On This Page – Quick Medical Summary
When Marcus, a 47-year-old construction supervisor from Ohio, began having shoulder pain and a drooping eyelid, his first three doctors treated it as a pinched nerve. Six months later, an oncologist discovered a Pancoast tumor — a rare type of lung cancer at the apex of his lung pressing on nearby nerves. His story is not unique.
Lung cancer has over 10 recognized subtypes. While most people know about common forms, the rare types of lung cancer — some affecting less than 1% of patients — are frequently misdiagnosed, undertreated, and almost never discussed in mainstream health content. This 2026 guide changes that.
⚠️ Disclaimer: This article is for educational purposes only and does not constitute medical advice. Always consult a qualified oncologist for diagnosis, staging, and treatment decisions.
What Makes a Lung Cancer “Rare” — And Why It Matters in 2026
In oncology, “rare” typically means a cancer subtype accounts for fewer than 5% of all diagnoses in that category. But here’s what most people don’t realize: when combined, rare lung cancer subtypes collectively account for 15–20% of all lung cancer cases diagnosed annually in the United States.
That’s not a small number.
According to the National Cancer Institute, approximately 234,580 new lung cancer cases are expected to be diagnosed in the U.S. in 2026. Even at a conservative 10% rare-type rate, that’s over 23,000 Americans per year facing an uncommon lung cancer subtype with limited research, fewer clinical trials, and higher misdiagnosis rates.
Why rare lung cancers are harder to catch:
- They often produce atypical symptoms unrelated to breathing
- Many are discovered incidentally on CT scans ordered for other reasons
- Pathologists at general hospitals may not encounter them frequently enough to identify them correctly
- Standard treatments developed for common lung cancers frequently don’t work for rare subtypes
The 2021 World Health Organization (WHO) classification formally codified several new rare lung cancer histological categories — including enteric, fetal, and colloid adenocarcinoma subtypes. This was a landmark shift. Before that update, many of these rare types of lung cancer were misclassified or grouped under “not otherwise specified.”
Genetic testing has become a game-changer. Next-generation sequencing (NGS) can now detect rare driver mutations — including MET amplification, ROS1 rearrangement, RET fusion, NTRK fusion, and HER2 mutations — that are disproportionately found in uncommon lung cancer subtypes. These mutations matter because they open the door to targeted therapies that are far more effective than standard chemotherapy.
If you have unexplained respiratory or neurological symptoms, use the Symptom Checker on mymedicineadvisor.com to help identify patterns worth discussing with your physician.
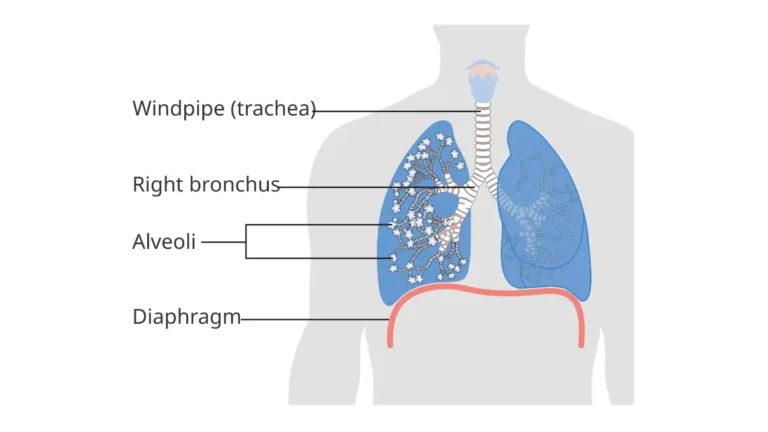
Understanding the broader picture of what lung cancer is — including how cells transform and spread — is the essential foundation before diving into its rarest subtypes.
The 7 Rare Types of Lung Cancer — Full 2026 Clinical Breakdown
This is the section no competitor has built for a general audience. Below is a comprehensive comparison table followed by individual clinical deep-dives for each rare lung cancer type.
