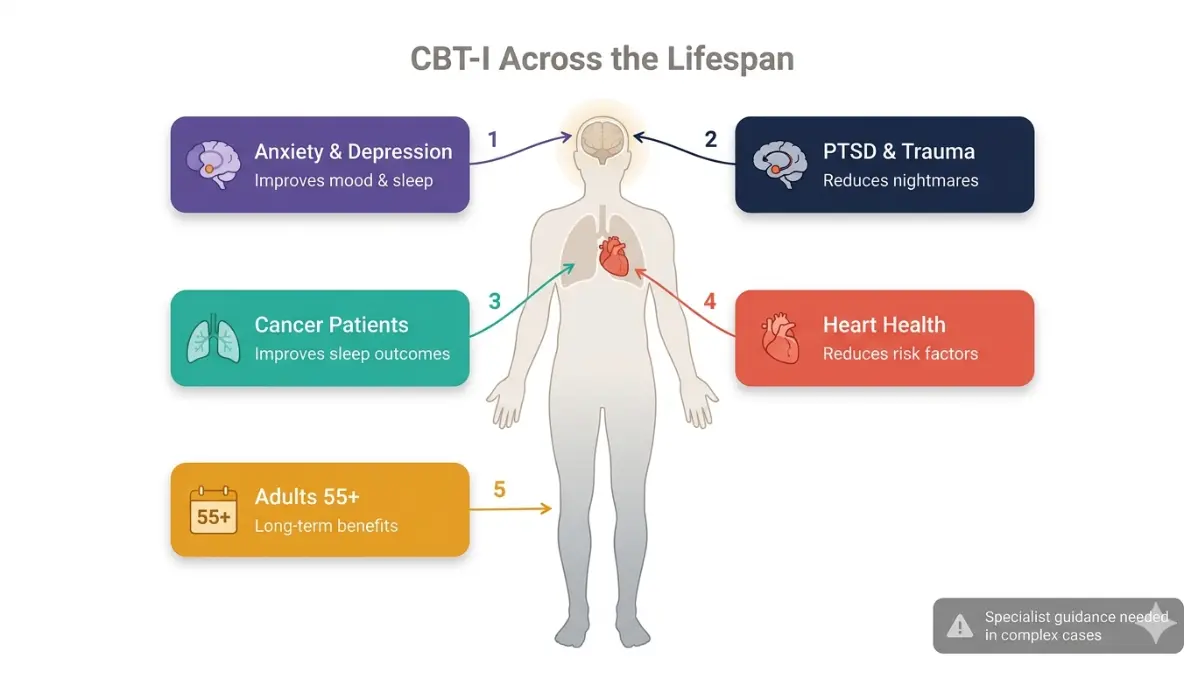
Who Is CBT-I For? Proven Effectiveness Across Conditions
Most articles on cognitive behavioral therapy for insomnia cover only “primary” chronic insomnia. This misses the majority of people who actually need it. CBT-I has been clinically validated across a wide range of conditions.
CBT-I for Anxiety and Depression
The relationship between insomnia and anxiety/depression runs both ways — each worsens the other. CBT-I is uniquely positioned to interrupt this cycle because treating insomnia with CBT-I independently improves mood and anxiety, even without targeting these conditions directly. If you suspect depression is connected to your sleep problems, read our in-depth article on whether depression causes sleep problems.
CBT-I for PTSD
Trauma-related insomnia is one of the most treatment-resistant forms of the condition. Research shows CBT-I significantly reduces nighttime PTSD symptoms including hypervigilance and fear of sleep. It is often combined with Imagery Rehearsal Therapy (IRT) — a technique where the patient rewrites and rehearses a modified version of their recurring nightmare to reduce its emotional charge.
CBT-I for Cancer Patients
Over 40% of cancer patients experience clinically significant insomnia during treatment and into survivorship. CBT-I has been validated in this population with strong evidence, and is now recommended by oncology nursing societies as a standard component of survivorship care.
