On This Page – Quick Medical Summary
When Jessica, 31, finished her second course of BV antibiotics in six months, she thought something was wrong with her. Her OB-GYN finally explained the truth: the antibiotic had worked — but it hadn’t fixed the underlying reason BV kept returning.
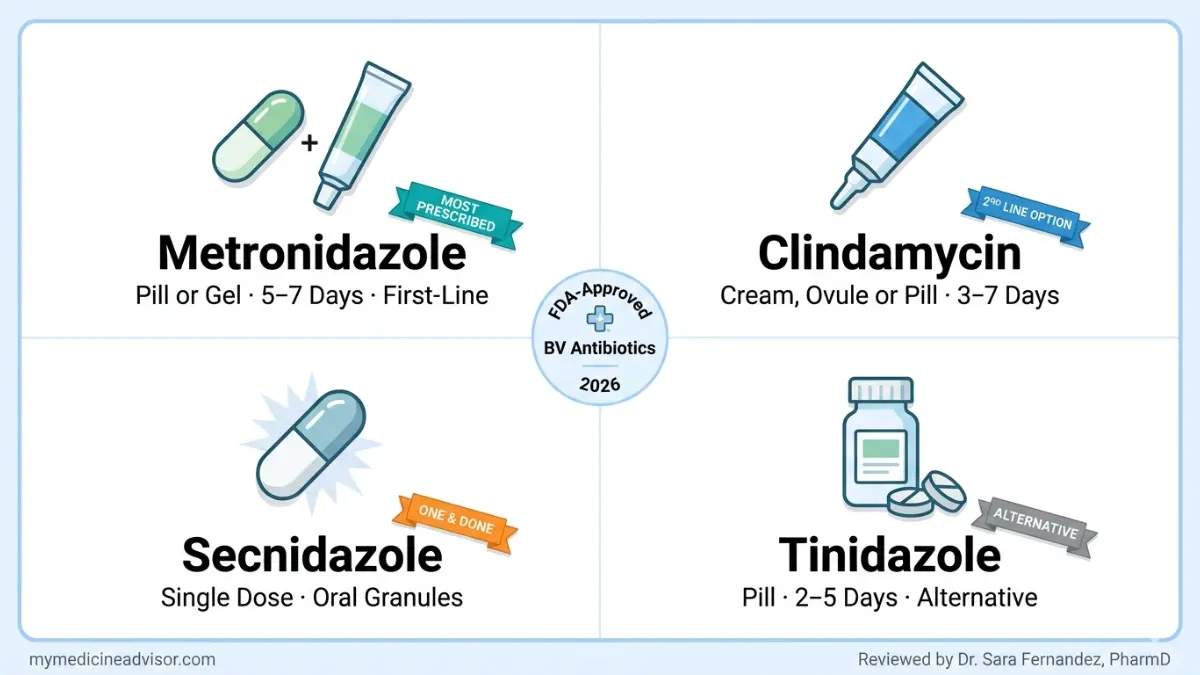
Here is the direct answer: The first-line BV antibiotics doctors prescribe are metronidazole and clindamycin, available as pills, vaginal gels, and creams. A single-dose option — secnidazole — is also FDA-approved. Most women clear the infection within 5–7 days. However, according to the CDC STI Treatment Guidelines, up to 80% of women experience a BV recurrence within 12 months of completing antibiotic treatment.
This guide explains exactly what doctors prescribe, why some antibiotics stop working, and what the 2026 evidence says about finally breaking the BV cycle.
The 4 FDA-Approved BV Antibiotics Doctors Use First
Doctors in the US have four main BV antibiotics to choose from — all FDA-approved, all evidence-backed. The choice depends on your medical history, symptoms, pregnancy status, and whether this is your first infection or a recurring one.
