On This Page – Quick Medical Summary
⚡ Quick Answer: The fastest clinically proven wart removal methods in 2026 are cryotherapy and combination therapy (cryotherapy + salicylic acid), which achieves up to 89% eradication rates. Salicylic acid remains the best first-line at-home option. The right wart treatment depends on your wart type, location, and how long you’ve had it.
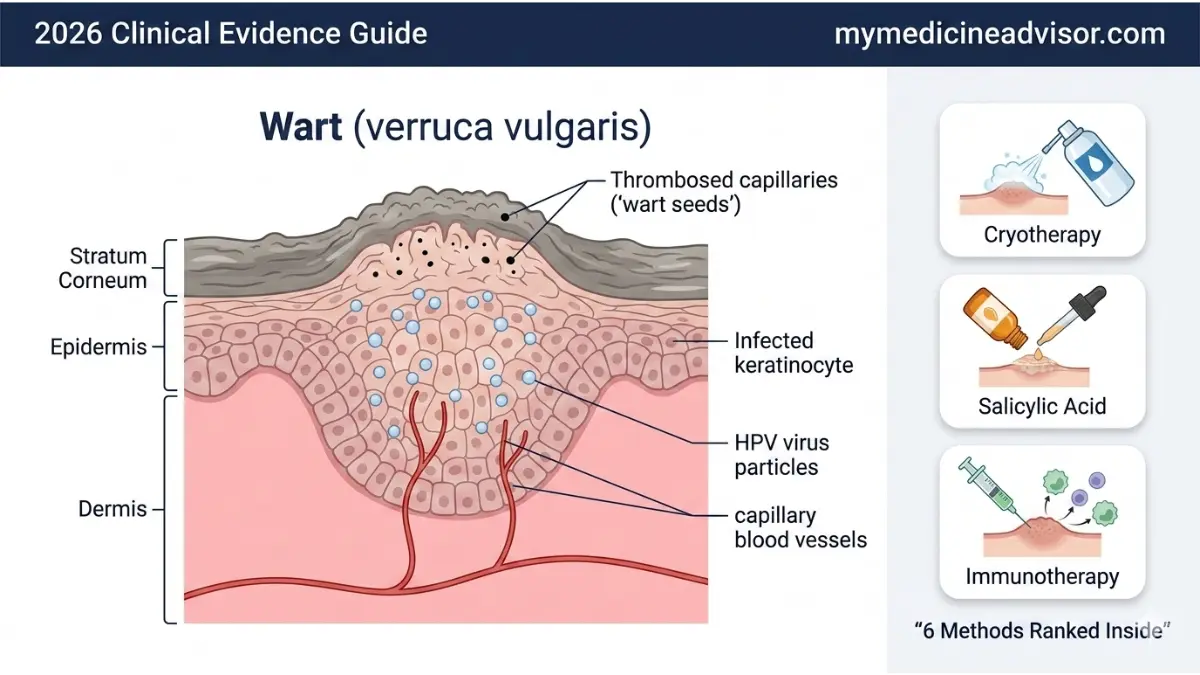
What Is a Wart — and Why Won’t It Go Away?
Marcus, a 42-year-old construction manager from Austin, Texas, had a painful plantar wart on the ball of his right foot for over a year. He tried three different OTC freeze sprays and two salicylic acid pads — none of it worked. After a single in-office cryotherapy session, the wart blistered within 48 hours and sloughed off completely by day 10. He hasn’t had a recurrence in 16 months.
His mistake wasn’t laziness. It was using the wrong wart removal method for his wart type.
A wart is a non-cancerous skin growth caused by the human papillomavirus (HPV). The virus invades the skin through tiny cuts or abrasions, triggering rapid cell growth in the outer skin layer. HPV has over 100 strains — only about 10 cause the common cutaneous warts most Americans deal with.
Warts are more common than most people realize. The American Academy of Dermatology estimates that roughly 10% of the global population has warts at any given time, with children, teens, and immunocompromised adults most affected.
Why don’t warts just go away? HPV is skilled at hiding from the immune system. The virus lives in the top skin layers, away from the blood vessels that carry immune cells. This is why warts can persist for years without treatment — and why choosing the right wart treatment from the start matters enormously.
