On This Page – Quick Medical Summary
Mesothelioma immunotherapy has permanently changed what is possible for patients diagnosed with this aggressive cancer. Two FDA-approved drugs — nivolumab (Opdivo) and ipilimumab (Yervoy) — now deliver survival rates more than double those of chemotherapy. The landmark 5-year CheckMate 743 data, published in the Journal of Clinical Oncology in March 2026, confirms this benefit is durable — not a temporary spike. For patients with sarcomatoid mesothelioma especially, these results represent the most dramatic improvement in outcomes this disease has ever seen.
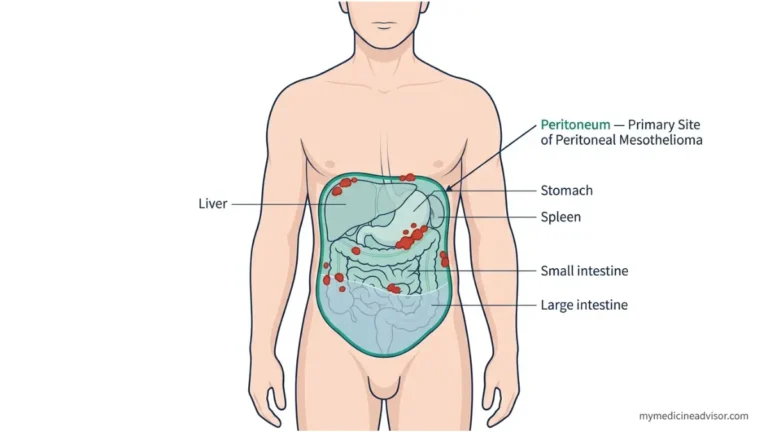
What Is Mesothelioma Immunotherapy — and How Do These 2 Drugs Actually Work?
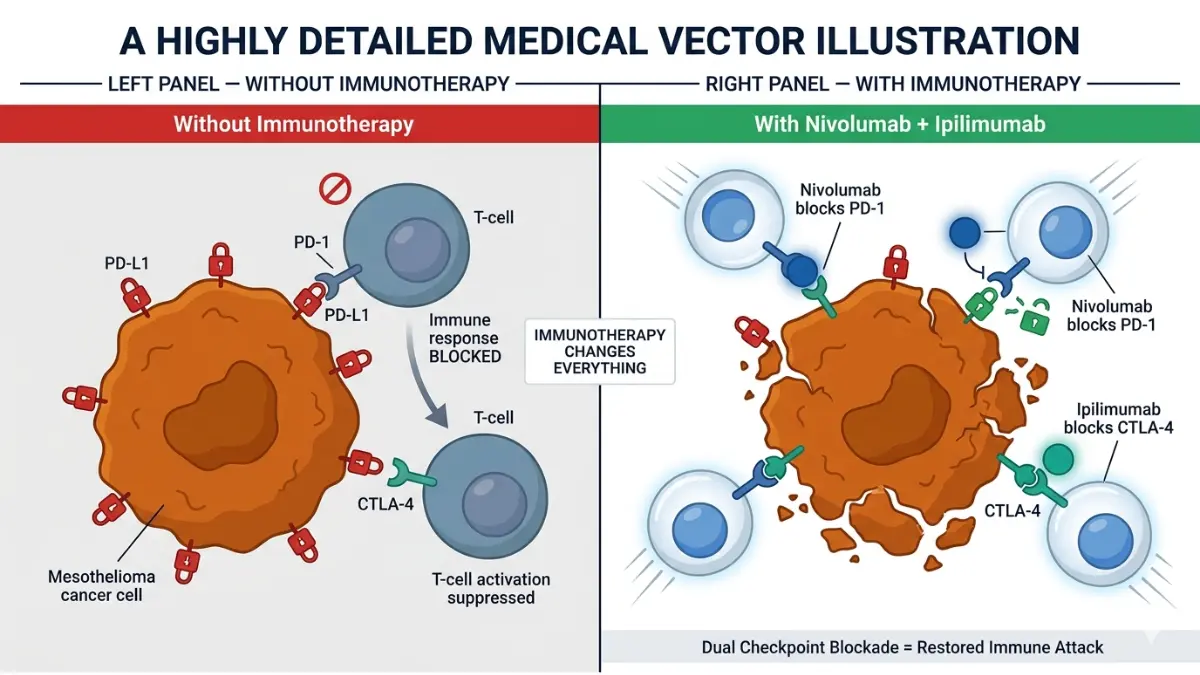
Mesothelioma is one of the most difficult cancers to treat because tumor cells actively hide from your immune system. They do this by exploiting checkpoint proteins — molecular switches that normally prevent immune cells from attacking healthy tissue.
