On This Page – Quick Medical Summary
Peritoneal mesothelioma is a rare abdominal cancer with a 5-year survival rate of 65% in patients who receive cytoreductive surgery combined with HIPEC — dramatically better than other mesothelioma types. Without treatment, median survival is under 12 months. In 2026, new immunotherapy combinations and surgical trials are pushing these numbers even higher for eligible patients.
What Is Peritoneal Mesothelioma? The 2026 Medical Definition
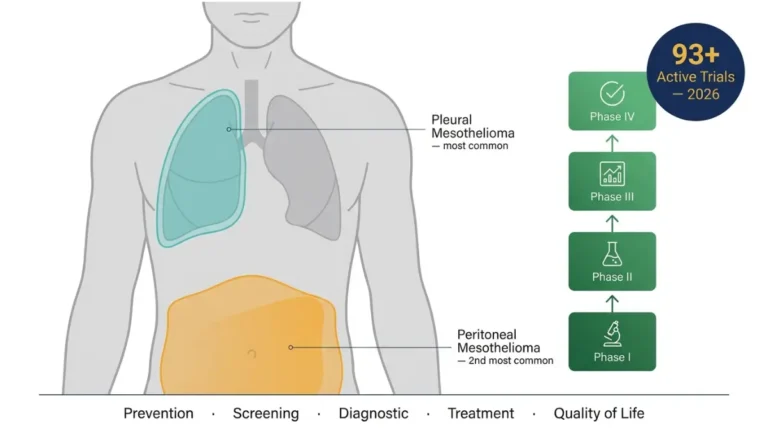
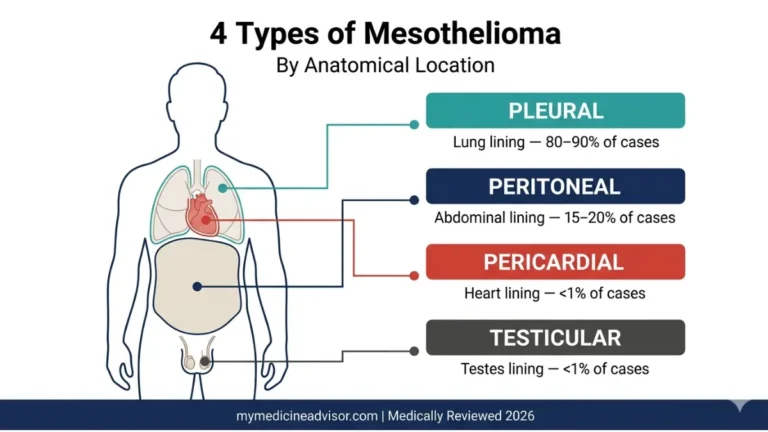
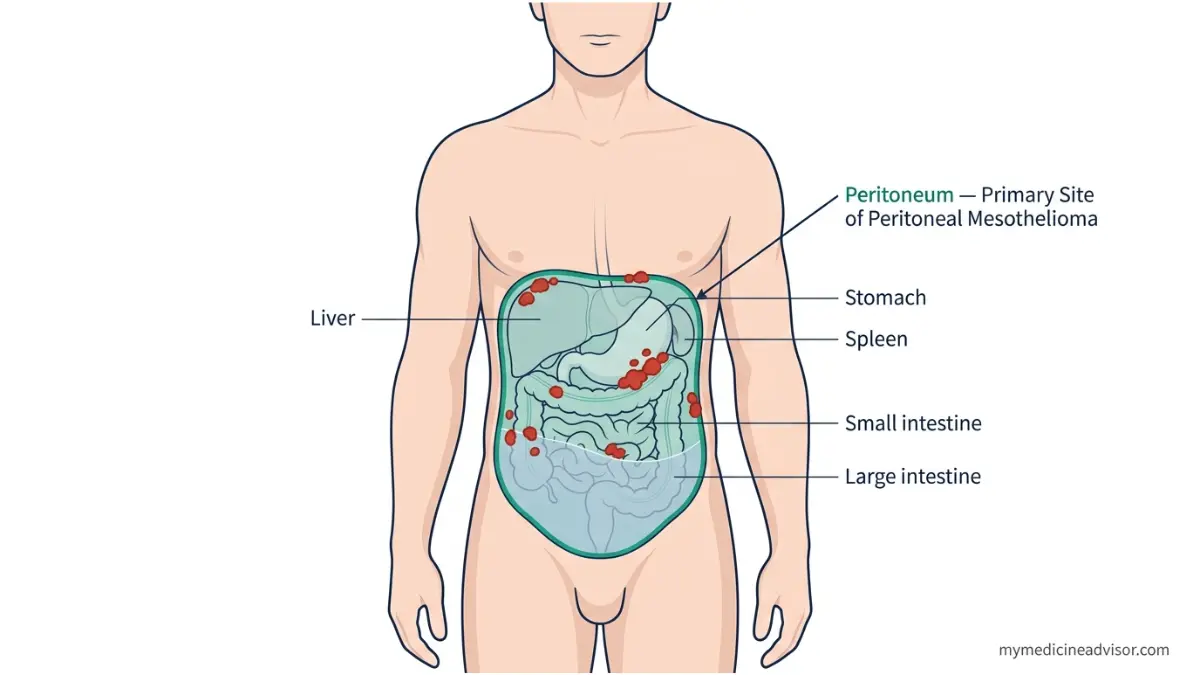
Peritoneal mesothelioma is a rare, aggressive cancer that forms in the peritoneum — the thin tissue membrane lining the inside of the abdomen and covering organs like the stomach, liver, and spleen. It accounts for 15–20% of all mesothelioma cases, with approximately 400–700 new diagnoses in the United States each year.
