
On This Page – Quick Medical Summary
HPV Throat Cancer: 11 Signs That Appear 7 Years Early
Michael, a 52-year-old financial advisor from Boston, felt a small, painless lump on the side of his neck while shaving one morning in 2017. He dismissed it as a swollen gland. Seven years later, doctors diagnosed him with stage III HPV-positive oropharyngeal cancer. A revolutionary blood test now detects these cancers up to a decade before symptoms emerge—but most men remain unaware of the early warning signs that could save their lives.
HPV throat cancer, medically termed oropharyngeal cancer HPV-positive, develops when human papillomavirus—specifically HPV-16—infects cells in the tonsils, base of tongue, or throat. Breakthrough research from Mass General Brigham revealed that specialized blood testing can identify circulating tumor HPV DNA in patients an average of 7.8 years before clinical diagnosis, creating an unprecedented window for life-saving intervention. Men face six times higher risk than women, with incidence now exceeding cervical cancer rates in the United States.
The disease progresses silently during its early stages. Most patients notice subtle changes—a persistent sore throat, unexplained neck swelling, or difficulty swallowing—that mirror common benign conditions. This diagnostic ambiguity explains why 60% of HPV throat cancer cases reach advanced stages before detection. Yet when caught early through screening or symptom recognition, survival rates soar above 95% with modern de-escalated treatment protocols.
What This Means For You:
If you’re experiencing unexplained throat symptoms lasting more than two weeks, neck lumps, or persistent ear pain, immediate medical evaluation is critical. The Symptom Checker can help assess your risk level in under two minutes, though it never replaces professional diagnosis.
New HPV throat cancer screening blood tests are now available at select academic medical centers and specialized oncology practices nationwide. The HPV-DeepSeek screening protocol, currently offered through research programs and early-access clinical sites, detects cancer-causing HPV DNA fragments years before tumors become visible on imaging. High-risk individuals—men aged 40-60 with multiple lifetime oral sex partners or known HPV-16 infection—should discuss screening eligibility with their primary care provider or oncologist.
The Centers for Disease Control and Prevention estimates HPV causes approximately 70% of all oropharyngeal cancers in the United States, with rates climbing 3% annually since 2015. Unlike cervical cancer, which has established screening protocols, throat cancer HPV testing remains limited to high-risk populations and research settings—creating an urgent need for public awareness about early warning signs that appear years before diagnosis.
The 11 Early Warning Signs
11 Early Signs of HPV Throat Cancer That Appear Years Before Diagnosis
Research from Mass General Brigham demonstrates that circulating tumor HPV DNA appears in bloodstreams an average of 7.8 years before clinical diagnosis—but physical symptoms often emerge 2-4 years into this window. Recognizing these early warning signs enables intervention when treatment is most effective and survival rates exceed 95%.
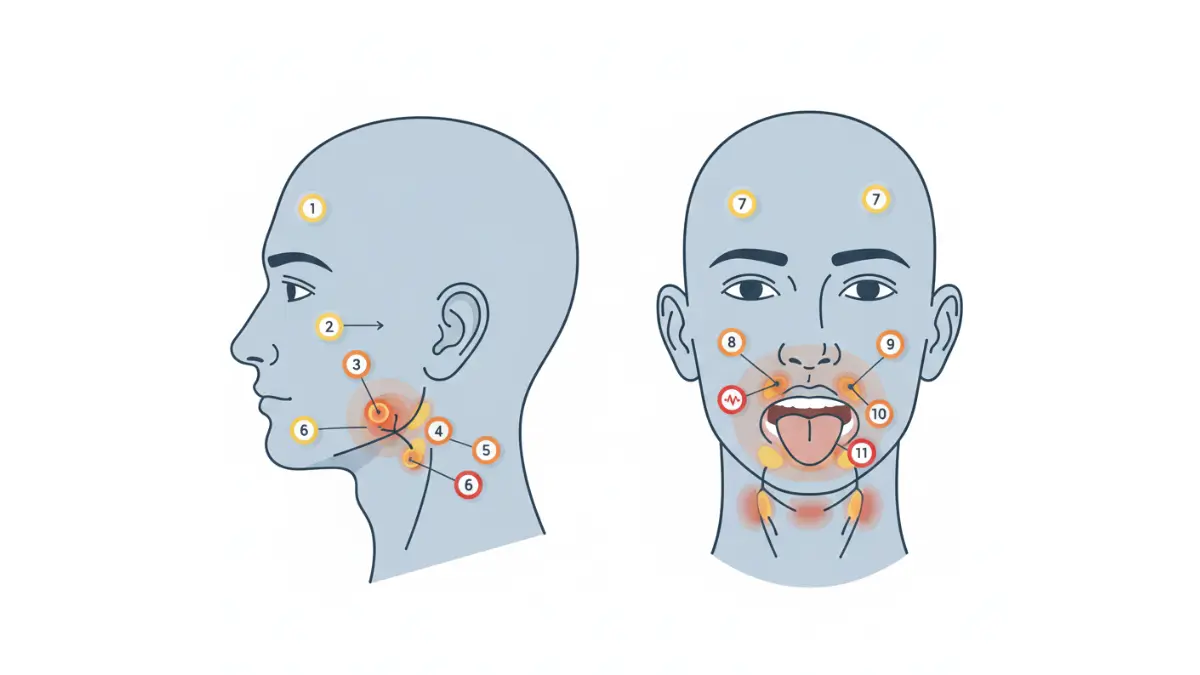
1. Painless Neck Lumps (Swollen Lymph Nodes)
