On This Page – Quick Medical Summary
If you or someone you love has just been told they have lung cancer, the first question is almost always: “What stage is it?” Lung cancer stages — from Stage 1 through Stage 4 — determine your treatment options, prognosis, and survival outlook. Stage 1 is localized and highly treatable. Stage 4 means the cancer has spread to distant organs. Understanding each stage is the single most important step toward making informed decisions.
Before you read further, use our Symptom Checker if you’re currently experiencing unexplained respiratory symptoms that haven’t yet been evaluated by a physician.
⚠️ Disclaimer: This article is for educational purposes only and does not constitute medical advice. Always consult a licensed healthcare provider for diagnosis and treatment decisions.
The TNM Staging System — How Doctors Determine Your Lung Cancer Stage
Lung cancer staging is not guesswork. It follows a structured framework called the TNM system, where each letter tells your doctor a specific piece of clinical information.
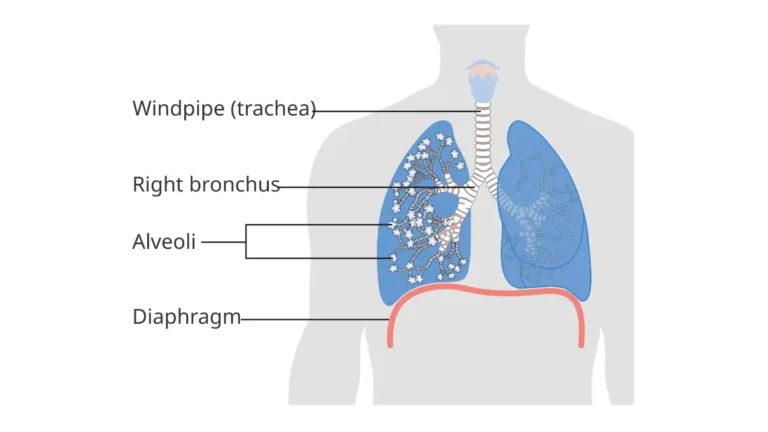
- T (Tumor): The size of the primary tumor and whether it has grown into nearby structures
- N (Node): Whether cancer has spread to regional lymph nodes
- M (Metastasis): Whether cancer has reached distant organs such as the brain, liver, or bones
Your TNM values are combined to assign a stage between 0 and IV. Understanding this system helps you have more informed conversations with your oncology team, as explained in our comprehensive guide on what is lung cancer.
NSCLC vs. SCLC: Two Cancers, Two Staging Systems
This is one of the most overlooked distinctions in lung cancer staging, and most competing resources bury it completely.
| Feature | NSCLC (Non-Small Cell) | SCLC (Small Cell) |
|---|---|---|
| Staging System | Stages 0–IV (TNM-based) | Limited Stage / Extensive Stage |
| % of Cases | ~85% of all lung cancers | ~15% of all lung cancers |
| Staging Detail | Highly granular (IA, IB, IIA, etc.) | Simplified two-stage model |
| Why It Matters | Surgery often viable early | SCLC spreads early; treatment differs significantly |
The distinction matters enormously because NSCLC staging drives surgical decisions, while SCLC staging focuses on whether radiation can safely cover the disease area. You can explore the full clinical comparison in our article on NSCLC vs SCLC.
According to the American Lung Association, staging is also divided into clinical stage (based on imaging before treatment) and pathological stage (based on tissue examined after surgery). These can differ — and when they do, your treatment plan is updated accordingly.
