On This Page – Quick Medical Summary
James, 58, had been managing his blood pressure with metoprolol for three months when the sleepless nights began. He’d fall asleep fine, then jolt awake at 2 a.m., heart racing, unable to return to sleep. His cardiologist said his heart was in perfect shape. His primary care physician suggested stress. Nobody thought to check his pill bottle — until a sleep specialist finally did.
Direct Answer: Medications that cause insomnia include SSRIs/SNRIs, beta-blockers, corticosteroids, ADHD stimulants, decongestants, ACE inhibitors, thyroid hormone, cholinesterase inhibitors, nicotine replacement therapy, statins, NSAIDs, and diuretics. According to the National Heart, Lung, and Blood Institute (NHLBI), insomnia is one of the most common reported sleep problems in the U.S., and certain medications are a frequently overlooked cause. This guide breaks down every major drug class, explains exactly why it disrupts sleep, and tells you what to do about it.
⚠️ Disclaimer: This article is for educational purposes only and does not constitute medical advice. Never stop, switch, or adjust any prescription medication without consulting your healthcare provider.
What Is Drug-Induced Insomnia — And How Does It Steal Your Sleep?
Drug-induced insomnia is difficulty falling or staying asleep that is directly caused by a medication’s pharmacological action, side effects, or withdrawal. It is distinct from lifestyle insomnia and can range from short-term disruption to chronic sleep deprivation that persists as long as the medication is taken.
According to the U.S. Department of Health and Human Services, over 17% of American adults take at least one medication that lists sleep disturbances as a side effect — yet this connection is routinely missed in clinical consultations.
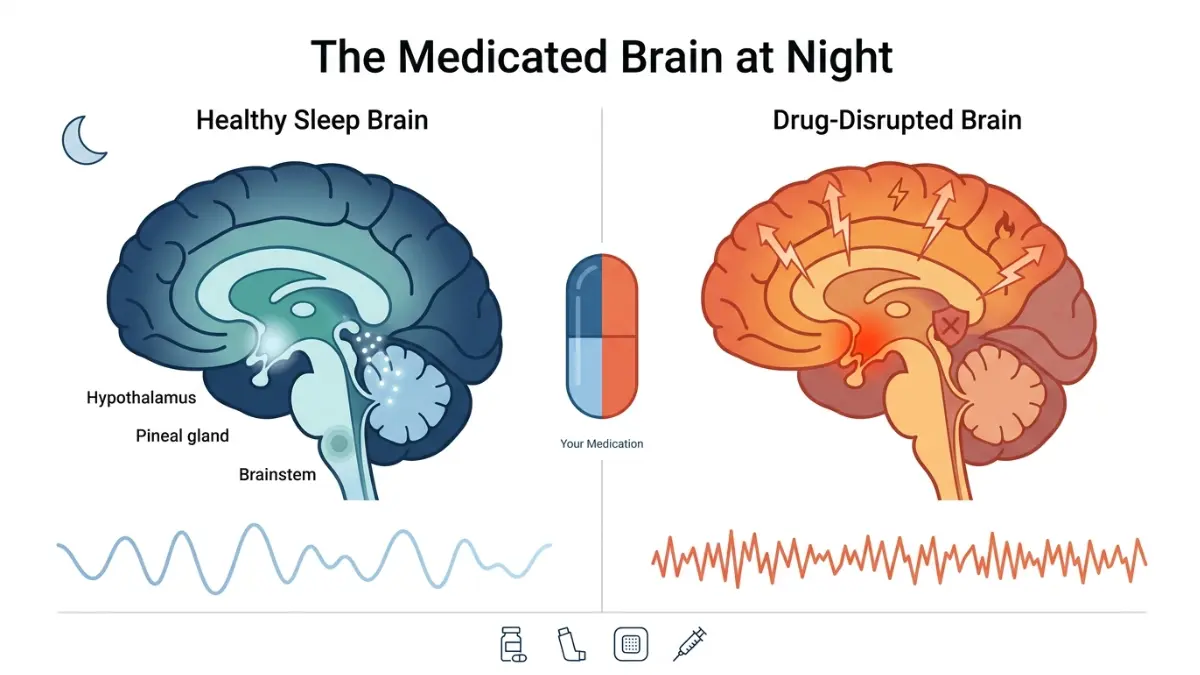