CBT-I for Older Adults (55+)
A major 2025 randomized controlled trial of 311 adults aged 55–95 evaluated a digital CBT-I program (SHUTi OASIS). Participants reported sustained, clinically meaningful improvements at post-treatment, 6-month, and 12-month follow-up. This is particularly important because sleeping pills carry elevated risks in older adults — increased fall risk, cognitive impairment, and rebound insomnia — making CBT-I the strongly preferred option for this age group.
CBT-I for Shift Workers
Shift work insomnia requires a modified approach since standard sleep scheduling advice can conflict with work patterns. A behavioral sleep medicine specialist can adapt stimulus control and sleep restriction rules to accommodate rotating or overnight shifts. For more on circadian rhythm disruption underlying shift work insomnia, see our guide on what is circadian rhythm.
Conditions That Require Specialist Clearance First
CBT-I should not be started without specialist evaluation if you have:
- Untreated obstructive sleep apnea (sleep restriction can worsen apnea symptoms — get evaluated first)
- Bipolar disorder (sleep restriction can trigger hypomanic/manic episodes)
- Severe untreated depression with active suicidal ideation
- Seizure disorders (sleep deprivation lowers seizure threshold)
| Condition | CBT-I Effectiveness | Special Consideration |
|---|---|---|
| Chronic primary insomnia | ⭐⭐⭐⭐⭐ Excellent | First-line, standalone |
| Anxiety-related insomnia | ⭐⭐⭐⭐ Very Good | May combine with anxiety treatment |
| Depression + insomnia | ⭐⭐⭐⭐ Very Good | Treat both simultaneously |
| PTSD insomnia | ⭐⭐⭐⭐ Very Good | Add IRT for nightmares |
| Cancer survivorship insomnia | ⭐⭐⭐⭐ Very Good | Oncology-adapted protocol |
| Older adults (65+) | ⭐⭐⭐⭐⭐ Excellent | Preferred over medications |
| Sleep apnea + insomnia | ⭐⭐⭐ Good | Treat apnea with CPAP first |
How to Access CBT-I in 2026 — In-Person, Online & Apps
One of the biggest frustrations patients report: “My doctor mentioned CBT-I but didn’t tell me how to actually get it.” Here is the complete access guide for US patients in 2026.
Option 1: In-Person CBT-I (Gold Standard)
In-person sessions with a certified Behavioral Sleep Medicine (BSM) specialist deliver the highest effectiveness. To find one:
- USA: Search the Society of Behavioral Sleep Medicine provider directory at behavioralsleep.org
- Accredited Sleep Centers: Find an AASM-certified sleep center through sleepeducation.org — programs at these centers include behavioral sleep medicine services
- Cost: $150–$400 per session; most major insurance plans cover behavioral health, though coverage for sleep-specific CBT-I varies by plan
Ask your insurer specifically: “Is CBT-I for insomnia disorder covered under my behavioral health benefit?”
Option 2: Telehealth CBT-I
Telehealth delivery of CBT-I is now well-established and produces results comparable to in-person treatment. Your primary care provider or a psychiatrist trained in sleep medicine can deliver this by video. Many patients find telehealth removes the biggest barrier: scheduling and travel.
Option 3: Digital CBT-I (dCBT-I) Apps — 2026 Guide
This is the fastest-growing access point for cognitive behavioral therapy for insomnia in the US — and it’s evolving rapidly.
FDA-Cleared Digital CBT-I (Prescription Required):
| App | FDA Status | Insurance | Notes |
|---|---|---|---|
| SleepioRx | ✅ FDA De Novo Cleared | ✅ CMS-reimbursable (2025) | Requires physician prescription; strongest evidence base |
| Somryst | ✅ FDA De Novo Cleared | Varies | Prescription required; 9-week program |
Important: Most sleep apps you find on the App Store are NOT full CBT-I programs. They may offer relaxation sounds or basic sleep hygiene tips — valuable, but not the same as evidence-based CBT-I. Only apps with peer-reviewed published RCTs and FDA clearance deliver validated CBT-I outcomes.