Stage 1 and Stage 2 Lung Cancer — Early Detection, Treatment, and Survival
Stage 1 Lung Cancer: The Best Possible Starting Point
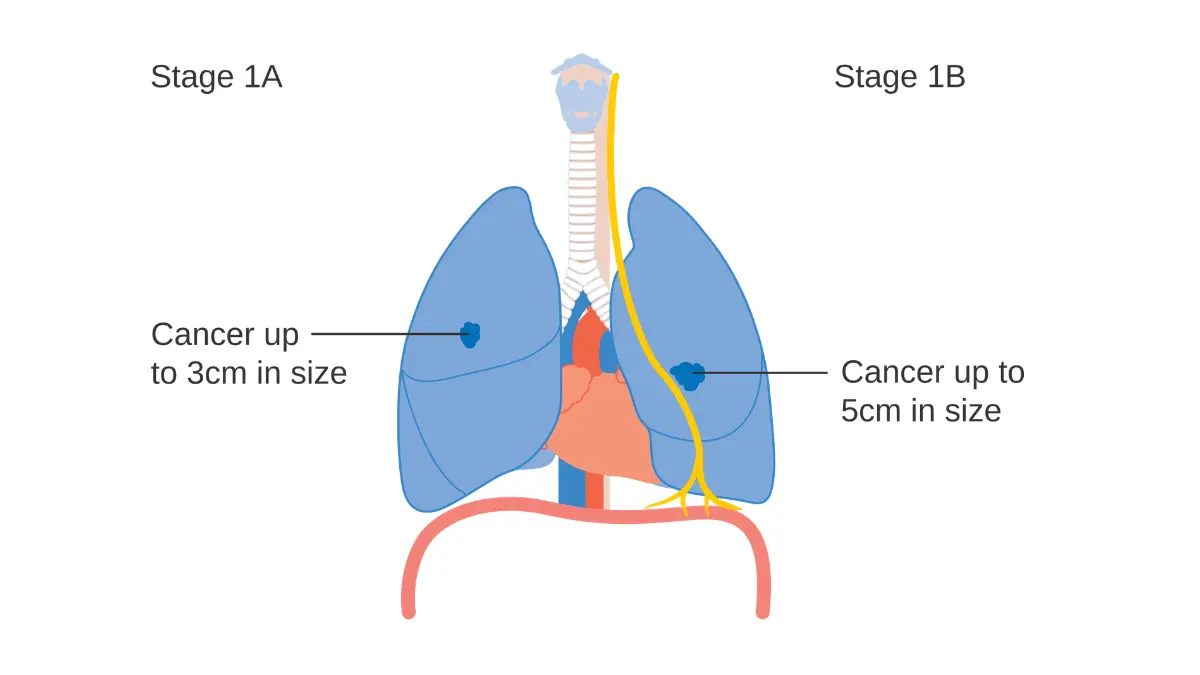
Stage 1 means the cancer is confined entirely to the lung. It has not reached lymph nodes or any other part of the body. According to the American Cancer Society’s NSCLC staging guide, Stage 1 is divided into two substages:
- Stage 1A: Tumor is ≤3 cm, no lymph node involvement whatsoever
- Stage 1B: Tumor is 3–4 cm, may involve the bronchus or visceral pleura, still no lymph nodes affected
The hard truth: Most Stage 1 patients have no symptoms at all. The cancer is silent, which is why it’s so rarely caught at this stage without screening. Read about the early warning signs of lung cancer to understand what to watch for.
Treatment options for Stage 1 lung cancer:
- Surgical lobectomy or segmentectomy (primary approach)
- Stereotactic body radiation therapy (SBRT) for patients who cannot undergo surgery
- Targeted therapy if EGFR or ALK mutations are identified
- Adjuvant immunotherapy in select cases (post-2024 guideline updates)
5-Year Survival Rate (Stage 1): According to SEER cancer statistics, the five-year relative survival rate for localized NSCLC is approximately 64%. With screening-detected cases, that figure climbs even higher.
💡 What This Means For You: Stage 1 lung cancer is among the most treatable solid tumors when caught early. Surgery alone can be curative in a significant proportion of patients. If your genetic or family history puts you at elevated risk, consider exploring our Genetic Risk Assessment Tool to identify personal risk factors.