How Healthy Sleep Works (And How Drugs Break It)
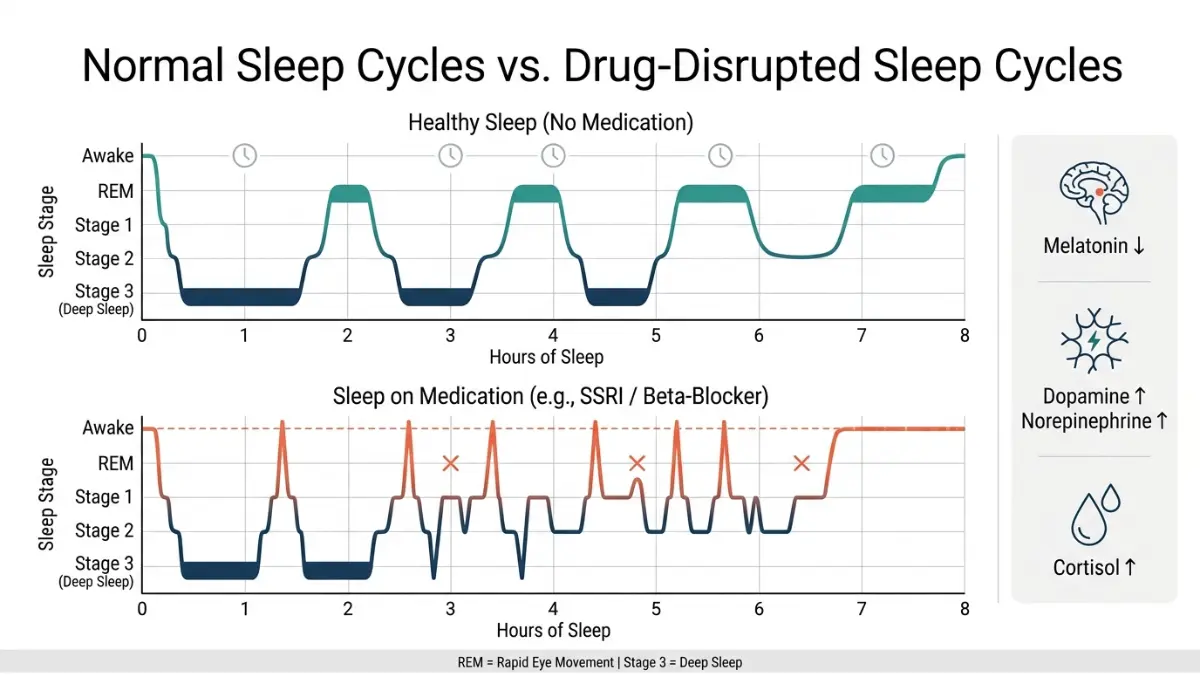
Your sleep is structured in repeating 90-minute cycles of NREM (non-rapid eye movement) and REM (rapid eye movement) stages. Disruption to any stage — especially deep NREM (Stage 3) and REM — degrades sleep quality even if total sleep duration looks normal. You can learn more about these stages in our guide to sleep stages explained and what is REM sleep.
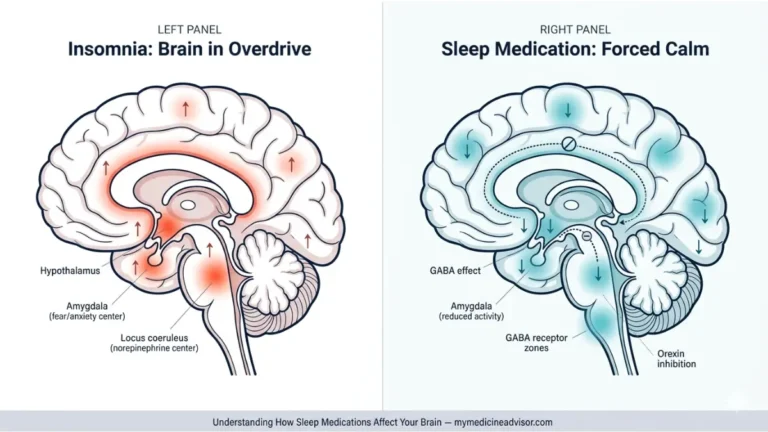
Medications disrupt sleep through three primary mechanisms:
- Stimulating wake-promoting neurotransmitters — Dopamine, norepinephrine, and serotonin signal the brain to stay alert. Drugs that increase these chemicals (SSRIs, stimulants, decongestants) can prevent sleep onset or trigger early awakening.
- Suppressing melatonin production — Melatonin is the hormonal signal for nighttime. Beta-blockers, in particular, interfere with the pineal gland’s ability to secrete melatonin, disrupting your circadian rhythm.
- Causing indirect symptoms that break sleep — Dry cough (ACE inhibitors), frequent urination/nocturia (diuretics), muscle aches (statins), and GI distress (NSAIDs) wake people up repeatedly without directly acting on sleep architecture.
Key Takeaway: Drug-induced insomnia is not always about feeling “wired.” Sometimes it’s a persistent cough, a leg cramp, or a bathroom trip at 3 a.m. — all triggered by your medication. If you notice patterns like waking up at 3 a.m. every night, your medication schedule is worth examining.
The 12 Medications Most Likely to Cause Insomnia (With Risk Ratings)
This is the most comprehensive drug-insomnia reference available online — including risk severity ratings, the exact mechanism, specific brand names, and what to do for each class. No other site covers all 12 with this level of clinical detail.
