On This Page – Quick Medical Summary
What Is a UCL Tear and Do You Need Surgery?
Marcus Chen, a 22-year-old Division I pitcher, felt the sharp “pop” in his elbow during the seventh inning. In that instant, his season—and potentially his career—hung in the balance. The diagnosis: Grade 2 ulnar collateral ligament tear.
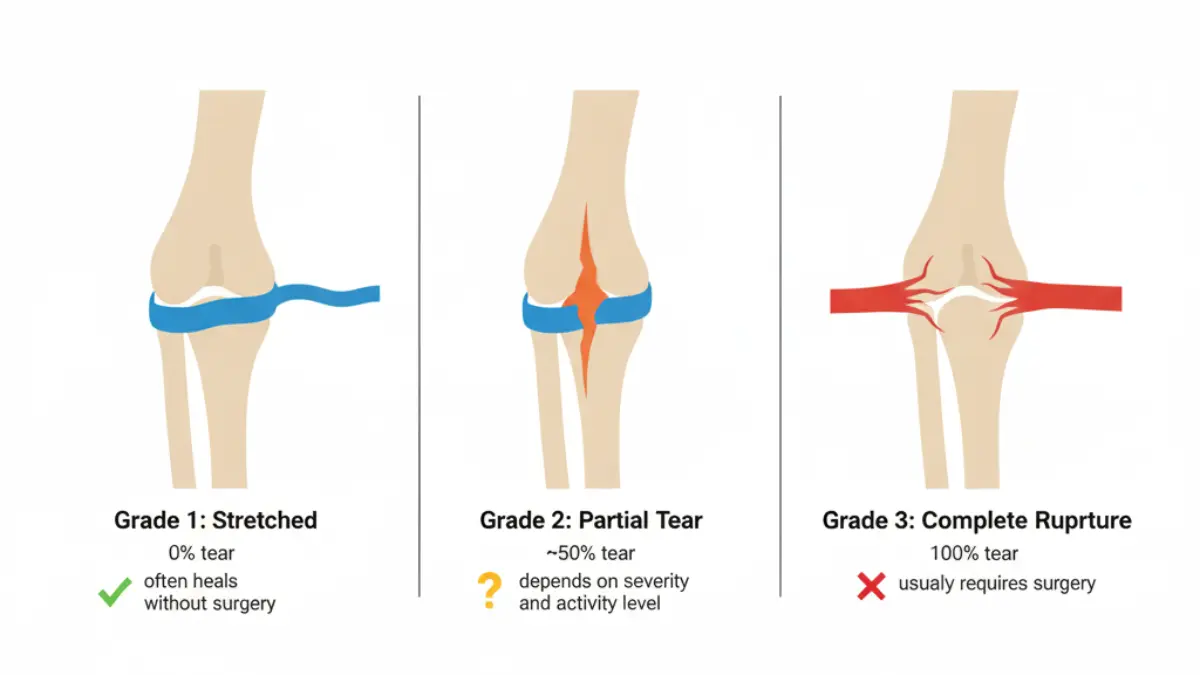
The answer to “Do I need surgery?” depends entirely on your tear grade. Grade 1 tears (ligament stretched but intact) typically heal without surgery in 85-90% of cases with 4-6 weeks of rest and physical therapy. Grade 2 tears (partial ligament disruption) represent a gray zone where treatment depends on your activity goals, age, and injury location. Grade 3 tears (complete rupture) usually require surgical reconstruction for athletes who want to return to competitive throwing.
In 2026, treatment outcomes have improved dramatically. Tommy John surgery now shows 92% success rates for return to sport—up from 85% just five years ago. New biologic treatments like platelet-rich plasma (PRP) injections offer promising results for select Grade 2 UCL injuries, with 75-88% of athletes avoiding surgery when combined with structured rehabilitation programs.
This guide covers everything you need to know: how doctors classify tear severity, when surgery becomes necessary, exact recovery timelines for each grade, real treatment costs, and the prevention strategies that reduce injury risk by 60%. Whether you’re a high school pitcher, recreational athlete, or concerned parent, you’ll find evidence-based guidance to make the right decision.
Understanding UCL Tears – Grades 1, 2, 3
What Is the Ulnar Collateral Ligament?
The ulnar collateral ligament is a thick triangular band of tissue on the inside of your elbow connecting the humerus (upper arm bone) to the ulna (forearm bone). This ligament stabilizes your elbow during overhead throwing motions, withstanding forces up to 64 Newton-meters—nearly the ligament’s breaking point—with every hard pitch.
The ligament consists of three bundles: anterior (front), posterior (back), and transverse (across). The anterior bundle is the most critical for throwing stability and the most frequently injured component in athletes.
Grade 1 UCL Tear: Stretched But Not Torn
Definition: The ligament fibers are overstretched but remain intact with no structural disruption.
Symptoms:
- Pain on the inside of the elbow during throwing
- Mild tenderness when pressing the medial elbow
- Decreased throwing velocity (5-10 mph loss)
- Pain resolves within minutes after stopping activity
Prognosis: 85-90% heal completely without surgery. Recovery takes 4-6 weeks with proper rest and rehabilitation. Most non-professional athletes return to their previous performance level.