Quick-Reference Comparison Table
| Rare Type | Prevalence | Who It Affects | 5-Year Survival | Key 2026 Treatment |
|---|---|---|---|---|
| Large Cell Neuroendocrine Carcinoma | ~3% of lung cancers | Older male smokers | 13–57% (stage-dependent) | Chemo + immunotherapy combo |
| Lung Carcinoid Tumor | <5% | Younger patients, non-smokers | 78–90% (typical type) | Surgery; PRRT for metastatic |
| Adenosquamous Carcinoma | 0.4–4% | Smokers | ~20% at 5 years | Dual-pathway therapy |
| Pancoast Tumor | <5% | Smokers; upper-lobe location | Improved significantly | Trimodality (chemo + radiation + surgery) |
| Sarcomatoid Carcinoma | <1% | Older males, smokers | <20% | Immunotherapy (high PD-L1) |
| Mesothelioma | <5% | Asbestos-exposed workers | ~12% at 5 years | Nivolumab + ipilimumab (FDA-approved) |
| Atypical Small Cell Carcinoma | ~3% of SCLC cases | Non-smokers, younger adults | Under active study | Targeted therapy trials |
1. Large Cell Neuroendocrine Carcinoma (LCNEC) — The Aggressive Hybrid
LCNEC is an aggressive, high-grade tumor that sits at a confusing intersection between small cell and non-small cell lung cancer. It accounts for roughly 3% of all lung cancer diagnoses and carries some of the worst survival statistics in the rare category.
Key facts:
- Primarily affects men over 60 with a significant smoking history
- Requires specialized immunohistochemistry to distinguish from small cell lung cancer
- Often presents at advanced stages due to rapid growth
- Median survival without treatment: 5–7 months at metastatic stage
A 2021 study published in Cureus via the NIH documents the diagnostic complexity of LCNEC and highlights the need for molecular profiling at diagnosis. In 2026, platinum-based chemotherapy combined with immunotherapy (atezolizumab) is emerging as the standard of care at major U.S. cancer centers.
For comprehensive staging information on how rare lung cancers are classified, see the Lung Cancer Stages Explained guide.
2. Lung Carcinoid Tumors — The “Slow Cancer” That Strikes Younger Patients
Lung carcinoid tumors are neuroendocrine tumors that grow far more slowly than most lung cancers. They make up less than 5% of all lung cancers, according to the American Lung Association, and they disproportionately affect younger patients, including non-smokers.
There are two types:
- Typical carcinoids — lower-grade, excellent surgical outcomes, 78–90% five-year survival
- Atypical carcinoids — higher-grade, more aggressive, lower survival rates
What makes carcinoid tumors unique is carcinoid syndrome — a set of symptoms caused by hormones secreted by the tumor:
- Facial flushing (sudden reddening)
- Wheezing or difficulty breathing
- Rapid heart rate
- Diarrhea
No major competitor covers carcinoid syndrome as part of their rare lung cancer content. If you notice these symptoms alongside respiratory issues, this combination is clinically significant and warrants immediate evaluation.
A 2023 systematic review published on PubMed Central confirms that surgery remains the primary treatment for localized carcinoids, while metastatic cases benefit from peptide receptor radionuclide therapy (PRRT) using Lu-177 DOTATATE.
Use the Genetic Risk Assessment Tool to evaluate your hereditary risk profile — carcinoid tumors have known familial clustering in some cases.
3. Adenosquamous Carcinoma — The Hybrid That Confuses Pathologists
Adenosquamous carcinoma is a rare subtype of non-small cell lung cancer that contains two distinct cell types in a single tumor: glandular cells (adenocarcinoma) and squamous cells. It accounts for 0.4–4% of all lung cancer cases.
Why it’s clinically challenging:
- More aggressive than either pure adenocarcinoma or squamous cell carcinoma alone
- Standard treatment protocols for either pure type often underperform
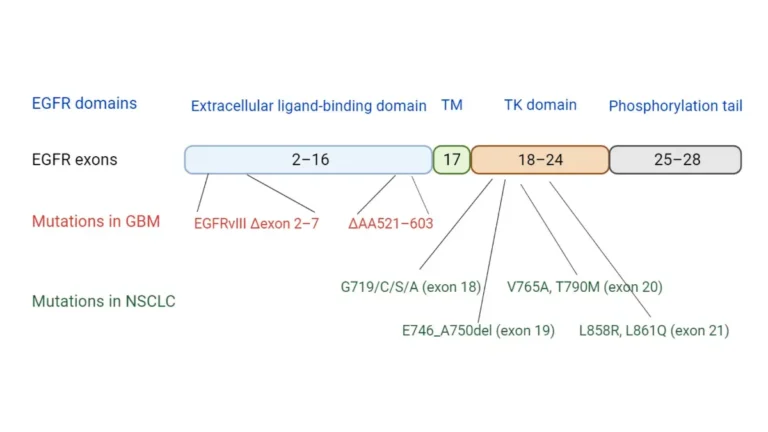
- As of 2026, EGFR mutation testing is now recommended as a standard first step — some patients respond well to EGFR-targeted inhibitors
Treatment requires a combination approach, and tumor board review is essential. Patients should ask specifically whether their biopsy has been tested for dual-lineage markers.