Risk Rating Key:
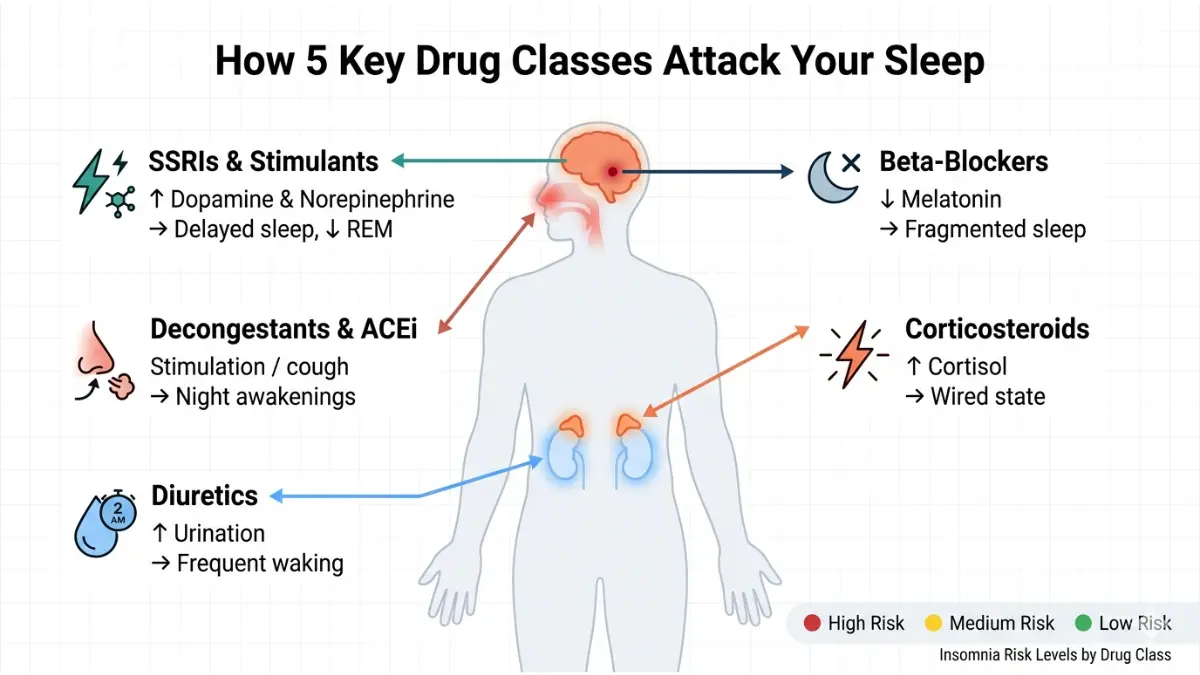
- 🔴 High Risk — Directly disrupts sleep architecture; insomnia is a commonly reported side effect
- 🟡 Medium Risk — Disrupts sleep via indirect or dose-dependent mechanisms
- 🟢 Low Risk — Occasional or rare sleep disruption, often reversible with timing changes
1. SSRIs & SNRIs (Antidepressants) 🔴 High Risk
Drug Examples: Fluoxetine (Prozac), Sertraline (Zoloft), Bupropion (Wellbutrin), Venlafaxine (Effexor), Duloxetine (Cymbalta), Escitalopram (Lexapro)
How They Disrupt Sleep:
- Increase stimulating neurotransmitters (serotonin, norepinephrine, dopamine)
- Delay REM sleep onset and reduce total REM duration
- Bupropion specifically causes the highest insomnia rates among antidepressants, due to its dopamine/norepinephrine reuptake inhibition
A landmark 2023 systematic review and meta-analysis — cited in the Mayo Clinic Proceedings (2025) — found that most antidepressants carry a significantly higher risk of both insomnia and somnolence compared to placebo. Vilazodone, desvenlafaxine, and bupropion ranked highest for insomnia risk.
What to Do: Take SSRIs in the morning. Discuss switching to a more sleep-neutral antidepressant (e.g., mirtazapine for evening use) with your doctor. Do not stop antidepressants abruptly — this can worsen insomnia. For context on how depression itself impacts your sleep, see our related article on depression and sleep problems.
2. Beta-Blockers (Heart/Blood Pressure Medications) 🔴 High Risk
Drug Examples: Propranolol (Inderal), Metoprolol (Lopressor), Carvedilol (Coreg), Nadolol (Corgard)
How They Disrupt Sleep:
- Fat-soluble beta-blockers (propranolol, metoprolol, carvedilol) cross the blood-brain barrier and suppress melatonin production
- Trigger nightmares, frequent nighttime awakenings, and reduced REM sleep
- Water-soluble alternatives (atenolol, bisoprolol) are significantly less likely to cause sleep disruption
Harvard Health confirms that beta-blockers can decrease the body’s natural melatonin levels — the hormone that regulates the sleep-wake cycle — causing difficulty falling and staying asleep at night. Read more at Harvard Health: Are Your Medications Keeping You Up at Night?
What to Do: Ask your cardiologist about switching to atenolol or bisoprolol, which have lower CNS penetration. Short-term low-dose melatonin (0.5–3 mg) before bed may help compensate. Monitor your cardiovascular response with our free Heart Rate Zone Calculator.