Stage 2 Lung Cancer: Early-Stage, But Spreading Begins
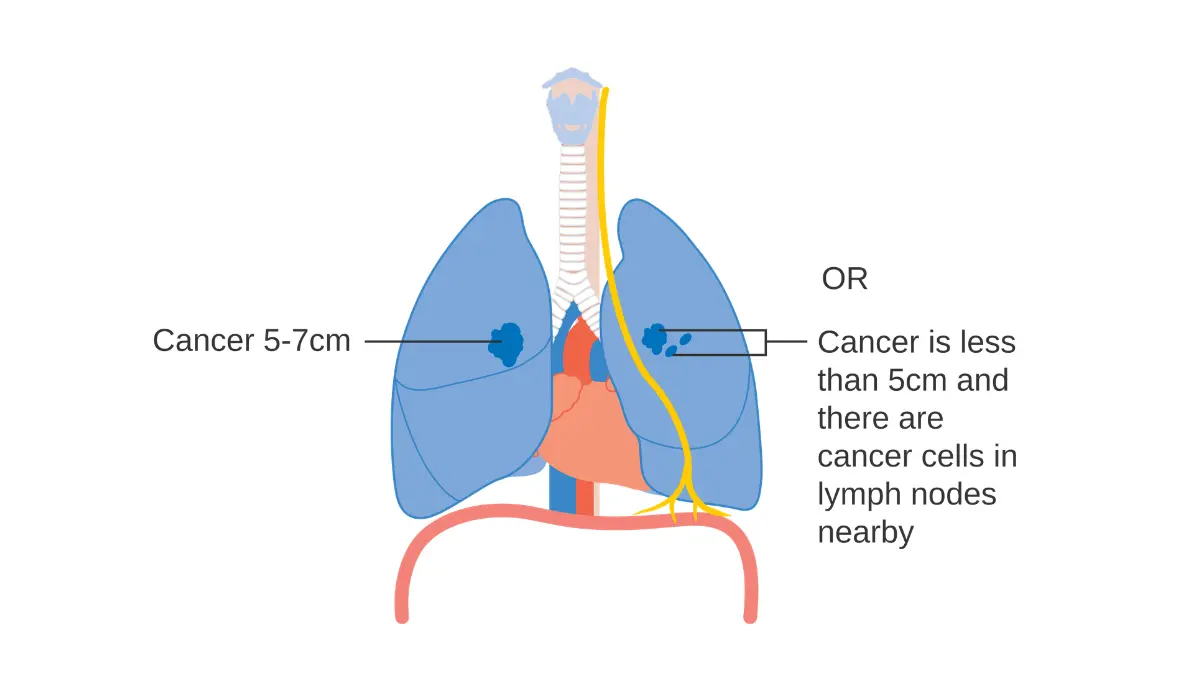
Stage 2 remains in or near the lung but shows early signs of regional spread. It is still considered an early-stage cancer with meaningful treatment potential.
- Stage 2A: Tumor is 4–5 cm, no lymph node involvement; or ≤3 cm tumor with spread to nearby lung lymph nodes (N1)
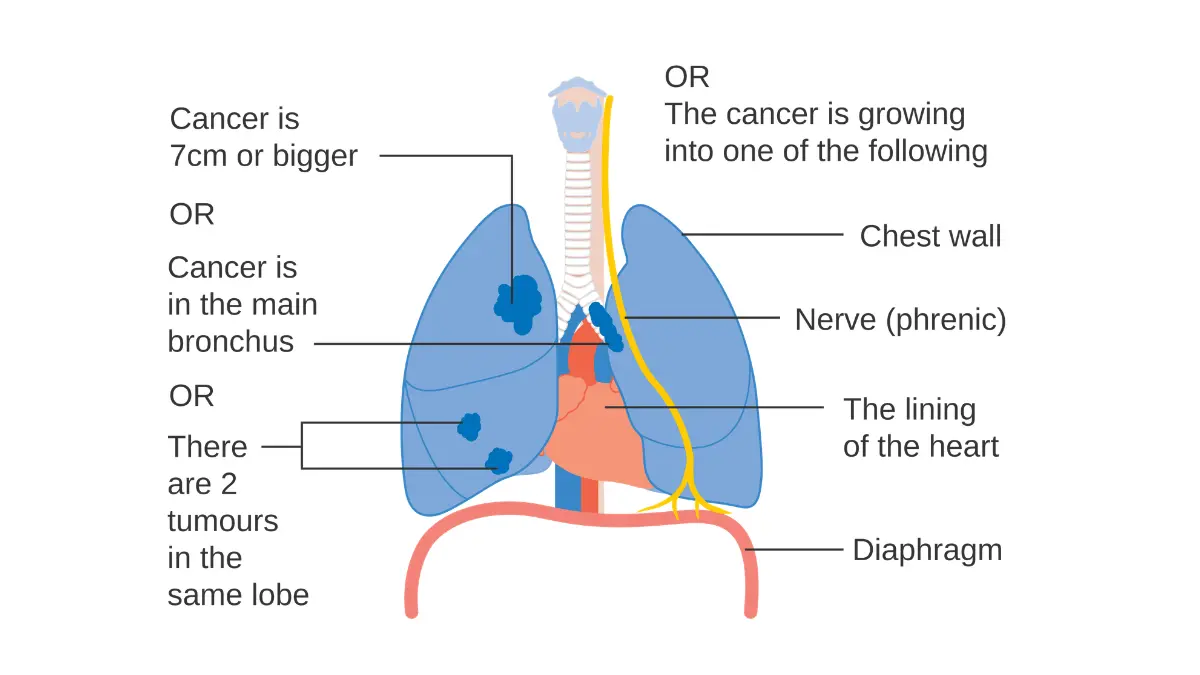
- Stage 2B: Tumor varies in size and may have grown into the chest wall, diaphragm, or pericardium; may involve N1 lymph nodes
Treatment options for Stage 2 lung cancer:
- Surgery (lobectomy) remains the primary option where resectable
- Adjuvant chemotherapy after surgery is standard practice
- Immunotherapy combinations increasingly used post-operatively in 2026 protocols
- Radiation therapy when surgery is not viable
| Stage 1 | Stage 2 | |
|---|---|---|
| Tumor Size | ≤4 cm | 4–7 cm |
| Lymph Nodes | None | Nearby (N1) possible |
| Distant Spread | None | None |