The most common early presentation of HPV throat cancer involves firm, painless lumps along the sides or back of the neck. Unlike infection-related swelling that resolves within weeks, cancerous lymph nodes persist and gradually enlarge over months. These enlarged nodes typically measure 1-3 centimeters and feel rubbery rather than tender.
2. Persistent Sore Throat Lasting 2+ Weeks
A sore throat that doesn’t resolve after two weeks—even with antibiotics—warrants immediate medical evaluation. HPV-positive oropharyngeal cancer frequently causes chronic throat discomfort that patients describe as a constant “raw” sensation. This differs from viral pharyngitis, which typically improves within 7-10 days.
3. Difficulty Swallowing (Dysphagia)
Progressive swallowing difficulty, medically termed dysphagia, occurs when tumors develop on the tonsils or base of tongue. Patients initially notice problems with solid foods, then liquids as disease advances. Weight loss often accompanies this symptom as eating becomes increasingly uncomfortable.
4. Unexplained Ear Pain (Otalgia)
Referred ear pain represents one of the most overlooked HPV throat cancer symptoms. Tumors in the oropharynx share nerve pathways with the ear, causing persistent aching or sharp pain without visible ear infection. This pain typically affects one side and worsens with swallowing.
5. Voice Changes and Persistent Hoarseness
Hoarseness lasting more than three weeks signals potential throat involvement. HPV-related throat cancer affecting the vocal cords or base of tongue produces gradual voice deterioration—patients sound increasingly raspy or strained. Unlike laryngitis, this hoarseness progressively worsens rather than fluctuating day-to-day.
6. White or Red Patches on Tonsils
Leukoplakia (white patches) or erythroplakia (red patches) on tonsil surfaces indicate abnormal cell changes. These lesions appear flat or slightly raised and don’t scrape off like oral thrush. The National Cancer Institute emphasizes that any persistent oral discoloration requires biopsy evaluation.
7. Unexplained Weight Loss
Unintentional weight loss exceeding 5% of body weight within six months—without dietary changes—frequently accompanies early oropharyngeal cancer. This results from swallowing difficulties, reduced appetite, and metabolic changes associated with malignancy. Tracking body composition changes with a BMI Calculator helps identify concerning trends.
8. Chronic Cough Without Infection
A persistent dry cough lasting more than three weeks, unresponsive to typical cold treatments, may indicate throat cancer. This cough often worsens at night and produces minimal phlegm. Patients describe a constant irritation sensation in the throat that triggers coughing episodes.
9. Tongue Swelling or Numbness
Base of tongue tumors cause swelling, numbness, or altered sensation when eating or speaking. Patients report feeling like their tongue is “too large” for their mouth or experiencing tingling on one side. This symptom progressively interferes with articulation and swallowing mechanics.
10. Coughing Up Blood (Hemoptysis)
Hemoptysis—coughing blood-streaked saliva or mucus—requires emergency medical evaluation. While small amounts may indicate tumor surface irritation, any blood in oral secretions demands immediate diagnostic workup. This symptom typically appears when tumors erode surface blood vessels.