Treatment: Rest from throwing activities, ice therapy, NSAIDs for pain management, and gradual return through a structured throwing program starting at week 5-6.
Grade 2 UCL Tear: Partial Tear (The Gray Zone)
Definition: Partial disruption of ligament fibers with some structural damage but the ligament remains partially connected.
Symptoms:
- Moderate to severe pain during throwing acceleration phase
- Noticeable loss of control and accuracy
- Velocity drop of 10-15 mph
- Pain persists 30-60 minutes after throwing
- Possible tingling in ring and pinky fingers (ulnar nerve irritation)
The Decision Crossroads: Grade 2 tears present the most difficult treatment decision. According to 2025 systematic review data, 79.7% of athletes with Grade 2 tears can return to sport with non-surgical management, but outcomes vary based on:
- Tear location: Proximal (near humerus) tears show 89.7% success with conservative treatment; distal (near ulna) tears only 41.2% success
- Age: Athletes under 25 have better non-surgical outcomes
- Activity level: Professional pitchers often choose surgery; recreational athletes succeed with PT
Treatment Options: 8-12 weeks of physical therapy, possible PRP injections (showing 75-88% success rates in recent studies), or surgical reconstruction if goals include return to competitive pitching.
Grade 3 UCL Tear: Complete Rupture
Definition: Full-thickness tear with complete ligament disruption—the two bone ends are no longer connected by ligament tissue.
Symptoms:
- Sudden “pop” sensation followed by immediate severe pain
- Inability to continue throwing
- Visible swelling within hours
- Elbow feels unstable or “loose”
- Significant weakness in gripping
Reality for Athletes: 90% of competitive throwing athletes with Grade 3 tears choose surgical reconstruction. Without surgery, the elbow remains permanently unstable for overhead activities, though daily functions typically aren’t affected.
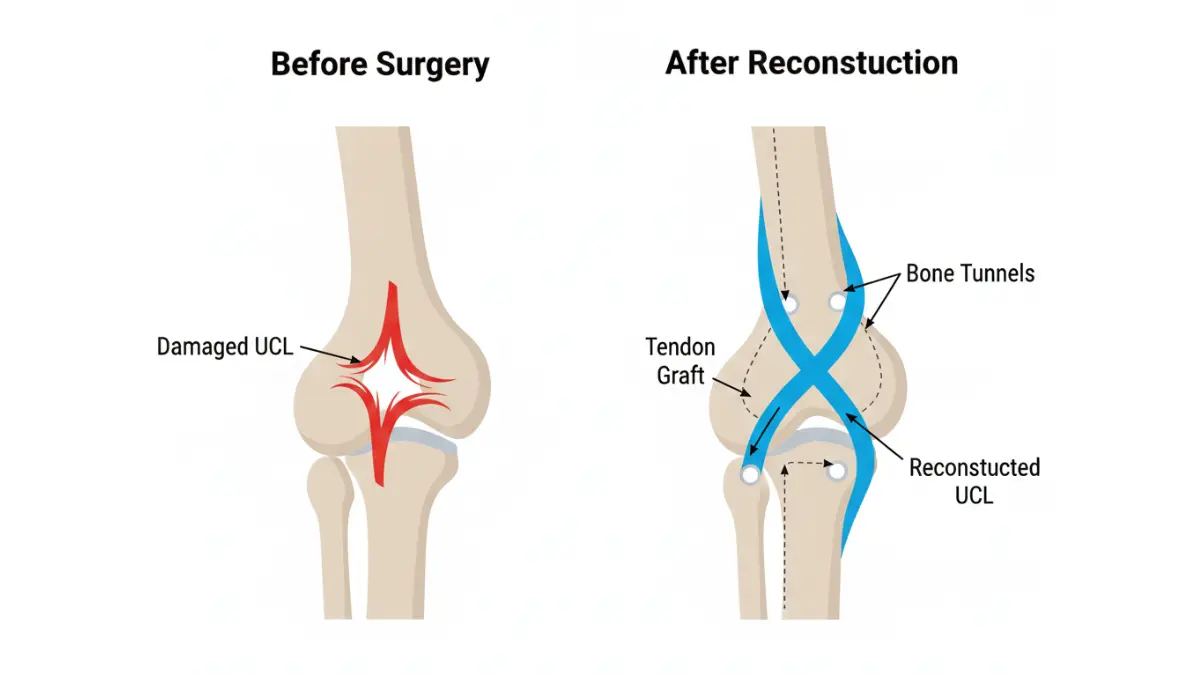
Treatment: Tommy John surgery (ulnar collateral ligament reconstruction) is the gold standard, with recovery requiring 12-18 months for return to competitive sports.