4. Pancoast Tumor — The Lung Cancer That Looks Like a Shoulder Problem
Pancoast tumors form at the very top (apex) of the lung. Because of their location, they don’t typically cause classic respiratory symptoms. Instead, they invade surrounding structures — the brachial plexus nerve network, ribs, and spine — producing symptoms that send most patients to orthopedic specialists first.
Signature symptoms that separate Pancoast from common lung cancer:
- Shoulder pain and arm weakness — often the first symptom
- Horner’s Syndrome — a drooping eyelid, constricted pupil, and reduced facial sweating on one side, caused by pressure on the sympathetic nerve chain
- Numbness or tingling down the arm (ulnar nerve distribution)
Marcus’s case from the introduction is a textbook Pancoast presentation. Historically considered inoperable, Pancoast tumors are now managed with trimodality therapy: concurrent chemoradiation followed by surgical resection. Outcomes at specialized thoracic centers have improved substantially over the past decade.
5. Pulmonary Sarcomatoid Carcinoma — The Immunotherapy Responder
Sarcomatoid carcinoma represents less than 1% of all lung cancers, making it one of the rarest types. It is characterized by spindle-shaped or giant cells and carries historically poor prognosis — but 2026 has changed the picture significantly.
The immunotherapy breakthrough: Sarcomatoid carcinomas express extremely high levels of PD-L1 — a protein that immunotherapy drugs like pembrolizumab (Keytruda) specifically target. Studies now show that patients with sarcomatoid carcinoma have higher response rates to pembrolizumab than patients with many common lung cancer types.
