On This Page – Quick Medical Summary
Non-small cell lung cancer (NSCLC) and small cell lung cancer (SCLC) differ in cell size, growth speed, staging, and treatment. NSCLC accounts for 80–85% of cases and grows more slowly; SCLC makes up 10–15%, spreads aggressively, and is almost exclusively caused by heavy smoking. The difference between NSCLC and SCLC determines everything — your treatment plan, your prognosis, and which 2026 breakthroughs apply to you.
What Are NSCLC and SCLC? The Core Biology Behind Both Diagnoses
James, a 62-year-old retired electrician and lifelong smoker, was told he had “small cell.” His colleague, a non-smoker diagnosed at the same hospital the same week, had “non-small cell.” Same organ. Wildly different diseases — different speeds, different treatment paths, different outcomes.
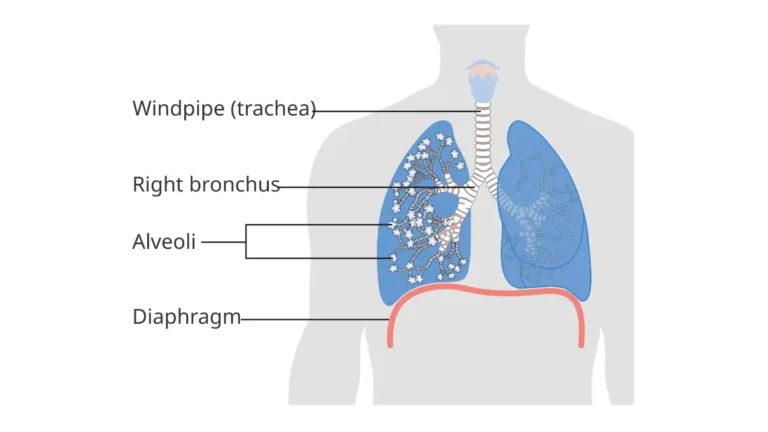
To understand exactly how lung cancer begins and why type matters, start with the comprehensive overview at what is lung cancer.