How Doctors Diagnose Your UCL Grade
Diagnosis combines clinical examination with advanced imaging:
- Physical exam: Valgus stress test applies sideways pressure to assess ligament stability
- MRI with contrast: Gold standard for visualizing ligament tears (95% accuracy)
- Ultrasound: Emerging diagnostic tool measuring elbow joint gap under stress
- Clinical correlation: Symptoms + imaging + physical exam together determine grade
| Grade | Ligament Status | Healing Time | Surgery Rate |
|---|---|---|---|
| Grade 1 | Stretched, intact | 4-6 weeks | 10-15% |
| Grade 2 | Partial tear | 8-12 weeks | 40-60% |
| Grade 3 | Complete rupture | 12-18 months (with surgery) | 85-90% |
Surgery Decision Framework
When Surgery Is Recommended
For Athletes: Surgery becomes necessary when:
- Complete Grade 3 tear with career/scholarship implications
- Grade 2 tear that failed 3+ months of conservative treatment
- Proximal or high-grade partial tears in professional/collegiate pitchers
- Age under 30 with desire to return to competitive overhead sports
- Recurrent injury after previous conservative treatment
For Non-Athletes: Surgery is rarely needed unless:
- Severe elbow instability affecting daily activities (lifting, carrying)
- Grade 3 tear with avulsion fracture (bone fragment pulled off)
- Chronic pain lasting 6+ months despite therapy
Age Considerations: Success rates for Tommy John surgery are highest in athletes under 30 (94% return to sport) compared to over 40 (72% return to sport). Older recreational athletes often achieve better outcomes with extended physical therapy.
Key Decision Factors:
- Activity goals: Return to pitching vs. recreational throwing
- Injury location: Proximal tears respond better to non-surgical treatment
- Competitive timeline: High school seniors may delay surgery until post-season
- Previous injuries: Recurrent tears typically require surgery
- Economic factors: Surgery costs $15,000-$35,000 vs. $800-$2,500 for PT only
When Conservative Treatment Works
Grade 1 Success Protocol (6-8 weeks):
- Weeks 1-2: Complete rest, ice 15-20 minutes 3x daily, NSAIDs
- Weeks 3-4: Range of motion exercises, light resistance training
- Weeks 5-6: Gradual return to throwing using interval program
- Success rate: 85-90% return to previous level
Grade 2 Conservative Approach: Recent clinical research demonstrates that properly selected Grade 2 tears can avoid surgery. A 2025 study in Arthroscopy showed 88% return-to-sport rates in athletes treated with PRP injections combined with 12-14 week rehabilitation protocols.
Best candidates for non-surgical Grade 2 treatment:
- Proximal tears (near humerus attachment)
- Recreational or non-throwing athletes
- Partial tears with <50% ligament disruption
- Athletes over age 25 without professional aspirations
- Patients willing to commit to 12-16 weeks of structured rehabilitation
2026 Biologic Treatment Options:
Platelet-Rich Plasma (PRP) Injections: Blood is drawn, centrifuged to concentrate healing platelets, then injected into the injured ligament under ultrasound guidance. Recent meta-analysis shows 75-88% of athletes with partial UCL tears return to sport after PRP therapy combined with physical therapy, with average return time of 12 weeks.
Stem Cell Therapy: Still experimental for UCL injuries. Early research shows promise but lacks large-scale clinical validation. Not yet considered standard of care.
Tommy John Surgery: What to Expect
Procedure Overview: Surgeons reconstruct the damaged ligament using a tendon graft harvested from your own body (palmaris longus from forearm, gracilis or semitendinosus from hamstring) or from a donor. Small tunnels are drilled in the humerus and ulna bones, and the graft is threaded through and secured.
2026 Surgical Techniques:
- Modified Jobe Technique: Traditional approach with excellent long-term outcomes
- Docking Technique: Smaller incisions, faster recovery, 95% strength restoration
- DANE TJ (Docking plus Interference Screw): Hybrid method combining benefits of both techniques
- Internal Brace Augmentation: Synthetic tape reinforcement (long-term data still pending)
Success Rates: Current data from the Journal of the American Academy of Orthopaedic Surgeons reports 92% of athletes return to their previous competitive level after Tommy John surgery, with MLB pitchers showing 83-87% return to major league play. These represent significant improvements from 85% success rates reported in 2020.
Surgery Duration: 60-90 minutes as an outpatient procedure under regional or general anesthesia.
Complications (occur in <5% of cases):
- Infection at incision site
- Ulnar nerve irritation (numbness/tingling in pinky/ring fingers)
- Graft failure requiring revision surgery
- Persistent pain or stiffness
- Failure to return to pre-injury performance level
Cost Breakdown: Surgery vs. Conservative Care
Understanding the financial investment helps with decision-making, especially for families evaluating treatment options for young athletes. If you’re also managing weight for optimal recovery and joint health, tools like our BMI Calculator can help track healthy ranges during rehabilitation.
