On This Page – Quick Medical Summary
What a lung cancer clinical trial really means for you
If you are reading this after a recent diagnosis, or after a conversation with your oncologist about limited remaining options, a lung cancer clinical trial is not what most patients think it is. It is not a last resort. It is a structured, federally regulated research study — with oversight, patient protections, and guaranteed treatment — that tests whether a new approach outperforms the current standard of care.
Use this guide based on where you are right now:
- Newly diagnosed — start with Sections 2 and 3 to understand what trials are and whether you might qualify
- Post-first-line treatment, exploring next steps — go directly to Section 3 to assess your eligibility criteria
- Caregiver supporting a family member — Section 6 is written specifically for you
Before your next oncologist appointment, use our Symptom Checker to document your current symptoms — a precise symptom record helps your oncologist evaluate your ECOG performance status more accurately.
If you are still building your foundational understanding of the disease, our complete guide to lung cancer types, stages, and treatment pathways covers everything before you explore trial options.
ℹ️ Medical Disclaimer: The clinical trial eligibility criteria, enrollment processes, insurance and Medicare coverage information, treatment options, and medication details discussed in this article reflect current clinical guidelines and federal regulations and are provided for educational purposes only. Whether a specific clinical trial is appropriate for an individual patient depends on factors including diagnosis subtype, staging, biomarker profile, ECOG performance status, prior treatment history, comorbidities, and specialist assessment. Consult a board-certified oncologist and your cancer center’s clinical trial navigator before acting on any clinical information in this article.
How lung cancer clinical trials actually work
A clinical trial is a scientific study with a defined protocol, a specific enrolled patient population, and a primary endpoint — the measurable outcome the study is designed to assess, such as progression-free survival, overall survival, or overall response rate.
The four phases of a lung cancer clinical trial
Clinical trials run in four sequential phases, each answering a different scientific question:
- Phase I — Tests safety and optimal dosing in 15–30 patients. The primary goal is identifying the maximum tolerated dose, not measuring therapeutic effectiveness.
- Phase II — Tests whether the treatment produces a measurable clinical response in a larger group. Effectiveness and the emerging side effect profile are both evaluated.
- Phase III — Compares the experimental treatment directly to the current standard of care in a randomized, controlled trial involving hundreds to thousands of patients. This is the phase most eligible lung cancer patients enroll in, and it is the phase where most breakthrough treatments are confirmed.
- Phase IV — Post-approval surveillance conducted after FDA authorization to monitor long-term safety in the broader patient population.
.
Randomization, placebo arms, and what the control group actually receives
Randomization in a Phase III lung cancer trial does not mean you might receive nothing. The control arm in virtually every Phase III lung cancer trial receives the current best available treatment — a platinum-based doublet chemotherapy regimen, an approved immunotherapy agent, or an approved targeted therapy, depending on biomarker status.
Placebo-only arms are exceptionally rare in oncology. They are used only in narrow situations where no effective standard therapy exists for the specific enrolled patient population. For any trial you are considering, ask the coordinator explicitly: what does the control arm receive?
🔬 How It Works: In a randomized Phase III trial, patients are assigned by chance to the experimental arm (new treatment) or the control arm (current best available standard therapy). Neither arm receives inferior care. The trial is testing whether the new treatment outperforms the current standard — not whether it beats nothing. This is the structural protection most patients don’t realize exists.
Who can qualify for a lung cancer clinical trial
Most lung cancer clinical trial eligibility falls into four categories: confirmed diagnosis documentation, biomarker status, ECOG performance status, and organ function. Understanding where you stand on each gives you a working starting point before your enrollment conversation.