Checkpoint inhibitors are drugs engineered to release those switches.
Understanding how immunotherapy works at a biological level can help patients and caregivers make more informed decisions with their oncology team.
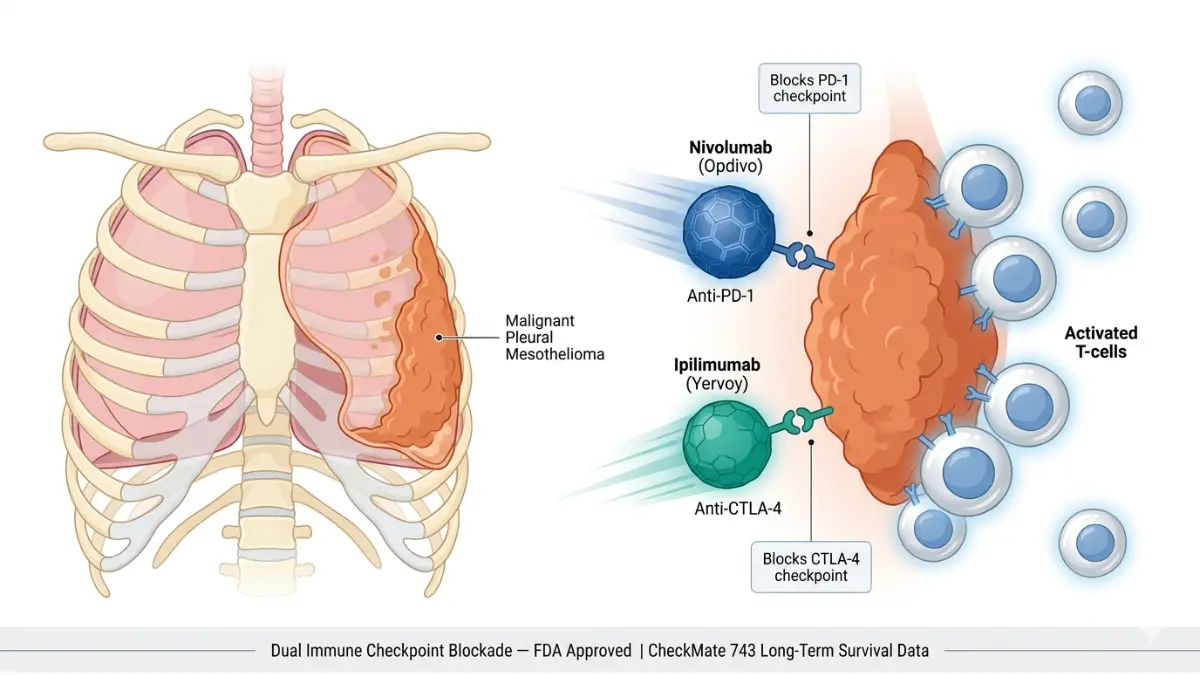
How Nivolumab (Opdivo) Works
Nivolumab targets a protein called PD-1, located on the surface of T cells — the immune system’s front-line fighters. When a mesothelioma cell sends a “do not attack” signal through PD-1, the T cell stands down.
Nivolumab blocks that signal completely. With PD-1 disabled, T cells recognize the tumor and attack it again.