Tommy John Surgery Total Costs:
- Surgeon fees: $5,000-$12,000
- Hospital/facility fees: $8,000-$18,000
- Anesthesia: $1,500-$3,000
- Post-surgical physical therapy (6+ months): $2,000-$5,000
- Total: $15,000-$35,000
Physical Therapy Only (Non-Surgical):
- Initial evaluation: $150-$300
- 24-36 PT sessions over 12-16 weeks: $800-$2,500
- Home exercise equipment: $100-$200
- Total: $800-$2,500
Insurance Coverage:
- Medicare: Covers 80% of approved surgery costs after deductible
- Private insurance: Typically covers 60-80% after deductible
- Out-of-pocket: Expect $3,000-$7,000 with insurance for surgery
- High-deductible plans: May require full payment until deductible met ($5,000-$8,000)
- Workers’ compensation: Usually covers 100% if work-related injury
Cost-Saving Strategies:
- Request pre-authorization from insurance before surgery
- Use in-network surgeons and facilities
- Ask about payment plans (most hospitals offer 12-24 month options)
- HSA/FSA funds can cover deductibles tax-free
- Compare facility costs—ambulatory surgery centers often 40% cheaper than hospitals
Recovery Timelines & What to Expect
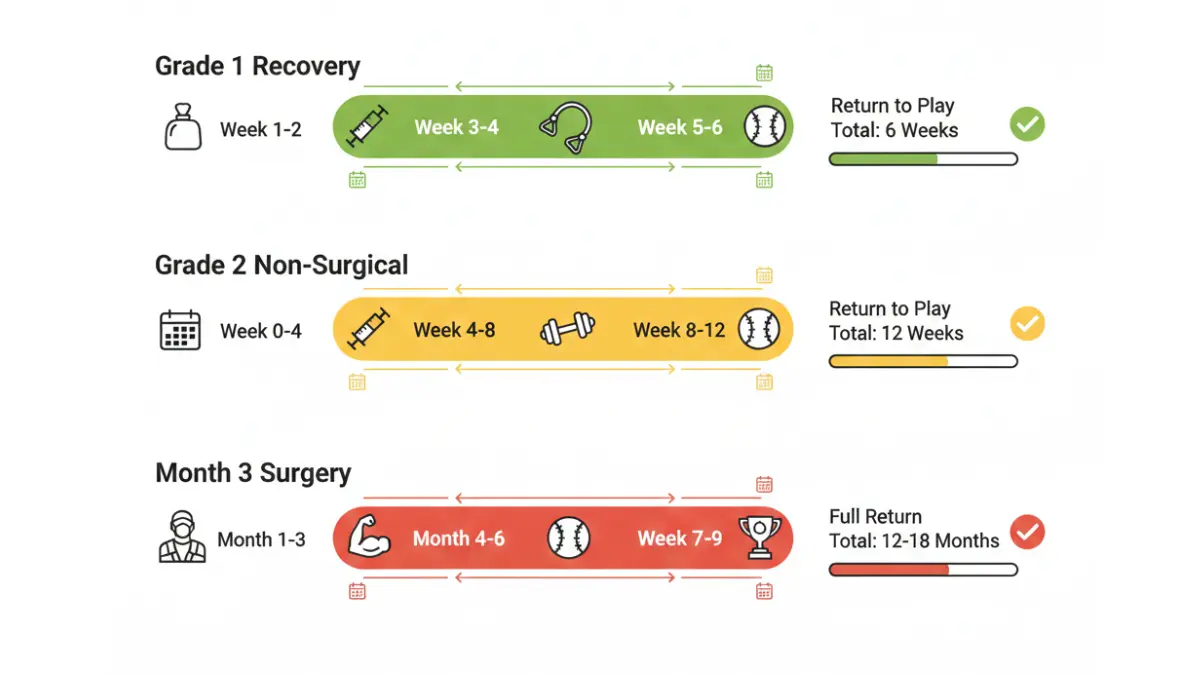
Grade 1 Recovery: 4-6 Weeks Back to Throwing
Week 1-2: Acute Protection Phase
- Complete rest from throwing and overhead activities
- Ice therapy 15-20 minutes, 3-4x daily
- NSAIDs (ibuprofen 600mg or naproxen 500mg) twice daily with food
- Maintain cardiovascular fitness through lower body conditioning using tools like our Heart Rate Zone Calculator to avoid detraining
Week 3-4: Strengthening Phase
- Begin pain-free range of motion exercises
- Wrist flexor/extensor strengthening with resistance bands
- Shoulder rotator cuff exercises (external/internal rotation)
- Scapular stabilization exercises
- Core strengthening (planks, anti-rotation movements)
Week 5-6: Return to Throwing
- Initiate interval throwing program at 50% effort
- Progress from 30 feet to 60 feet to 90 feet
- Monitor pain levels—discontinue if pain exceeds 2/10
- Gradual return to pitching mechanics with video analysis
Success Markers: Pain-free full range of motion, 90% strength return compared to uninjured arm, ability to throw at 75% effort without pain.