11. Mouth Numbness or Tingling
Advanced oropharyngeal cancer can affect cranial nerves, producing facial numbness, mouth tingling, or difficulty fully opening the jaw. These neurological symptoms indicate potential tumor spread to surrounding structures. The Genetic Risk Assessment Tool helps evaluate whether your risk factors warrant immediate screening.
HPV-Positive vs HPV-Negative Throat Cancer
When to See a Doctor Immediately
Contact your healthcare provider within 48 hours if you experience:
- Any neck lump persisting longer than two weeks
- Sore throat unresponsive to antibiotics for 14+ days
- Swallowing difficulty with solid foods or liquids
- Ear pain without visible infection for 10+ days
- Hoarseness lasting more than three weeks
- Any blood in saliva or mucus
Commercial Bridge:
Early symptom recognition dramatically improves outcomes. While waiting for medical appointments, document symptom duration and severity—this information helps physicians determine appropriate diagnostic pathways. Related cancer screening information is available in our comprehensive guides on cervical cancer symptoms and thyroid cancer warning signs, which share similar HPV-related risk factors.
Breakthrough Early Detection & Screening
Revolutionary Blood Test Detects HPV Throat Cancer 7-10 Years Before Symptoms
HPV-DeepSeek: The Game-Changing Screening Protocol
Mass General Brigham researchers unveiled HPV-DeepSeek in September 2025, demonstrating that blood-based screening for HPV throat cancer detection achieves unprecedented early identification windows. The liquid biopsy technology analyzes circulating tumor HPV DNA—viral genome fragments released by developing cancers years before tumors become clinically apparent.
Breakthrough Detection Statistics:
- 79% sensitivity in detecting cancer 7.8 years before diagnosis
- 96% accuracy when combined with machine learning algorithms
- 100% specificity eliminating false positive results
- 10-15 year cancer development window creates unprecedented intervention opportunities
The HPV-DeepSeek test utilizes whole genome sequencing to identify HPV-16 DNA fragments circulating in plasma. Unlike transient oral HPV infections that clear naturally, persistent circulating tumor HPV DNA indicates active malignant transformation.
Current HPV Throat Cancer Screening Options
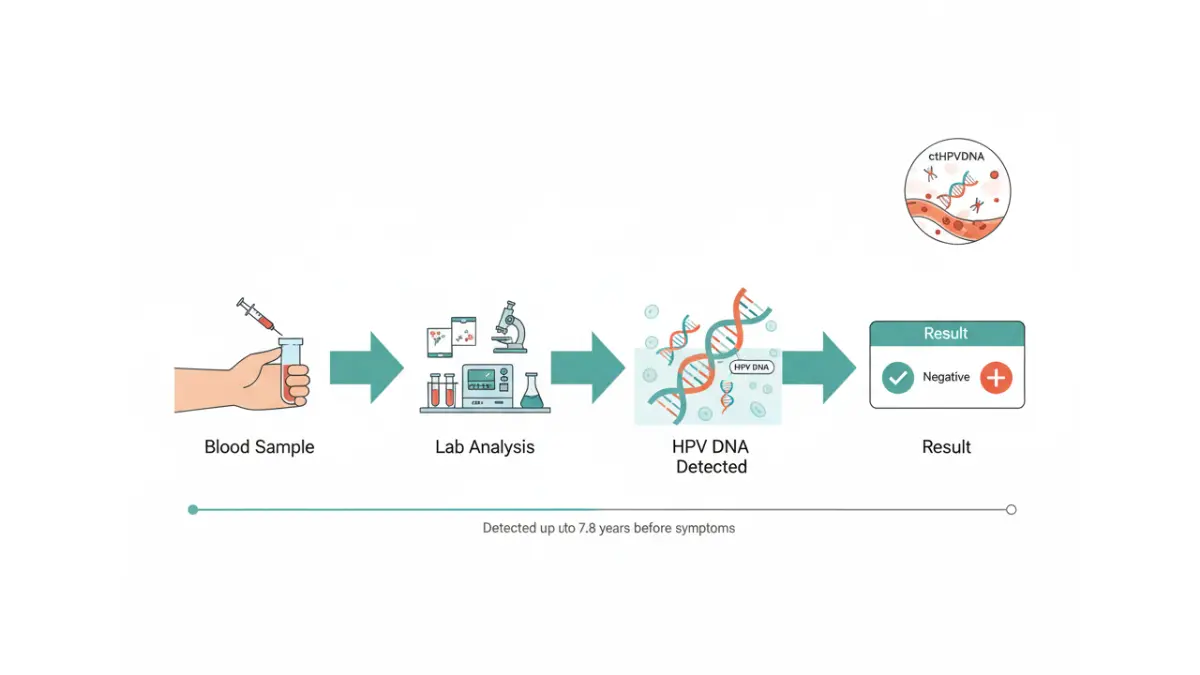
How Blood-Based HPV Screening Works
The breakthrough testing methodology detects HPV-related throat cancer through three validated approaches:
Circulating Tumor HPV DNA (ctHPVDNA): Blood samples undergo digital droplet PCR or whole genome sequencing to identify viral DNA fragments. This biomarker demonstrates higher reliability than mutation-based cancer detection methods.