Unlike most cancers, malignant peritoneal mesothelioma spreads within the abdominal cavity rather than quickly reaching distant organs. This contained pattern of spread is a key reason why survival outcomes are significantly better compared to pleural mesothelioma (which affects the lung lining).
How Peritoneal Mesothelioma Differs From Pleural Mesothelioma
| Feature | Peritoneal Mesothelioma | Pleural Mesothelioma |
|---|---|---|
| Location | Abdominal lining | Lung lining |
| US cases per year | 400–700 | 2,500–3,000 |
| 5-year survival (with treatment) | 65% | 12% |
| Primary treatment | CRS-HIPEC | Surgery + chemo/immunotherapy |
| Gender distribution | Equal (men and women) | Predominantly men |
If you are experiencing unexplained abdominal symptoms, use our Symptom Checker to document them before your next medical appointment.
Who Gets Peritoneal Mesothelioma?
The mean age at diagnosis is 64 years, but cases have been diagnosed across a broad age range.
- Primary cause: Asbestos fiber ingestion (rather than inhalation) — fibers reach the peritoneum through the digestive system
- Secondary exposure: Living with asbestos workers — family members exposed to fibers carried home on clothing
- Latency period: Symptoms typically appear 20–50 years after initial exposure, meaning many patients have no memory of contact with asbestos
- Race: Over 90% of US patients are non-Hispanic white, according to SEER database data from the National Cancer Institute
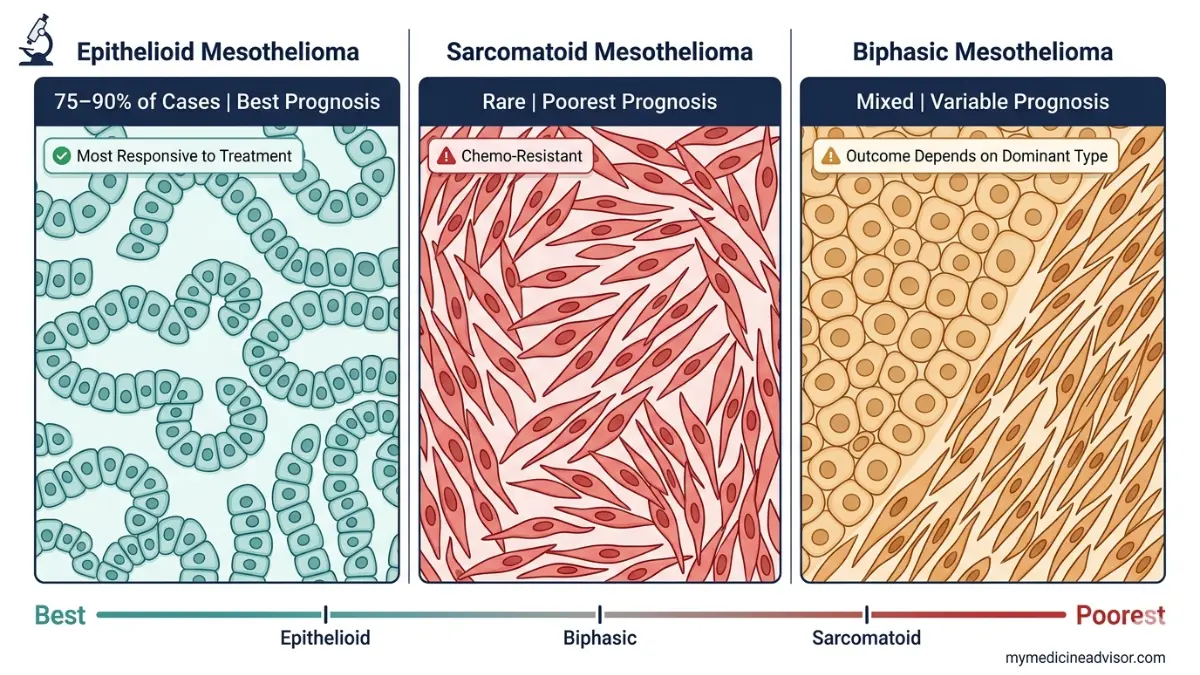
The 3 Cell Types — Why They Determine Everything
Your cell type (histology) is one of the single most important factors shaping your treatment options and survival outlook.
- Epithelioid (75–90% of cases): Best prognosis; responds well to HIPEC and immunotherapy. Resembles normal mesothelial cell structure.
- Sarcomatoid: Most aggressive subtype; largely resistant to chemotherapy; associated with poor survival regardless of treatment
- Biphasic: Contains both epithelioid and sarcomatoid elements; outcomes vary depending on which type dominates
Key takeaway: Ask your oncologist specifically which cell type your tumor is — it directly determines which treatment options are available to you.