Grade 2 Non-Surgical Recovery: 8-12 Weeks
Phase 1 (Weeks 0-4): Protection & Inflammation Control
- Complete throwing rest minimum 4-6 weeks
- Consider PRP injection at week 2-3 if eligible
- Daily ice therapy and anti-inflammatory management
- Gentle range of motion to prevent stiffness
- Begin rotator cuff and scapular stabilization exercises
Phase 2 (Weeks 4-8): Progressive Strengthening
- Advanced forearm strengthening (FlexBar exercises, wrist weights)
- Proprioception training (balance board, ball catches)
- Simulate throwing motions without release
- Address kinetic chain deficits (hip mobility, core strength)
- Begin plyometric exercises for upper extremity
Phase 3 (Weeks 8-12): Return to Sport Progression
- Structured interval throwing program
- Pitching mechanics analysis and correction
- Pitch count restrictions (50% of pre-injury volume initially)
- Monitor velocity and accuracy benchmarks
- Weekly strength testing to ensure 95% symmetry
Real Patient Example: Jake Martinez, a 19-year-old college pitcher with Grade 2 proximal UCL tear, chose PRP injection combined with physical therapy. He returned to competitive pitching at 11 weeks with velocity matching pre-injury levels. Two years later, he remains symptom-free and was drafted by an MLB organization.
Red Flags Requiring Re-Evaluation:
- Pain increases during rehabilitation progression
- Recurrent pain after 2+ weeks of rest
- Inability to progress throwing distance
- Numbness or tingling in fingers
- Velocity loss >10% despite full effort
Tommy John Surgery Recovery: 12-18 Months Step-by-Step
Month 1-3: Protection & Early Motion
- Weeks 0-2: Elbow splinted at 90° to protect graft
- Week 3: Begin gentle passive range of motion
- Week 6: Remove splint, start active motion exercises
- Week 8: Progress to light resistance training
- No throwing activities during this phase
Month 4-6: Strengthening Without Throwing
- Focus on rebuilding forearm, shoulder, and scapular strength
- Plyometric exercises for power development
- Address kinetic chain deficits identified pre-surgery
- Simulate pitching motions without ball release
- Cardiovascular conditioning to maintain fitness
Month 7-9: Throwing Program Initiation
- Month 7: Begin long-toss program starting at 45 feet
- Month 8: Progress to 120 feet, increase to 75% effort
- Month 9: Throwing from mound (fastball only), no breaking pitches
- Gradual velocity progression monitored with radar gun
Month 10-12: Advanced Pitching Development
- Introduce breaking pitches (curveball, slider) gradually
- Bullpen sessions with pitch count restrictions
- Simulated game situations
- Video analysis of mechanics for optimal graft protection
- Continue strength maintenance program
Month 13-18: Return to Competition
- Month 13-14: Begin competitive throwing in practice games
- Month 15: Limited game appearances (2-3 innings maximum)
- Month 16-18: Full competitive return with monitoring
2026 MLB Recovery Data: Recent analysis shows the average recovery time for Major League Baseball pitchers has decreased from 16.2 months (2018-2020 data) to 14.2 months (2024-2026 data)—a testament to improved surgical techniques and rehabilitation protocols.
Success Indicators:
- Full pain-free range of motion
- Grip strength ≥95% of contralateral side
- Shoulder external rotation strength ≥90%
- Throwing velocity ≥95% of pre-injury baseline
- No pain with maximum effort throwing
Physical Therapy Essentials for All Grades
Core Exercises Critical for UCL Recovery:
- Wrist Flexor Strengthening: Reduces medial elbow stress by 23% during throwing
- External Rotation Band Work: Improves rotator cuff stability
- Scapular Retraction Exercises: Enhances shoulder mechanics
- Hip Mobility Drills: Proper hip-shoulder separation reduces elbow load
- Core Anti-Rotation: Plank variations, Pallof press improve kinetic chain
The 5-Minute Daily Routine (Prevention Focus): This evidence-based protocol demonstrated 40% faster recovery in athletes who maintained compliance throughout rehabilitation, according to biomechanics research:
- Sleeper stretch: 30 seconds each arm (posterior capsule flexibility)
- Band external rotation: 15 reps (rotator cuff activation)
- Wrist flexor/extensor stretch: 30 seconds each (forearm flexibility)
- Elbow plank: 45 seconds (core stability)
- Scapular wall slides: 15 reps (shoulder blade control)
PT Compliance = 40% Faster Recovery: Research consistently shows athletes who complete prescribed home exercises 6-7 days per week return to sport significantly faster than those with sporadic compliance.
Prevention & Risk Reduction
For Throwing Athletes: The Evidence-Based 5-Minute Daily Protocol
This scientifically validated routine reduces UCL injury risk by 60% in youth pitchers when performed 6+ days per week, according to a 2025 study published in the American Journal of Sports Medicine.