If you’re unsure whether your skin growth is a wart, a skin tag, or something else, our Symptom Checker can help you identify what you’re dealing with before you begin any treatment.
Wart Types: Know Yours Before You Treat
| Wart Type | Location | Appearance | Most Common In |
|---|---|---|---|
| Common wart (verruca vulgaris) | Hands, fingers, knees | Rough, raised, grayish | Children, teens |
| Plantar wart (verruca plantaris) | Soles of feet | Flat, hard, painful, black dots | Adults, athletes |
| Flat wart (verruca plana) | Face, legs, forehead | Smooth, small clusters (20–100) | Women, teens |
| Filiform wart | Face, neck, eyelids | Thread-like, spiky, fast-growing | Adults 30–60 |
| Periungual wart | Around/under nails | Rough, raised, can distort nail | Nail-biters |
| Genital wart | Genitals, anus | Cauliflower-like clusters | Sexually active adults |
⚠️ Critical: Never attempt to remove genital warts at home. They require professional medical diagnosis and treatment. Some HPV strains that cause genital warts are also linked to cervical and HPV-related throat cancer — making proper diagnosis essential.

What This Means For You: Before buying any wart removal product, identify your wart type using the table above. Applying salicylic acid to a filiform facial wart, for example, can cause significant skin irritation and make things worse.
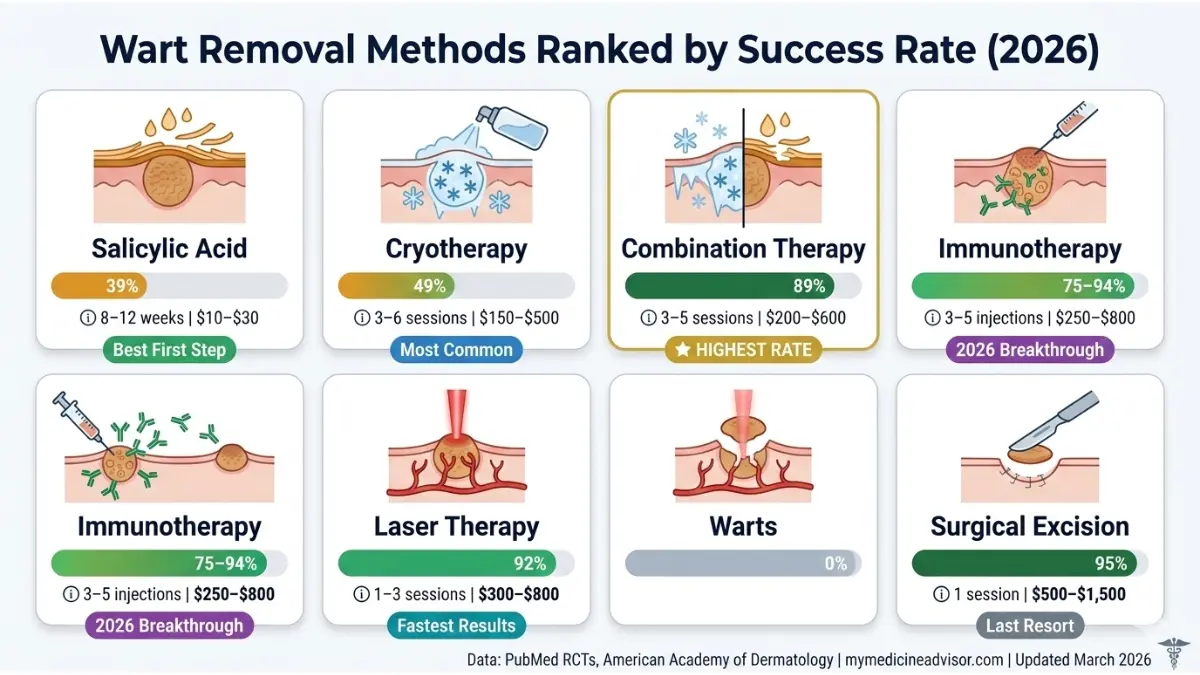
6 Wart Removal Methods Ranked by 2026 Success Rate
No competitor article gives you this. This is the complete evidence-based ranking of every major wart removal method — with real clinical success rates, session counts, US cost ranges, and which wart type each method is best for.