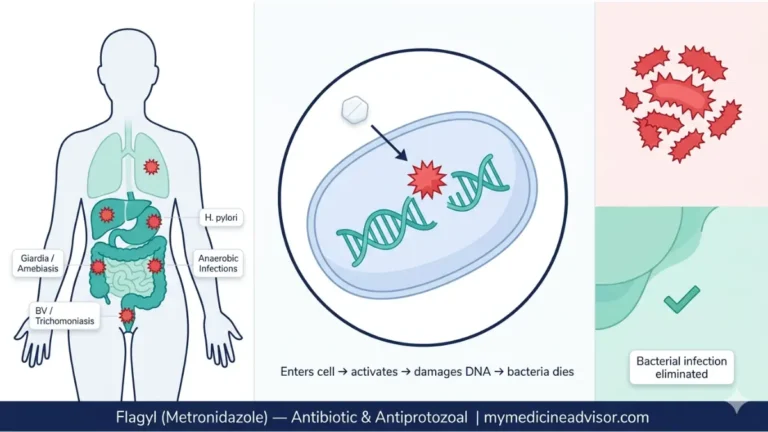
Metronidazole (Flagyl) — The #1 First-Line BV Antibiotic
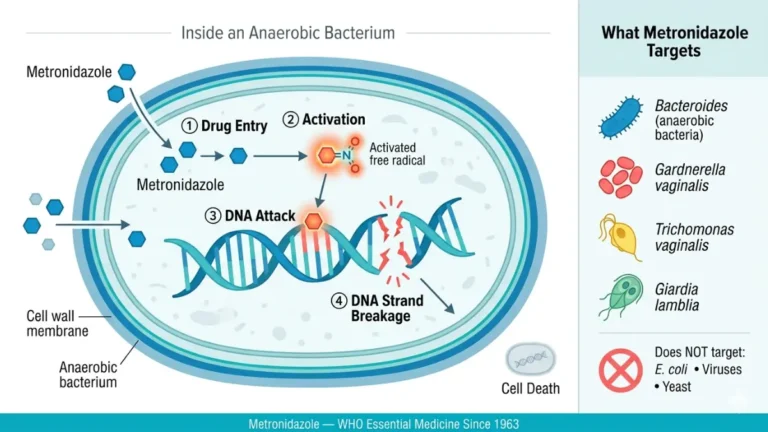
Metronidazole is the most commonly prescribed antibiotic for bacterial vaginosis in the United States. It kills anaerobic bacteria — the type that overgrow during BV — while largely sparing the protective Lactobacillus strains.
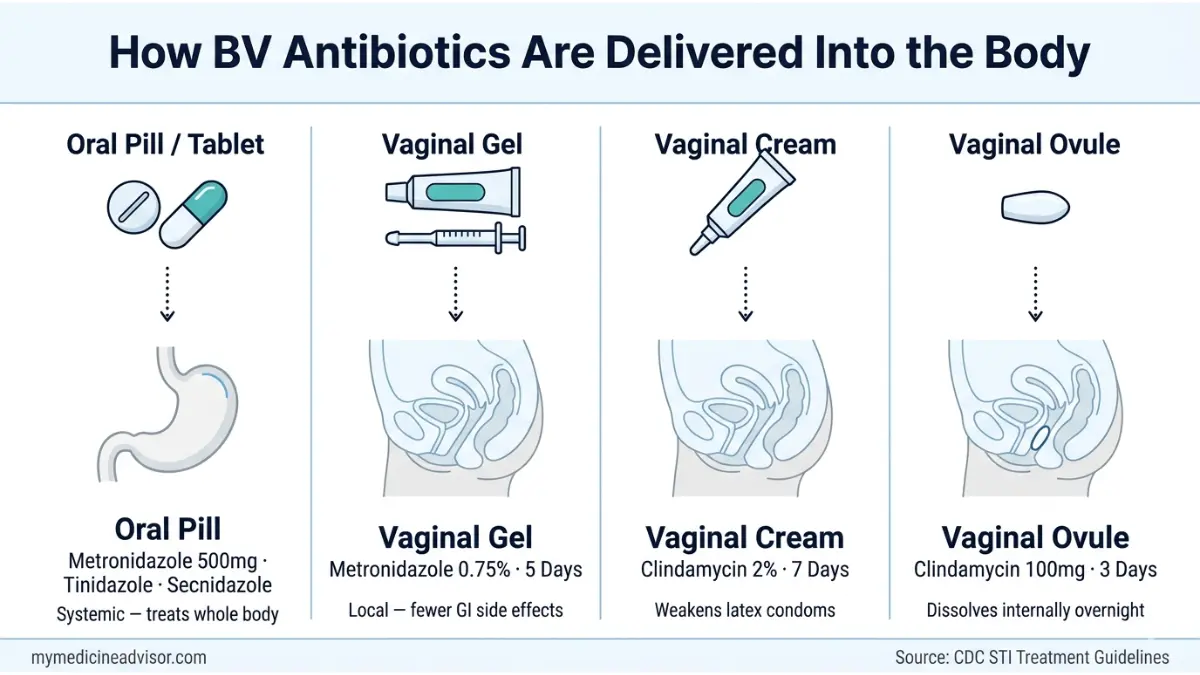
- Pill form: 500 mg orally, twice daily for 7 days
- Gel form: 0.75% vaginal gel, once daily for 5 days
- Key warning: Do not consume alcohol during treatment or for 24–48 hours after. The combination causes severe nausea, vomiting, and flushing.