HPV Serology Combined with ctDNA: Combining antibody testing for HPV-16 E6 protein with circulating DNA analysis improves detection accuracy to 96%. The National Institutes of Health confirmed this dual-marker approach reduces false negatives in high-risk populations.
Machine Learning Enhancement: Artificial intelligence algorithms analyze multiple biomarkers simultaneously—including viral load, antibody titers, and DNA methylation patterns—achieving detection rates approaching 96% sensitivity.
Who Should Pursue HPV Throat Cancer Screening?
High-Priority Candidates:
- Men aged 40-60 with multiple lifetime oral sex partners
- Known HPV-16 infection confirmed through previous testing
- Persistent oropharyngeal symptoms lasting 2+ weeks despite treatment
- Smokers with oral HPV exposure combining dual risk factors
- Family history of head and neck cancers
Screening Access Considerations:
HPV-DeepSeek and advanced ctHPVDNA screening currently operate through research protocols and early-access programs at academic medical centers. Mass General Brigham, Johns Hopkins, and select National Cancer Institute-designated comprehensive cancer centers offer testing to high-risk individuals.
The MedlinePlus HPV testing guide explains that while cervical HPV screening is routine, throat cancer HPV testing remains limited to symptomatic patients or high-risk screening candidates. Insurance coverage varies significantly—research protocol participation may provide free testing, while clinical screening typically costs $500-$1,500 out-of-pocket.
Comparing Detection Methods
Traditional diagnostic pathways identify oropharyngeal cancer only after symptoms emerge—typically when 60% of cases reach advanced stages. Blood-based HPV throat cancer screening fundamentally shifts this paradigm by detecting malignancy during the 7-15 year pre-symptomatic development window.
Patients diagnosed through early screening protocols demonstrate 95%+ five-year survival rates compared to 70-80% for symptomatically detected cases. Additionally, early detection enables de-escalated treatment approaches—reducing radiation doses by 50% and shortening treatment duration from six weeks to two weeks.
Commercial Bridge:
High-risk individuals should discuss HPV throat cancer screening eligibility with their oncologist or primary care provider. Early detection through blood-based testing may qualify patients for reduced-intensity treatment protocols that preserve quality of life while maintaining cure rates above 95%. For comprehensive health tracking during monitoring periods, maintaining optimal wellness metrics using tools like the BMI Calculator helps identify concerning changes that warrant additional evaluation.