What Is Non-Small Cell Lung Cancer (NSCLC)?
NSCLC is the most common form of lung cancer, accounting for approximately 85% of all cases in the United States. It grows more slowly than SCLC, which means early detection is more achievable.
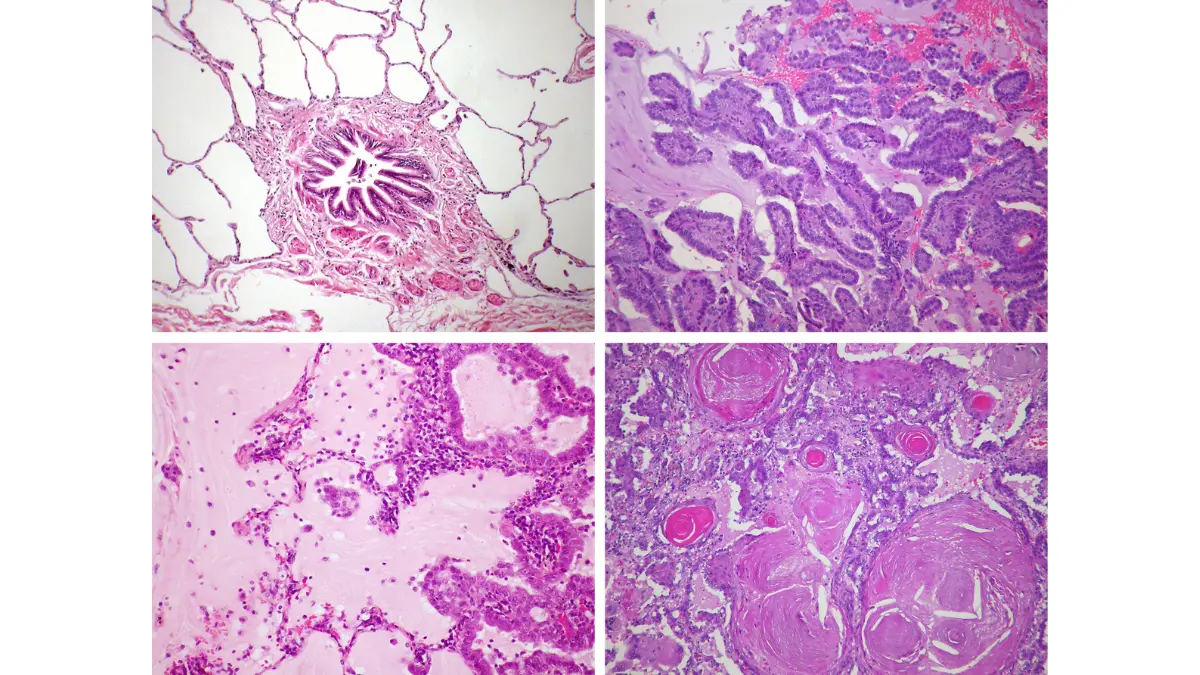
NSCLC has three main subtypes:
| Subtype | Location in Lung | % of NSCLC Cases |
|---|---|---|
| Adenocarcinoma | Outer lung regions (glandular cells) | ~40% |
| Squamous Cell Carcinoma | Central airways (bronchi) | ~30% |
| Large Cell Carcinoma | Anywhere in the lung | ~10–15% |
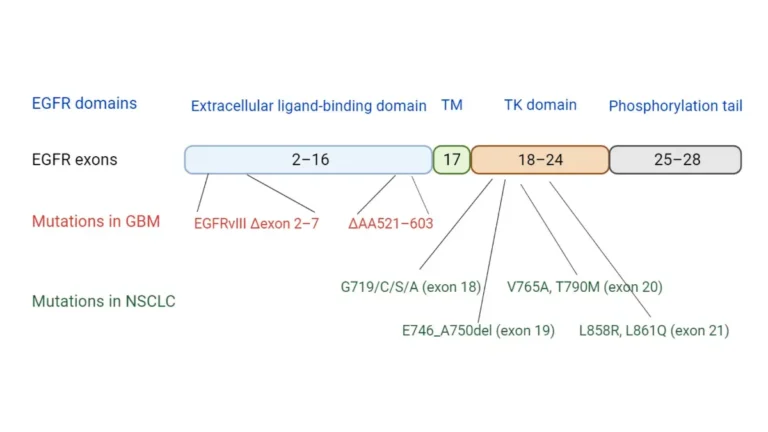
Adenocarcinoma is rising sharply in never-smokers — particularly among Asian women — driven by specific gene mutations like EGFR, ALK, and KRAS. This makes molecular testing essential before any treatment decision.
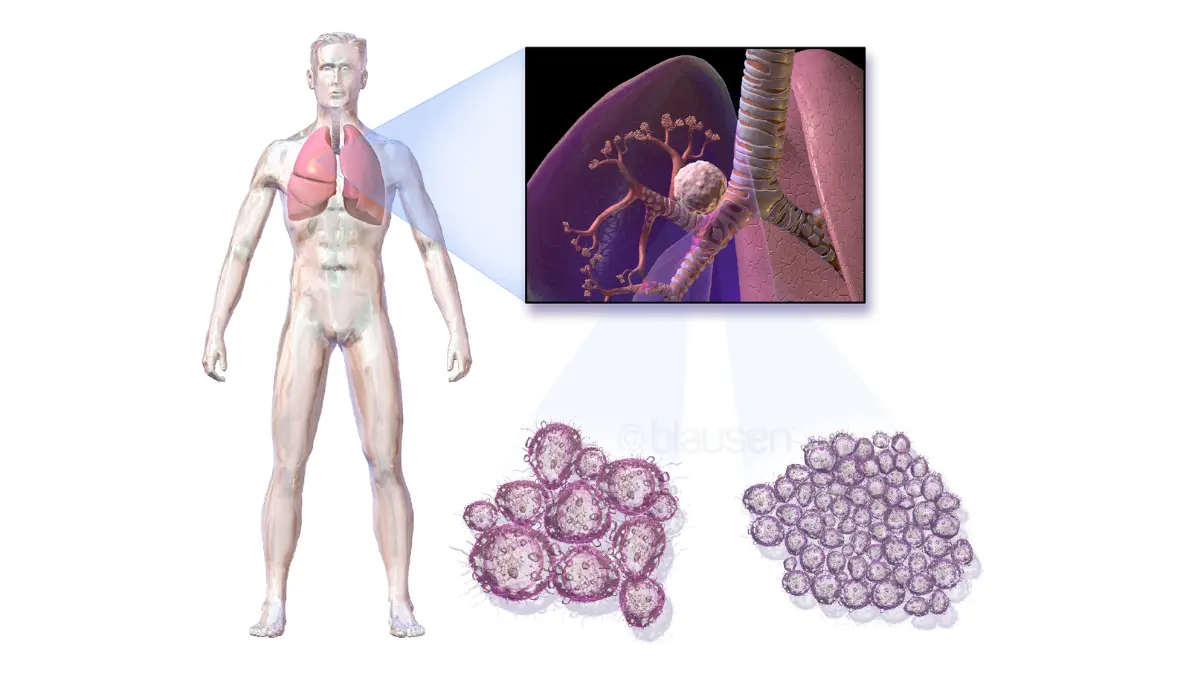
What Is Small Cell Lung Cancer (SCLC)?