How Ipilimumab (Yervoy) Works
Ipilimumab targets a different checkpoint protein called CTLA-4, which acts as a volume dial on the immune response. By blocking CTLA-4, ipilimumab amplifies the immune attack that nivolumab initiates.
Together, the two drugs deliver a dual immune blockade — significantly more powerful than either alone. Think of nivolumab as unlocking the door, and ipilimumab as forcing it wide open.
Drug Comparison at a Glance
| Drug | Brand Name | Target Protein | Role in Combination | Administration |
|---|---|---|---|---|
| Nivolumab | Opdivo | PD-1 | Removes “do not attack” signal | IV infusion every 3 weeks |
| Ipilimumab | Yervoy | CTLA-4 | Amplifies immune attack | IV infusion every 6 weeks |
The CheckMate 743 Trial — What the 5-Year Survival Data Actually Shows
The CheckMate 743 trial is the most important study ever conducted in mesothelioma treatment history. Most competing sites cite only the 2020 approval data. What they are missing is far more powerful.
What Was CheckMate 743?
It was a global, Phase 3, randomized controlled trial — the gold standard in clinical research. 605 patients across 29 countries with unresectable malignant pleural mesothelioma were enrolled. Half received nivolumab plus ipilimumab. The other half received standard platinum-based chemotherapy.
The FDA approved nivolumab plus ipilimumab for first-line mesothelioma treatment in October 2020 based on the initial results.
The 5-Year Update — March 2026 Landmark Data
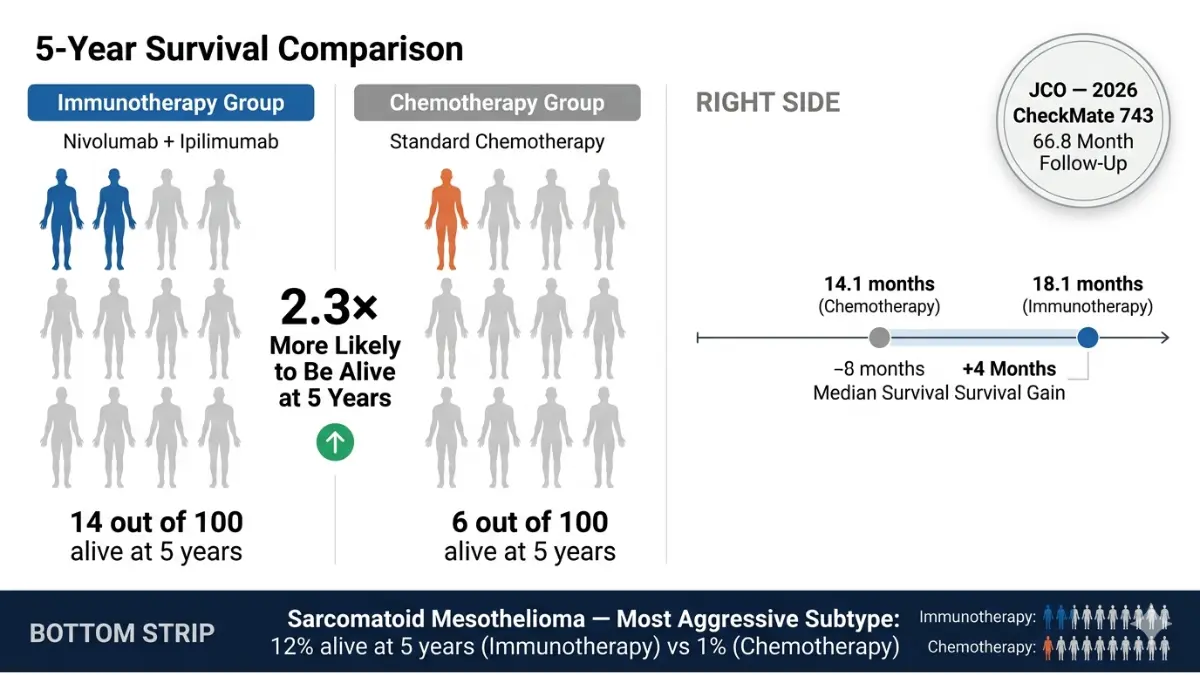
The 5-year follow-up, published in the Journal of Clinical Oncology (March 20, 2026), confirmed that the survival benefit is durable and sustained — not a short-term effect. Median follow-up reached 66.8 months.