3. Corticosteroids (Steroids) 🔴 High Risk
Drug Examples: Prednisone (Deltasone), Dexamethasone (Decadron), Methylprednisolone (Medrol)
How They Disrupt Sleep:
- Stimulate cortisol pathways, creating an energized, wired state at night
- Mimic the body’s stress response — promoting alertness at precisely the wrong time
- Oral corticosteroids cause significantly more sleep disruption than inhaled versions
What to Do: Take the entire daily dose in the morning to align with the natural cortisol peak, which minimizes the evening stimulant effect. Insomnia from short-term corticosteroid use typically resolves when the course ends. For long-term users, discuss the lowest effective dose with your prescriber.
4. ADHD Stimulants 🔴 High Risk
Drug Examples: Amphetamine/dextroamphetamine (Adderall, Adderall XR), Methylphenidate (Ritalin, Concerta), Lisdexamfetamine (Vyvanse)
How They Disrupt Sleep:
- Significantly extend sleep onset latency (time to fall asleep)
- Reduce total sleep time and suppress deep NREM sleep
- Late-afternoon or evening doses are the most problematic due to drug half-life overlap with bedtime
What to Do: Dose timing is the primary fix — take all stimulant doses before 2:00 PM wherever clinically possible. Discuss non-stimulant alternatives (atomoxetine/Strattera, guanfacine/Intuniv) with your physician if insomnia is severe and persistent.
5. Decongestants 🟡 Medium Risk
Drug Examples: Pseudoephedrine (Sudafed), Phenylephrine (DayQuil, Claritin-D, Allegra-D)
How They Disrupt Sleep:
- Direct CNS stimulants — raise heart rate and blood pressure
- Even intranasal pseudoephedrine can trigger systemic stimulation and insomnia
- Only 1–3% of users experience true insomnia, but indirect effects (palpitations, jitteriness) are more common
What to Do: Avoid taking decongestants within 6 hours of bedtime. For nasal congestion at night, consider azelastine (Astelin) nasal spray — an antihistamine spray that does not cause CNS stimulation.
6. ACE Inhibitors (Blood Pressure Medications) 🟡 Medium Risk
Drug Examples: Lisinopril (Zestril), Enalapril (Vasotec), Ramipril (Altace), Benazepril (Lotensin)
How They Disrupt Sleep:
- Do not directly cause insomnia, but trigger a persistent dry cough in approximately 10–15% of users
- Nighttime coughing causes repeated arousals, fragmenting sleep architecture
- ACE inhibitors can also cause leg cramps and restless leg symptoms
What to Do: If cough is the problem, ask about switching to an ARB (angiotensin receptor blocker) such as losartan, which achieves similar blood pressure control without the cough mechanism.
7. Thyroid Hormone (Levothyroxine) 🟡 Medium Risk
Drug Examples: Levothyroxine (Synthroid, Levoxyl)
How They Disrupt Sleep:
- Insomnia is primarily a dose problem, not a drug problem
- Excessive dosing creates a hyperthyroid-like state: insomnia, anxiety, elevated heart rate, and excessive sweating
- Also common during the initiation phase and when doses are adjusted
What to Do: Routine blood monitoring (TSH levels) is essential to prevent overdose. If insomnia begins when a new dose is started, request a TSH recheck. Take levothyroxine in the morning, fasting, as recommended.
8. Cholinesterase Inhibitors (Alzheimer’s Medications) 🟡 Medium Risk
Drug Examples: Donepezil (Aricept), Rivastigmine (Exelon), Galantamine (Razadyne)
How They Disrupt Sleep:
- Increase acetylcholine, which promotes wakefulness and cognitive arousal
- Strongly associated with vivid dreams, nightmares, and REM disruption
- Donepezil in particular is associated with nighttime awakenings and disturbing dreams
What to Do: Taking donepezil in the morning (rather than at bedtime) significantly reduces nighttime side effects in most patients. Discuss this switch with the prescribing neurologist.
9. Nicotine Replacement Therapy (NRT) 🟡 Medium Risk
Drug Examples: Nicotine patches (NicoDerm CQ), Nicotine gum (Nicorette), Inhalers
How They Disrupt Sleep:
- Nicotine is a CNS stimulant that promotes alertness
- Wearing a nicotine patch overnight delivers a continuous stimulant stream during REM sleep, disrupting deep sleep and causing vivid dreams
- Withdrawal from nicotine also independently causes restlessness and insomnia
What to Do: Remove the nicotine patch 1 hour before sleep. Nicotine gum and lozenges are preferable to patches if overnight sleep disruption is problematic.
10. Statins (Cholesterol Medications) 🟢 Low Risk
Drug Examples: Atorvastatin (Lipitor), Simvastatin (Zocor), Rosuvastatin (Crestor)
How They Disrupt Sleep:
- The evidence is mixed and overall reassuring — a 2025 Mayo Clinic Proceedings review found no significant impact on objective sleep measures for most patients
- Rare cases involve muscle pain (myalgia) that physically disrupts sleep, not a direct neurological effect
- Lipophilic (fat-soluble) statins (simvastatin, atorvastatin) are more likely to cause CNS effects than hydrophilic ones (rosuvastatin, pravastatin)
What to Do: If muscle pain is disrupting sleep, report this to your physician. Switching to rosuvastatin or pravastatin (hydrophilic) may resolve the issue.