Peritoneal Mesothelioma Symptoms Most Doctors Initially Miss
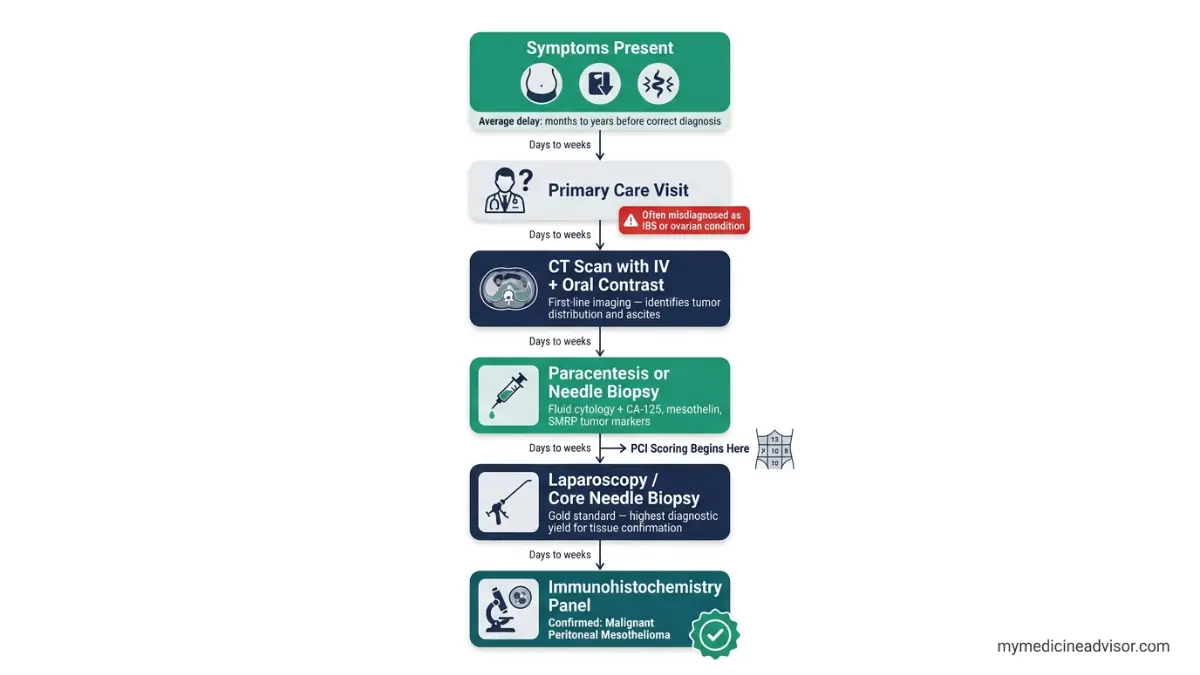
One of the most dangerous aspects of peritoneal mesothelioma is how long it goes undetected. Many patients are initially told they have irritable bowel syndrome, ovarian cysts, or general gastrointestinal problems before a correct diagnosis is made.
Early Warning Signs to Never Ignore
The earliest symptoms are vague and easily attributed to common conditions:
- Abdominal bloating or distension — often the first noticeable sign, frequently dismissed as digestive issues
- Unexplained weight loss — unintentional loss of 10+ pounds without dietary changes
- Persistent abdominal pain or discomfort
- Early satiety — feeling full after eating very small amounts
- New-onset ascites — abnormal fluid buildup in the abdominal cavity, causing visible swelling
- Fatigue and weakness — not explained by other causes
- Nausea or vomiting — particularly in later disease stages
Key takeaway: Symptoms typically appear 20–50 years after initial asbestos exposure. If you or a family member ever worked in construction, shipbuilding, automotive manufacturing, or industrial settings, report this history to your doctor immediately.
Why Diagnosis Almost Always Comes Late
There is no routine screening test for peritoneal mesothelioma. No blood test, no standard imaging protocol, and no national screening program exists in the United States.
The diagnostic pathway typically involves:
- CT scan with oral and IV contrast — first-line imaging to identify tumor spread and ascites
- Paracentesis — drawing abdominal fluid to examine cells for mesothelioma markers
- Core needle biopsy or laparoscopy — gold standard for tissue confirmation; provides better diagnostic yield than fine needle biopsy
- Tumor markers: CA-125, mesothelin, and SMRP — elevated levels support diagnosis but are not definitive alone
- Immunohistochemistry panel — pathology review checking at least two mesothelioma markers and two carcinoma markers for definitive diagnosis
The 2026 Staging Breakthrough Competitors Aren’t Covering
The traditional staging tool for peritoneal mesothelioma is the Peritoneal Carcinomatosis Index (PCI) — a 0–39 score that divides the abdomen into 13 regions, scoring each 0–3 based on tumor size and spread.
In 2026, researchers at the University of California San Francisco proposed a groundbreaking new “survival tree” staging model. Unlike PCI alone, this model analyzes combinations of tumor characteristics to predict patient survival more precisely — enabling oncologists to better explain prognosis and plan appropriate treatment.
| PCI Score | Stage | Surgical Eligibility | Expected Outcome |
|---|---|---|---|
| 0–10 | Early | Strong HIPEC candidate | Best survival outcomes |
| 11–20 | Intermediate | Selective HIPEC candidate | Intermediate outcomes |
| 21–39 | Advanced | Palliative focus | Limited surgical options |
Key takeaway: If your oncologist is using only PCI scoring, ask them about the 2026 survival tree model from UCSF — it may give you a more accurate picture of your prognosis and treatment options.
For a deeper understanding of how this cancer compares to related conditions, read our guide on pleural mesothelioma stages and types.
Peritoneal Mesothelioma Survival Rates — What the 2026 Data Actually Shows
This is where most patients and families need the clearest information — and where almost every competitor fails them by either burying the data or mixing peritoneal statistics with pleural statistics.
The Core Survival Numbers (SEER-Sourced, 2026)
According to NCI’s National Cancer Institute treatment data, survival outcomes for peritoneal mesothelioma vary dramatically based on whether and how a patient is treated.
| Metric | No Treatment | Chemo Only | CRS-HIPEC |
|---|---|---|---|
| Median survival | < 12 months | ~13 months | ~53 months |
| 1-year survival | ~40% | ~56% | ~92% |
| 5-year survival | < 5% | ~18–20% | 65% |
| 10-year survival | Rare | Rare | ~39% |
Key takeaway: Peritoneal mesothelioma patients who receive CRS-HIPEC are 65% likely to be alive at 5 years — compared to less than 5% without any treatment. Treatment is the single most important variable in your prognosis.
What Determines Your Individual Survival Rate?