This is a major finding that no general health website currently communicates to patients. If you or a loved one receives this diagnosis, requesting immediate PD-L1 expression testing is critical.
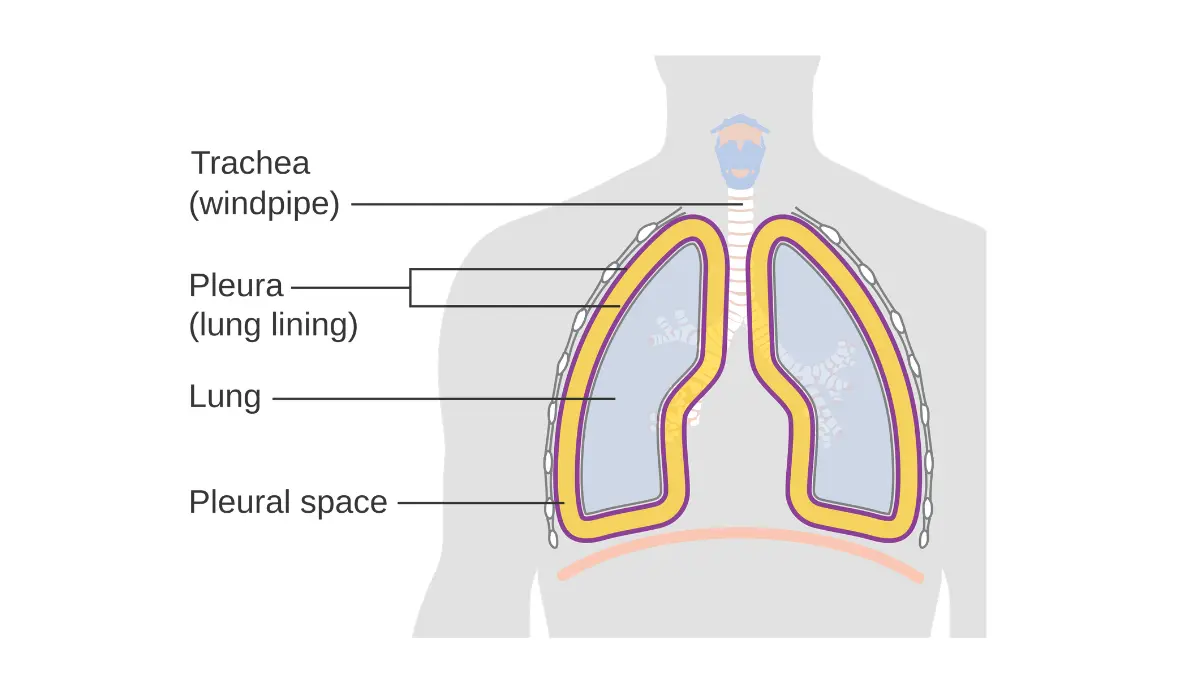
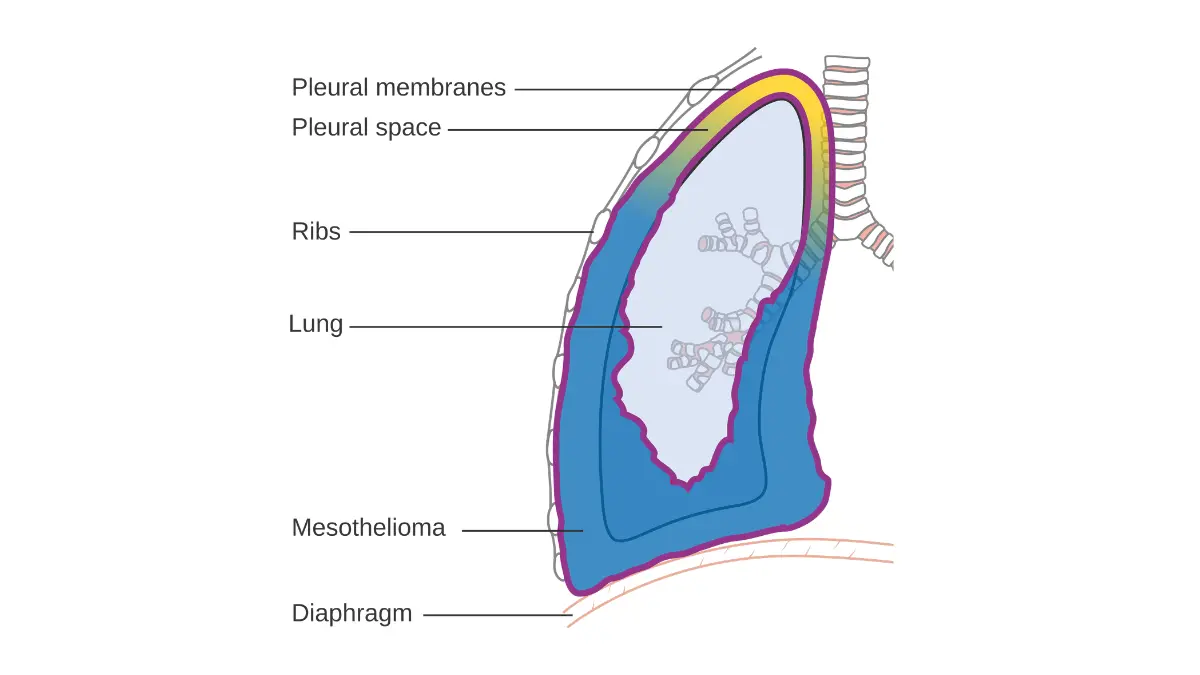
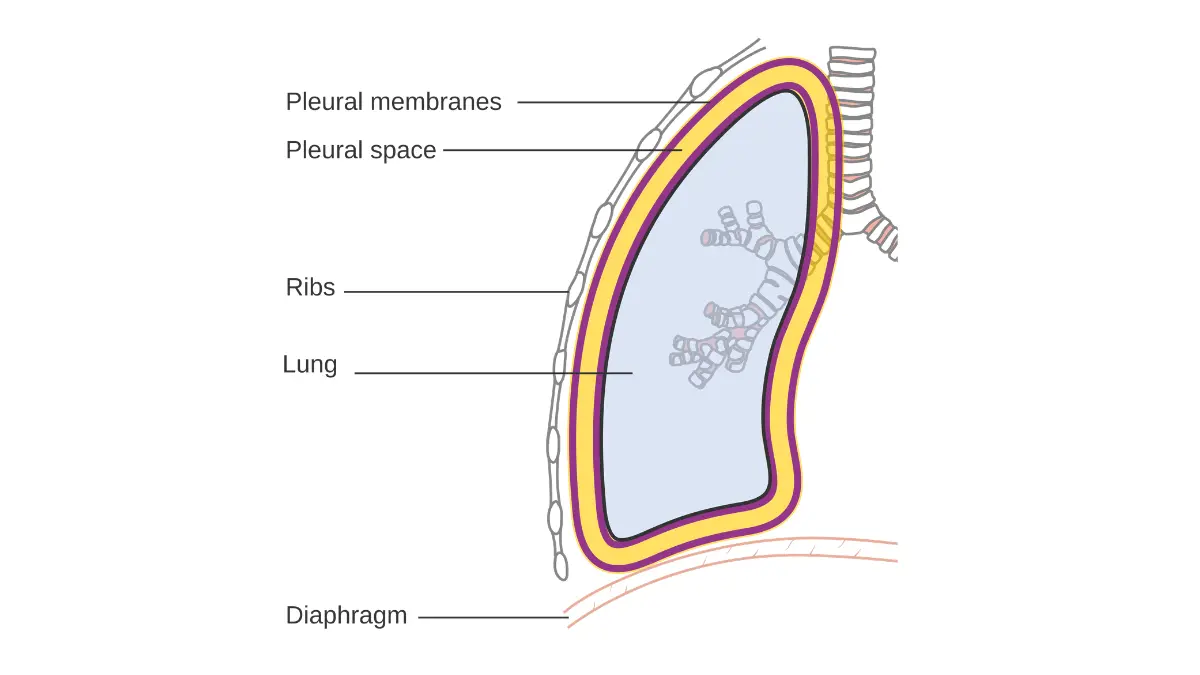
6. Mesothelioma — Not Technically “In” the Lung, But Always Listed
Mesothelioma develops in the pleura — the thin membrane lining the outside of the lungs and chest cavity — not in lung tissue itself. However, because of its location and clinical presentation, it is universally discussed alongside lung cancers.
Key facts for 2026:
- Directly and almost exclusively caused by asbestos exposure
- Latency period: 20–50 years between exposure and diagnosis
- High-risk occupations: construction workers, shipyard workers, firefighters, veterans
- Fewer than 20,000 cases diagnosed annually in the U.S.
In 2020, the FDA approved nivolumab plus ipilimumab as a first-line combination immunotherapy for unresectable malignant pleural mesothelioma — a landmark change that has extended median survival beyond previous limits. For full mesothelioma vs. lung cancer comparisons, see the dedicated comparison guide.
For more information on the FDA’s approval, visit FDA.gov directly.
7. Atypical Small Cell Lung Carcinoma — The 2025 Discovery
This is the newest entry in the rare lung cancer landscape. In 2025, researchers at Memorial Sloan Kettering Cancer Center identified a new subtype of small cell lung cancer that primarily affects never-smokers and younger adults — a profound departure from classic SCLC, which is almost always linked to heavy smoking.
What makes atypical SCLC different:
- Mean age at diagnosis: 53 (versus 70 for standard SCLC)
- 65% of identified patients were never-smokers
- Distinct genetic signature from classic SCLC
- Early data suggests different vulnerabilities that may respond to targeted therapies
Among 600 SCLC patients analyzed, only 20 (3%) were found to have this rare subtype. But those numbers likely underrepresent the true prevalence, since this subtype has only recently been defined.
Clinical trials specifically for this subtype are now recruiting. The NCI’s clinical trials registry is the best starting point for patients seeking experimental treatment options.
Warning Signs You Shouldn’t Ignore — Rare vs. Common Lung Cancer Symptoms
Some rare lung cancers produce zero respiratory symptoms at early stages. This is the critical fact that delays diagnosis by months — sometimes years.
Symptom Differentiation Table
| Symptom | Common Lung Cancer? | Rare Type Associated |
|---|---|---|
| Persistent cough | ✅ Very common | SCLC, NSCLC |
| Shoulder or arm pain | ❌ Rarely flagged | Pancoast Tumor |
| Facial flushing + diarrhea | ❌ Almost never mentioned | Carcinoid Syndrome |
| Drooping eyelid + pupil change | ❌ Not covered by competitors | Horner’s Syndrome (Pancoast) |
| Tumor found on incidental CT scan | ❌ Not addressed | Carcinoid, LCNEC |
| Chest wall tenderness | ❌ Underreported | Mesothelioma |
| Unexplained weight loss in younger adults | ❌ Overlooked | Atypical SCLC |
What This Means For You
If you experience shoulder pain combined with any respiratory symptom — request a chest CT scan immediately, not just an X-ray. Standard X-rays frequently miss Pancoast tumors and early-stage rare lung cancers.