Risk Factors, Causes & Who Gets HPV Throat Cancer
Understanding HPV Throat Cancer Risk: Men Face 6X Higher Rates
Primary Causes of HPV-Related Oropharyngeal Cancer
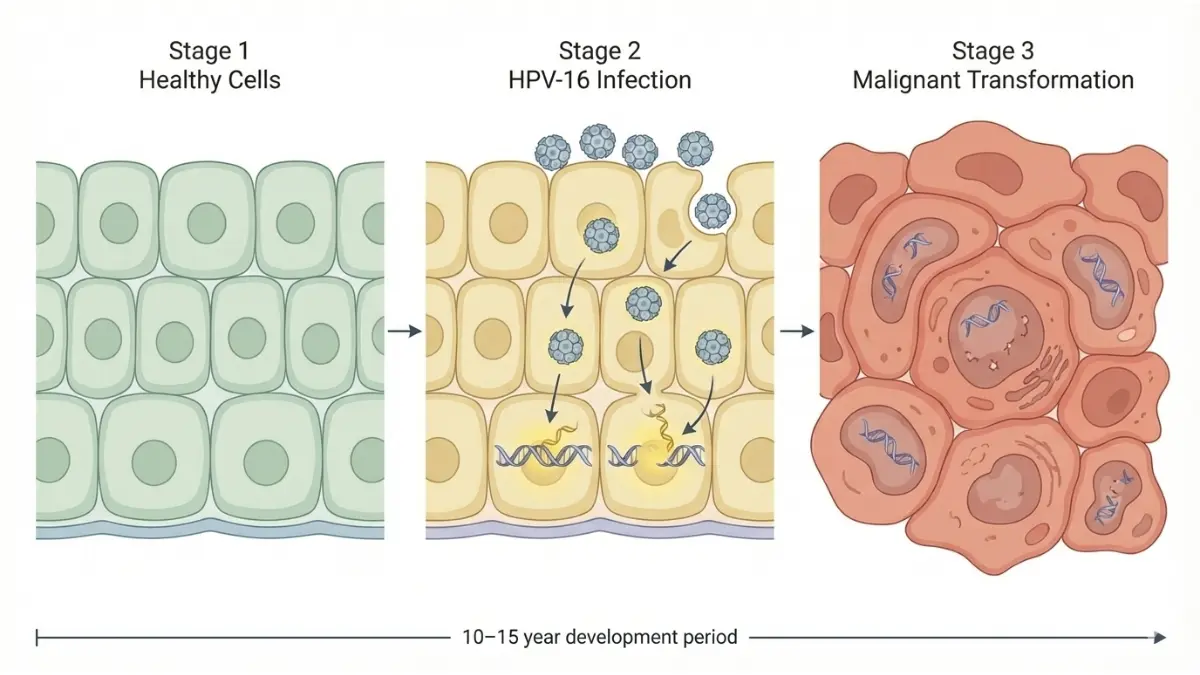
HPV-16 infection causes approximately 70% of all oropharyngeal cancers in the United States, transmitted primarily through oral-genital contact during sexual activity. The virus infects epithelial cells in the tonsils and base of tongue, producing oncoproteins E6 and E7 that disable cellular DNA repair mechanisms. Unlike cervical HPV infections that often clear within 2 years, oral HPV-16 can persist for decades before triggering malignant transformation.
Critical Transmission Pathways:
- Oral sex exposure represents the primary transmission route, with risk increasing proportionally to lifetime partner numbers
- Skin-to-skin contact during intimate activity transfers virus from genital areas to oral mucosa
- Persistent infection lasting 10+ years precedes cancer development in most cases
High-Risk Demographics
Men Face Disproportionate Burden:
Male incidence of HPV throat cancer exceeds female rates by 6:1, with approximately 11% of men carrying oral HPV-16 compared to 1.7% of women. Research published in the National Institutes of Health database reveals that HPV-16 E6 seropositive men aged 50-60 face 17-27% ten-year cancer risk compared to 4-6% for similarly aged women.
Peak Diagnosis Age:
- 40-60 years: Highest incidence window for HPV-positive cases
- 60+ years: Traditional tobacco-related throat cancer demographic
- Under 40: Rare but increasing among younger cohorts
HPV Throat Cancer Risk Factors
HPV-16 vs Other Cancer-Causing Strains
HPV-16 Dominance:
HPV-16 accounts for 90-95% of all HPV-related oropharyngeal cancers, demonstrating uniquely high oncogenic potential. While 13 HPV types possess carcinogenic properties, HPV-16 E6 oncoprotein exhibits particularly aggressive cellular transformation mechanisms. HPV-18 contributes 3-5% of cases, with other high-risk strains causing fewer than 2% collectively.
Seropositive Individuals:
The CDC reports that HPV-16 E6 antibody positivity indicates 34.8% prevalence among oropharyngeal cancer patients compared to 0.6% in general populations. This biomarker provides the strongest predictor of future cancer development currently available.
Non-Smokers Represent Growing Demographic
Unlike traditional throat cancer linked to heavy tobacco and alcohol use, 60% of HPV-positive oropharyngeal cancer patients report minimal or no smoking history. This demographic shift explains rising incidence among professional, health-conscious populations who would traditionally exhibit low cancer risk profiles.
White heterosexual males aged 45-60 represent the highest-incidence demographic, though Rutgers University research reveals that Black and Hispanic men experience 40-50% higher mortality rates despite lower incidence. These disparities reflect healthcare access inequities rather than biological differences.