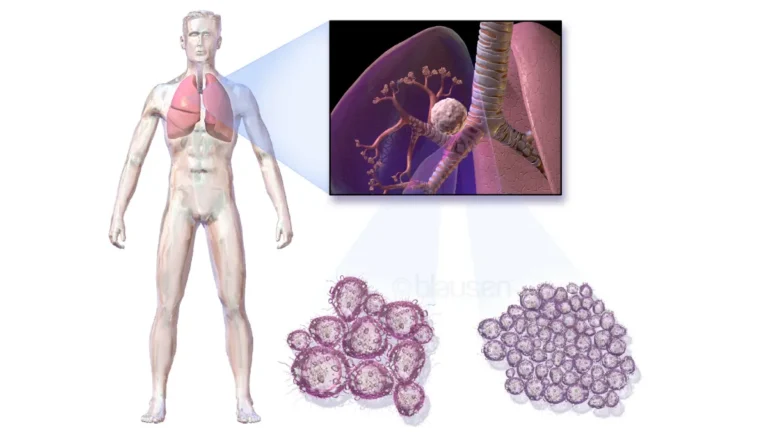
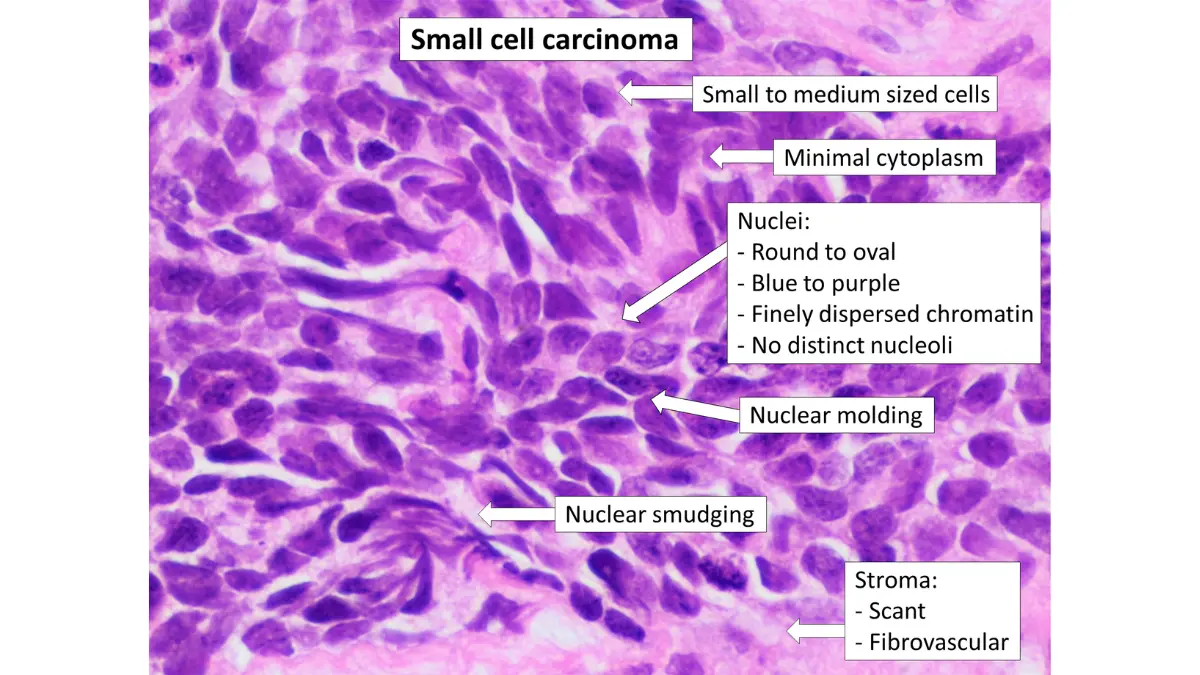
SCLC accounts for roughly 10–15% of lung cancer diagnoses. Under a microscope, its cells appear small, round, and densely packed — resembling oat grains — which is why it is also called “oat cell cancer.” SCLC is a neuroendocrine malignancy, biologically distinct from NSCLC in origin, not just appearance.