Red flag combinations specific to rare types:
- Shoulder/arm pain + voice changes = possible Pancoast
- Facial flushing + wheezing + diarrhea = possible carcinoid syndrome
- Sudden drooping of one eyelid + chest discomfort = possible Horner’s Syndrome
- Shortness of breath + chest wall pain in someone with asbestos exposure history = possible mesothelioma
Use the Symptom Checker if you’re experiencing any unexplained combination of the above symptoms. Early reporting saves lives with every type of lung cancer — but especially rare ones.
How Rare Lung Cancers Are Diagnosed — And Why It Often Takes Too Long
The average rare lung cancer patient sees 2–3 physicians before receiving the correct diagnosis. Understanding the diagnostic pathway can help you advocate for yourself or a loved one.
The Diagnostic Pathway in 2026
Step 1 — Imaging
- Low-dose CT scan: first-line screening, detects nodules and masses
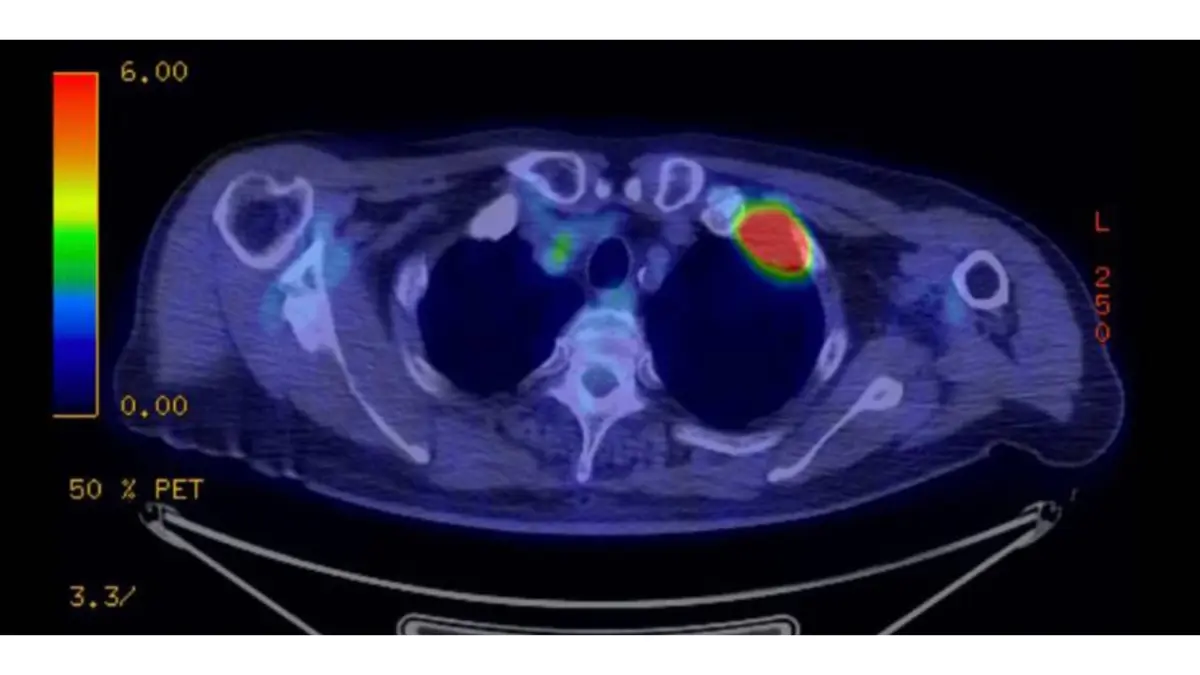
- PET scan: determines metabolic activity and spread
- Note: Pancoast tumors and pleural mesothelioma require specific imaging protocols that general practitioners may not order
Step 2 — Biopsy
- Bronchoscopy for central airway tumors
- CT-guided needle biopsy for peripheral masses
- Video-assisted thoracoscopic surgery (VATS) for pleural sampling
Step 3 — Molecular Profiling (The Critical Step)
This is where rare lung cancer diagnosis either succeeds or fails. Standard pathology alone is insufficient for rare subtypes. Next-generation sequencing (NGS) — a comprehensive genetic test performed on tumor tissue — identifies:
- MET exon 14 skipping mutations
- ROS1 rearrangements
- RET fusions
- NTRK fusions
- HER2 mutations
- BRAF V600E mutations
According to the NIH’s rare lung cancer research, molecular characterization is now essential for accurate classification and treatment planning for all rare subtypes.
Questions to Ask Your Oncologist
- “Has full NGS (next-generation sequencing) been performed on my biopsy?”
- “Has my case been reviewed by a multidisciplinary thoracic tumor board?”