📊 Survival Data: Immunotherapy vs Chemotherapy (CheckMate 743, 2026)
| Survival Milestone | Nivolumab + Ipilimumab | Chemotherapy | What It Means |
|---|---|---|---|
| Median Overall Survival | 18.1 months | 14.1 months | +4 months median gain |
| 2-Year Survival Rate | 41% | 27% | +14 percentage points |
| 3-Year Survival Rate | 23% | 15% | +8 percentage points |
| 5-Year Survival Rate | 14% | 6% | More than doubled |
| Sarcomatoid 5-Year Survival | 12% | 1% | 12× greater — historic |
The Sarcomatoid Breakthrough
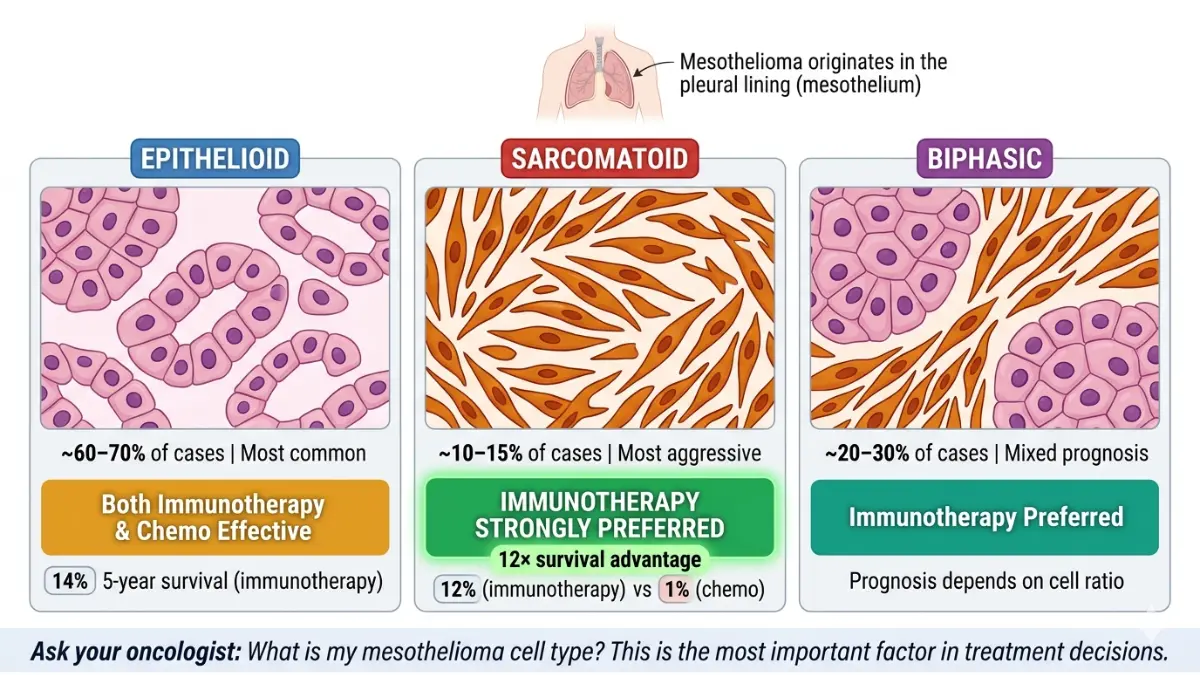
The most dramatic finding involves nonepithelioid mesothelioma — sarcomatoid and biphasic subtypes that were historically the hardest to treat and offered patients the least hope.
At 5 years, 12% of sarcomatoid patients on immunotherapy were alive — versus just 1% on chemotherapy. No prior treatment has achieved anything remotely comparable for this subtype.