A 2025 meta-analysis of 49 RCTs with over 20,000 participants confirmed that fully automated digital CBT-I programs deliver significant, sustained improvement in insomnia severity — making them a legitimate option when in-person therapy is unavailable.
Cost Summary by Pathway (USA, 2026)
| Access Method | Estimated Cost | Insurance |
|---|---|---|
| In-person BSM specialist | $150–$400/session (6–8 sessions) | Behavioral health benefit |
| Telehealth CBT-I | $100–$250/session | Often covered |
| SleepioRx (digital, prescription) | $0–$50/month | CMS-reimbursable |
| Somryst (digital, prescription) | Check with prescriber | Varies |
What This Means For You: If in-person CBT-I isn’t accessible where you live, a prescription for an FDA-cleared digital program from your primary care doctor is now a clinically valid — and increasingly insurance-covered — first step. Understanding your sleep disorder symptoms in detail before your appointment will help your provider determine the best access pathway.
CBT-I Success Rates, Realistic Timeline & What to Do If It Doesn’t Work
The Real Numbers on CBT-I Effectiveness
Let’s move past vague statements like “CBT-I is effective” and look at the actual data:
From a landmark meta-analysis of 20 RCTs:
- Sleep onset time reduced by 19 minutes on average
- Time awake during the night reduced by 26 minutes on average
- Sleep efficiency improved by 10 percentage points
- Total sleep time improved by 8 minutes — a modest number that misleads people. The goal of CBT-I is better quality, consolidated sleep, not necessarily more hours
Long-term durability: Studies tracking patients 3 years after completing CBT-I show sleep improvements continue to accumulate — the opposite of what happens with sleeping pills. Patients who complete CBT-I have genuinely learned to sleep better, not just temporarily suppressed symptoms.
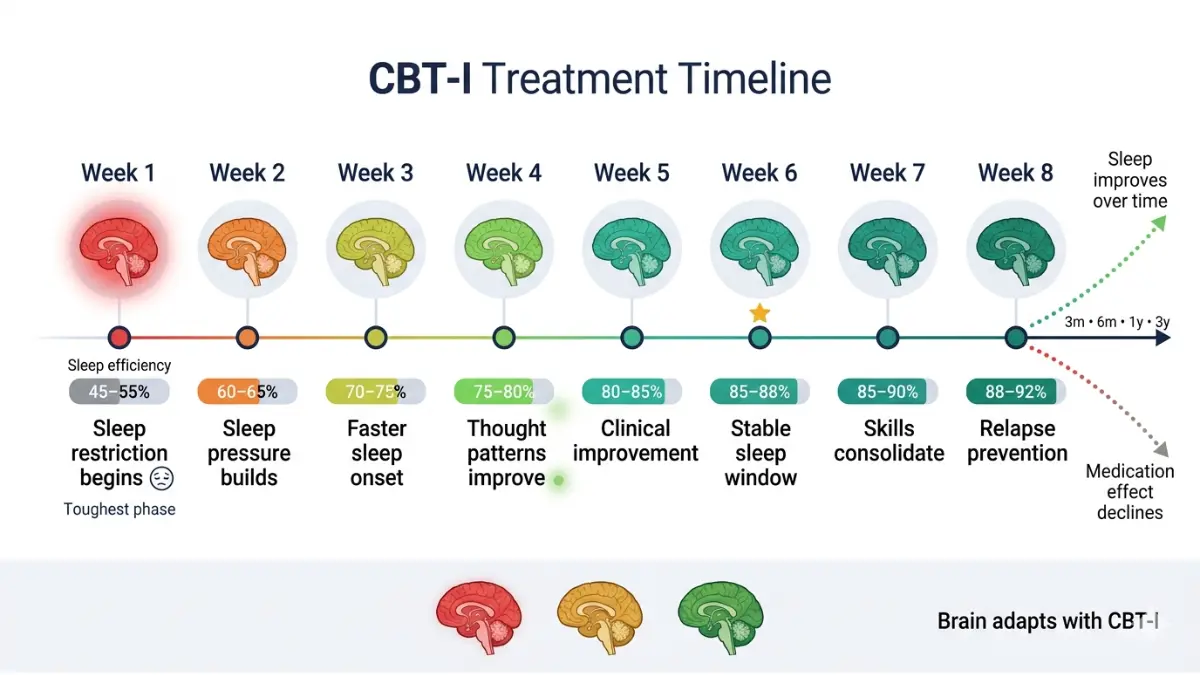
Week-by-Week Realistic Timeline
| Timeline | What to Expect |
|---|---|
| Week 1 | Tiredness, frustration — this is normal. Sleep restriction is working. |
| Week 2 | Sleep pressure builds; falling asleep becomes faster |
| Week 3–4 | Nighttime wakefulness reduces; sleep window expands |
| Week 5–6 | Most patients reach clinical improvement threshold |
| Week 7–8 | Consolidating gains; relapse prevention planning |
| 3–6 months post-treatment | Continued improvement even without sessions |
⚡ Critical Expectation-Setter: The hardest moment in CBT-I is Week 1 of sleep restriction. This is when most people quit — right before the breakthrough. If you push through Week 1, the trajectory changes significantly.