- “Am I at a center with experience treating this specific rare subtype?”
- “Is there an active clinical trial I qualify for?”
For context on how NSCLC and SCLC differ in diagnosis, the NSCLC vs. SCLC guide provides a detailed clinical comparison.
You can also explore your personal genetic risk profile using the Genetic Risk Assessment Tool — particularly relevant if rare cancers appear in your family history.
2026 Treatment Advances for Rare Lung Cancers — What’s New Right Now
This is the section that makes 2026 content genuinely different from everything published before it. Rare lung cancer treatment has shifted dramatically.
Treatment Advances by Rare Type
| Rare Type | Previous Standard | 2026 Update |
|---|---|---|
| LCNEC | Platinum-based chemo alone | Atezolizumab + chemo; improved OS |
| Carcinoid (metastatic) | Octreotide | Lu-177 DOTATATE (PRRT) approved and active |
| Sarcomatoid | Limited options | Pembrolizumab (high PD-L1 expression) — significant responders |
| Mesothelioma | Pemetrexed + cisplatin | Nivolumab + ipilimumab (FDA-approved first-line) |
| Atypical SCLC | Standard SCLC chemo | Targeted therapy trials underway at MSK and MSKCC |
| Pancoast | Surgery only | Trimodality now standard at NCI-designated centers |
| Adenosquamous | Standard NSCLC chemo | EGFR-targeted inhibitors for mutation-positive patients |
Targeted Therapy in Rare Lung Cancers
The expansion of targeted therapies is the single most important development in rare lung cancer treatment:
- Larotrectinib (Vitrakvi) — approved for NTRK fusion-positive cancers including rare lung subtypes
- Selpercatinib (Retevmo) — targets RET fusions, found in some rare lung adenocarcinomas
- Tepotinib / Capmatinib — for MET exon 14 skipping mutations
For a comprehensive overview of the latest FDA-approved lung cancer drugs in 2026, including rare-subtype indications, see the dedicated guide. The NCI’s clinical trials portal is the definitive resource for finding trials enrolling rare lung cancer patients right now.
What This Means For You
Do not accept “there are no options” as a final answer for a rare lung cancer diagnosis. The treatment landscape for rare subtypes in 2026 is more robust than at any prior point in medical history. Seek a second opinion at an NCI-designated comprehensive cancer center.
Maintaining healthy body weight during treatment supports treatment tolerance and recovery. Track treatment-related weight changes with the BMI Calculator. Quality sleep is equally critical during cancer care — the Sleep Calculator can help optimize rest cycles, which directly impacts immune function and treatment recovery.
For full survival data context, the Lung Cancer Statistics and Survival Rates guide breaks down outcomes by subtype and stage.
Living With a Rare Lung Cancer Diagnosis — Real Steps, Real Support
A rare diagnosis adds a layer of uncertainty that patients with common lung cancers don’t face. There are fewer online communities, fewer published patient stories, and often fewer doctors with direct experience treating your specific subtype.
Here is what the evidence — and patient experience — says works:
Immediate Action Steps After Diagnosis
1. Request a multidisciplinary tumor board review Every major cancer center convenes a board of oncologists, surgeons, radiologists, and pathologists to review complex cases. Rare lung cancers qualify without question. Insist on this.
2. Seek a second pathology opinion Send your biopsy slides to a comprehensive cancer center. Misclassification of rare subtypes is documented in the medical literature — particularly between LCNEC and small cell lung cancer, and between adenosquamous and pure adenocarcinoma.
3. Ask about clinical trials immediately Clinical trials are not a last resort. For rare lung cancers, they are often the pathway to the most advanced treatments available. Search ClinicalTrials.gov using your specific subtype and mutation status.
4. Connect with condition-specific advocacy organizations
- LUNGevity Foundation — the largest U.S. lung cancer advocacy organization, with rare subtype resources
- Mesothelioma Applied Research Foundation (MARF) — specific to mesothelioma
- Lung Cancer Research Foundation — funds research into all subtypes
5. Nutritional and lifestyle support during treatment
Maintaining adequate protein intake supports immune function and muscle preservation during chemotherapy. See the Protein Intake Calculator for personalized guidance. Staying well-hydrated is equally important — track fluid needs with the Water Intake Calculator.
For a complete understanding of how rare lung cancer fits within the broader survival picture, the Small Cell Lung Cancer Survival Rates article provides detailed stage-by-stage data.