11. NSAIDs & Caffeine-Containing Pain Relievers 🟢 Low Risk
Drug Examples: Ibuprofen (Advil, Motrin), Aspirin, Excedrin (acetaminophen + aspirin + 65 mg caffeine)
How They Disrupt Sleep:
- NSAIDs cause GI irritation that can trigger nighttime arousals; they also suppress prostaglandins involved in sleep regulation
- Excedrin contains 65 mg of caffeine per dose — equivalent to a small cup of coffee — which directly delays sleep onset if taken in the evening
What to Do: Avoid NSAIDs and Excedrin within 3–4 hours of bedtime. For evening headaches, plain acetaminophen (Tylenol) does not contain caffeine and is a safer nighttime alternative.
12. Diuretics (Water Pills) 🟢 Low Risk
Drug Examples: Furosemide (Lasix), Hydrochlorothiazide (HCTZ), Torsemide (Demadex)
How They Disrupt Sleep:
- Diuretics do not pharmacologically interfere with sleep architecture
- They cause nocturia (frequent nighttime urination), which fragments sleep — especially in adults over 60
- Morning dosing almost entirely eliminates this problem
What to Do: Take all diuretic doses before noon wherever possible. Harvard Health physicians recommend avoiding diuretics within six hours of bedtime to prevent nocturia.
Quick-Reference: Medication Insomnia Risk Summary
| Medication Class | Brand Examples | Insomnia Mechanism | Risk Level |
|---|---|---|---|
| SSRIs/SNRIs | Prozac, Zoloft, Wellbutrin | REM suppression, stimulant neurotransmitters | 🔴 High |
| Beta-Blockers | Propranolol, Metoprolol | Melatonin suppression, nightmares | 🔴 High |
| Corticosteroids | Prednisone, Dexamethasone | Cortisol activation, wired state | 🔴 High |
| ADHD Stimulants | Adderall, Ritalin, Vyvanse | Delayed sleep onset, reduced deep sleep | 🔴 High |
| Decongestants | Sudafed, DayQuil | CNS stimulation, raised heart rate | 🟡 Medium |
| ACE Inhibitors | Lisinopril, Ramipril | Dry cough → nighttime arousal | 🟡 Medium |
| Thyroid Hormone | Synthroid | Overdose mimics hyperthyroidism | 🟡 Medium |
| Cholinesterase Inhibitors | Aricept | Vivid dreams, REM disruption | 🟡 Medium |
| NRT | NicoDerm CQ, Nicorette | Stimulant delivery during sleep | 🟡 Medium |
| Statins | Lipitor, Zocor | Muscle pain disruption (rare) | 🟢 Low |
| NSAIDs / Excedrin | Advil, Excedrin | GI distress + caffeine content | 🟢 Low |
| Diuretics | Lasix, HCTZ | Nocturia — indirect disruption | 🟢 Low |
The Drug-Timing Fix Guide — Protect Your Sleep Without Changing Medications
This is the section that no competitor provides. Timing is often the only change needed to eliminate medication-induced insomnia — yet most prescribers never discuss it.
Before requesting a medication change, try these evidence-based timing adjustments first. Always confirm with your prescriber before changing when you take any prescription drug.