Commercial Bridge:
Understanding your personal risk profile guides appropriate screening decisions. Men aged 40-60 with multiple lifetime sexual partners should discuss HPV throat cancer screening eligibility with healthcare providers. The Genetic Risk Assessment Tool helps evaluate combined risk factors including family history, HPV exposure, and lifestyle elements that influence cancer development probability.
Diagnosis, Staging, Treatment & Survival Rates
From Diagnosis to Treatment: What HPV-Positive Patients Need to Know
Diagnostic Process for HPV Throat Cancer
Step 1: Physical Examination
Otolaryngologists perform thorough head and neck examinations, palpating lymph nodes and inspecting oral cavity structures with indirect laryngoscopy. Suspicious lesions, persistent neck masses, or unexplained throat symptoms trigger comprehensive workups.
Step 2: Advanced Imaging
CT scans, MRI, and PET imaging define tumor extent and lymph node involvement. PET-CT demonstrates superior sensitivity for detecting occult metastases compared to conventional imaging alone.
Step 3: Tissue Biopsy
Fine needle aspiration or excisional biopsy provides tissue for histopathological analysis. Pathologists examine cellular architecture to confirm squamous cell carcinoma diagnosis.
Step 4: HPV Status Confirmation
p16 immunohistochemistry serves as the gold standard HPV surrogate marker, demonstrating 99% concordance with HPV DNA presence. Patients testing p16-positive receive distinct staging classifications and treatment protocols compared to p16-negative cases.
Step 5: Blood-Based Biomarkers
Emerging diagnostic pathways incorporate HPV-16 E6 serology and circulating tumor HPV DNA analysis, providing prognostic information beyond traditional staging.
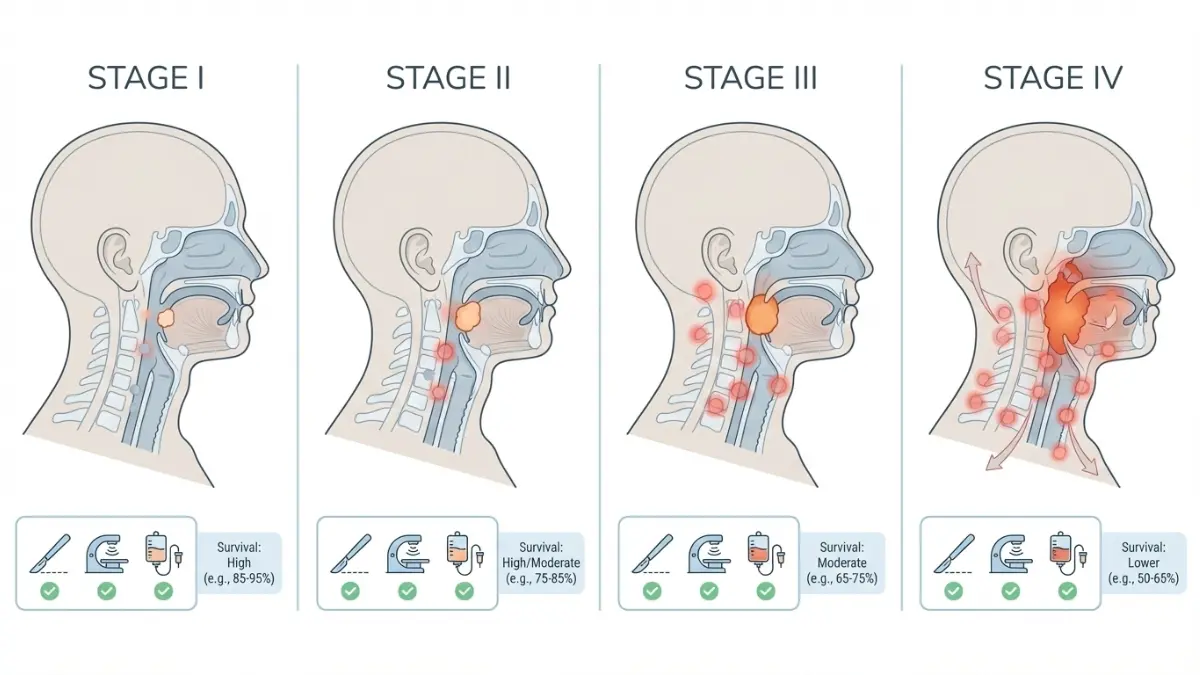
HPV Throat Cancer Stages
The American Joint Committee on Cancer established separate staging systems for HPV-positive versus HPV-negative oropharyngeal cancers in 2017, recognizing their fundamentally different biological behaviors.