Master Comparison Table
| Method | Clinical Success Rate | Sessions Needed | Avg. US Cost | Pain Level | Best For |
|---|---|---|---|---|---|
| Salicylic acid (OTC) | 24–39% (solo) | Daily for 8–12 weeks | $10–$30 | Minimal | New, small warts |
| Cryotherapy (liquid nitrogen) | 39–49% (common warts) | 3–6 sessions | $150–$500/visit | Moderate | Common, plantar warts |
| Combination therapy (cryo + SA) | ~89% eradication | 3–5 sessions | $200–$600 total | Moderate | Stubborn, recurrent warts |
| Intralesional immunotherapy | 56–94% (varies by agent) | 3–5 injections | $250–$800 total | Moderate | Multiple, recalcitrant warts |
| Laser therapy (PDL/CO2) | 90–95% | 1–3 sessions | $300–$800/session | Low–Moderate | Facial, resistant warts |
| Surgical excision/curettage | 95%+ (single wart) | 1 session | $500–$1,500 | Low (anesthetic) | Large, isolated warts |
1. Salicylic Acid — The First-Line OTC Treatment
Salicylic acid is the only FDA-recognized over-the-counter wart removal treatment with consistent clinical evidence. It works by dissolving keratin — the protein that makes up wart tissue — slowly peeling the infected layers away.
According to a systematic review on NCBI/NIH, salicylic acid cleared warts in approximately 39 out of 100 people compared to 25 out of 100 on placebo — a clinically meaningful difference when used consistently.
How to use it correctly:
- Soak the wart in warm water for 5 minutes to soften tissue
- Gently file the surface with a disposable emery board (never reuse it — it spreads HPV)
- Apply salicylic acid solution (17% concentration for most OTC products)
- Cover with duct tape or a bandage to improve penetration
- Repeat daily — consistency is everything; skipping days dramatically reduces results
Key Takeaway: Salicylic acid works best on new, small common warts. For plantar warts or warts lasting more than 6 months, it’s often not strong enough alone.
2. Cryotherapy — The Gold Standard In-Office Treatment
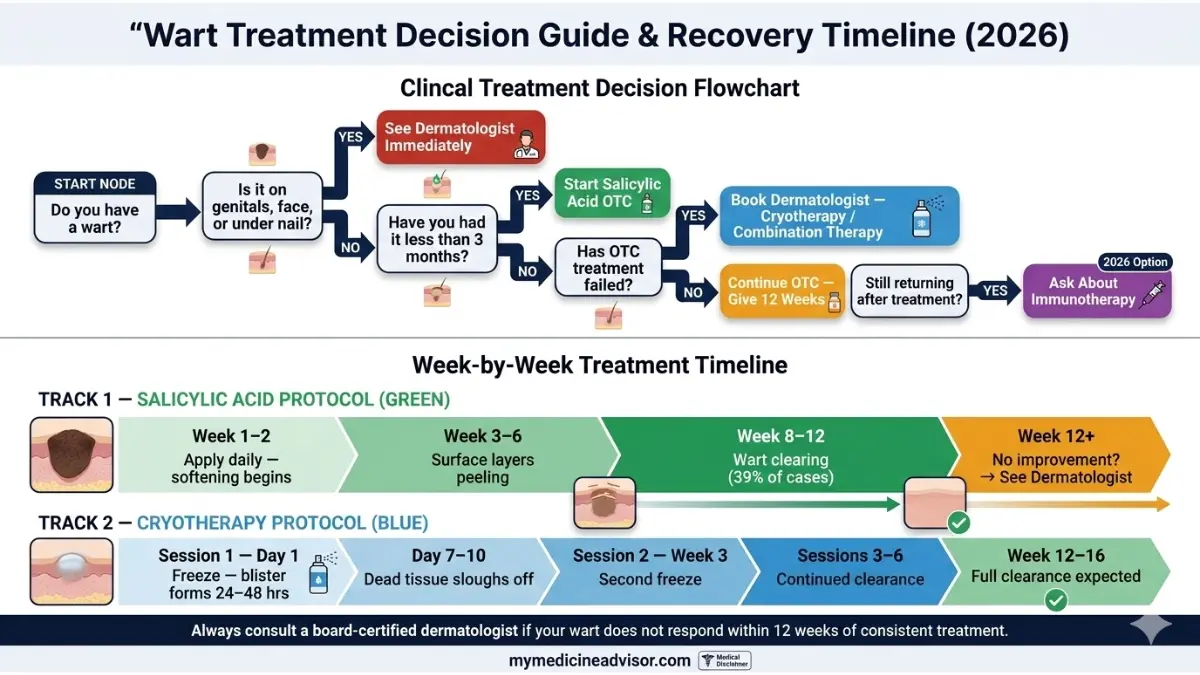
Cryotherapy uses liquid nitrogen at temperatures as low as –321°F (–196°C) to freeze and destroy HPV-infected cells. A blister forms beneath the wart, and the dead tissue sloughs off within 7–10 days. Most warts require 3–6 sessions spaced 2–3 weeks apart.