If you’re unsure whether your symptoms are BV or another infection, use our Symptom Checker for an initial self-assessment before your appointment.
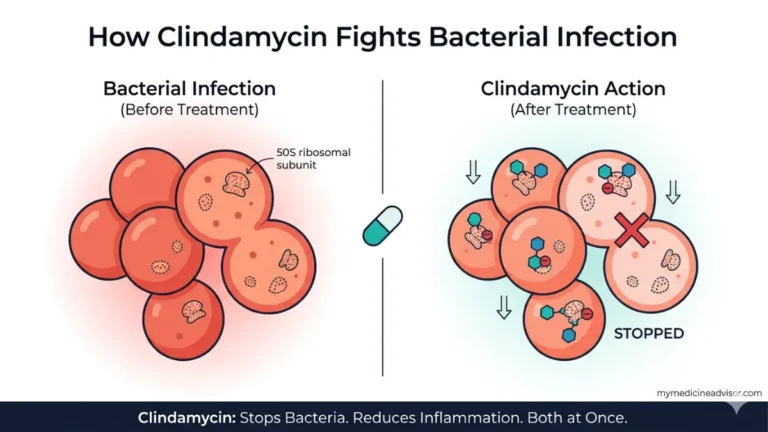
Clindamycin (Cleocin) — The Second-Choice BV Antibiotic
Clindamycin is prescribed when metronidazole has failed, caused intolerable side effects, or when a patient is in the second half of pregnancy.
- Vaginal cream: 2%, inserted at bedtime for 7 days
- Vaginal ovule: 100 mg, once nightly for 3 days
- Oral pill: 300 mg, twice daily for 7 days (less common)
- Critical safety point: Clindamycin cream and ovules weaken latex condoms and diaphragms for up to 5 days after the last dose. This is one of the most under-communicated warnings in women’s health.
For a deeper look at how clindamycin works at a pharmacological level, our guide on metronidazole — what doctors don’t tell you explores related antibiotic mechanisms in detail.
Secnidazole (Solosec) — The Single-Dose BV Antibiotic
Secnidazole was FDA-approved in 2017 and remains the only single-dose oral BV treatment available. A woman sprinkles the 2-gram granule packet onto soft food — applesauce, yogurt — and takes it once.
- Cure rate: Comparable to 7-day metronidazole in clinical trials
- Advantage: One dose eliminates the compliance problem (no forgetting doses mid-course)
- Warning: Avoid alcohol; not recommended during pregnancy
Tinidazole (Tindamax) — When Others Don’t Work
Tinidazole is a nitroimidazole antibiotic — in the same class as metronidazole — but with a longer half-life and slightly different bacterial activity profile.
- Dose options: 2g orally once daily for 2 days, or 1g once daily for 5 days
- Alcohol warning: Avoid for 72 hours after the last dose
BV Antibiotic Comparison Table
| Antibiotic | Form Available | Duration | ~1-Month Cure Rate | Alcohol Restriction | Pregnancy Safe? |
|---|---|---|---|---|---|
| Metronidazole | Pill / Vaginal gel | 5–7 days | 70–80% | 24–48 hrs after | ✅ Yes (all trimesters) |
| Clindamycin | Cream / Ovule / Pill | 3–7 days | 70–80% | None | ⚠️ Caution (2nd half) |
| Secnidazole | Single oral dose | 1 dose | ~70% | 24 hrs after | ❌ Not recommended |
| Tinidazole | Pill | 2–5 days | 37–65% | 72 hrs after | ❌ Not recommended |
What This Means For You: If this is your first BV episode with no complicating factors, your doctor will almost certainly start with metronidazole. If you have a penicillin sensitivity, are in late pregnancy, or have had metronidazole fail before, expect a different conversation.
Metronidazole vs Clindamycin — Which BV Antibiotic Is Right for Your Case?
Both are equally effective as first-line BV medication — clinical trials show over 90% of women are symptom-free at 1–2 weeks regardless of which drug they use, according to InformedHealth.org via NCBI. But the right choice depends on your specific situation.