Treatment Options: Latest Innovations
De-Escalated Therapy Revolution
Yale Medicine research demonstrates that reducing post-operative radiation doses achieves 95.3% overall survival and 90.6% progression-free survival at 54 months—matching or exceeding standard intensity outcomes while dramatically reducing side effects. This paradigm shift enables HPV-positive patients to maintain quality of life without compromising cure rates.
Transoral Robotic Surgery (TORS):
Minimally invasive surgical approaches access base of tongue and tonsil tumors through the mouth, eliminating external incisions. TORS patients experience faster recovery, preserved swallowing function, and reduced hospital stays compared to traditional open surgery.
Intensity-Modulated Radiation Therapy (IMRT):
Precision radiation targeting delivers therapeutic doses to tumors while sparing surrounding healthy tissues. IMRT reduces xerostomia (dry mouth), dysphagia, and other radiation-related toxicities by 40-60% compared to conventional techniques.
Concurrent Chemoradiation:
Combining cisplatin-based chemotherapy with radiation therapy represents the standard approach for locally advanced stage III-IV disease. This multimodal strategy achieves superior locoregional control compared to radiation alone.
Immunotherapy for Advanced Disease:
Checkpoint inhibitors targeting PD-1/PD-L1 pathways show promise for recurrent or metastatic HPV-positive oropharyngeal cancer resistant to conventional therapies. Clinical trials continue investigating optimal immunotherapy combinations and sequencing.
HPV Throat Cancer Survival Rates
Outstanding Prognosis Compared to HPV-Negative Disease:
Jefferson University research demonstrates three-year overall survival rates of 82.4% for HPV-positive patients versus 57.1% for HPV-negative cases—a 25% absolute survival advantage. This dramatic difference stems from HPV-positive tumors’ superior radiation sensitivity and more favorable metastatic patterns.
Five-Year Survival by Stage:
- Stage I HPV-Positive: 95-98% disease-free survival
- Stage II HPV-Positive: 90-95% overall survival
- Stage III HPV-Positive: 85-90% overall survival
- Stage IV HPV-Positive (non-metastatic): 75-85% overall survival
- Stage IV HPV-Positive (metastatic): 70-80% overall survival
HPV-Negative Comparison:
- All Stages Combined HPV-Negative: 55-65% five-year survival
- Stage III-IV HPV-Negative: 40-50% five-year survival
Treatment Duration and Recovery
Standard Treatment Timelines:
- Surgery alone: 2-3 hour procedure, 1-2 week recovery
- Radiation therapy: 6-7 weeks daily treatment (standard)
- De-escalated radiation: 2-3 weeks reduced-dose treatment
- Concurrent chemoradiation: 6-7 weeks combined therapy
Quality of Life Preservation:
De-escalated protocols reduce severe side effects by 50% while maintaining cure rates above 95%. Patients treated with reduced-intensity approaches experience less difficulty swallowing, better taste preservation, and superior long-term functional outcomes.
Commercial Bridge:
HPV throat cancer treatment costs vary significantly based on staging and modality selection, ranging from $50,000-$150,000 for complete treatment courses. Most insurance plans cover 80-90% of medically necessary cancer care, though out-of-pocket maximums apply. Maintaining optimal health during and after treatment requires attention to nutrition—use the Protein Intake Calculator to ensure adequate protein consumption supporting tissue healing and immune function recovery.
Prevention, Vaccination & Taking Action Today
Prevention Strategies & Accessing HPV Throat Cancer Care
HPV Vaccine: Your Most Powerful Defense
Gardasil-9 prevents over 90% of HPV-caused cancers, including oropharyngeal malignancies linked to HPV-16 and HPV-18 strains. The vaccine demonstrates 96-100% efficacy when administered before viral exposure, making pre-adolescent vaccination the optimal prevention strategy.