Population statistics cannot predict individual outcomes. These are the specific factors your oncologist weighs:
- Cell type: Epithelioid patients consistently outperform sarcomatoid and biphasic patients across all treatment types
- PCI score at diagnosis: A PCI below 20 dramatically increases eligibility for complete cytoreduction, which is the strongest predictor of long-term survival
- Age and fitness: Younger, healthier patients tolerate aggressive multimodal treatment better and qualify for more interventions
- Treatment center expertise: Outcomes at high-volume specialized mesothelioma centers are significantly better than at general hospitals — this single factor can be the difference between curative and palliative intent treatment
- Gender: Female patients statistically have better survival outcomes, partly linked to peritoneal mesothelioma’s higher incidence in women and estrogen receptor interactions with tumor cells
- Completeness of cytoreduction (CC score): A CC-0 result (no visible tumor remaining post-surgery) is the strongest surgical predictor of long-term survival
Real Patient Outcomes — Beyond the Statistics
Michael’s story: Diagnosed with peritoneal mesothelioma in his mid-50s, Michael was initially given a prognosis of under 12 months. After being referred to a specialized mesothelioma center and undergoing CRS-HIPEC, he enrolled in a subsequent immunotherapy clinical trial. Four years post-surgery, his cancer has not recurred.
Dana’s journey: A peritoneal mesothelioma patient who underwent five separate clinical trials stated: “Each trial has extended my life a bit longer.” Her case illustrates why clinical trial access is now considered part of the standard of care conversation.
What This Means For You: Statistics reflect population averages built on historical data. Your PCI score, cell type, treatment center, and willingness to pursue emerging therapies all push your individual outcome beyond what any average can predict. Use our Genetic Risk Assessment Tool to understand hereditary factors that may influence your cancer biology.
You can also read our complete guide on mesothelioma survival rates and symptoms for additional data context.
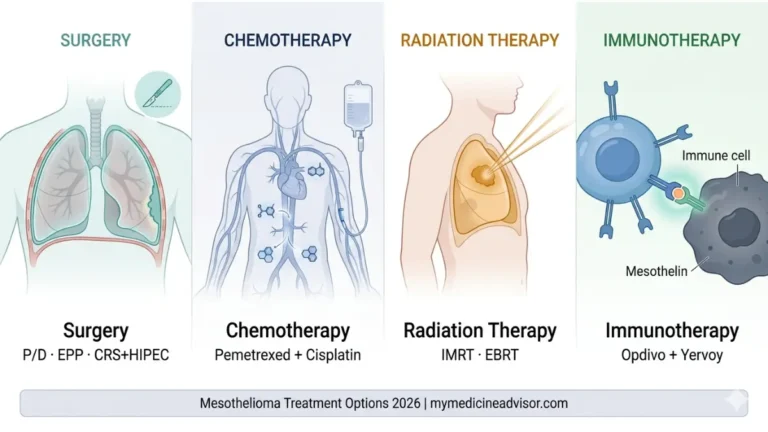
Peritoneal Mesothelioma Treatment Options in 2026 — The Complete Arsenal
This section covers every treatment available in 2026 — from the proven gold standard to the emerging therapies that competitors aren’t writing about yet.
The Gold Standard: CRS-HIPEC Explained in Plain Language
Cytoreductive surgery with hyperthermic intraperitoneal chemotherapy (CRS-HIPEC) remains the most effective treatment for eligible peritoneal mesothelioma patients and represents the only realistic pathway to long-term survival.
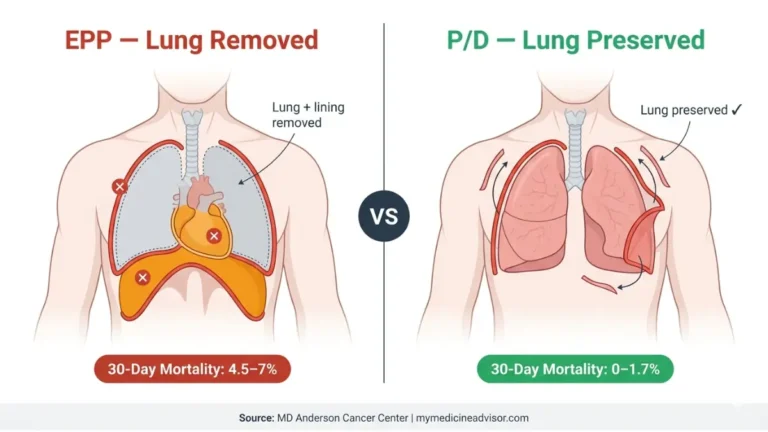