When Doctors Choose Metronidazole First
- First BV episode with no history of treatment failure
- Not currently breastfeeding (metronidazole passes into breast milk at low levels; most providers consider it acceptable, but some prefer clindamycin)
- Patient can reliably complete a 7-day course
- Pill vs Gel: The vaginal gel causes fewer gastrointestinal side effects (nausea, metallic taste) than the oral pill. For women with sensitive stomachs, the gel is the smarter first choice.
When Doctors Switch to Clindamycin
- Metronidazole intolerance or previous allergic reaction
- Recurrent BV where metronidazole has already failed
- Second half of pregnancy (clindamycin cream is preferred; secnidazole and tinidazole are contraindicated)
- Specific bacterial profiles where anaerobic coverage of clindamycin is advantageous
The condom warning no competitor mentions clearly: Clindamycin cream contains an oil base that degrades latex. If you rely on condoms or a diaphragm for contraception, you need a backup method for at least 5 days after completing clindamycin treatment.
Side Effect Comparison at a Glance
| Side Effect | Metronidazole | Clindamycin |
|---|---|---|
| Metallic taste | Common | Rare |
| Nausea / GI upset | Common (pill) | Mild |
| Yeast overgrowth | Possible | More common |
| Alcohol interaction | Yes — severe | No |
| Condom breakdown | No | Yes (cream/ovule) |
What This Means For You: If you’ve tried one and it stopped working, the answer isn’t more of the same drug — it’s a switch. Ask your provider specifically about the secnidazole single-dose option if compliance has been your challenge.
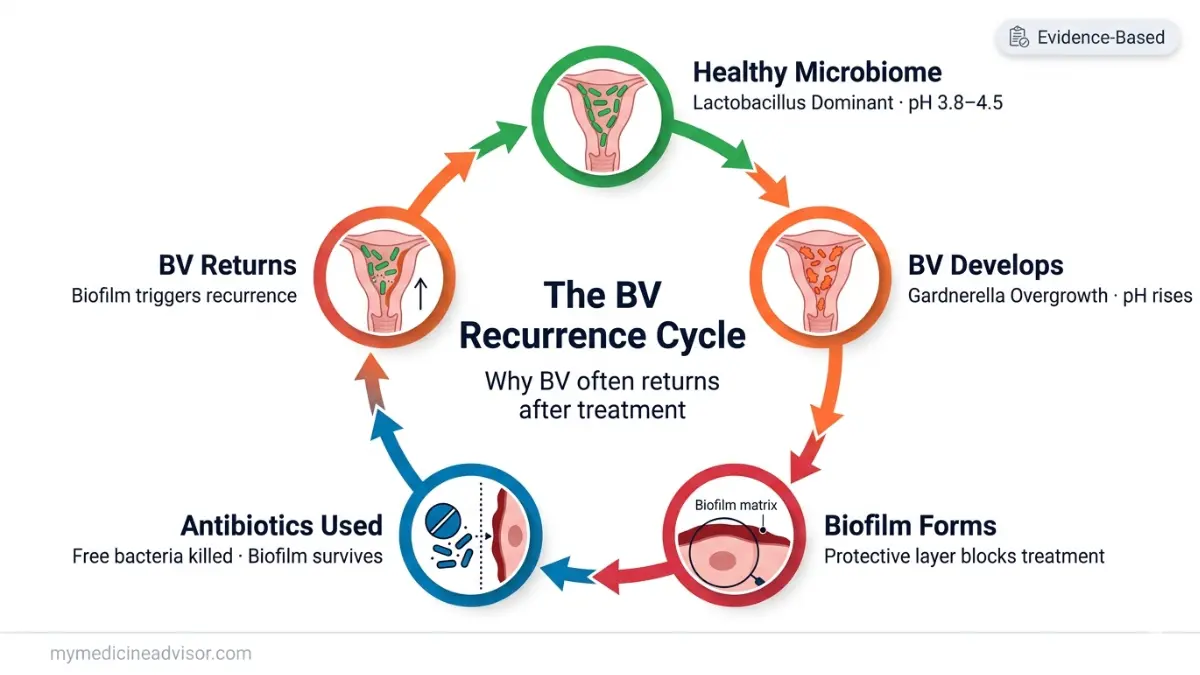
Why BV Antibiotics Fail — The Biofilm Truth No Competitor Explains
This is the most important section for the estimated 80% of women who get BV again within a year. The reason isn’t that the antibiotic was too weak. It’s biology — and it’s finally being explained clearly in 2026 research.