Vaccination Recommendations:
- Ages 11-12 years: CDC-recommended primary vaccination window (2-dose series)
- Ages 9-26 years: Catch-up vaccination for previously unvaccinated individuals
- Ages 27-45 years: Shared clinical decision-making with healthcare providers
- Post-exposure benefit: Limited efficacy after sexual activity initiation
The vaccine protects against HPV types 6, 11, 16, 18, 31, 33, 45, 52, and 58—collectively responsible for 90% of HPV-related cancers. Harvard School of Public Health research confirms maximum cost-effectiveness occurs with pre-adolescent vaccination, though adults aged 27-45 may benefit from individualized assessment.
HPV Throat Cancer Prevention Checklist
- Get vaccinated if under age 45 and previously unvaccinated
- Practice safer sex using barrier methods during oral-genital contact
- Avoid tobacco products which compound HPV infection risks
- Limit alcohol consumption to reduce mucosal inflammation
- Schedule annual dental exams for oral cavity screening
- Self-examine monthly for persistent mouth or throat changes
- Seek early evaluation for symptoms lasting 2+ weeks
Taking Action Today
Immediate Next Steps:
- Assess Personal Risk: Complete the Genetic Risk Assessment Tool evaluating combined risk factors including age, sexual history, vaccination status, and tobacco use.
- Document Symptoms: If experiencing concerning throat or neck symptoms, track duration and severity before medical appointments using the Symptom Checker for preliminary evaluation.
- Schedule Screening: High-risk individuals aged 40-60 should discuss HPV throat cancer screening eligibility with oncologists or primary care providers, especially if experiencing persistent symptoms.
- Get Vaccinated: Contact healthcare providers about HPV vaccination if under age 45 and previously unvaccinated—protection remains possible even after sexual activity initiation.
- Adopt Preventive Behaviors: Implement tobacco cessation, moderate alcohol intake, maintain oral hygiene, and practice safer sexual behaviors to minimize cumulative risk exposure.
Commercial Bridge:
Early detection through symptom recognition and appropriate screening saves lives while reducing treatment intensity by 50%+ compared to late-stage diagnosis. For comprehensive health guidance and additional cancer prevention strategies, explore our complete health resources library covering screening recommendations, risk reduction techniques, and evidence-based wellness approaches.
Medical Disclaimer:
This article is for educational purposes and does not constitute medical advice. HPV throat cancer diagnosis, screening, and treatment require professional medical evaluation. Consult qualified healthcare providers for personalized assessment, diagnostic testing, and treatment planning. Information presented reflects current research as of January 2026 and may evolve as new evidence emerges.
Frequently Asked Questions About HPV Throat Cancer
1. Can HPV throat cancer be detected early?
Yes. New blood tests like HPV-DeepSeek can detect cancer 7-10 years before symptoms appear, with 96% accuracy.
2. What is the survival rate for HPV-positive throat cancer?
HPV-positive throat cancer has 85-90% five-year survival rates, significantly higher than HPV-negative cases at 60-70%.
3. How does HPV cause throat cancer?
HPV-16 infects throat cells through oral-genital contact, producing oncoproteins that disable DNA repair mechanisms, eventually causing cancer after 10-15 years.
4. Who is most at risk for HPV throat cancer?
Men aged 40-60 with multiple oral sex partners face highest risk—6 times more likely than women to develop HPV throat cancer.
5. Does the HPV vaccine prevent throat cancer?
Yes. Gardasil-9 prevents over 90% of HPV-caused cancers, including throat cancer, when administered before viral exposure.
6. What are the first signs of HPV throat cancer?
Painless neck lumps, persistent sore throat lasting 2+ weeks, difficulty swallowing, and unexplained ear pain are earliest warning signs.
7. How is HPV throat cancer different from tobacco-related throat cancer?
HPV-positive cases affect younger non-smokers, respond better to treatment, and have 25% higher survival rates than tobacco-related throat cancer.
8. Can you get throat cancer if you’ve been vaccinated?
Vaccination reduces risk by 90%+, but doesn’t eliminate it entirely. Post-exposure vaccination offers limited protection.
9. How much does HPV throat cancer treatment cost?
Treatment ranges $50,000-$150,000 depending on stage and approach, with insurance typically covering 80-90% of medically necessary care.
10. Is HPV throat cancer curable?
Yes. Early-stage HPV-positive throat cancer achieves 95-98% cure rates with modern de-escalated treatment protocols.
11. Should I get screened for HPV throat cancer?
Screening is recommended for high-risk individuals: men 40-60 with multiple sexual partners, known HPV-16 infection, or persistent throat symptoms lasting 2+ weeks.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.