Additionally, 17% of immunotherapy responders were still in active response at 5 years. In the chemotherapy arm, the number was zero.
The 3-year CheckMate 743 analysis in the Annals of Oncology had already shown durable benefit. The 5-year data now confirms this is long-term, life-changing survival.
💡 What This Means For You: If you or a loved one has been diagnosed with sarcomatoid or biphasic mesothelioma — the subtypes with historically the worst prognosis — immunotherapy is not just an option. It is the standard of care, backed by the strongest 5-year survival data in mesothelioma history.
For context on how diagnosis staging shapes treatment decisions, see our mesothelioma stages and survival guide.
Who Qualifies for Mesothelioma Immunotherapy in 2026?
Not every mesothelioma patient is automatically eligible for nivolumab plus ipilimumab. Eligibility depends on several clinical factors.
FDA-Approved Eligibility Criteria
According to the National Cancer Institute’s mesothelioma treatment PDQ, the current FDA approval covers:
- ✅ Adult patients (18 years or older)
- ✅ Unresectable malignant pleural mesothelioma (cannot be surgically removed)
- ✅ First-line treatment only (no prior systemic anticancer therapy)
- ✅ ECOG performance status ≤1 (able to perform light physical activity)
Which Cell Type Benefits Most?
Your mesothelioma cell type is the single most critical predictor of immunotherapy benefit.
| Cell Type | 5-Year Immunotherapy Survival | Recommendation |
|---|---|---|
| Sarcomatoid | 12% vs 1% on chemo | Immunotherapy strongly preferred |
| Biphasic | Significant benefit | Immunotherapy strongly preferred |
| Epithelioid | 14% vs 8% on chemo | Either option; physician and biomarker-guided |
Patient Eligibility Quick-Check
Before your specialist appointment, confirm:
- [ ] Has your mesothelioma been confirmed unresectable by a thoracic surgeon?
- [ ] Have you had no prior systemic therapy (chemo, targeted therapy)?
- [ ] Is your performance status good enough for outpatient infusions?
- [ ] Has your doctor confirmed cell type (epithelioid, sarcomatoid, or biphasic)?
- [ ] Are you aged 18 or older?
Global Approval Status — 2026
| Country / Region | Regulatory Body | Approval Status |
|---|---|---|
| United States | FDA | ✅ October 2020 |
| European Union | EMA | ✅ 2021 |
| Australia | TGA | ✅ 2021 |
| Canada | Health Canada | ✅ 2021 |
| Brazil | ANVISA | ✅ 2021 |
If you have a history of asbestos exposure and are experiencing unexplained respiratory, chest, or abdominal symptoms, use our Symptom Checker as a first step — and consult a specialist immediately.
Dosing, Administration, and Managing Side Effects
Understanding how mesothelioma immunotherapy is delivered — and what to expect physically — prepares both patients and caregivers for what is ahead.
How Treatment Is Given
Both drugs are administered as intravenous (IV) infusions in an outpatient oncology clinic. No hospital admission is required for the infusions themselves.
Treatment continues for up to 2 years — or until disease progression, unacceptable toxicity, or the patient chooses to stop.
Official Dosing Schedule (FDA-Approved):
- Nivolumab: 360 mg every 3 weeks
- Ipilimumab: 1 mg/kg every 6 weeks
Common Side Effects (Occurring in ≥20% of Patients)
| Side Effect | Clinical Frequency | Practical Management |
|---|---|---|
| Fatigue | Very common | Prioritize rest; use our Sleep Calculator to optimize sleep timing during treatment |
| Musculoskeletal pain | Common | Low-impact movement; discuss safe pain relief with your care team |
| Rash / Skin reactions | Common | Report early to oncology nurse; topical steroids often effective |
| Diarrhea | Common | Stay well hydrated — our Water Intake Calculator helps you calculate daily fluid targets |
| Nausea | Common | Small, frequent meals; prescription anti-nausea medications available |
| Decreased appetite | Common | High-calorie, high-protein focus; our Protein Intake Calculator can help maintain adequate nutrition |

Serious Immune-Related Adverse Events (irAEs)
Dual checkpoint blockade can cause the immune system to attack healthy organs. These are called immune-related adverse events (irAEs) and require prompt medical attention.