What Is a Vaginal Biofilm and Why Antibiotics Can’t Break It
Gardnerella vaginalis — the primary bacteria implicated in BV — builds a dense, protective polymicrobial biofilm on vaginal epithelial cells. Think of it as a bacterial fortress made of a sticky protein matrix.
Standard BV antibiotics kill planktonic bacteria — the free-floating cells moving through vaginal fluid. But they cannot fully penetrate the biofilm structure. After treatment ends, bacteria embedded in the biofilm begin repopulating — and BV returns.
A landmark review published in PMC/NIH confirmed that persistent polymicrobial biofilm is more common in women with recurrent BV than in those with a single episode, and that biofilm persists even after clinically successful antibiotic treatment.
Antibiotic Resistance — A Growing Problem in 2026
Resistance is emerging, and it’s underreported in consumer health content.
- One study found that the majority of tested Gardnerella vaginalis strains showed resistance to both metronidazole and clindamycin
- The WHO has flagged nitroimidazole overuse (metronidazole, tinidazole) as a contributor to antimicrobial resistance globally
- Repeated short-course antibiotic treatment may actually select for more resistant bacterial strains in some women
Understanding how antibiotics interact with bacterial resistance is part of why our drug interactions guide is an important companion resource for anyone on repeated antibiotic courses.
Why Lactobacillus Doesn’t Come Back After Treatment
A healthy vaginal microbiome is dominated by Lactobacillus crispatus — a hydrogen peroxide-producing species that keeps vaginal pH low (3.8–4.5) and hostile to BV-causing bacteria.
After antibiotics clear BV, L. crispatus often fails to recolonize the vagina naturally. The absence of this protective species creates the window for BV to return — usually within weeks to months.
What This Means For You: If you’ve had BV more than twice, you’re not doing anything wrong. The antibiotic worked — but the microbiome didn’t reset. That’s the gap 2026 research is now focused on fixing.
BV Antibiotics During Pregnancy — What’s Safe and What Isn’t
BV during pregnancy isn’t just uncomfortable — it’s a clinical priority. The CDC STI Treatment Guidelines are unambiguous: all symptomatic pregnant women with BV should be treated, regardless of trimester.
Why Treating BV in Pregnancy Is Non-Negotiable
Untreated BV in pregnancy is associated with:
- 2× increased risk of preterm birth
- Low birth weight
- Premature rupture of membranes
- Chorioamnionitis (infection of the amniotic sac)
- Late miscarriage risk (weeks 13–24)