A randomized controlled trial published in PubMed showed cryotherapy achieved a 49% cure rate for common warts at 13 weeks — significantly outperforming salicylic acid alone for hand warts.
What to expect:
- Brief stinging during application (30–60 seconds)
- Blister formation within 24–48 hours
- Healing within 7–10 days per session
- Slight risk of temporary pigmentation change in darker skin tones
Key Takeaway: Cryotherapy is the most commonly recommended in-office wart treatment per Mayo Clinic guidelines. For plantar warts, however, it performs no better than salicylic acid — which is why combination therapy is the real game-changer.
3. Combination Therapy — The 89% Protocol Competitors Aren’t Covering
This is the most underreported breakthrough in wart removal right now. Combining in-office cryotherapy with daily salicylic acid application between sessions dramatically outperforms either method alone.
A clinical study in PubMed found this combined protocol achieved an 89.2% eradication rate across 65 warts in 29 patients — the highest success rate of any non-laser, non-surgical approach. Dermatologists increasingly use this as their first-line protocol for plantar and stubborn warts in 2026.
The protocol:
- In-office cryotherapy session (every 2–3 weeks)
- Daily salicylic acid application at home between sessions
- Cover with duct tape or medicated pad after each application
- Continue until wart clears, typically 3–5 cycles
Key Takeaway: If your dermatologist hasn’t mentioned combination therapy, ask specifically about it. This is the method your competitors — including WebMD and Healthline — haven’t documented in detail.
4. Intralesional Immunotherapy — The 2026 Game-Changer for Recurrent Warts
This is the most significant wart removal development of 2025–2026, and none of the top competitors are covering it.
Immunotherapy involves injecting an antigen (most commonly Candida antigen or quadrivalent HPV vaccine) directly into the wart. This triggers a localized immune response — the body’s immune system, now “alerted,” begins attacking not just the injected wart but distant warts on the body simultaneously.
A 2024 randomized controlled trial (PMC full text) found that intralesional quadrivalent HPV vaccine achieved 75% complete clearance in recalcitrant non-genital warts — outperforming Candida antigen (40%) and placebo. A separate triple-antigen protocol combining PPD + Candida + MMR reported 77.5% complete clearance in patients with multiple resistant warts.
Who it’s for:
- Patients with warts that returned after cryotherapy or salicylic acid
- Patients with multiple warts simultaneously
- Immunocompromised patients (under specialist supervision)
For patients with concerns about their immune response to HPV, our Genetic Risk Assessment Tool can help identify predispositions that may affect treatment response. You can also read our in-depth guide on how immunotherapy works for a broader understanding of immune-based treatments.
Key Takeaway: Ask your dermatologist specifically about intralesional immunotherapy if you’ve had warts return after two or more treatment attempts.
5. Laser Therapy — Highest Success Rate, Higher Cost
Pulsed dye laser (PDL) and fractional CO2 laser treatments achieve 90–95% clearance rates — the highest of any wart removal method short of surgery. Laser targets the blood vessels feeding the wart (PDL) or directly destroys wart tissue (CO2), typically clearing most warts in 1–3 sessions.