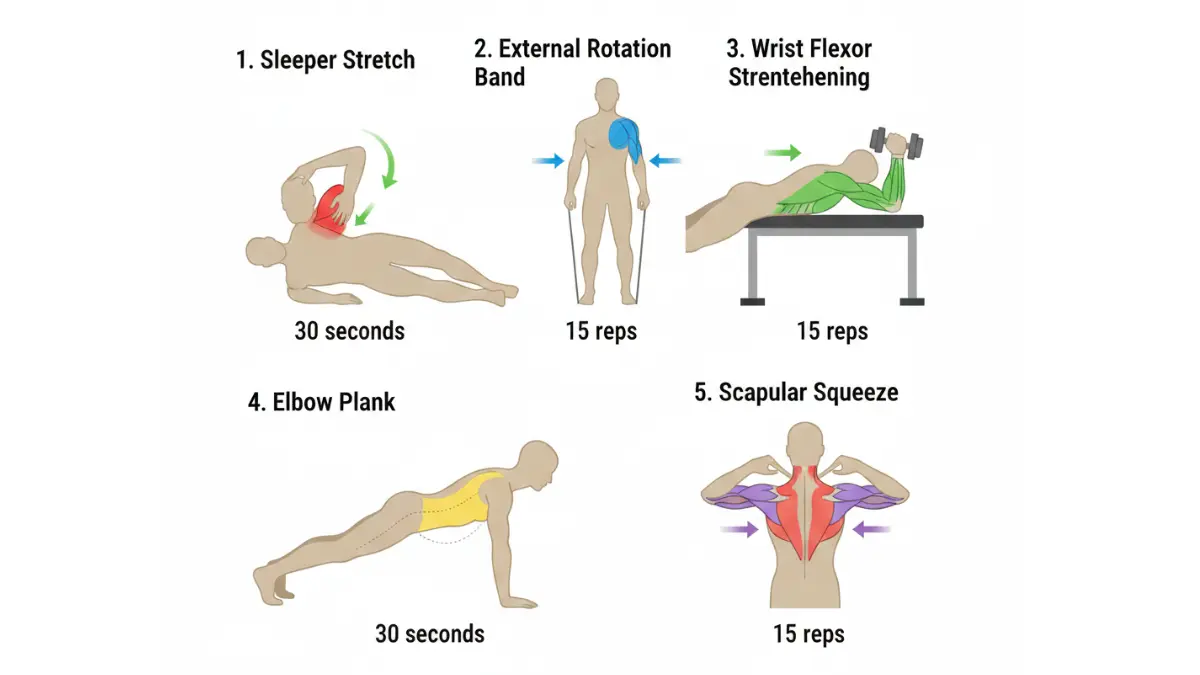
Exercise 1: Sleeper Stretch (Posterior Capsule)
- Lie on throwing side, arm at 90° in front of body
- Use opposite hand to gently press throwing hand toward ground
- Hold 30 seconds, repeat 3 times
- Purpose: Maintains shoulder internal rotation, preventing compensatory elbow stress
Exercise 2: External Rotation Band Work
- Attach resistance band at elbow height
- Elbow bent 90°, tucked to side
- Rotate forearm outward against resistance
- 15 reps, 3 sets daily
- Purpose: Strengthens rotator cuff muscles that protect elbow during throwing
Exercise 3: Wrist Flexor/Extensor Strengthening
- Use FlexBar or light dumbbells (2-5 lbs)
- Wrist curls (palms up): 15 reps
- Reverse wrist curls (palms down): 15 reps
- Purpose: Directly strengthens muscles that support medial elbow
Exercise 4: Elbow Plank Holds
- Standard plank position, hold 45-60 seconds
- Progress to side planks for lateral core stability
- Purpose: Core stability reduces compensatory stress on upper extremity
Exercise 5: Scapular Squeezes
- Stand facing wall, arms at shoulder height
- Slide arms up wall while squeezing shoulder blades together
- 15 controlled repetitions
- Purpose: Optimizes shoulder blade positioning in throwing motion
Scientific Validation: A 2025 American Journal of Sports Medicine study tracked 342 youth baseball pitchers over two seasons. Athletes performing this 5-minute routine 6+ days per week experienced 60% fewer UCL injuries compared to control group (4.2% vs. 10.8% injury rate).
Maintaining healthy body composition during training also reduces joint stress—consider using our Body Fat Percentage Calculator to track optimal ranges for athletic performance.
Pitch Count Limits & Rest Guidelines: The Non-Negotiable Rules
These evidence-based limits are endorsed by USA Baseball, Major League Baseball, and the American Sports Medicine Institute:
Youth Ages 9-12:
- 50-75 pitches per game maximum
- 2-3 days rest between outings
- No more than 8 months of competitive pitching per year
- Strict rule: No throwing breaking pitches (curveballs, sliders) before age 14
Adolescent Ages 13-16:
- 75-95 pitches per game maximum
- 3-4 days rest after 75+ pitch outing
- Limit to 100 pitches per week in combined games/practices
- 3-4 months off from competitive throwing annually
High School Ages 17-18:
- 95-110 pitches per game maximum
- 4+ days rest after 90+ pitch outing
- Monitor cumulative workload across season
- Avoid “showcase overload”—tournaments every weekend
College & Professional:
- 95-120 pitches per game (varies by organization)
- Minimum 4 days rest between starts
- Advanced biomechanics monitoring with motion capture
- Season workload management (innings pitched limits)
The Hidden Danger: Year-round throwing increases UCL tear risk by 500%. Athletes who pitch for more than 8 months per year without significant rest periods have dramatically higher injury rates, as documented by USA Baseball pitch count research.
Travel Team & Showcase Warning: The combination of weekend tournaments, travel team commitments, and showcase events creates epidemic-level injury risk. Youth pitchers throwing 100+ competitive pitches on Saturday, then pitching again Sunday, violate every evidence-based guideline.