If you’re currently pregnant and tracking your timeline alongside treatment, our Pregnancy Due Date Calculator can help you organize your prenatal care schedule.
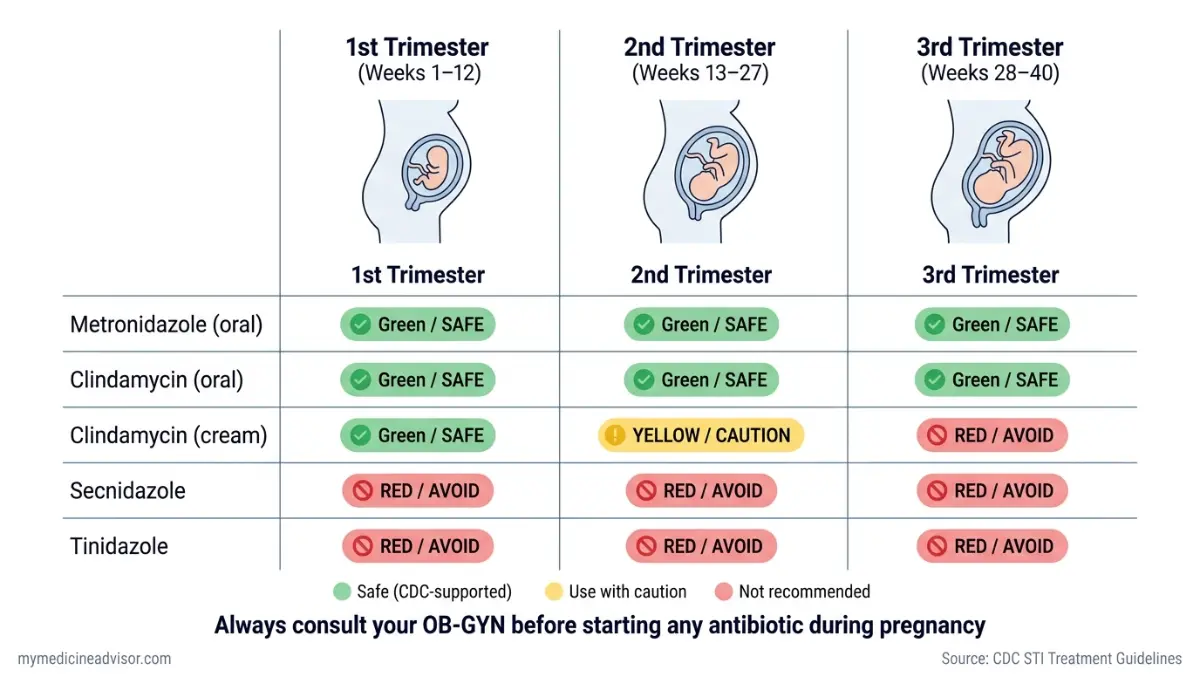
Trimester-by-Trimester Safety Matrix
| Antibiotic | 1st Trimester | 2nd Trimester | 3rd Trimester |
|---|---|---|---|
| Metronidazole (oral) | ✅ Safe | ✅ Safe | ✅ Safe |
| Metronidazole (gel) | ✅ Safe | ✅ Safe | ✅ Safe |
| Clindamycin (oral) | ✅ Safe | ✅ Safe | ✅ Safe |
| Clindamycin (cream) | ✅ Safe | ⚠️ Use with caution | ❌ Not recommended |
| Secnidazole | ❌ Avoid | ❌ Avoid | ❌ Avoid |
| Tinidazole | ❌ Avoid | ❌ Avoid | ❌ Avoid |
What the 2026 CDC Guidance Says
The CDC recommends oral metronidazole as the preferred treatment in pregnancy — not the gel — because systemic treatment is more likely to address the upper reproductive tract where BV-related complications originate.
Women who are pregnant and want to monitor fetal development in parallel with their treatment course can also use our Fetal Growth Percentile Calculator to track week-by-week progress.
What This Means For You: If you’re pregnant and have BV symptoms — discharge, odor, irritation — contact your OB-GYN immediately. This is not a “wait and see” situation. Treatment is safe, and the risk of not treating is far higher than the risk of the antibiotic.
After Antibiotics — How to Stop BV From Coming Back
The antibiotic course ends. Symptoms resolve. Then, weeks or months later — BV is back. For millions of American women, this is the maddening reality of recurrent bacterial vaginosis. Here is what the evidence actually supports for breaking the cycle.
The Probiotic + Antibiotic Stack Doctors Now Recommend
A 2022 meta-analysis found that probiotic supplementation alongside — and after — antibiotic treatment meaningfully reduced BV recurrence rates compared to antibiotics alone.
The strains that matter:
- Lactobacillus crispatus (most clinically studied for BV prevention)
- Lactobacillus rhamnosus GR-1
- Lactobacillus reuteri RC-14
Timing protocol:
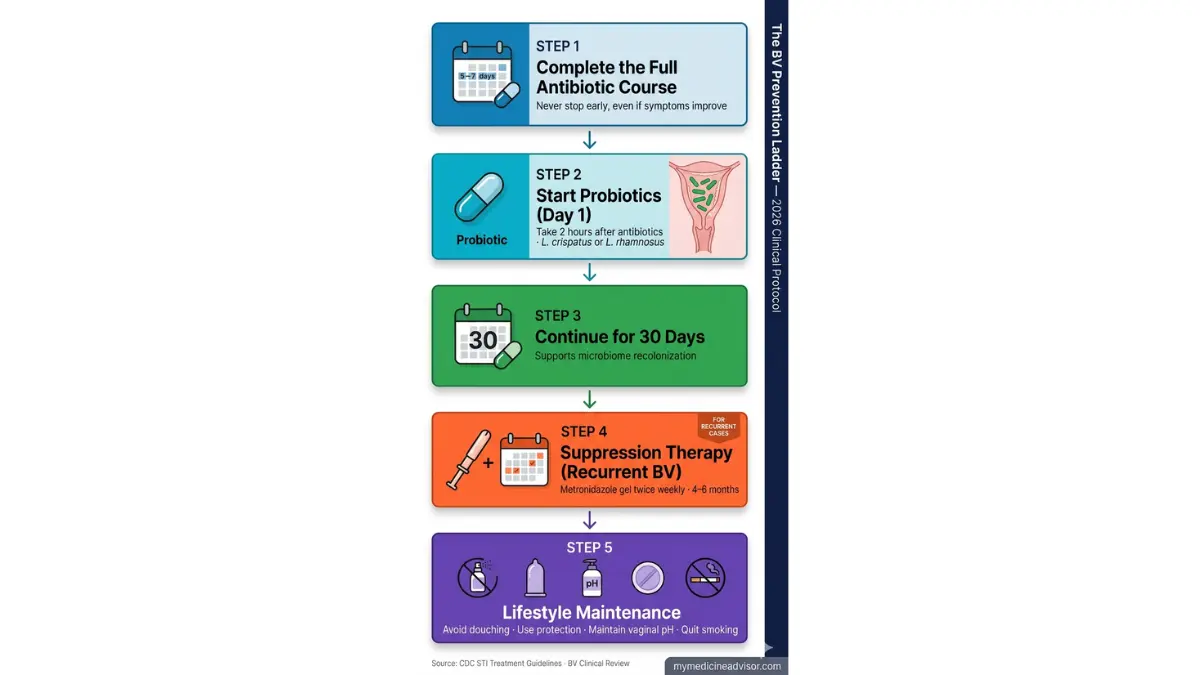
- Take probiotics 2 hours after each antibiotic dose (not simultaneously)
- Continue for at least 30 days after completing the antibiotic course
- Choose a refrigerated, multi-strain probiotic with CFU counts above 5 billion
The Recurrent BV Suppression Protocol
If you’ve had BV four or more times in a year, your doctor can prescribe a long-term suppression protocol — not just another short course.
CDC-supported options for recurrent BV:
- Metronidazole 0.75% vaginal gel, twice weekly for 4–6 months