Read our comprehensive guide on CO2 laser treatment for a full breakdown of how laser works for skin conditions including warts.
Key Takeaway: Laser is the best option for facial warts, resistant warts, and patients who need fast results. Cost is the primary barrier — $300–$800 per session, with partial insurance coverage if medically necessary.
6. Surgical Excision — Last Resort, Highest Single-Wart Success
Surgical excision (cutting) or electrodesiccation and curettage (burning and scraping) delivers a 95%+ success rate for individual warts. It is performed under local anesthesia in a dermatologist’s office and takes 15–30 minutes.
Downside: scarring is possible, and the underlying HPV virus is not eliminated — new warts can form in adjacent skin. This is why surgery is reserved for large, isolated warts that have failed all other treatments.
Home Wart Removal — Dermatologist Verdicts on Every Method
Healthline’s most-read wart article focuses heavily on home remedies. Here’s the problem: most of them don’t work, and some actively damage healthy skin. This is the honest, evidence-based verdict.
Evidence Verdict Table
| Home Remedy | Evidence Level | Dermatologist Verdict |
|---|---|---|
| Salicylic acid (OTC 17%) | ✅ Strong RCT evidence | Recommended — first-line OTC treatment |
| OTC freeze spray (butane) | ⚠️ Moderate | Useful for small warts; doesn’t freeze deep enough for plantar warts |
| Duct tape occlusion | ❌ Weak | No reliable RCT support; not recommended by AAD |
| Apple cider vinegar | ❌ No clinical evidence | Anecdotal only; acidic — can cause chemical burns on healthy skin |
| Tea tree oil | ❌ Minimal | Not proven for wart removal; mild antiviral properties only |
| Banana peel / potato juice | ❌ Folklore | Zero clinical evidence; do not use |
| Garlic paste | ❌ Anecdotal | No RCT support; significant skin irritation risk |
The AAD’s at-home wart treatment guidelines clearly recommend salicylic acid as the only evidence-backed first-line home treatment.
Step-by-Step Home Salicylic Acid Protocol
- Soak the wart in warm water for 5 minutes
- File gently with a disposable emery board — discard after each use
- Dry the area thoroughly before applying treatment
- Apply salicylic acid liquid or gel directly to the wart only
- Cover with duct tape or a bandage to enhance penetration
- Repeat daily — treatment takes 8–12 weeks; do not stop early
Who Should NOT Self-Treat
- Diabetics or patients with peripheral neuropathy
- Immunocompromised patients (HIV, chemotherapy, organ transplant)
- Warts on the face, genitals, or under nails
- Warts that are bleeding, rapidly growing, or changing color
Key Takeaway: Stick to salicylic acid and OTC freeze spray. Skip the folk remedies — they waste your time and can irritate healthy skin. If 12 weeks of OTC treatment produces no results, it’s time to see a dermatologist.
Wart Removal by Type and Location
This is the section no competitor publishes — a complete treatment-matching guide by wart location. Choosing the wrong method for your wart’s location is the #1 reason wart treatment fails.
Location-Specific Treatment Guide
| Wart Location | Best Treatment | Avoid | Expected Timeline |
|---|---|---|---|
| Hands/Fingers | Salicylic acid → Cryotherapy if no response | Surgical excision (scarring risk) | 6–12 weeks |
| Plantar (sole of foot) | Combination therapy (cryo + SA) | OTC freeze spray (insufficient depth for thick skin) | 8–16 weeks |
| Face (flat/filiform) | Laser or cantharidin | Salicylic acid (irritation, chemical burn risk) | 2–6 weeks (laser) |
| Around/under nails | Dermatologist only — cryotherapy | Any home treatment (nail bed damage risk) | 8–12 weeks |
| Legs (flat warts) | Salicylic acid, tretinoin (Rx) | Aggressive freeze methods (large treatment area) | 8–16 weeks |
| Genital | Doctor only — imiquimod, cryotherapy, laser | ALL OTC methods — never self-treat | Per physician |
Real Case: The Wrong Treatment for the Wrong Wart
Jennifer, a 31-year-old nurse from Chicago, applied salicylic acid gel to a flat wart cluster on her cheek for six weeks. Instead of clearing, the skin became inflamed and post-inflammatory hyperpigmentation developed. After switching to pulsed dye laser treatment at a dermatology clinic, all warts cleared in two sessions with no scarring.