What If CBT-I Doesn’t Work?
CBT-I doesn’t work for everyone on the first attempt. If you’ve completed a full 6–8 session course and seen minimal improvement, your clinician should consider:
1. Rule out undiagnosed comorbidities
- Undiagnosed sleep apnea is the most common reason CBT-I underperforms. Before concluding CBT-I failed, consider a home sleep apnea test or a full polysomnography sleep study
2. Add Acceptance and Commitment Therapy (ACT)
- A 2014 study found that ACT — which teaches non-judgmental acceptance of sleep variability — can help CBT-I non-responders who are stuck in high-anxiety sleep monitoring
3. Biofeedback
- Listed in American Academy of Sleep Medicine treatment guidelines, biofeedback uses real-time physiological data (EEG, EMG) to train patients to reduce arousal. It’s particularly useful when anxious over-monitoring of body signals drives insomnia
4. Combination Approach
- Short-term medication alongside CBT-I (not instead of it) can bridge the gap in severe cases, particularly for patients in acute distress. This is discussed in full in our evidence review of what causes insomnia and treatments that address root causes
What This Means For You: A non-response to CBT-I is information, not failure. It signals there may be an unaddressed comorbidity or a technique adherence issue. Work with your provider rather than abandoning the approach entirely.
Your CBT-I Sleep Diary — Start Tracking Tonight
Every CBT-I program begins with 1–2 weeks of sleep diary data. This isn’t optional paperwork — it’s the clinical foundation your therapist uses to calibrate your treatment. No diary means no accurate baseline, which means a less effective treatment plan.
What to Record Each Day
| Field | What to Note |
|---|---|
| Bedtime | When did you get into bed? |
| Sleep onset | Roughly how long before you fell asleep? |
| Nighttime awakenings | How many times? How long awake? |
| Final wake time | When did you wake up for the last time? |
| Time out of bed | When did you actually get up? |
| Sleep quality rating | 1–10 scale |
| Daytime naps | Duration and timing |
| Caffeine/alcohol | Amount and timing |
| Exercise | Type and timing |
Use our Sleep Calculator alongside your diary to calculate your sleep efficiency percentage — the ratio of time asleep to time in bed. A sleep efficiency below 85% is a clinical red flag and the primary target of sleep restriction therapy.
For a complete understanding of normal versus disordered sleep patterns, our guide on sleep stages explained and hours of sleep by age provide the clinical context that makes your diary data meaningful.