Frequently Asked Questions — 11 Clinical Answers
1. What is the rarest type of lung cancer?
Pulmonary sarcomatoid carcinoma is among the rarest, accounting for less than 1% of all lung cancers. The newly identified atypical small cell carcinoma (MSK, 2025) may be even rarer, affecting roughly 3% of SCLC patients — themselves only 13–15% of all lung cancer cases.
2. Can you get rare lung cancer without ever smoking?
Yes. Lung carcinoid tumors and the newly discovered atypical SCLC disproportionately affect non-smokers. Carcinoid tumors have the highest rate of occurrence in non-smoking younger adults. Atypical SCLC showed 65% never-smokers in its initial patient cohort.
3. What are the early warning signs of rare lung cancer?
Early signs vary dramatically by subtype. Pancoast tumors cause shoulder and arm pain first. Carcinoid tumors may cause facial flushing or wheezing. LCNEC and sarcomatoid carcinoma may produce few symptoms until advanced. General early lung cancer signs — persistent cough, unexplained weight loss, fatigue — apply broadly.
4. How long can you live with a rare lung cancer diagnosis?
Survival depends entirely on the specific subtype and stage. Typical lung carcinoids have a five-year survival of 78–90%. Mesothelioma has a median survival of 18–21 months with modern immunotherapy. Sarcomatoid carcinoma historically averaged under a year, but immunotherapy is extending survival significantly.
5. Is Pancoast tumor a type of rare lung cancer?
Yes. Pancoast tumor is defined not by cell type but by its location at the apex of the lung. It is most commonly a non-small cell lung cancer subtype. Its rarity lies in its location-specific symptoms and the specialized trimodality treatment it requires.
6. What is Large Cell Neuroendocrine Carcinoma?
LCNEC is a high-grade, fast-growing tumor with features of both small cell and non-small cell lung cancer. It accounts for approximately 3% of all lung cancers, primarily affects older male smokers, and requires molecular profiling for accurate diagnosis and treatment planning.
7. Is mesothelioma technically lung cancer?
No — mesothelioma develops in the pleura (lung lining), not lung tissue itself. However, it is clinically managed by thoracic oncologists and staged similarly to lung cancer. It is almost exclusively caused by asbestos exposure.
8. What genetic mutations are specific to rare lung cancers?
Rare lung cancer subtypes are associated with MET exon 14 mutations, ROS1 rearrangements, RET fusions, NTRK fusions, and HER2 mutations. Next-generation sequencing at diagnosis is the only reliable way to identify these actionable alterations.
9. Are there new treatments for rare lung cancers approved in 2026?
Yes. As of 2026, PRRT with Lu-177 DOTATATE for metastatic carcinoid tumors, nivolumab + ipilimumab for mesothelioma, and pembrolizumab for high-PD-L1 sarcomatoid carcinoma represent the major treatment advances. Targeted therapies for NTRK, RET, and MET mutations are also now accessible.
10. Can rare lung cancer be hereditary?
Some rare subtypes have familial clustering. Carcinoid tumors, in particular, are associated with Multiple Endocrine Neoplasia type 1 (MEN1). If multiple family members have had rare cancers or carcinoid tumors, genetic counseling is recommended.
11. What should I do immediately after a rare lung cancer diagnosis?
Request full NGS molecular profiling on your tumor biopsy, seek a second pathology opinion from a major cancer center, ask for a multidisciplinary tumor board review, and search ClinicalTrials.gov for active trials specific to your rare subtype. Do not delay — treatment windows in aggressive rare types like LCNEC are time-sensitive.
This article is reviewed by the mymedicineadvisor.com Global Medical Advisory Board. Last updated: April 2026. For educational purposes only — not a substitute for professional medical advice, diagnosis, or treatment. If you are experiencing symptoms, please consult a licensed healthcare provider immediately.
About this content
This medical content is prepared through a structured publishing workflow with expert writing, clinical review and editorial quality checks.

Board Certifications: Internal Medicine (2005); Medical Oncology (2008); Hematology (2009) Experience: 20 years | Location: Houston, Texas Education: BS Biology, Duke University (1999); MD, Baylor College of Medicine…

Board Certifications: Medical Oncology (2011); Haematology (2012) Experience: 14 years | Location: New York City, New York Education: BS Biochemistry, Princeton University (2002); MD, Columbia University College of…

Board Certifications: Preventive Medicine (2010); Public Health & General Preventive Medicine (2010) Experience: 15 years | Location: Washington, DC Education: BA Public Policy, Georgetown University (2001); MD, George…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.