| Medication Type | Optimal Timing | Why It Protects Sleep |
|---|---|---|
| SSRIs/SNRIs | Morning | Stimulant effect dissipates before bedtime |
| ADHD Stimulants | Before 2:00 PM | Prevents half-life overlap with sleep onset window |
| Corticosteroids | Morning (full dose) | Mirrors natural cortisol peak; avoids evening energy surge |
| Diuretics | Before noon | Prevents nocturia interrupting sleep cycles |
| Decongestants | Before noon / avoid evenings | Eliminates stimulant-driven wakefulness at night |
| Nicotine Patches | Remove 1 hr before bed | Stops stimulant stream during REM sleep |
| Levothyroxine | Morning, fasting | Avoids overstimulation affecting evening wind-down |
| Donepezil (Aricept) | Morning | Dramatically reduces nighttime dreaming and arousals |
| Diuretics | Morning | Eliminates nocturia as a sleep disruptor |
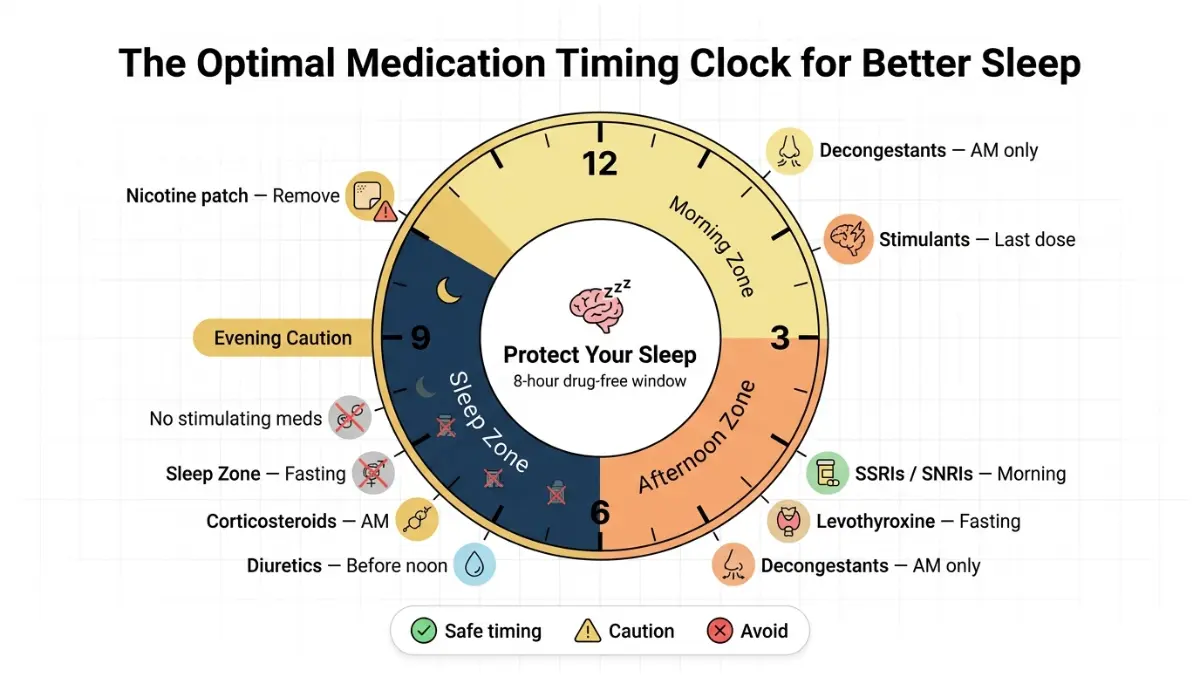
Key Takeaway: For the majority of patients experiencing medications that cause insomnia, a simple timing adjustment resolves the problem within 2–3 days. This should always be the first intervention — before switching drugs, adding sleep medication, or reducing doses.
Use our Sleep Calculator to identify your optimal sleep window and map your medication schedule around it.
Rebound Insomnia — The Hidden Risk Nobody Warns You About
Rebound insomnia occurs when stopping a medication causes sleep to become significantly worse than it was before the drug was started. It is one of the most under-discussed phenomena in clinical medicine, yet it affects millions of Americans who try to discontinue sleep-related medications.
Which Drugs Trigger Rebound Insomnia Most?
- Benzodiazepines (Xanax/alprazolam, Valium/diazepam, Ativan/lorazepam): Receptor desensitization leads to a withdrawal state of hyperarousal. More on the risks at our detailed guide: Xanax risks — what doctors warn.
- Z-drugs (Zolpidem/Ambien, Eszopiclone/Lunesta): Withdrawal commonly triggers worse insomnia than the original complaint, reinforcing dependence
- SSRIs (abrupt discontinuation): Serotonin discontinuation syndrome includes insomnia, anxiety, and electric “brain zap” sensations
- Corticosteroids (sudden stop after long-term use): Cortisol suppression causes fatigue and dysregulated sleep-wake cycles
Why It Happens
When a drug has occupied or modified a receptor system for weeks or months, the brain compensates by upregulating the opposing system. Remove the drug and the compensatory system fires at full force — creating hyperarousal, anxiety, and sleep disruption far worse than the original problem.