SCLC has two subtypes:
- Small cell carcinoma — the more common form; cells appear flat under the microscope
- Combined small cell carcinoma — a tumor containing both SCLC and NSCLC cells
SCLC grows aggressively, spreads to lymph nodes and distant organs rapidly, and is almost exclusively linked to heavy, long-term cigarette smoking.
What About Mixed SCLC/NSCLC? (The Type No One Talks About)
Between 5–28% of SCLC cases contain both small cell and non-small cell components in the same tumor. This “combined” subtype can behave differently from pure SCLC and may respond to a broader range of therapies. If you’re experiencing unexplained respiratory or systemic symptoms, use our Symptom Checker to document them accurately before your oncology appointment.
NSCLC vs SCLC — The Complete Side-by-Side Comparison (2026)
No competitor article provides a fully comprehensive comparison table. Here is the definitive breakdown.
Master Comparison Table: Non-Small Cell vs Small Cell Lung Cancer
| Feature | NSCLC | SCLC |
|---|---|---|
| Prevalence | 80–85% of lung cancers | 10–15% of lung cancers |
| Cell appearance | Large, distinct glandular or squamous cells | Small, round, densely packed (“oat”) cells |
| Growth speed | Slower; may grow for years before spreading | Rapid; often metastatic at time of diagnosis |
| Staging system | Stage I, II, III, IV | Limited Stage / Extensive Stage |
| Primary treatment | Surgery, targeted therapy, immunotherapy | Chemotherapy + immunotherapy (surgery rarely used) |
| Smoking link | Strong, but includes significant non-smoker cases | Almost exclusively heavy smokers |
| 5-year survival (all stages) | 28% | 7% |
| Genetic/molecular testing | Critical — EGFR, ALK, KRAS, HER2, ROS1, BRAF | Less targetable; molecular subtypes emerging (SCLC-A/N/P/I) |
| 2026 key breakthrough | Zongertinib (HER2, FDA Feb 2026), FLAURA2 OS data | Tarlatamab (Imdelltra) — 40% death risk reduction in Phase 3 |
Key Takeaways:
- NSCLC is more common but slower. It offers more treatment options, particularly when caught at an early stage.
- SCLC is rarer but far more aggressive. It is almost always diagnosed at an advanced stage.
- Genetic testing is non-negotiable for NSCLC. Missing a targetable mutation means missing the most effective therapy available.
- 2026 has fundamentally changed SCLC treatment. Tarlatamab is now the new standard of care for relapsed SCLC.
Which Type of Lung Cancer Is More Dangerous?
SCLC is significantly more dangerous than NSCLC. Its 5-year overall survival rate of just 7% versus 28% for NSCLC reflects how rapidly it invades the body. The majority of SCLC patients experience relapse within 12 months of completing first-line treatment.
That said, NSCLC diagnosed at Stage IV carries a grim 9% survival rate — which reinforces why early screening changes outcomes for both types.
Symptoms, Risk Factors & Who Gets Each Type
NSCLC vs SCLC Symptoms: What’s the Same, What’s Different
Both types share the same core warning signs — and both are notoriously silent in early stages. Read our complete guide to early lung cancer warning signs for a full symptom breakdown.
Shared symptoms of both NSCLC and SCLC:
- Persistent cough that worsens or doesn’t resolve
- Shortness of breath or new-onset wheezing
- Chest pain that deepens with breathing or coughing
- Coughing up blood (hemoptysis)
- Unexplained significant weight loss
- Ongoing fatigue with no clear cause
SCLC-specific symptoms (due to faster spread):
- Bone pain — from early skeletal metastases
- Facial or arm swelling — from Superior Vena Cava (SVC) syndrome
- Confusion, seizures, or sudden balance problems — from brain metastases
- All symptoms tend to appear and worsen faster than in NSCLC
NSCLC-specific pattern:
- Often entirely asymptomatic until Stage III or IV
- Adenocarcinoma in non-smokers may only be found incidentally on a CT scan performed for another reason
Risk Factors: NSCLC vs SCLC
Shared risk factors:
- Cigarette smoking — responsible for approximately 80% of all lung cancer deaths in the U.S., according to the American Lung Association
- Secondhand smoke exposure
- Radon gas in the home
- Asbestos or occupational chemical exposure
- Family history of lung cancer
- Long-term air pollution exposure
SCLC-specific: Almost exclusively a disease of heavy, long-term smokers (typically 1+ pack per day). SCLC in never-smokers is extremely rare.
NSCLC and never-smokers: A clinically significant proportion of adenocarcinoma cases — especially in women of Asian descent — are EGFR-mutation driven with zero smoking history. This group responds remarkably well to targeted oral therapies.