| 5-Yr Survival | ~64% | ~36–46% |
| Primary Treatment | Surgery / SBRT | Surgery + Adjuvant chemo |
💡 What This Means For You: Stage 2 lung cancer is still categorized as early-stage. Most patients who receive surgery plus adjuvant therapy achieve meaningful long-term survival. Ask your surgeon explicitly whether your tumor is resectable before accepting any treatment plan.
Stage 3 Lung Cancer — Locally Advanced Disease, Substages, and 2026 Breakthroughs
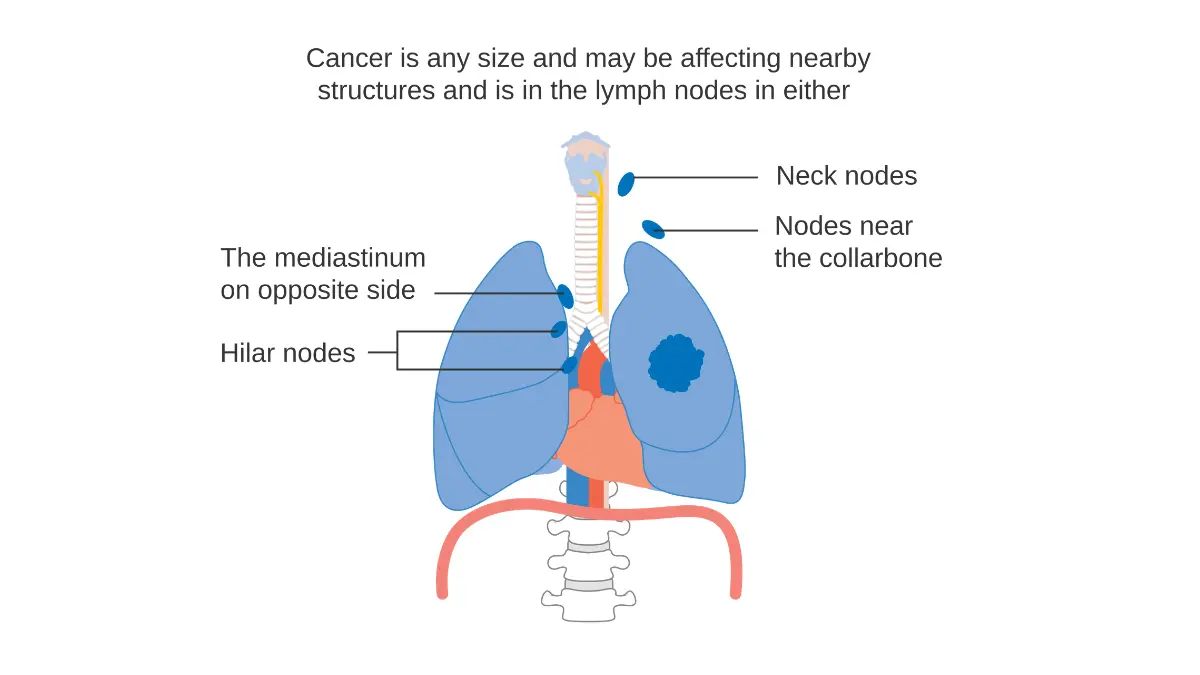
Stage 3 is where lung cancer becomes significantly more complex. It is called locally advanced lung cancer — the cancer has spread further within the chest but has not yet reached distant organs. This is the most misunderstood stage, and the substage you receive has enormous treatment implications.
Stage 3A, 3B, and 3C: Why the Letter Matters
According to LUNGevity Foundation’s staging guide, Stage 3 is divided into three substages:
| Substage | Key Feature | Typical Treatment Approach |