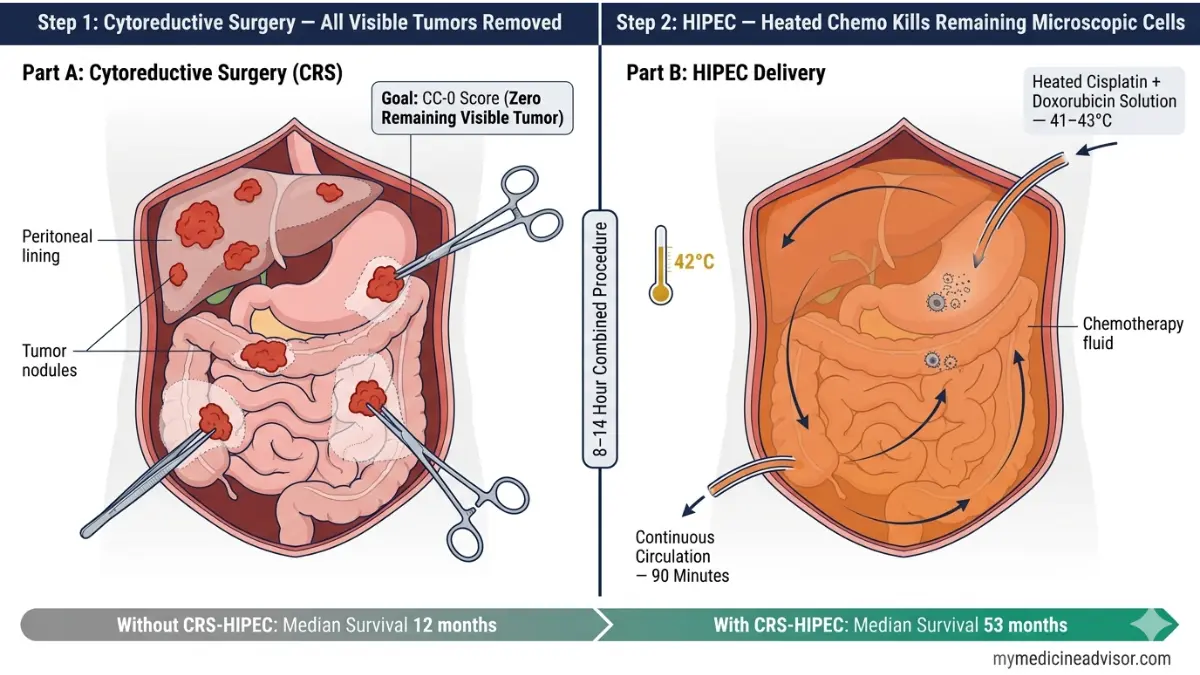
What happens during CRS-HIPEC:
- The surgeon removes all visible tumor tissue from the abdominal cavity — this includes portions of the peritoneal lining and, in some cases, sections of affected organs (peritonectomy)
- Immediately after tumor removal, a heated chemotherapy solution (41–43°C) — typically cisplatin plus doxorubicin — is circulated directly inside the abdominal cavity for 90 minutes
- The heat enhances chemotherapy absorption into microscopic residual cancer cells while limiting systemic toxicity
Key facts about CRS-HIPEC:
- Procedure duration: 8–14 hours
- Average cost in the US: approximately $84,000
- Best results in patients with PCI score below 20 and epithelioid cell type
- Median survival with optimal cytoreduction: 53+ months
- 5-year survival with complete cytoreduction (CC-0): 65%
- Must be performed at a high-volume specialized center to achieve these outcomes — general surgeons should not perform this procedure
The National Cancer Institute’s treatment guidelines confirm CRS-HIPEC as the standard of care for patients with resectable malignant peritoneal mesothelioma and no extraperitoneal disease spread.
Key takeaway: CRS-HIPEC is not available at most US hospitals. Seeking care at a mesothelioma-specialized center is not optional — it is essential.
HIPEC vs. NIPEC — The 2025 Trial That Could Change Post-Surgical Care
A landmark Phase II randomized trial, ICARuS II (NCT06057935), is currently enrolling at Memorial Sloan Kettering Cancer Center, Siteman Cancer Center at Washington University, and Fred & Pamela Buffett Cancer Center (University of Nebraska).
The trial compares two post-surgical chemotherapy approaches:
- NIPEC (normothermic intraperitoneal chemotherapy): Body-temperature chemo solution delivered directly into the abdominal cavity after CRS-HIPEC
- IV chemotherapy: Standard intravenous delivery into the bloodstream
This trial could redefine post-surgical standard of care within the next 2–3 years. If you have recently undergone CRS-HIPEC or are planning surgery, ask your oncologist whether you are eligible to enroll. Trial details are available at ClinicalTrials.gov NCT06057935.
Systemic Chemotherapy — When Surgery Is Not an Option
For patients with advanced disease (high PCI score, extraperitoneal spread, or poor surgical fitness), systemic chemotherapy remains the primary treatment.
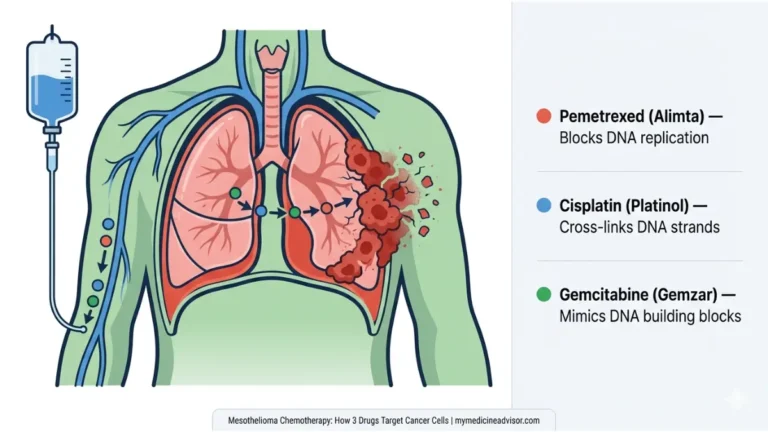
Standard first-line regimen: Pemetrexed + cisplatin (or carboplatin)
- Objective response rate: only 13–25%
- Median survival: approximately 10–13 months
- The honest reality: Chemotherapy alone produces modest results in peritoneal mesothelioma. The disease is largely considered chemotherapy-resistant compared to other cancers.