- Boric acid vaginal suppositories, 600mg daily for 14–21 days as an adjunct (not standalone) — shown to improve cure rates in metronidazole-resistant cases
- Combination therapy: Metronidazole course followed by boric acid followed by long-term probiotic maintenance
For women with recurrent BV who are also managing PCOS or hormonal imbalance — conditions that affect vaginal microbiome health — our PCOS symptoms guide provides important context on the hormonal-microbiome connection.
5 Evidence-Backed Lifestyle Changes That Reduce BV Recurrence
- Stop douching — it destroys vaginal pH and the protective Lactobacillus layer. No exceptions.
- Use condoms consistently — particularly with new or multiple partners; BV-associated bacteria can be transmitted sexually
- Switch to pH-balanced intimate wash — ordinary soap (pH 9–10) disrupts the vaginal environment
- Consider hormonal contraception — CDC data indicates oral contraceptives may lower BV risk by stabilizing vaginal hormone levels
- Quit smoking — smokers show significantly altered vaginal microbiomes with lower Lactobacillus dominance
What This Means For You: If your BV keeps returning, a single antibiotic course is not your long-term solution. Ask your doctor specifically: “Am I a candidate for suppression therapy?” That question could save you years of recurring infections.
Emerging BV Treatments in 2026 — Beyond Standard Antibiotics
The standard BV antibiotic regimens have barely changed in 20 years. But 2026 marks a pivotal moment: for the first time, genuinely new treatment categories are moving through clinical trials with promising results.
Vaginal Microbiome Transplantation (VMT) — The Frontier Therapy
VMT is exactly what it sounds like: donor Lactobacillus crispatus — from a woman with a proven healthy vaginal microbiome — is transferred to a recipient with recurrent BV.
- Phase I/II clinical trials are actively recruiting in the US and UK
- Early data shows durable microbiome restoration in women who have failed multiple antibiotic courses
- Who may qualify: Women with recurrent BV unresponsive to three or more antibiotic courses
- Trials can be found at ClinicalTrials.gov — a live, searchable registry of all active studies
This is still experimental — not a clinical standard in 2026 — but for the most treatment-resistant cases, it represents genuine hope.
LACTIN-V, pH Modulators, and Non-Antibiotic BV Treatments
- LACTIN-V (L. crispatus CTV-05): An FDA fast-tracked live biotherapeutic product. Phase III clinical trials are ongoing. It delivers a specific, high-potency strain of L. crispatus vaginally to prevent recurrence after metronidazole treatment.