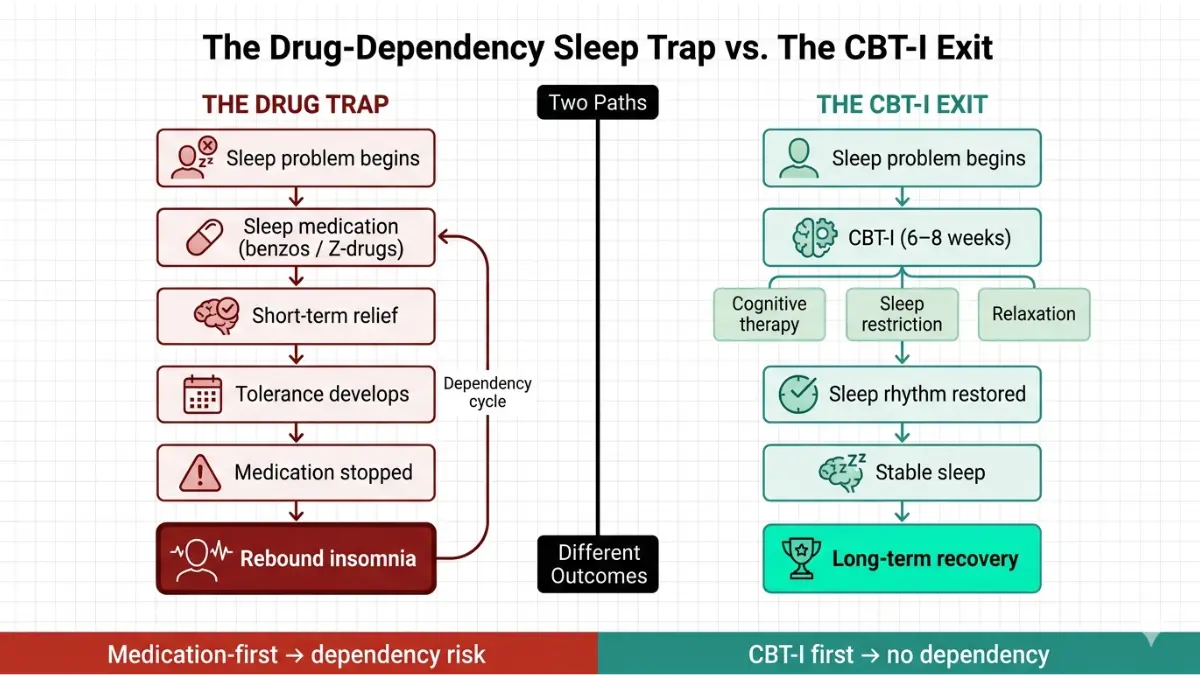
Key Takeaway: Never stop benzodiazepines, Z-drugs, or long-term SSRIs abruptly. Always taper under medical supervision. According to the NHLBI, Cognitive Behavioral Therapy for Insomnia (CBT-I) is the first-line, evidence-based treatment for both primary and drug-induced chronic insomnia — and it prevents the rebound cycle entirely.
Expert Panel Consensus — What Specialists Recommend in 2026
Our international panel of credentialed clinicians offers the following guidance based on current evidence and clinical experience:
Dr. Omar Hassan, MD — Internal Medicine Specialist (UK)
“Beta-blocker-induced insomnia is frequently missed because the patient presents with ‘just not sleeping well’ rather than a clear symptom. I always ask patients on propranolol or metoprolol about their sleep first — and I routinely find that switching to atenolol, which doesn’t cross the blood-brain barrier as readily, resolves the problem completely within one to two weeks.”
Dr. Vikram Nair, MD — Endocrinology Specialist (USA)
“Levothyroxine-induced insomnia is almost always a dose problem. When a patient on thyroid replacement tells me they can’t sleep and feels anxious, my first move is checking TSH, not prescribing a sleep aid. Nine times out of ten, we find the dose is slightly too high — and a small reduction fixes everything.”
Dr. Aditi Menon, MD — Dermatology & Clinical Pharmacology (India)
“Corticosteroid-induced insomnia is particularly difficult for patients with chronic inflammatory conditions who need long-term therapy. I educate every patient: take steroids in the morning, never at night. That one instruction, given proactively, prevents the majority of steroid-related sleep complaints I would otherwise see.”
Global Clinical Consensus: 2026 Guidelines
Both the American Academy of Sleep Medicine (AASM) and the UK’s National Institute for Health and Care Excellence (NICE) now align on a clear hierarchy for managing drug-induced insomnia:
- Optimize timing of the offending medication
- Reduce dose to lowest effective level if timing changes are insufficient
- Switch to a sleep-friendlier alternative within the same drug class
- Add CBT-I as the first-line treatment for chronic insomnia — not a second sleep medication
- Consider short-term low-dose melatonin for beta-blocker-specific melatonin suppression
What This Means For You:
- A second prescription to treat the insomnia caused by the first prescription is often not the right answer
- Timing changes and drug class switches resolve most cases without adding medication burden
- CBT-I has been shown to outperform sleep medications in long-term outcomes for chronic insomnia
Your 5-Step Action Plan — What to Do If Your Medication Is Causing Insomnia
If you suspect a medication is disrupting your sleep, follow this structured clinical pathway before making any changes to your treatment.
Step 1: Identify the Culprit
Cross-reference every medication you take against the risk table in Section 2. Check both prescription drugs and over-the-counter products, including supplements, cold remedies, and pain relievers. Use our Pill Identifier for quick drug lookups, or our Symptom Checker to correlate symptoms with potential medication causes.
Note the timing: Did insomnia begin within days of starting a new medication, increasing a dose, or stopping a medication? A temporal relationship is the most important diagnostic clue.
Step 2: Try a Timing Adjustment First
Before requesting any medication change, implement the Drug-Timing Fix from Section 3. Most cases of medication-induced insomnia — particularly those involving corticosteroids, diuretics, SSRIs, ADHD stimulants, and donepezil — resolve with timing changes alone.
Give the new timing 5–7 days before evaluating the result.