A 2023 real-world study of 184 mesothelioma patients treated with nivolumab plus ipilimumab outside of clinical trials found:
- 27.7% experienced Grade 3–4 (severe) adverse events
- 25% discontinued at least one drug due to toxicity
- Older patients carried a meaningfully higher toxicity risk
🚨 Contact Your Care Team Immediately If You Experience:
- Diarrhea exceeding 4 bowel movements above your baseline per day
- Chest pain, shortness of breath, or persistent cough
- Yellowing of skin or whites of the eyes (jaundice)
- Severe skin blistering or peeling
- Sudden confusion, severe headache, or vision changes
💡 Key Takeaway: Side effects from mesothelioma immunotherapy are manageable in most patients — but early reporting is critical. Never wait for symptoms to worsen before contacting your oncology team.
For a side-by-side comparison of immunotherapy and chemotherapy toxicities, see our full guide on mesothelioma chemotherapy side effects.
Mesothelioma Immunotherapy vs Chemotherapy — Which Is Actually Better?
This is the question every patient asks the moment they are diagnosed. The honest, evidence-based answer is: it depends entirely on your cell type.
Head-to-Head Comparison Table
| Factor | Nivolumab + Ipilimumab | Chemotherapy (Pemetrexed + Platinum) |
|---|---|---|
| Median Survival | 18.1 months | 14.1 months |
| 5-Year Survival | 14% | 6% |
| Objective Response Rate | 39% | 44% |
| Durable Responses at 5 Yrs | 17% ongoing | 0% ongoing |
| Best Subtype | Sarcomatoid, Biphasic | Epithelioid (certain profiles) |
| Administration | IV infusion, up to 2 years | IV infusion, 6 cycles maximum |
| Primary Risk | Immune-related adverse events | Nausea, bone marrow suppression |
The Second FDA-Approved Option: Pembrolizumab + Chemotherapy (2024)
In September 2024, the FDA approved a second immunotherapy-based regimen: pembrolizumab (Keytruda) combined with pemetrexed and platinum chemotherapy. This combination achieved a 52% objective response rate — the highest ever recorded in any first-line mesothelioma trial.
This approach may be preferable for epithelioid mesothelioma patients where a high initial tumor shrinkage rate is the priority.
The Role of Biomarkers — What Your Blood May Predict
The 5-year JCO analysis published in 2026 revealed that monocytic myeloid-derived suppressor cell (M-MDSC) levels predict immunotherapy response. Patients with high M-MDSC levels had worse outcomes on dual checkpoint blockade.
PD-L1 expression also plays a role, though it is not yet a definitive eligibility criterion.
💡 What This Means For You: Ask your oncologist about biomarker testing before treatment begins. Your PD-L1 and M-MDSC profile could meaningfully influence which of the two FDA-approved regimens gives you the best chance.
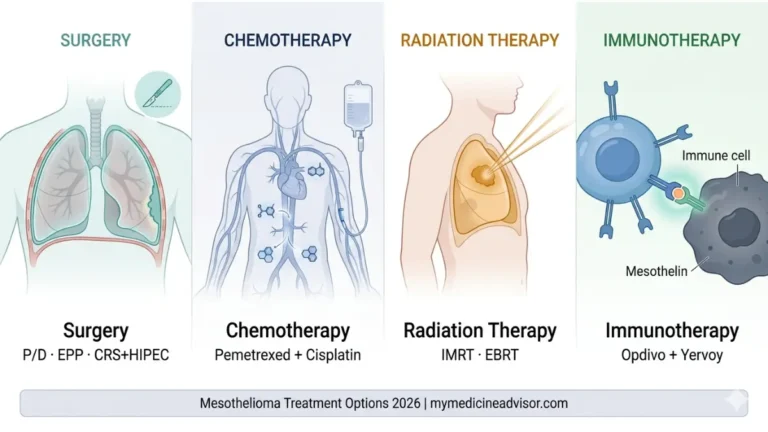
For the full landscape of available options — surgery, chemotherapy, radiation, and immunotherapy compared — see our comprehensive mesothelioma treatment options guide.