|---|---|---|
| Stage 3A | Spread to ipsilateral mediastinal lymph nodes; tumor may be resectable | Surgery + concurrent chemoradiation or chemoimmunotherapy |
| Stage 3B | Spread to contralateral mediastinal nodes or upper mediastinum; usually unresectable | Definitive concurrent chemoradiation + durvalumab (Imfinzi) |
| Stage 3C | Most extensive regional spread; multiple nodes, tumor ≥5 cm | Systemic immunotherapy-based regimens; surgery not viable |
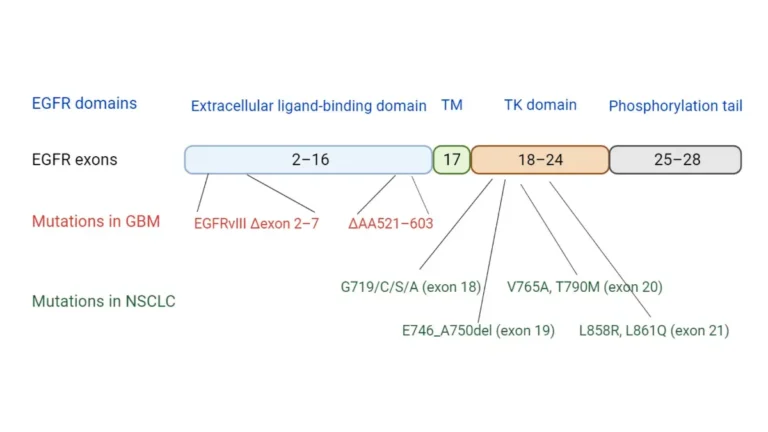
The biomarker angle competitors miss: At Stage 3, genetic mutation testing — specifically for EGFR, ALK, ROS1, and KRAS mutations — has become critical. Patients with targetable mutations respond very differently to immunotherapy versus those without. Getting tested before treatment starts is no longer optional; it is standard of care per 2026 ASCO guidelines. You can assess your personal genetic risk profile using our Genetic Risk Assessment Tool.