> Know your personal risk: Use our free Genetic Risk Assessment Tool to evaluate your lung cancer risk profile based on smoking history, family genetics, and environmental exposures.
Staging Explained — The Critical Difference Most Articles Miss
The most misunderstood aspect of non-small cell vs small cell lung cancer is why they use entirely different staging systems. Most competitor articles skip this explanation entirely.
NSCLC Staging: Stage I Through Stage IV
NSCLC uses the standard TNM (Tumor, Node, Metastasis) staging system. According to NCI SEER cancer statistics, survival rates shift dramatically by stage:
| NSCLC Stage | Description | 5-Year Survival Rate |
|---|---|---|
| Stage I | Localized — confined to the lung only | 64% |
| Stage II | Spread to nearby lymph nodes | 36% |
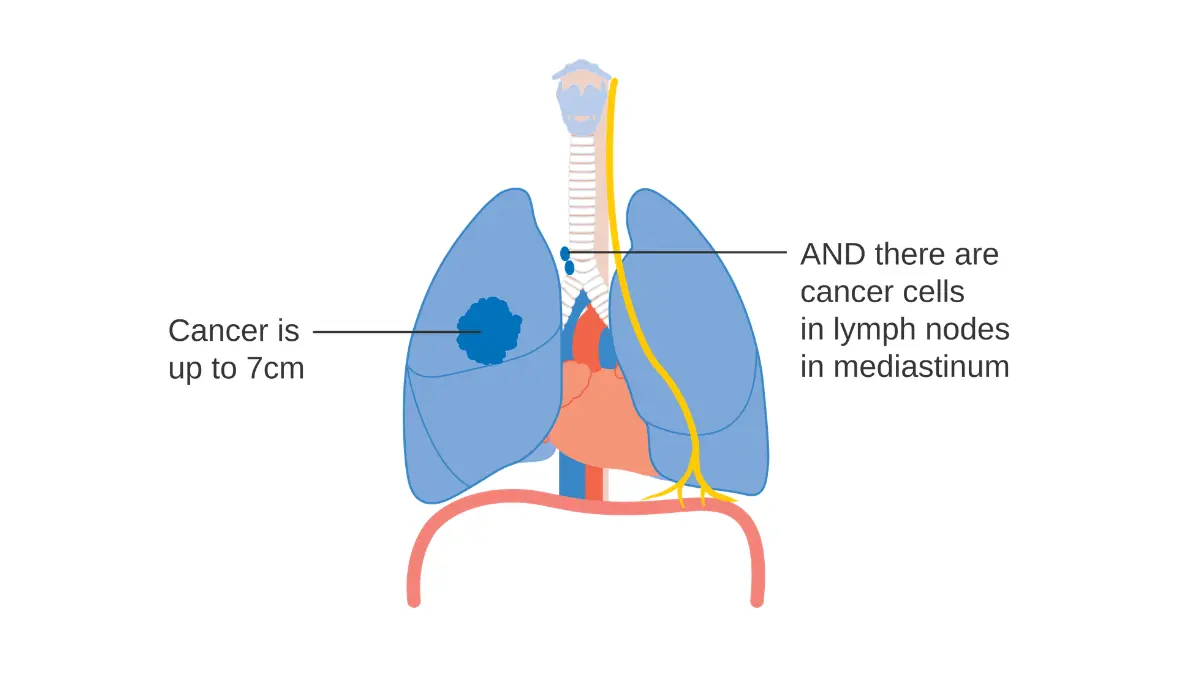
| Stage III | Spread to chest structures or regional lymph nodes | 26% |
| Stage IV | Spread to the brain, liver, bones, or opposite lung | 9% |
This is why Stage I lung cancer survival outcomes are so dramatically superior — getting diagnosed early via screening is genuinely life-saving. The ASCO staging criteria for NSCLC details the full TNM criteria oncologists use.
SCLC Staging: Limited vs. Extensive Stage
SCLC uses a simpler binary system because it has almost always spread far beyond the original tumor site by the time symptoms appear:
- Limited Stage (LS-SCLC): Cancer is confined to one lung and nearby lymph nodes within the chest. With chemoradiation, approximately 30% 5-year survival is achievable.
- Extensive Stage (ES-SCLC): Cancer has spread to the other lung, distant lymph nodes, or other organs. Under 10% 5-year survival. This is where the majority of SCLC patients are diagnosed.
For the full SCLC prognosis breakdown, see our dedicated guides on SCLC survival rates and treatment costs and the latest small cell lung cancer survival rates by stage.
> What This Means For You:
- For NSCLC: your exact stage determines whether surgery is an option and which systemic therapies apply.