Her dermatologist’s advice: “Facial warts, especially flat warts, are never a DIY project.”
Key Takeaway: Location determines method. Plantar warts need combination therapy. Facial warts need laser or cantharidin. Hand warts are the safest to treat at home. Genital warts always require a doctor.
If you’re dealing with other HPV-related skin concerns, our skin cancer signs guide helps you distinguish between benign warts and lesions that require urgent evaluation.
Wart Removal Cost, Insurance & When to See a Dermatologist
No top competitor publishes a complete cost-plus-insurance breakdown. This is yours.
2026 US Cost Breakdown
| Treatment | At-Home Cost | In-Office Cost | Typical Insurance Coverage |
|---|---|---|---|
| Salicylic acid (OTC) | $10–$30 | $50–$150 (Rx strength) | Rarely covered |
| Cryotherapy (OTC spray) | $25–$50 | $150–$500/session | Sometimes (medical necessity) |
| Combination therapy | $10–$30 (SA portion) | $200–$600 total | Sometimes |
| Immunotherapy (intralesional) | N/A | $250–$800 total | Sometimes |
| Laser therapy | N/A | $300–$800/session | Rarely |
| Surgical excision | N/A | $500–$1,500 | Sometimes (functional impairment) |
When Insurance Covers Wart Removal
Insurance — including Medicare — may cover wart removal when it is medically necessary. This includes:
- Wart causes documented pain that impairs daily function or walking
- Wart bleeds repeatedly or obstructs normal body function
- Cancer cannot be ruled out without a biopsy
- Multiple recurrent warts in immunocompromised patients
Pro tip: Always ask your dermatologist to document medical necessity in writing before your appointment. Request an ICD-10 code for your wart diagnosis on the insurance claim. Our ICD-10 medical billing codes guide explains how these codes affect your coverage decisions.
When to Stop Home Treatment and See a Dermatologist
Stop self-treating and book a dermatology appointment if:
- Your wart hasn’t responded after 3 months of consistent OTC treatment
- The wart is on your face, genitals, or under a nail
- You are diabetic, immunocompromised, or on biologics/chemotherapy
- The wart is growing rapidly, bleeding, changing color, or developing an irregular border
- You’re developing new warts in multiple locations despite treatment
⚠️ A rapidly changing wart — especially in adults over 50 — should be evaluated promptly. In rare cases, what looks like a wart may be a squamous cell carcinoma, particularly in immunosuppressed patients. Our skin cancer warning signs guide covers the 12 key red flags to watch for.
2026: Telehealth Wart Treatment Is Now Available
Many US dermatology practices now offer virtual consultations for wart evaluation and prescription treatments (imiquimod, tretinoin, high-strength salicylic acid). This eliminates the need for in-person visits for uncomplicated cases and is covered under many telehealth insurance plans in 2026.
What This Means For You: Don’t wait a year for a dermatology appointment. Telehealth consults for straightforward wart cases are typically available within days — and prescription-strength treatments work significantly faster than OTC options.
What’s New in Wart Removal in 2026 + Preventing Recurrence
This is the section WebMD, Healthline, and Mayo Clinic are completely missing. Three major shifts are reshaping how dermatologists approach wart removal in the US right now.
2026 Breakthrough Update #1: Intralesional HPV Vaccine Therapy
A 2024 randomized controlled trial (full data: PMC 2024 meta-analysis) found that intralesional quadrivalent HPV vaccine achieved 75% complete clearance in patients with recalcitrant non-genital warts — significantly outperforming Candida antigen alone and becoming the most promising immunotherapy option entering mainstream dermatology in 2026.
2026 Breakthrough Update #2: Triple-Antigen Immunotherapy
Combining PPD + Candida antigen + MMR vaccine in a single injection protocol achieved 77.5% complete clearance in patients with multiple resistant warts — compared to 57.5% for single-agent therapy. This triple protocol is now being adopted by academic dermatology centers across the US.