Second-line options (no established standard of care exists):
- Gemcitabine (single agent or in combination)
- Raltitrexed — an antifolate alternative used primarily in Europe and Australia
- Clinical trial enrollment is strongly recommended at this stage
Immunotherapy in 2026 — The Most Significant Treatment Advance
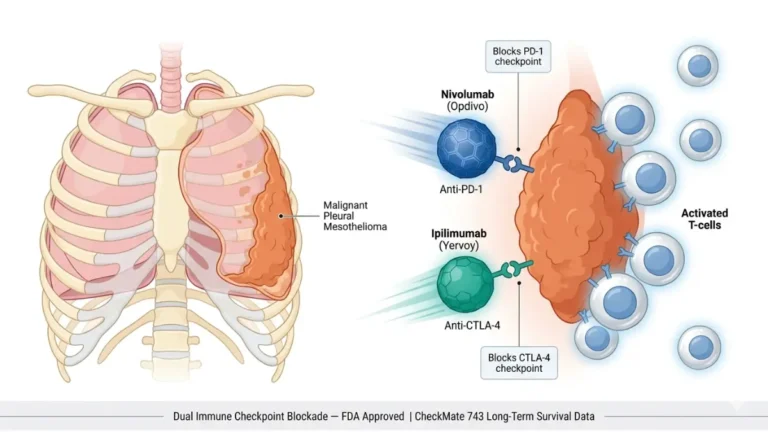
Immunotherapy represents the most exciting development in peritoneal mesothelioma treatment in two decades. These drugs work by helping the immune system recognize and destroy cancer cells that have been hiding from immune detection.
Current immunotherapy landscape for peritoneal mesothelioma:
- Nivolumab + ipilimumab (Opdivo + Yervoy): FDA-approved in 2020 for unresectable pleural mesothelioma — actively being studied in peritoneal mesothelioma through ongoing trials
- Atezolizumab + bevacizumab: MD Anderson Cancer Center trial in platinum-failed patients — 40% objective response rate, 1-year overall survival of 86% in this heavily pre-treated group
- SMARTEST trial (Princess Margaret Cancer Centre, Toronto): Testing tremelimumab + durvalumab as post-CRS-HIPEC immunotherapy — actively enrolling in 2025
- Neoadjuvant nivolumab + ipilimumab: A 2025 case report from Université de Montréal demonstrated a patient with previously borderline-unresectable peritoneal mesothelioma who responded sufficiently to immunotherapy to then undergo CRS-HIPEC — remaining disease-free 30 months post-surgery
Key takeaway: Immunotherapy is not yet FDA-approved specifically for peritoneal mesothelioma. However, 2025–2026 trial data is producing the most meaningful survival signals this disease has ever seen. Ask your oncologist about trial eligibility before starting any systemic treatment.
Our comprehensive guide on how immunotherapy works explains the mechanism in plain language.
Emerging Therapies 2026 — What the Competitors Aren’t Writing About
These treatments are not yet standard of care but represent the frontier of what is being studied:
- CAR T-cell therapy targeting mesothelin: Phase I trial at Memorial Sloan Kettering — genetically engineering a patient’s own T-cells to attack the mesothelin protein expressed on mesothelioma cells. Combined with pembrolizumab in the ongoing trial.
- ADI-PEG20 (pegargiminase) — ATOMIC-Meso trial: This drug starves mesothelioma cells of arginine, an amino acid they cannot produce independently. Combined with chemotherapy, it quadrupled the 3-year survival rate compared to chemotherapy alone in the trial data.
- Photodynamic therapy (PDT): Light-activated drugs (photosensitizers) that kill cancer cells when exposed to specific light wavelengths — currently in Phase I/II trials for peritoneal mesothelioma
- MCY-M11: A therapy derived from a patient’s own white blood cells, currently in clinical trials
- Gene therapy: Modifying mesothelioma cells to become susceptible to targeted treatments — investigational stage
| Treatment | Stage | Best For | Key Data Point |
|---|---|---|---|
| CRS-HIPEC | Standard of care | Resectable disease, PCI < 20 | 65% 5-year survival |
| Pemetrexed + cisplatin | Standard (inoperable) | All patients | 13–25% response rate |
| Nivolumab + ipilimumab | Trials/emerging | Post-platinum failure | 86% 1-year OS (atezolizumab combo) |
| ADI-PEG20 (ATOMIC-Meso) | Phase II/III | Arginine-auxotrophic tumors | 4x 3-year survival vs chemo alone |
| CAR T-cell (mesothelin) | Phase I | Advanced/refractory | Trial ongoing at MSK |
Choosing the Right Treatment Center & Questions to Ask Your Doctor
This section is entirely missing from every major competitor’s article for US patients. It is among the most actionable content you will find anywhere.
Why Your Treatment Center Matters More Than Almost Anything
CRS-HIPEC is one of the most technically demanding procedures in surgical oncology. Outcomes at specialized, high-volume centers are dramatically better than at general hospitals.
The Peritoneal Surface Oncology Group International (PSOGI) explicitly recommends that all malignant peritoneal mesothelioma patients be treated at high-volume centers with strong consideration for inclusion in tumor registries and clinical trials. A surgeon performing CRS-HIPEC twice a year versus a surgeon who performs it 50 times a year produces fundamentally different survival results for their patients.
Top US Centers Specializing in Peritoneal Mesothelioma
These centers are recognized by the National Cancer Institute as NCI-Designated Cancer Centers with established mesothelioma programs:
- Memorial Sloan Kettering Cancer Center — New York, NY (site of CAR T-cell mesothelin trial)
- MD Anderson Cancer Center — Houston, TX (site of atezolizumab + bevacizumab peritoneal trial)
- University of California San Francisco (UCSF) — San Francisco, CA (home of 2026 survival tree staging model research)
- Washington University Siteman Cancer Center — St. Louis, MO (ICARuS II trial site)
- University of Pittsburgh Medical Center — Pittsburgh, PA
Key takeaway: If your current oncologist has not performed CRS-HIPEC at least 20–30 times, requesting a referral or second opinion at one of the above centers is strongly recommended.
5 Questions Every Peritoneal Mesothelioma Patient Should Ask Their Oncologist
Before leaving any oncology appointment, confirm you have answers to these five questions:
- What is my exact PCI score? What does this number mean for my HIPEC eligibility right now?
- What is my cell type? Am I epithelioid, sarcomatoid, or biphasic — and how does this change my treatment plan?
- How many CRS-HIPEC procedures has this center performed? If fewer than 20 annually, ask for a referral to a high-volume center.