- Dequalinium chloride (Fluomizin): Already approved and used as a first-line BV treatment in multiple European countries. An antiseptic — not an antibiotic — that disrupts Gardnerella biofilm more effectively than metronidazole in some studies.
- Sucrose vaginal gel: Promotes selective growth of beneficial Lactobacillus species by modulating vaginal pH; small but promising clinical data.
The science of vaginal microbiome restoration connects to broader patterns in gut and immune health. Our guide on 7 gut bacteria and their effects on weight, mood, and immunity explores the wider role of microbiome balance in overall health.
What This Means For You: You don’t have to accept that recurrent BV is just “how it is.” The treatment landscape is changing fast. Asking your gynecologist about LACTIN-V trials or dequalinium chloride puts you ahead of 99% of patients walking into a clinic today.
Frequently Asked Questions — BV Antibiotics
1. What is the fastest-working BV antibiotic?
Metronidazole typically produces noticeable symptom improvement within 2–3 days. Secnidazole’s single-dose format is the most convenient, but symptom resolution timelines are similar across all four FDA-approved options.
2. How long does it take for BV antibiotics to work?
Most women notice improvement within 2–3 days and full symptom resolution by day 5–7. Even if symptoms clear early, always complete the full antibiotic course to reduce recurrence risk.
3. Can I get BV antibiotics without seeing a doctor in person?
Yes — in most US states, telehealth platforms can prescribe metronidazole or clindamycin after a brief online consultation. You’ll typically need to describe symptoms; in-person diagnosis using Amsel criteria or a Nugent score remains the gold standard.
4. What happens if BV doesn’t respond to antibiotics?
Your doctor will likely switch antibiotic class (e.g., from metronidazole to clindamycin), consider boric acid adjunct therapy, test for antibiotic-resistant strains, or refer you for a suppression protocol. Persistent BV unresponsive to two antibiotic courses warrants specialist evaluation.
5. Is metronidazole or clindamycin better for BV?
Neither is definitively superior — cure rates at one month are equivalent (70–80%) per the NIH evidence review. The choice is individualized based on pregnancy status, breastfeeding, tolerance, and prior treatment history.
6. Can BV come back after finishing the full antibiotic course?
Yes — and this is the norm, not the exception. Up to 80% of women experience recurrence within 12 months even after completing treatment correctly. This is due to biofilm persistence and failure of Lactobacillus recolonization, not treatment failure.
7. Are BV antibiotics safe while breastfeeding?
Metronidazole passes into breast milk at low levels. Most providers consider it acceptable during breastfeeding, but some recommend clindamycin as an alternative to minimize infant exposure. Always discuss with your provider.
8. Do I need to avoid alcohol with all BV antibiotics?
Not all — but most. Metronidazole, secnidazole, and tinidazole all require alcohol avoidance (24–72 hours depending on the drug). Clindamycin has no alcohol interaction. This is one of the most frequently misunderstood points in BV treatment.
9. Should my partner be treated for BV too?
Current evidence, including CDC guidelines, does not recommend treating male sex partners — studies show it does not reduce BV recurrence rates. Female partners in same-sex relationships should discuss concurrent treatment with their provider, as BV shows high concordance among female partners.
10. What is the single-dose antibiotic for bacterial vaginosis?
Secnidazole (Solosec) — FDA-approved in 2017 — is the only single-dose oral treatment for BV. The 2-gram granule packet is sprinkled onto soft food and consumed once. It requires no multi-day compliance.
11. What do doctors prescribe for recurring BV that keeps coming back?
For recurrent BV (4+ episodes/year), doctors typically prescribe long-term suppression with metronidazole vaginal gel (twice weekly for 4–6 months), often combined with boric acid suppositories and a post-treatment probiotic protocol. Some patients are candidates for newer approaches including LACTIN-V or VMT trials.
Sources:
- CDC STI Treatment Guidelines — Bacterial Vaginosis
- NIH/NCBI — Which treatments are effective for bacterial vaginosis?
- PMC — Bacterial vaginosis: a review of approaches to treatment and prevention
- ClinicalTrials.gov — Active BV Microbiome Trials
Related Reading on mymedicineadvisor.com:
- Metronidazole — What Doctors Don’t Tell You
- Drug Interactions Guide
- PCOS Symptoms in Women
- 7 Gut Bacteria and Their Effects on Your Body
- STI Test Results Decoded
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.