- For SCLC: limited-stage diagnosis opens access to chemoradiation with curative intent — extensive-stage shifts focus to systemic control and quality of life.
- Always ask your oncologist: “What is my exact stage, and what does the survival data show for patients at this stage with my subtype?”
Treatment Differences — Including Every 2026 FDA-Approved Breakthrough
NSCLC Treatment Options in 2026
NSCLC offers more treatment options than any other lung cancer type — and 2026 has added significant new approvals. Our complete guide to FDA-approved lung cancer drugs in 2026 documents every current approved therapy.
Surgery (Early-Stage NSCLC — Stage I and II):
- Surgical resection remains the gold standard when cancer has not spread
- Over 90% of early-stage lung surgeries at major NCI-designated centers now use minimally invasive VATS (Video-Assisted Thoracic Surgery) or robotic-assisted techniques
- Earlier surgery means earlier recovery and faster access to adjuvant therapy if needed
Chemotherapy:
- Standard backbone remains platinum-based regimens (cisplatin or carboplatin + pemetrexed)
- Used adjuvantly after surgery, concurrently with radiation, or alongside immunotherapy
- Full side effect management strategies are covered in our guide to chemotherapy in 2026
Targeted Therapy for NSCLC: Precision Medicine by Gene Mutation
This is where NSCLC treatment has advanced furthest. Comprehensive molecular testing before treatment is no longer optional — it is the standard of care. The NCI’s NSCLC treatment guidelines explicitly require full genomic profiling before initiating any systemic therapy.
| Gene Mutation | Approved Drug (2026) | Key Clinical Data |
|---|---|---|
| EGFR (exon 19/21) | Osimertinib + chemo (FLAURA2) | 47.5-month median OS — NEJM, January 2026 |
| HER2 mutation | Zongertinib (Hernexeos) | FDA accelerated approval Feb 26, 2026; 75% response rate |
| ALK+ | Alectinib (adjuvant) | Substantial DFS benefit in resected ALK+ NSCLC |
| KRAS G12C | Sotorasib, Adagrasib | Both approved for previously treated advanced NSCLC |
| ROS1 | Entrectinib, Crizotinib | Durable intracranial responses in ROS1+ disease |
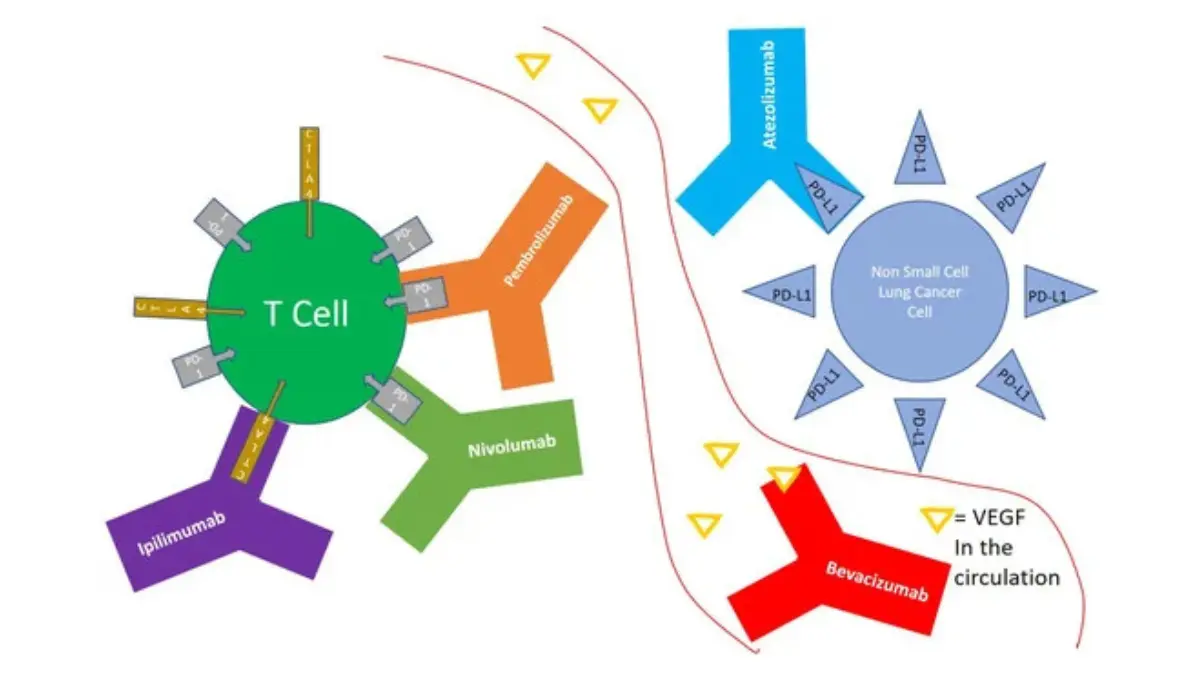
Immunotherapy for NSCLC:
- PD-L1 testing determines eligibility for pembrolizumab (Keytruda) as first-line monotherapy (if PD-L1 ≥ 50%)
- Checkpoint inhibitors are now a standard component of first-line treatment for most NSCLC patients without targetable mutations
- Learn how immunotherapy works to fight cancer cells — and who responds best
- Emerging TIL (Tumor-Infiltrating Lymphocyte) therapy is showing early promise, as documented in MSK’s 2026 lung cancer treatment update
SCLC Treatment Options in 2026
SCLC historically had the fewest treatment options of any major lung cancer type. The NCI patient guide to SCLC treatment is the most comprehensive reference for patients navigating this diagnosis.