Frequently Asked Questions About CBT-I
1. What exactly is CBT-I and how is it different from regular therapy?
CBT-I (cognitive behavioral therapy for insomnia) is a specialized, structured treatment targeting only the thoughts and behaviors that perpetuate sleeplessness. Unlike general CBT, it uses specific protocols — sleep restriction, stimulus control, and cognitive restructuring — tailored to sleep physiology. Regular therapists are not trained to deliver it; you need a behavioral sleep medicine specialist.
2. How many sessions does CBT-I take to work?
Most people complete 6–8 sessions over 6–8 weeks. Some cases resolve in as few as 4 sessions; complex cases with comorbidities may require up to 10. Meaningful improvement typically begins by Week 3–4, with clinical remission for most patients by Week 6.
3. Can I do CBT-I online or through an app?
Yes. FDA-cleared digital CBT-I programs (SleepioRx, Somryst) require a physician prescription and have strong clinical evidence. In 2025, CMS established reimbursement codes for these programs — making them increasingly insurance-covered. Not all sleep apps qualify; look for FDA clearance and published RCTs.
4. Is CBT-I better than sleeping pills for chronic insomnia?
For chronic insomnia, yes — according to the AASM, NHS, and American College of Physicians. CBT-I produces equivalent short-term results to sleep medication but with no dependency risk, no side effects, and improvements that continue for years after treatment ends. Sleeping pills are recommended only when CBT-I is unavailable or as a short-term bridge.
5. Does CBT-I work for anxiety-related insomnia?
Yes. Anxiety-driven insomnia responds particularly well to the cognitive restructuring component of CBT-I. Research also shows that treating insomnia with CBT-I improves anxiety symptoms independently — the benefits run in both directions.
6. How much does CBT-I cost, and is it covered by insurance?
In-person sessions typically cost $150–$400 each. Most US insurance plans cover behavioral health treatment, but coverage for sleep-specific CBT-I varies. Since 2025, FDA-cleared digital CBT-I programs are CMS-reimbursable for Medicare beneficiaries. Always call your insurer and ask specifically about “behavioral sleep medicine” or “CBT for insomnia disorder.”
7. What is sleep restriction therapy and does it make you feel worse at first?
Sleep restriction compresses your time in bed to match your actual sleep time — typically 5–6 hours initially. Yes, it causes tiredness in Week 1. This is intentional: it builds the biological sleep drive needed to consolidate your sleep. Patients who persist through the first week experience the most significant improvements.
8. Can CBT-I help with insomnia caused by PTSD or trauma?
Yes. CBT-I significantly reduces trauma-related sleep disruption, including nightmares and hypervigilance. It is often delivered alongside Imagery Rehearsal Therapy (IRT) for patients with recurring nightmares — a combination endorsed by VA sleep medicine programs for veterans with PTSD.
9. What do I do if CBT-I isn’t working for me?
First, ensure you’ve completed the full protocol (6–8 sessions with a qualified provider). If results are poor, rule out undiagnosed sleep apnea, consider ACT as an adjunct, or discuss a brief combined medication-plus-CBT-I approach with your doctor. Poor adherence — particularly skipping the sleep restriction component — is the most common reason CBT-I underperforms.
10. Is there an FDA-approved CBT-I app?
Yes. Two digital CBT-I programs have received FDA De Novo clearance: SleepioRx and Somryst. Both require a physician prescription. SleepioRx is now reimbursable under CMS codes established in 2025. These are distinct from general wellness sleep apps and have peer-reviewed clinical evidence behind them.
11. How do I find a qualified CBT-I therapist near me?
Search the Society of Behavioral Sleep Medicine (SBSM) provider directory at behavioralsleep.org — this lists certified Behavioral Sleep Medicine (CBSM) credentialed clinicians across the US. You can also find AASM-accredited sleep centers at sleepeducation.org, most of which offer behavioral sleep medicine services. Telehealth removes geographic barriers significantly.
This article is for educational purposes only and does not constitute medical advice. Always consult a qualified healthcare provider for diagnosis and treatment of insomnia or any sleep disorder.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.