Clinical Trials, Insurance Coverage, and Your Next Steps
A mesothelioma diagnosis demands immediate, informed action. Here is exactly what to prioritize.
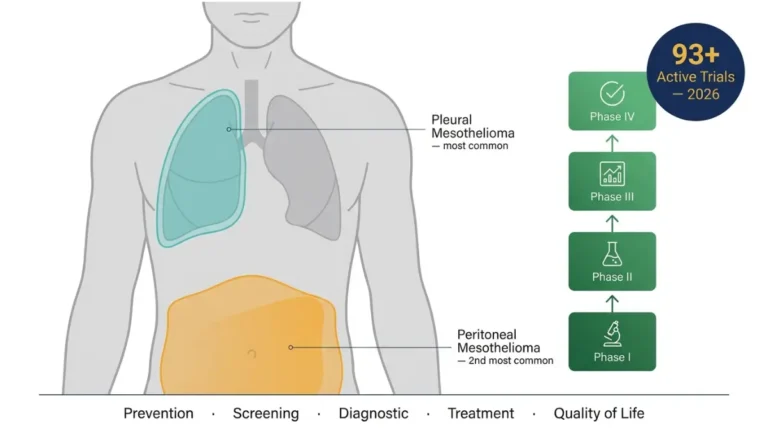
Active Clinical Trials in 2026
As of April 2026, 92 mesothelioma clinical trials are actively recruiting participants across the United States, searchable on ClinicalTrials.gov. Key trials your oncologist should know about:
| Trial | Focus | What It Showed |
|---|---|---|
| ATOMIC-Meso | Arginine depletion + non-epithelioid disease | Quadrupled 3-year survival vs chemo |
| Perioperative Immunotherapy | Nivolumab ± ipilimumab before/after surgery | Safe, feasible; ctDNA predicts response (Nature Medicine, 2025) |
| KEYNOTE-483 | Pembrolizumab + chemotherapy | 52% response rate — highest ever recorded |
| CAR-T Cell Trials | Next-gen immunotherapy | Early-phase, enrollment open at major cancer centers |
Always ask your oncologist: “Am I eligible for any currently recruiting mesothelioma trials?” Enrollment at specialist centers like MD Anderson, Memorial Sloan Kettering, or Penn Medicine often gives access to therapies years before they reach general oncology practice.
If you want to explore your personal genetic risk factors for cancer susceptibility — including BAP1 mutations linked to mesothelioma — our Genetic Risk Assessment Tool can help identify inherited risk patterns to discuss with your care team.
Insurance Coverage and Cost Access
Because nivolumab plus ipilimumab is FDA-approved for malignant pleural mesothelioma, major U.S. insurers and Medicare Part B are required to cover it under existing oncology coverage rules. Prior authorization is standard and typically approved for this indication.
Financial Assistance Resources:
- Bristol Myers Squibb (BMS) Access Support — direct patient assistance for Opdivo and Yervoy costs
- CancerCare Financial Assistance — grants and co-pay support for US-based cancer patients
- NeedyMeds.org — connects patients to manufacturer patient assistance programs nationwide
10 Questions to Bring to Your Oncologist
According to the American Cancer Society’s immunotherapy resource, patients who actively engage with treatment decisions consistently achieve better outcomes. Print this list:
- What is my exact cell type — epithelioid, sarcomatoid, or biphasic?
- Is my mesothelioma confirmed unresectable, and has that been verified by a surgeon?
- Is nivolumab + ipilimumab or pembrolizumab + chemo the better choice for my profile?
- What are my PD-L1 expression and M-MDSC levels?
- Am I eligible for any currently recruiting clinical trials?
- What are the most likely side effects for someone my age and health status?
- What happens if I must stop immunotherapy early — do I lose the benefit?