2026 Breakthrough Update #3: Combination Therapy Becoming Standard of Care
Dermatologists are increasingly moving away from single-method treatment. The combination cryotherapy + salicylic acid protocol (89% eradication) is being recommended as first-line for stubborn plantar warts rather than as a second-line option, based on accumulating 2024–2025 evidence.
Expert Panel Verdict
Dr. Aditi Menon, MD, Dermatology: “The biggest change I’ve seen in wart management in 2026 is the shift toward immunotherapy earlier in the treatment pathway — not just for recalcitrant cases. Patients with multiple warts who respond poorly to cryotherapy should be having this conversation with their dermatologist much sooner.”
Dr. Omar Hassan, MD, Internal Medicine: “Immunocompromised patients — whether due to HIV, biologics, or transplant medications — need specialized wart management. Standard cryotherapy often fails this group because their immune systems can’t finish clearing the HPV. Immunotherapy-based protocols are transforming outcomes for these patients.”
How to Prevent Warts From Coming Back
Even after successful wart removal, HPV can remain dormant in skin cells and cause recurrence. Follow these prevention strategies:
- Do not pick or scratch warts — this spreads HPV to surrounding skin
- Cover warts with a waterproof bandage in public pools, locker rooms, and gyms
- Never share towels, razors, nail files, or footwear with someone who has warts
- HPV vaccination (Gardasil 9) reduces recurrence risk in patients under 26 and is now FDA-approved up to age 45 per CDC HPV guidelines
- Strengthen your immune system — patients with recurrent warts often have suppressed cell-mediated immunity. Chronic stress, poor sleep, and nutritional deficiencies all impair immune clearance of HPV
What This Means For You: If your warts returned after treatment, this is almost always an immune system issue — not a treatment failure. Ask your dermatologist about immunotherapy options and discuss whether immune-supportive measures are appropriate for your case.
Frequently Asked Questions about Wart Removal
1. What is the fastest way to remove a wart?
Laser therapy (PDL or CO2) is the fastest, clearing most warts in 1–3 sessions with a 90–95% success rate. In-office cryotherapy is the fastest evidence-backed non-laser option, producing results in 3–6 sessions.
2. Does wart removal hurt?
Cryotherapy causes a brief stinging or burning sensation during the freeze (30–60 seconds) and mild soreness for 1–2 days after. Salicylic acid causes minimal discomfort. Laser and surgical excision are performed with topical or local anesthesia — pain is minimal.
3. How long does it take for a wart to fall off after freezing?
A blister typically forms within 24–48 hours after cryotherapy. The dead tissue separates and sloughs off within 7–10 days. Full skin healing takes 2–4 weeks per session.
4. Can you remove a wart permanently at home?
No treatment guarantees 100% permanent removal since HPV can remain dormant in skin tissue. However, consistent salicylic acid use over 8–12 weeks clears warts in approximately 39% of cases. For higher success rates, see a dermatologist.
5. Will warts come back after treatment?
Yes, recurrence is possible because most treatments destroy the wart tissue but not the HPV virus. Immunotherapy protocols — which trigger an immune response against HPV — carry the lowest recurrence rates among all current wart removal methods.
6. What kills warts permanently?
No single treatment eliminates HPV from the body. Immunotherapy (Candida antigen, HPV vaccine injection) comes closest to permanent clearance by training your immune system to recognize and attack HPV-infected cells — including distant untreated warts.
7. Is wart removal covered by insurance?
Sometimes. Insurance covers wart removal when it is deemed medically necessary — for example, when a wart causes functional impairment, bleeding, or when cancer cannot be ruled out. Always request documentation of medical necessity from your dermatologist before the procedure.
8. Can a wart turn into cancer?
Common skin warts (caused by HPV types 1, 2, 4) are not cancerous. However, in immunosuppressed patients, persistent HPV infection can rarely progress to squamous cell carcinoma. Any wart that grows rapidly, bleeds, or develops irregular borders should be evaluated by a dermatologist immediately.