- Am I eligible for any 2025–2026 immunotherapy clinical trials? Specifically ask about ICARuS II (NCT06057935) and the atezolizumab combination trials.
- What is the primary goal of my treatment — curative intent or symptom management? Understanding this distinction shapes every decision that follows.
Key takeaway: Getting a second opinion at a mesothelioma-specialized center is not disloyalty to your doctor. For this disease, it can add years to your life.
Use our Symptom Checker to track and organize your symptoms before your consultation — documenting changes over time gives your oncologist more actionable information.
Read our related guide on what is the main cause of mesothelioma to understand your exposure history before your specialist appointment.
Living With Peritoneal Mesothelioma — Quality of Life, Nutrition & Palliative Care 2026
A peritoneal mesothelioma diagnosis changes every part of life — not just your treatment schedule. This section covers what happens between appointments, during treatment, and for patients whose focus shifts from curing the disease to living well with it.
Palliative Care Is Not Giving Up
Palliative care is concurrent care — it runs alongside active cancer treatment, not instead of it. Every patient with peritoneal mesothelioma, regardless of stage, benefits from palliative care integration.
Key palliative interventions for peritoneal mesothelioma:
- Paracentesis: Procedure to drain accumulated abdominal fluid (ascites), relieving pressure and pain. Can be performed repeatedly as needed. Provides significant short-term quality of life improvement.
- Pain management protocols: Multimodal pain management including NSAIDs, opioids when appropriate, and nerve blocks for refractory pain
- Bowel obstruction prevention: Dietary management, prokinetics, and surgical intervention when necessary
- Palliative chemotherapy: Lower-dose systemic chemotherapy to slow disease progression and control symptoms without curative intent
Nutrition During Treatment — A Factor Most Oncologists Don’t Discuss Enough
Malnutrition and cancer-related cachexia (muscle wasting) are among the leading causes of reduced treatment eligibility and poorer post-surgical outcomes in peritoneal mesothelioma patients.
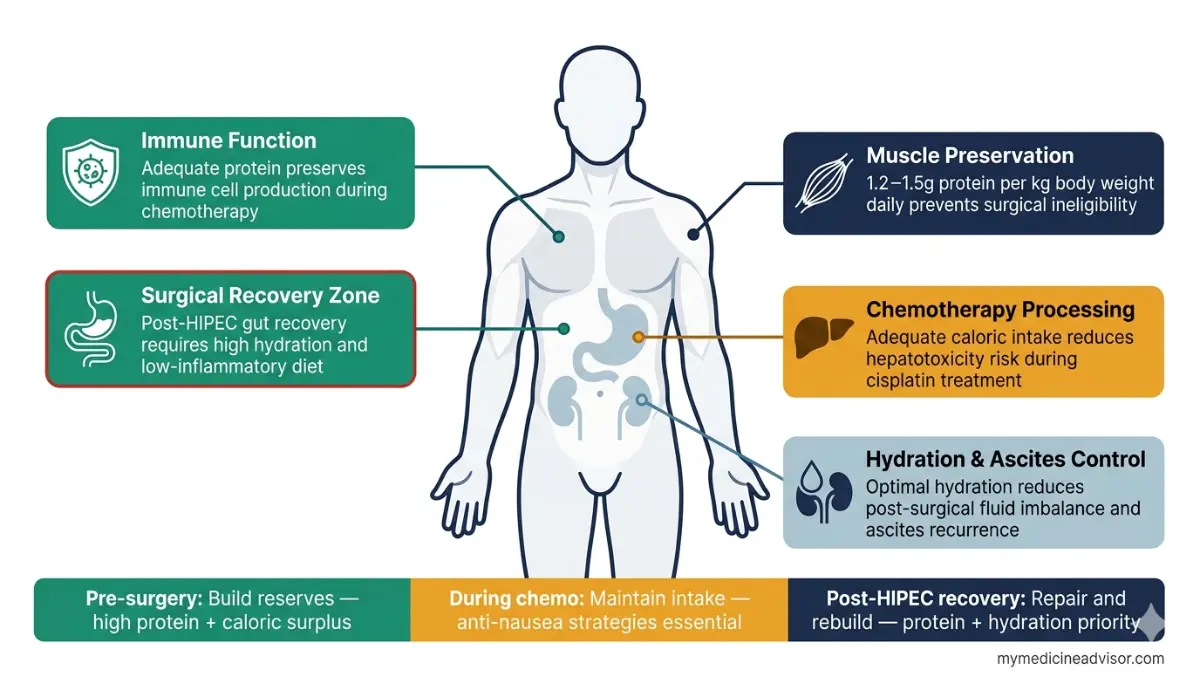
Why nutrition matters specifically for this disease:
- Adequate protein intake is essential for surgical recovery after CRS-HIPEC
- Muscle mass affects your eligibility for aggressive treatment — frail patients are often excluded from surgery
- Chemotherapy significantly affects appetite, taste, and nutrient absorption
- Maintaining healthy body weight improves immune function and treatment tolerance
Evidence-based nutritional targets during treatment:
- Protein: 1.2–1.5g per kilogram of body weight daily during active treatment and recovery
- Calories: Avoid unintentional caloric restriction — malnutrition accelerates disease progression
- Hydration: Critical during and after HIPEC recovery — monitor fluid balance closely
Use our Protein Intake Calculator to determine your personal daily protein target based on your current body weight, and our Water Intake Calculator to track daily hydration targets during your recovery period.
Key takeaway: Discuss nutritional support with your oncology team before starting treatment. A registered oncology dietitian referral should be standard practice — ask for one if it hasn’t been offered.
Emotional Support and Mental Health
Living with a rare YMYL-level diagnosis creates profound psychological pressure — not only for the patient but for the entire family system.