2026 Breakthrough: Data presented at the European Lung Cancer Congress (ELCC 2026) demonstrated significant progression-free survival improvements using new immunotherapy combinations in Stage 3 NSCLC, including gotistobart (ONC-392) showing superior outcomes over standard docetaxel in previously treated squamous NSCLC. This builds on already improving Stage 3 outcomes driven by checkpoint inhibitors.
5-Year Survival Rate (Stage 3): According to Moffitt Cancer Center’s staging resource, the five-year survival rate ranges from 13% to 37% depending on substage — a wide range that reflects how much substage and treatment choice matter.
💡 What This Means For You: Stage 3 does not automatically rule out surgery or long-term survival. Your substage (3A vs. 3B vs. 3C) and your tumor’s genetic profile are the two most important variables. Do not accept a blanket “Stage 3” prognosis — insist on substage clarification and biomarker testing.
Stage 4 Lung Cancer — Metastatic Disease, Real Survival Data, and New Hope in 2026
Stage 4 is called metastatic lung cancer or advanced lung cancer. The cancer has spread beyond the chest to distant organs. This is where the majority of American patients are unfortunately diagnosed, because lung cancer is often silent until it has spread significantly.
What “Stage 4” Actually Means
- Stage 4A: Cancer has spread to the opposite lung, to the pleural or pericardial fluid, or to a single distant organ (e.g., one brain lesion, one liver lesion)
- Stage 4B: Cancer has spread to multiple locations in one or more distant organs — the most advanced presentation
Common metastatic sites in Stage 4 lung cancer:
- Brain (causes headaches, dizziness, seizures)
- Liver (causes jaundice, right-sided abdominal pain)
- Bones (causes bone pain, fractures)
- Adrenal glands (often asymptomatic)
- Opposite lung
Survival Rates and Immunotherapy’s Game-Changing Role
This is the most important section competitors consistently fail to update. Older resources cite Stage 4 five-year survival rates of 1–5%. That era is over.
According to a landmark study published in PMC / National Institutes of Health tracking SEER registry data, Stage 4 NSCLC one-year survival improved by 2.09% per year from 2014 to 2019 — a striking acceleration that directly corresponds with immunotherapy approvals beginning in 2015.
Current five-year survival for Stage 4 NSCLC is approximately 10–21%, with the higher end seen in patients receiving first-line immunotherapy combinations such as:
- Pembrolizumab (Keytruda) + chemotherapy: 5-year survival ranged 18.4–19.4% in clinical data
- Nivolumab (Opdivo) + Ipilimumab (Yervoy): Long-term durable responses in PD-L1 high expressors
- Zongertinib (Hernexeos): ELCC 2026 data showed exceptional efficacy in HER2-mutant NSCLC with brain metastases — a previously very difficult-to-treat population
For detailed guidance on currently approved drugs, see our article on FDA-approved lung cancer drugs in 2026.
For SCLC extensive stage, the cancer has spread widely beyond one lung. Prognosis remains more challenging, but immunotherapy combinations have improved one-year survival significantly. Explore our dedicated guide on SCLC survival rates and treatment costs for stage-specific data.
According to Cancer Research Institute’s 2026 statistics report, localized lung cancer carries a five-year survival of 65% — compared to only 10% for distant-stage disease. The gap underscores why early detection is the single most powerful lever available.
💡 What This Means For You: Stage 4 lung cancer is not a death sentence. Immunotherapy and targeted therapies are actively rewriting survival statistics. The single most important step after a Stage 4 diagnosis is biomarker and genetic mutation testing before starting any treatment. Your treatment options in 2026 depend entirely on your tumor’s molecular profile.
How Fast Does Lung Cancer Progress? Progression, Risk Factors, and Early Detection
Why Most Patients Are Diagnosed at Stage 3 or 4
Lung cancer is one of the most asymptomatic cancers in its early stages. Symptoms like persistent cough, shortness of breath, or coughing up blood typically only appear once the cancer has grown large enough to irritate airways or spread to lymph nodes.
A study published in PMC examining NSCLC immunotherapy confirmed that the majority of patients are diagnosed at advanced stages precisely because early-stage disease produces no clinical warning signals.