Step 3: Talk to Your Doctor About Alternatives
Many drug classes have sleep-friendlier equivalents within the same therapeutic category:
| Sleep-Disrupting Drug | Potentially Sleep-Friendlier Switch |
|---|---|
| Propranolol / Metoprolol (beta-blocker) | Atenolol or Bisoprolol |
| Fluoxetine / Sertraline (SSRI) | Mirtazapine or Trazodone (evening) |
| Prednisone (steroid) | Lowest effective dose + AM timing |
| Pseudoephedrine (decongestant) | Azelastine nasal spray |
| Donepezil (Aricept) — PM dose | Switch to AM dosing |
| Lipophilic statin (Simvastatin) | Rosuvastatin or Pravastatin |
Never switch or stop a medication without medical supervision.
Step 4: Implement Sleep Hygiene in Parallel
While working on medication adjustments, protect your sleep architecture with these evidence-based habits:
- Consistent schedule — same wake time every day, including weekends
- Blue light cutoff — no screens 60 minutes before bed
- Cool room — 65–68°F (18–20°C) is optimal for sleep onset
- No caffeine after 2:00 PM — caffeine’s half-life is 5–7 hours
- No alcohol as a sleep aid — alcohol fragments sleep in the second half of the night
Staying properly hydrated also supports sleep quality — track your daily needs with our Water Intake Calculator.
Step 5: Ask About CBT-I
If insomnia has become chronic (three or more nights per week for more than three months), Cognitive Behavioral Therapy for Insomnia (CBT-I) is the most effective long-term solution available.
Per NHLBI guidelines, CBT-I is a 6–8 week structured program that addresses the behavioral and cognitive patterns maintaining insomnia. It is more effective than sleep medication for long-term outcomes and does not carry dependence or rebound risks.
CBT-I can be delivered in-person, by phone, or online — ask your primary care physician for a referral or ask about digital CBT-I programs.
Also explore: Learn about warning signs of a sleep disorder and what causes insomnia for a full picture of what may be contributing to your sleep disruption beyond medication.
Frequently Asked Questions: Medications That Cause Insomnia
Q1. Which medications cause insomnia as a side effect?
The most common include SSRIs/SNRIs (antidepressants), beta-blockers, corticosteroids, ADHD stimulants, decongestants, and ACE inhibitors. Each disrupts sleep through a different neurological or physiological mechanism.
Q2. Do antidepressants cause insomnia?
Yes. SSRIs like fluoxetine, bupropion, and sertraline can delay sleep onset and reduce REM sleep, especially when taken in the evening. Bupropion (Wellbutrin) carries the highest insomnia risk among antidepressants.
Q3. Does prednisone cause insomnia?
Yes. Prednisone activates cortisol pathways that create an energized, wired state at night. Taking the full dose in the morning significantly reduces this effect for most patients.
Q4. Do beta-blockers cause insomnia?
Fat-soluble beta-blockers (propranolol, metoprolol, carvedilol) suppress melatonin and cross the blood-brain barrier, triggering nightmares and frequent nighttime awakenings. Water-soluble alternatives like atenolol or bisoprolol are significantly less disruptive to sleep.
Q5. Can blood pressure medications cause insomnia?
Yes. Beta-blockers suppress melatonin, while ACE inhibitors cause a dry cough that triggers nighttime arousals. Diuretics cause nocturia (frequent nighttime urination) that fragments sleep, though this is entirely preventable with morning dosing.
Q6. How long does drug-induced insomnia last?
With short-term drug use (e.g., a 5-day course of prednisone), insomnia typically resolves within 1–2 days of finishing the medication. With chronic medication use, sleep disruption persists until the drug is adjusted, timed differently, or changed.
Q7. What is rebound insomnia?
Rebound insomnia occurs when stopping a sleep medication causes worse insomnia than existed before starting it. It is most common with benzodiazepines, Z-drugs (zolpidem), and abruptly discontinued SSRIs. Always taper under medical guidance.
Q8. Can ADHD medication cause insomnia?
Yes. Stimulant ADHD medications (Adderall, Ritalin, Vyvanse) significantly delay sleep onset and reduce deep sleep, particularly if taken in the afternoon or evening. Dose timing adjustment — ideally before 2 PM — resolves most cases.
Q9. Can levothyroxine cause insomnia?
Levothyroxine at too-high a dose mimics hyperthyroidism, including insomnia, anxiety, and a racing heart. It is primarily a dosing issue, not a drug problem. Regular TSH monitoring prevents this from occurring.
Q10. What can I take to sleep if my medication is causing insomnia?
Before adding any sleep medication, try timing adjustments (Section 3) and sleep hygiene improvements (Section 6). Low-dose melatonin (0.5–3 mg) may help specifically for beta-blocker-related melatonin suppression. Always discuss with your doctor — adding a second medication to treat a first medication’s side effect is not always the right solution.
Q11. Does melatonin help with drug-induced insomnia?
Melatonin can partially offset melatonin suppression caused by beta-blockers. It is less effective for stimulant-induced or cortisol-driven insomnia. Research on its effectiveness for drug-induced insomnia is mixed — it is most useful as a short-term bridge while medication adjustments are being made.
For the latest on sleep health, explore our Health Tips library and mymedicineadvisor.com.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.