Standard First-Line Treatment:
- Limited Stage: Concurrent platinum-etoposide chemotherapy + thoracic radiation, followed by durvalumab (immunotherapy) maintenance — based on ADRIATIC trial data, 2024–2025
- Extensive Stage: Platinum-etoposide + atezolizumab or durvalumab — real-world median OS has improved to approximately 13.2 months with immunotherapy combinations
Prophylactic Cranial Irradiation (PCI):
- SCLC cells metastasize to the brain in a majority of patients
- Selected limited-stage SCLC patients receive preventive brain radiation to reduce this risk
- Not all patients qualify — discuss specific eligibility criteria with your radiation oncologist
Tarlatamab (Imdelltra): The 2026 SCLC Breakthrough Every Patient Needs to Know
This is the most important SCLC development in 2026. No major competitor article discusses this in patient-accessible language.
Tarlatamab is a DLL3/CD3 bispecific T-cell engager — an immunotherapy that physically bridges immune T-cells directly to cancer cells expressing the DLL3 protein found on SCLC tumor surfaces. In the DeLLphi-304 Phase 3 trial, tarlatamab demonstrated a 40% reduction in the risk of death compared to standard chemotherapy in patients with relapsed extensive-stage SCLC. It is now the established standard of care for this setting, as reviewed in this peer-reviewed PMC analysis of emerging SCLC strategies.
For patients relapsing after first-line platinum-etoposide, ask your oncologist specifically about tarlatamab eligibility.
> What This Means For You:
- NSCLC patients: Request a full molecular panel — EGFR, ALK, HER2, KRAS, ROS1, BRAF, MET, NTRK, and PD-L1 — before starting any treatment. This single step could qualify you for oral targeted therapy with dramatically superior outcomes. Check the FDA’s oncology approvals tracker for the latest approved options.
- SCLC patients: Ask your oncologist about tarlatamab eligibility after first-line therapy. For limited-stage patients, ask specifically whether concurrent chemoradiation with durvalumab maintenance is appropriate for your case.
Diagnosis, Screening & Your 5-Step Patient Action Guide
How Are NSCLC and SCLC Diagnosed?
Both types require imaging followed by tissue sampling — but the diagnostic urgency differs significantly.
The diagnostic sequence:
- Chest X-ray — often the first step; misses small or early-stage tumors frequently
- Low-dose CT scan (LDCT) — far more sensitive; the standard for detecting early lung cancer. See our guide to what CT scan abnormalities mean and what happens next
- PET scan — determines metabolic activity and whether cancer has spread to other organs
- Biopsy — bronchoscopy, CT-guided needle biopsy, or surgical sampling — confirms type and subtype through pathological examination
- Molecular/biomarker testing (NSCLC) — runs simultaneously or immediately after biopsy; identifies actionable gene mutations and PD-L1 expression level
The pathologist’s report distinguishes NSCLC from SCLC by cellular appearance — large structured cells (NSCLC) versus small densely packed oat-like cells (SCLC). This distinction is confirmed by immunohistochemistry staining.
Who Should Get Screened for Lung Cancer in 2026?
Annual low-dose CT lung cancer screening is recommended under current USPSTF guidelines if you meet all three criteria:
- Age 50–80 years old
- Currently smoke or quit within the past 15 years
- 20+ pack-year history (e.g., 1 pack/day × 20 years, or 2 packs/day × 10 years)
> Critical statistic: Screening-detected NSCLC at Stage I carries a 64% five-year survival rate. Waiting until symptoms appear typically means a Stage IV diagnosis — where survival drops to 9%.