How Fast Does Lung Cancer Progress Between Stages?
Progression speed varies significantly by subtype:
- Adenocarcinoma: Slower growth; median volume doubling time of 400–600 days
- Squamous cell carcinoma (SCC): Faster doubling time (~100–200 days); more rapid stage progression
- Small cell lung cancer: Fastest of all subtypes; can progress from limited to extensive stage within weeks without treatment
Factors that accelerate progression include:
- Active smoking or heavy smoking history (≥20 pack-years)
- KRAS mutation — associated with faster progression and worse survival in Caucasian populations
- Prior chemotherapy resistance — cancer cells develop accelerated growth mechanisms
- Delayed access to care — every 3-month delay in diagnosis increases stage advancement risk
For full statistics on how lung cancer progression affects long-term outcomes in the United States, see our in-depth analysis of lung cancer statistics and survival rates.
Low-Dose CT Screening: The Most Underused Life-Saving Tool
The U.S. Preventive Services Task Force (USPSTF) recommends annual low-dose CT (LDCT) screening for adults aged 50–80 who have a 20 pack-year smoking history and currently smoke or quit within the past 15 years.
The evidence is compelling: lung cancer screening programs in multiple randomized trials have detected cancer at an early stage with detection rates of 40–66%, with 5- and 10-year survival rates approaching 90% when discovered through screening — compared to under 20% when discovered symptomatically.
Despite this, only an estimated 5–6% of eligible Americans currently undergo LDCT screening. If you qualify, speaking to your doctor today could be the decision that changes your outcome. Explore our broader lung cancer signs and early warnings guide for a complete overview of detection red flags.
💡 What This Means For You: If you are aged 50–80 with a 20 pack-year smoking history, you are USPSTF-eligible for free annual LDCT screening under the Affordable Care Act. Don’t wait for symptoms.
Master Summary Table and 3 Immediate Next Steps After Diagnosis
Complete Lung Cancer Stages at a Glance (2026)
| Stage | Spread | Tumor Size | 5-Year Survival (NSCLC) | Primary Treatment |
|---|---|---|---|---|
| Stage 1A | Lung only | ≤3 cm | ~73–92% | Surgery / SBRT |
| Stage 1B | Lung only | 3–4 cm | ~68% | Surgery / SBRT |
| Stage 2A | Lung ± N1 nodes | 4–5 cm | ~46% | Surgery + adjuvant chemo |
| Stage 2B | Lung + chest structures | Up to 7 cm | ~36% | Surgery + adjuvant chemo/immunotherapy |
| Stage 3A | Regional chest | Any | ~26–37% | Chemoradiation ± immunotherapy |
| Stage 3B | Bilateral mediastinum | Any | ~13–26% | Concurrent chemoimmunotherapy |
| Stage 3C | Extensive regional | Any | ~13% | Systemic therapy |
| Stage 4A | Single distant site | Any | ~10–21% | Immunotherapy / targeted therapy |
| Stage 4B | Multiple distant sites | Any | ~5–10% | Immunotherapy / palliative-intent therapy |
Source: ACS Cancer Statistics 2026 / SEER Database / Moffitt Cancer Center
3 Non-Negotiable Next Steps for Every Newly Diagnosed Patient
1. Request comprehensive biomarker testing immediately. Before any treatment begins, insist on molecular profiling for EGFR, ALK, ROS1, KRAS, HER2, BRAF, MET, and PD-L1 expression. These results determine whether targeted therapy or immunotherapy will work for your tumor. Reviewing our guide on how immunotherapy works provides important context.
2. Seek a second opinion at a designated NCI Cancer Center. Treatment recommendations for lung cancer vary widely between institutions. A second opinion from an NCI-designated center can change your treatment plan in up to 30% of cases. Find a center through the NCI clinical trials database.
3. Ask about active clinical trials. In 2026, there are more open clinical trials for lung cancer than any point in history — particularly for Stage 3 and Stage 4 patients. Trials often provide access to cutting-edge therapies years before FDA approval.