Biomechanical Risk Factors You Can Modify
Elbow Valgus Stress During Throwing: During the late cocking phase of pitching, the elbow experiences approximately 64 Newton-meters of torque—approaching the ligament’s ultimate failure strength of 35 Nm. Proper mechanics distribute these forces across multiple joints rather than concentrating stress at the elbow.
Shoulder-Hip Separation Timing: Excessive separation (>45°) between shoulder and hip rotation at ball release transfers abnormal stress to the medial elbow. Athletes should work with pitching coaches using video analysis to optimize this crucial timing relationship.
Reduced Hip/Shoulder Mobility: Limited hip internal rotation and shoulder external rotation force compensation through increased elbow valgus stress. Research from biomechanics laboratories shows that improving hip and shoulder range of motion reduces medial elbow stress by 15-20%.
Video Analysis Benefits: High-speed video (240+ fps) identifies mechanical flaws before they cause injury:
- Early trunk rotation (opens too soon)
- Insufficient hip-shoulder separation
- Arm slot too low or inconsistent
- Poor follow-through mechanics
- Timing disruptions in kinetic chain
Professional biomechanics analysis costs $150-$400 but can prevent $30,000 surgery.
Nutrition & Recovery for Ligament Health
Collagen Synthesis Support:
- Vitamin C: 1,000mg daily promotes collagen cross-linking essential for ligament strength
- Protein: 1.6g per kilogram body weight supports tissue repair (use our Protein Intake Calculator for personalized needs)
- Glycine: 5-15g daily (collagen supplement) enhances ligament tensile strength
Anti-Inflammatory Nutrition:
- Omega-3 Fatty Acids: 2-3g daily (fish oil) reduces chronic inflammation
- Turmeric/Curcumin: 500mg curcumin with black pepper (piperine) for absorption
- Tart Cherry Juice: 8-12 oz daily reduces muscle soreness and inflammation
Hydration for Ligament Viscoelasticity: Ligaments depend on proper hydration for shock absorption properties. Athletes should consume:
- Minimum 0.5 oz water per pound body weight daily
- Additional 16-24 oz per hour of training
- Electrolyte replacement during intense activity
- Track using our Water Intake Calculator
Sleep: The Ultimate Recovery Tool:
- Youth athletes (ages 13-18): Need 8-10 hours nightly for growth hormone release
- Adults: Minimum 7-8 hours for optimal tissue repair
- Sleep deprivation: Increases injury risk by 70% in adolescent athletes
- Optimize sleep timing with our Sleep Calculator
For athletes managing injuries or recovery, understanding related conditions can be helpful—learn about other orthopedic injuries like ACL tear recovery for comprehensive joint health knowledge.
Warning Signs & When to Seek Medical Care
Red Flag Symptoms Requiring Immediate Evaluation
Emergency Symptoms (Seek Care Within 24 Hours):
- Sudden “pop” with severe pain during throwing followed by inability to continue activity
- Visible elbow deformity or significant swelling within first hour
- Numbness/tingling in ring and pinky fingers persisting more than 10 minutes (ulnar nerve compression)
- Complete inability to straighten elbow or locked joint position
- Severe pain at rest that doesn’t improve with ice and elevation
Urgent Evaluation (Within 48-72 Hours):
- Inner elbow pain lasting more than 1 week despite rest
- Progressive loss of throwing velocity (>10 mph) without explanation
- Pain during daily activities like carrying groceries or lifting objects
- Elbow instability sensation or feeling of “giving way”
- Pain that worsens rather than improves with 2 weeks of rest
When to See Your Doctor (Within 1-2 Weeks):
- Persistent medial elbow tenderness with palpation
- Gradual decline in pitching performance over several weeks
- Pain that consistently returns with resumption of throwing
- Clicking or catching sensation in elbow
- Any elbow pain in youth athlete (ages 12-16) throwing competitively
Don’t Wait—Early Diagnosis = Better Outcomes: Athletes who seek evaluation within 2 weeks of symptom onset have significantly better outcomes with conservative treatment compared to those who delay 6+ weeks. Early intervention can prevent Grade 1 tears from progressing to Grade 2 or 3 injuries.
If you’re experiencing concerning symptoms, our Symptom Checker can help you understand when to seek immediate care.
Choosing the Right Specialist
Sports Medicine Orthopedist (Preferred for Athletes):
- Fellowship-trained in sports medicine
- Specializes in upper extremity/shoulder-elbow surgery
- Performs 20+ Tommy John surgeries annually
- Works with overhead athletes regularly
Questions to Ask Your Surgeon:
- How many UCL reconstructions do you perform each year? (Look for 20+ annually)
- What is your return-to-sport rate for athletes at my competition level?
- Which surgical technique do you use and why?
- What are your complication rates?
- How many of your patients return to their previous performance level?
- What is your typical recovery timeline for my age and sport?