Find active clinical trials for both NSCLC and SCLC through ClinicalTrials.gov — many Phase 2 and Phase 3 studies are open to newly diagnosed patients.
Your 5-Step Action Plan After a Lung Cancer Diagnosis
- Confirm your exact type and subtype. NSCLC vs SCLC, then your specific histological subtype (adenocarcinoma vs squamous vs limited-stage SCLC, etc.)
- Request comprehensive molecular testing if NSCLC. This step must be completed before chemotherapy begins — treatment can alter tumor tissue and compromise testing accuracy
- Consult a thoracic oncology specialist. Seek a second opinion at an NCI-designated comprehensive cancer center whenever possible
- Search for active clinical trials. New therapies available through trials may outperform current standard of care for your specific subtype and stage
- Track your symptoms systematically. Use our Symptom Checker before every oncology appointment to document changes, new symptoms, and treatment responses your care team needs to know
Frequently Asked Questions: Non-Small Cell vs Small Cell Lung Cancer
1. What is the main difference between non-small cell and small cell lung cancer?
NSCLC cells are larger with distinct glandular or squamous patterns; it makes up 80–85% of cases and grows slowly. SCLC cells are small and round, account for 10–15% of cases, and are highly aggressive with rapid spread.
2. Which type of lung cancer is more dangerous — SCLC or NSCLC?
SCLC is significantly more dangerous, with a 5-year overall survival rate of just 7% compared to 28% for NSCLC. Most SCLC patients are diagnosed at the extensive stage, when the cancer has already spread widely.
3. What is the survival rate for NSCLC vs SCLC?
NSCLC survival ranges from 64% (Stage I) to 9% (Stage IV). SCLC survival is approximately 30% for limited-stage disease and under 10% for extensive-stage disease.
4. Can non-small cell lung cancer be cured?
Yes — Stage I NSCLC has a 64% five-year survival rate and surgery can be curative. Even Stage III NSCLC can achieve long-term remission with combined chemoradiation and immunotherapy maintenance.
5. Why is SCLC staged as “limited” vs “extensive” instead of Stage I–IV?
SCLC spreads so rapidly that standard TNM staging has limited clinical utility. The limited/extensive binary system allows oncologists to make treatment decisions immediately — since SCLC requires urgent intervention.
6. What are the latest NSCLC treatments approved in 2026?
Key 2026 approvals include zongertinib (Hernexeos) for HER2-mutant NSCLC (FDA accelerated approval, February 2026) and updated data confirming osimertinib-chemotherapy combination (FLAURA2: 47.5-month median OS) as frontline standard for EGFR-mutated NSCLC.
7. Is SCLC always caused by smoking?
Almost always. SCLC in never-smokers is extremely rare. In contrast, NSCLC adenocarcinoma occurs in a meaningful proportion of never-smokers — particularly those with EGFR mutations.
8. What is tarlatamab and why does it matter for SCLC patients?
Tarlatamab (Imdelltra) is a DLL3/CD3 bispecific T-cell engager. The DeLLphi-304 Phase 3 trial demonstrated a 40% reduction in the risk of death versus chemotherapy in relapsed extensive-stage SCLC — establishing it as the new second-line standard of care in 2026.
9. What genetic tests should NSCLC patients request before starting treatment?
All NSCLC patients should receive comprehensive molecular profiling for EGFR, ALK, ROS1, KRAS G12C, HER2, BRAF, MET, RET, and NTRK mutations — plus PD-L1 expression testing. This panel directly determines the optimal treatment path.
10. Can someone have both SCLC and NSCLC at the same time?
Yes — between 5–28% of SCLC cases are “combined” tumors containing both SCLC and NSCLC cells. This mixed subtype behaves differently from pure SCLC and requires specific pathological identification to guide treatment.
11. Who qualifies for annual lung cancer screening in 2026?
Adults aged 50–80 who currently smoke or quit within the past 15 years and have a 20+ pack-year smoking history qualify for annual low-dose CT screening per current USPSTF guidelines.
⚠️ Disclaimer: This article is intended for educational and informational purposes only. It does not constitute medical advice, diagnosis, or treatment recommendations. Always consult a board-certified oncologist or qualified healthcare provider for personalized medical guidance regarding lung cancer diagnosis and treatment decisions.
Related Reading:
- What Is Lung Cancer? Complete 2026 Guide
- SCLC Survival Rates & Treatment Costs
- FDA-Approved Lung Cancer Drugs 2026
- Early Lung Cancer Warning Signs
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.