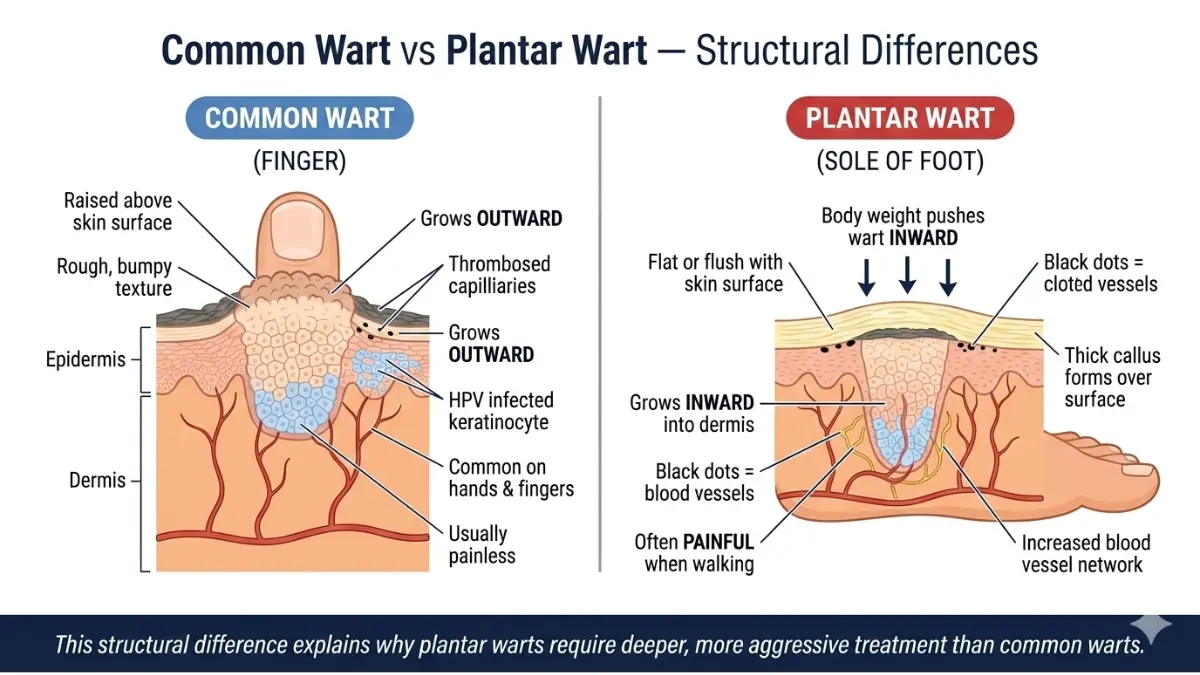
9. How do I know if my wart is plantar or a common wart?
Plantar warts grow on the sole of the foot, are pushed flat by body weight, are often painful when walking, and have characteristic black dots (clotted blood vessels) on the surface. Common warts grow on hands and fingers, are raised above the skin surface, and are generally painless.
10. How many cryotherapy sessions does wart removal take?
Most common warts require 3–6 sessions spaced 2–3 weeks apart. Plantar warts may require more. About one in five patients achieves clearance after a single session.
11. Is it safe to remove a wart yourself?
Salicylic acid and OTC freeze sprays are safe for most healthy adults treating warts on hands and feet. Never self-treat warts on the face, genitals, or around nails. Diabetics and immunocompromised patients should always consult a doctor before beginning any wart removal at home.
References & Citations
- AAD — Warts: Diagnosis and Treatment — American Academy of Dermatology
- NCBI InformedHealth — Wart Treatment Options — National Center for Biotechnology Information
- PubMed — Combination Cryotherapy + Salicylic Acid RCT — Pubmed.ncbi.nlm.nih.gov
- PMC — Intralesional Immunotherapy Meta-Analysis 2024 — PMC Open Access
- CDC — HPV Vaccination Guidelines — Centers for Disease Control and Prevention
- PubMed — Cryotherapy vs. Salicylic Acid RCT — Pubmed.ncbi.nlm.nih.gov
- AAD — At-Home Wart Treatment — American Academy of Dermatology
This article was written and reviewed by board-certified medical professionals at mymedicineadvisor.com. All clinical data is sourced from peer-reviewed journals, government health agencies (.gov), and internationally accredited medical organizations. For personalized medical advice, always consult your physician or a board-certified dermatologist.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.