Hand/Upper Extremity Surgeon:
- Option for complex reconstructions or revision surgeries
- May have more experience with difficult cases
- Often affiliated with academic medical centers
Second Opinion Criteria:
- Any Grade 2 tear where treatment recommendations vary
- Career-critical decisions (college scholarship, professional contract)
- Young athletes (ages 14-18) considering surgery
- Recommendation for surgery after less than 8 weeks of conservative treatment
- Previous UCL surgery with recurrent symptoms
Finding a Qualified Specialist:
- American Orthopaedic Society for Sports Medicine physician directory
- MLB team physicians (often accept non-professional patients)
- Academic medical center sports medicine departments
- Ask for referrals from athletic trainers, physical therapists
Final Takeaways: Your UCL Tear Action Plan
Key Decision Points:
✓ Grade determines treatment path: Grade 1 = PT, Grade 2 = depends on factors, Grade 3 = usually surgery
✓ Surgery success is excellent: 92% of athletes return to competitive play after Tommy John surgery
✓ Conservative treatment works for many: 79.7% return to sport with non-surgical management for Grade 1-2 tears
✓ Recovery varies dramatically: 6 weeks (Grade 1 PT) to 18 months (Grade 3 surgery)
✓ Prevention is possible: 60% risk reduction with 5-minute daily routine and proper pitch counts
Your Next Steps:
- If you have elbow pain lasting >1 week: Schedule evaluation with sports medicine physician
- If diagnosed with UCL tear: Get MRI to determine exact grade and location
- Grade 1-2 tear: Commit to 8-12 weeks of structured rehabilitation before considering surgery
- Grade 3 tear: Consult fellowship-trained surgeon about reconstruction timing
- All athletes: Implement prevention program immediately, regardless of current symptoms
Resources for Ongoing Support:
- Continue exploring evidence-based health information in our Health Tips section
- Learn about other surgical procedures and recovery processes on our main website
- Stay informed about related orthopedic injuries including shoulder surgery recovery
Remember: Every UCL injury is unique. This guide provides evidence-based information, but your treatment plan should be individualized based on your specific injury, goals, age, and medical history. Always work with qualified healthcare professionals to make informed decisions about your care.
Frequently Asked Questions About UCL Tears
1. Can a Grade 1 UCL tear heal on its own?
Yes, 85-90% of Grade 1 UCL tears heal completely with rest and physical therapy in 4-6 weeks. Avoid all throwing activities until you’re pain-free, then follow a gradual return-to-throw program under professional guidance.
2. How long is Tommy John surgery recovery?
Recovery takes 12-18 months for competitive athletes, with 14.2 months being the average return time for MLB pitchers based on 2026 data. Recreational athletes may return to light throwing around 9-12 months.
3. What does a UCL tear feel like?
Most UCL tears cause sharp pain on the inside of the elbow during the throwing motion, particularly during the acceleration phase. Some athletes experience a sudden “pop” sensation followed by immediate severe pain, swelling, and inability to continue throwing.
4. Can you throw with a torn UCL?
Grade 1 tears may allow throwing with pain and reduced velocity. Grade 2 tears significantly impair throwing performance and accuracy. Grade 3 (complete) tears make competitive throwing impossible without surgical reconstruction.
5. Is Tommy John surgery covered by insurance?
Yes, most insurance plans cover 60-80% of Tommy John surgery costs. Expect out-of-pocket expenses of $3,000-$7,000 with insurance. Medicare covers 80% after deductible. Always verify coverage and get pre-authorization before surgery.
6. What is the success rate of UCL surgery?
Tommy John surgery has a 92% success rate for return to previous level of sport based on 2026 data. MLB pitchers show 83-87% return to major league play. Factors affecting success include age, surgical technique, rehabilitation compliance, and pre-injury performance level.
7. Do non-athletes need UCL surgery?
Rarely. Non-throwing athletes with Grade 1-2 tears usually manage successfully with physical therapy alone. Surgery is only recommended if severe elbow instability affects daily activities or if Grade 3 tear causes chronic pain and functional limitations.
8. Can PRP injections heal a UCL tear?
Emerging evidence shows promise for Grade 1-2 partial tears. Recent studies demonstrate 75-88% of athletes return to sport after PRP combined with structured rehabilitation, with average return time of 12 weeks. PRP is not effective for complete Grade 3 tears.
9. How do I know if my UCL is torn or just strained?
MRI with contrast is the gold standard for diagnosis (95% accuracy). A sports medicine physician performs a valgus stress test during physical examination. Ultrasound can measure elbow joint gap under stress. Definitive diagnosis requires combining physical exam findings with imaging results.
10. Can kids get UCL tears?
Yes, UCL tears are increasingly common in youth baseball players ages 12-16, largely due to excessive pitch counts, year-round throwing, and early introduction of breaking pitches. Prevention through strict pitch count limits and proper rest is critical for young athletes.
11. What happens if I don’t treat a UCL tear?
Grade 1-2 tears may heal slowly with extended rest but can become chronic pain conditions if you continue throwing. Grade 3 tears result in permanent elbow instability for overhead activities, with high risk of developing arthritis over time. Early treatment prevents progression and complications.
Medical Disclaimer: This article provides educational information and is not a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health provider with questions regarding a medical condition. Never disregard professional medical advice or delay seeking it because of information you read online.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.