- How will we monitor whether the drugs are working?
- Should I be seen at a specialized mesothelioma center alongside my local oncologist?
- What financial assistance programs is your practice able to help me access?
For long-term prognosis data to guide your decision-making, our mesothelioma survival rate guide provides a full breakdown by stage, cell type, and treatment received.
Frequently Asked Questions — Mesothelioma Immunotherapy 2026
1. What is mesothelioma immunotherapy?
Mesothelioma immunotherapy uses drugs called checkpoint inhibitors to help your immune system identify and destroy mesothelioma cells. The two FDA-approved drugs are nivolumab (Opdivo) and ipilimumab (Yervoy), used together as first-line treatment.
2. What are nivolumab and ipilimumab?
Nivolumab (Opdivo) blocks the PD-1 protein to restore your immune system’s ability to attack cancer cells. Ipilimumab (Yervoy) blocks CTLA-4 to amplify that immune response. Combined, they are the only dual checkpoint blockade regimen FDA-approved for mesothelioma.
3. Is immunotherapy better than chemotherapy for mesothelioma?
For sarcomatoid and biphasic subtypes, yes — dramatically. Five-year survival was 12% on immunotherapy versus just 1% on chemotherapy in nonepithelioid patients. For epithelioid disease, both are valid options, and the choice depends on biomarker profiles and physician judgment.
4. What are the survival rates for mesothelioma immunotherapy?
The March 2026 CheckMate 743 5-year data shows 14% of immunotherapy patients alive at 5 years versus 6% on chemotherapy — more than double. Median overall survival was 18.1 months versus 14.1 months for chemotherapy.
5. Who qualifies for mesothelioma immunotherapy?
Adults with unresectable malignant pleural mesothelioma who have received no prior systemic therapy and have an ECOG performance status of ≤1. Sarcomatoid and biphasic subtypes benefit most significantly.
6. What are the side effects of nivolumab and ipilimumab?
Common side effects include fatigue, rash, diarrhea, nausea, and musculoskeletal pain. Serious immune-related adverse events — including colitis, hepatitis, and pneumonitis — affect approximately 27.7% of patients in real-world settings.
7. How is mesothelioma immunotherapy given?
Both drugs are given as outpatient IV infusions. Nivolumab is infused every 3 weeks; ipilimumab every 6 weeks. Treatment continues for up to 2 years unless disease progression or intolerable side effects occur.
8. What is CheckMate 743?
CheckMate 743 is the landmark Phase 3 clinical trial that led to FDA approval of nivolumab plus ipilimumab for mesothelioma. It enrolled 605 patients in 29 countries and demonstrated superior survival versus chemotherapy at 2, 3, and now 5 years.
9. Does mesothelioma immunotherapy work for sarcomatoid type?
Yes — it is the most effective treatment ever documented for sarcomatoid mesothelioma. The 5-year survival rate was 12% on immunotherapy versus just 1% on chemotherapy, a 12-fold improvement that is unprecedented in mesothelioma oncology.
10. Is mesothelioma immunotherapy covered by insurance?
Yes. Because nivolumab plus ipilimumab is FDA-approved, major U.S. insurers and Medicare Part B are legally required to cover it. Prior authorization is standard and typically granted. Bristol Myers Squibb also offers patient financial assistance directly.
11. Are there new mesothelioma immunotherapy clinical trials in 2026?
Yes. As of April 2026, 92 mesothelioma trials are actively recruiting across the United States. Key studies include perioperative immunotherapy (before and after surgery) and CAR-T cell therapy approaches for advanced disease. Ask your oncologist at your next visit.
📋 Medical Disclaimer: This article is intended for educational and informational purposes only and does not constitute medical advice, diagnosis, or treatment. Individual outcomes vary significantly based on mesothelioma subtype, stage, performance status, and other clinical factors. Always consult a board-certified oncologist or mesothelioma specialist before making any treatment decisions. If you or a loved one has been exposed to asbestos and are experiencing symptoms, seek evaluation from a qualified medical professional without delay.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.