- Support resources: Mesothelioma Applied Research Foundation (MARF) offers patient navigator services and support communities specifically for mesothelioma patients
- Family members: Those exposed through secondary asbestos contact (children of workers, spouses) face additional emotional complexity around diagnosis and guilt
- Mental health integration: Ask your treatment center about oncology psychologists and social workers — major NCI-designated centers offer these services as part of integrated care
What This Means For You: You are not a statistic. The 65% five-year survival rate for CRS-HIPEC patients reflects thousands of cases. Your individual outcome depends on your PCI score, cell type, treatment center, and the treatment decisions made in the next weeks and months. Getting to the right center, asking the right questions, and maintaining your physical condition through treatment are all factors within your control.
For broader context on related cancer treatments, our guides on radiation therapy and chemotherapy side effects 2026 cover what to expect from combined treatment approaches. For information on the asbestos-related lung condition that sometimes precedes diagnosis, our guide on asbestosis symptoms and the deadly delay provides important context.
Peritoneal Mesothelioma — Frequently Asked Questions (2026)
Q1. What is the survival rate for peritoneal mesothelioma in 2026?
The 5-year survival rate for peritoneal mesothelioma is 65% in patients who receive cytoreductive surgery with HIPEC, based on SEER data tracked by the National Cancer Institute. Without treatment, median survival is under 12 months. The gap between treated and untreated outcomes is wider for this cancer than almost any other rare malignancy.
Q2. Is peritoneal mesothelioma curable?
There is no confirmed cure for peritoneal mesothelioma as of 2026. However, approximately 39% of patients who receive CRS-HIPEC have survived beyond 10 years — a milestone some oncologists describe as functional long-term remission. A 2025 patient survey found that 11% of mesothelioma respondents who received active treatment reported achieving complete remission.
Q3. How is peritoneal mesothelioma different from pleural mesothelioma?
Peritoneal mesothelioma develops in the abdominal lining; pleural develops in the lung lining. The abdominal location means peritoneal mesothelioma does not compromise breathing capacity, responds better to direct surgical intervention, and has a 65% 5-year survival rate compared to 12% for pleural. They share the same cellular origin and primary cause — asbestos exposure.
Q4. What causes peritoneal mesothelioma?
Asbestos exposure is the primary cause in the vast majority of cases. Asbestos fibers can be ingested rather than inhaled, with fibers traveling to the peritoneum through the digestive system. Secondary exposure — living with an asbestos worker who unknowingly brought fibers home on clothing or hair — is a documented and tragically common cause. Symptoms appear 20–50 years after exposure.
Q5. What is HIPEC and how does it work?
HIPEC (hyperthermic intraperitoneal chemotherapy) is heated chemotherapy — typically 41–43°C — delivered directly into the abdominal cavity immediately following cytoreductive surgery. The heat enhances drug penetration into microscopic cancer cells while limiting systemic side effects. The procedure circulates the solution for approximately 90 minutes and is performed in the same surgical session as tumor removal.
Q6. What is a PCI score and why does it matter?
The Peritoneal Carcinomatosis Index (PCI) scores tumor spread by dividing the abdomen into 13 regions, each rated 0–3 based on tumor size. The total score ranges from 0–39. A PCI below 20 generally indicates HIPEC eligibility and is associated with significantly better survival outcomes. A score above 20 typically means the disease is too widespread for complete cytoreduction.
Q7. Can immunotherapy treat peritoneal mesothelioma?
Immunotherapy is not yet FDA-approved specifically for peritoneal mesothelioma as of April 2026. However, active trials using nivolumab, ipilimumab, atezolizumab, and tremelimumab combinations are showing meaningful response rates. The MD Anderson atezolizumab + bevacizumab trial produced a 40% objective response rate and 86% 1-year overall survival in platinum-failed patients — the most promising results yet reported.
Q8. How long can you live with peritoneal mesothelioma without treatment?
Without any treatment, median survival is 6–12 months from diagnosis for malignant peritoneal mesothelioma. With CRS-HIPEC-based multimodal treatment, median survival extends to approximately 53 months (over 4 years). This is one of the largest treatment-versus-no-treatment survival gaps of any rare cancer.
Q9. What are the first symptoms of peritoneal mesothelioma?
Early symptoms include abdominal bloating, unexplained weight loss, persistent abdominal discomfort, and early satiety (feeling full after small meals). New-onset ascites — visible abdominal fluid buildup — is a red flag that warrants immediate investigation. These symptoms are frequently misdiagnosed as IBS, ovarian conditions, or general GI disorders for months or years before the correct diagnosis.
Q10. Is peritoneal mesothelioma the same as stomach cancer?
No. Peritoneal mesothelioma arises from the mesothelial cells lining the abdominal cavity — not from the stomach wall itself. It has completely different causes, treatments, and prognosis from stomach (gastric) adenocarcinoma. The confusion arises from overlapping abdominal symptoms, but the two diseases require entirely different diagnostic pathways and treatment approaches.
Q11. What new treatments are available for peritoneal mesothelioma in 2026?
Key 2026 developments include: the ICARuS II trial comparing NIPEC versus IV chemotherapy post-CRS-HIPEC (enrolling at MSK, Siteman, and Fred Hutchinson); the SMARTEST trial testing tremelimumab + durvalumab immunotherapy post-surgery at Princess Margaret Cancer Centre; CAR T-cell therapy targeting mesothelin protein at MSK; and the ATOMIC-Meso ADI-PEG20 trial, which quadrupled 3-year survival compared to chemotherapy alone.
For further reading, explore our related guides:
- Mesothelioma Life Expectancy — a deeper look at prognosis factors
- End Stage Mesothelioma — what to expect in advanced disease
- 5 Signs and Symptoms of Mesothelioma — early detection guide
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.