For a complete overview of the lung cancer treatment landscape and newly approved drugs in 2026, see our detailed guide on lung cancer FDA drugs and treatments 2026.
Frequently Asked Questions — Lung Cancer Stages
Q1. What are the 4 stages of lung cancer?
Stage 1 is cancer confined to the lung. Stage 2 has limited local spread. Stage 3 is regionally advanced within the chest. Stage 4 has spread to distant organs such as the brain or liver.
Q2. Is Stage 1 lung cancer curable?
Yes. With surgery, Stage 1 lung cancer carries a 5-year survival rate of approximately 64–92% depending on substage. Early surgical removal is often curative. See our dedicated guide on Stage 1 lung cancer survival.
Q3. What is the survival rate for Stage 4 lung cancer?
The current 5-year survival rate for Stage 4 NSCLC is approximately 10–21%, significantly improved by immunotherapy. Patients with actionable mutations (EGFR, ALK, HER2) often achieve longer survival with targeted drugs.
Q4. What does Stage 3B lung cancer mean?
Stage 3B means cancer has spread to lymph nodes on both sides of the chest or above the collarbone. It is typically unresectable and treated with concurrent chemotherapy plus immunotherapy (often durvalumab).
Q5. How is lung cancer staged by doctors?
Doctors use CT scans, PET scans, bronchoscopy, mediastinoscopy, and biopsy results to assign a clinical TNM stage. After surgery, a pathological stage is confirmed from tissue analysis.
Q6. What is the TNM system in lung cancer?
TNM stands for Tumor (size/location), Nodes (lymph node involvement), and Metastasis (distant spread). Each is scored numerically, and the combined scores determine your overall stage from 0 to IV.
Q7. Can Stage 4 lung cancer go into remission?
Yes. With modern immunotherapy and targeted therapy, a subset of Stage 4 patients achieve partial or complete remission — some for several years. Long-term durable responses are now documented in clinical trial data published through PMC/NIH.
Q8. How fast does lung cancer progress from Stage 1 to Stage 4?
Speed depends entirely on subtype. Adenocarcinoma may take years to progress. Squamous cell carcinoma moves faster. Small cell lung cancer can progress within weeks. Most patients are diagnosed at Stage 3 or 4 because early stages produce no symptoms.
Q9. What is the difference between NSCLC and SCLC staging?
NSCLC uses a detailed 0–IV TNM system. SCLC uses a simplified two-stage model: limited stage (one lung, treatable with radiation) and extensive stage (widespread, systemic therapy required). Explore the full breakdown in our NSCLC vs SCLC guide.
Q10. Does Stage 2 lung cancer require chemotherapy?
Not always as a standalone treatment. However, adjuvant chemotherapy after surgery is standard for Stage 2 to reduce recurrence risk. In 2026, adjuvant immunotherapy is increasingly added for patients with PD-L1-positive tumors or specific mutations.
Q11. What are the first signs of Stage 1 lung cancer?
Most Stage 1 patients have no symptoms. When symptoms do occur, they include a new persistent cough, mild shortness of breath, or unexplained fatigue. Annual LDCT screening is the only reliable way to detect Stage 1 lung cancer. Review our full early lung cancer warning signs guide for a comprehensive symptom breakdown.
About this content
This medical content is prepared through a structured publishing workflow with expert writing, clinical review and editorial quality checks.

Board Certifications: Internal Medicine (2005); Medical Oncology (2008); Hematology (2009) Experience: 20 years | Location: Houston, Texas Education: BS Biology, Duke University (1999); MD, Baylor College of Medicine…

Board Certifications: Medical Oncology (2011); Haematology (2012) Experience: 14 years | Location: New York City, New York Education: BS Biochemistry, Princeton University (2002); MD, Columbia University College of…

Board Certifications: Preventive Medicine (2010); Public Health & General Preventive Medicine (2010) Experience: 15 years | Location: Washington, DC Education: BA Public Policy, Georgetown University (2001); MD, George…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.