Standard eligibility criteria most lung cancer trials require
Every trial has inclusion and exclusion criteria written into its IRB-approved protocol. Most Phase II and Phase III lung cancer trials require:
- A histologically confirmed lung cancer diagnosis with a current pathology report, typically within the past 6–12 months
- Documented completion of standard biomarker testing — at minimum EGFR mutation status, ALK rearrangement status, and PD-L1 expression percentage
- An ECOG performance status of 0, 1, or 2
- Adequate organ function confirmed on recent complete blood count and comprehensive metabolic panel
- No prior treatment with the specific drug class being studied (in most targeted therapy trials)
- At least one measurable lesion on imaging per RECIST 1.1 criteria
Biomarker-specific criteria: EGFR, ALK, ROS1, KRAS G12C, and PD-L1
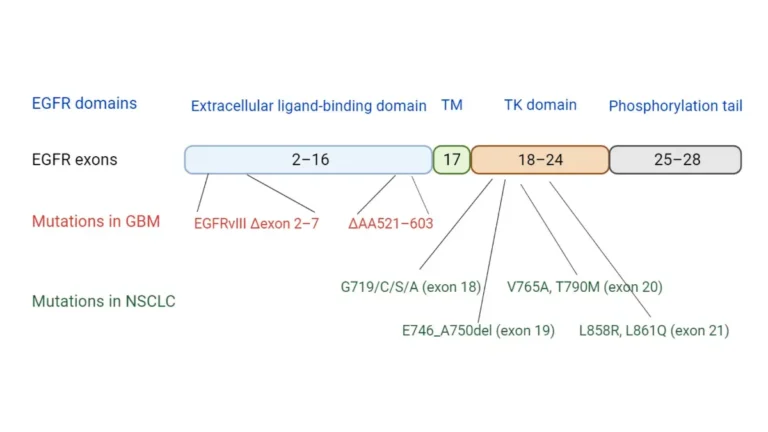
If you have had next-generation sequencing (NGS) testing done, your molecular results are the single most important document for trial eligibility. Different trials are built around specific targets:
| Mutation / Marker | What It Means for Trial Eligibility | Key Clinical Detail |
|---|---|---|
| EGFR exon 19 del or L858R | Eligible for next-generation EGFR inhibitor trials | Most appropriate for treatment-naive patients in Phase III |
| ALK rearrangement | Eligible for ALK inhibitor trials | Check prior ALK inhibitor exposure — may be exclusion criterion |
| KRAS G12C | Eligible for KRAS G12C inhibitor trials (sotorasib, adagrasib combinations) | One of the fastest-growing active trial categories in NSCLC |
| PD-L1 ≥50% | Eligible for first-line immunotherapy monotherapy trials | TPS score must be on pathology report |
| PD-L1 1–49% | May qualify for combination immunotherapy + chemotherapy trials | Combination arm eligibility varies by protocol |
| No actionable mutation (NSCLC) | Eligible for immunotherapy and novel combination trials | Broader trial pool; chemo backbone often in control arm |
| SCLC | Eligible for SCLC-specific trials only — separate from NSCLC pools | Limited-stage vs. extensive-stage criteria differ significantly |
Source: Eligibility criteria consistent with current NCCN Clinical Practice Guidelines in Oncology: Non-Small Cell Lung Cancer, 2026
.
To understand how your subtype shapes your trial options, see our detailed comparison of NSCLC and SCLC differences in diagnosis and treatment.
ECOG performance status: what the scoring scale means for your eligibility
ECOG performance status is a validated 0–4 clinical scale that measures how much a patient’s illness affects their daily functioning:
- ECOG 0 — Fully active. No restrictions on physical activity.
- ECOG 1 — Restricted in strenuous activity but fully ambulatory. Able to perform light work.
- ECOG 2 — Ambulatory. Capable of self-care. Unable to perform any work activities. Out of bed more than 50% of waking hours.
- ECOG 3 — Limited self-care. Confined to bed or chair more than 50% of waking hours.
- ECOG 4 — Completely disabled. No self-care possible.
Most Phase II and Phase III trials accept ECOG 0–2. Phase I dose-escalation trials frequently restrict enrollment to ECOG 0–1. Your oncologist calculates your ECOG score based on direct clinical assessment — it is not a patient self-report.
Your confirmed lung cancer stage and staging documentation is the first filter every trial coordinator applies when reviewing your file. Confirm your current staging records are up to date before making contact with any trial site.
✅ Patient Action: Before your next oncologist appointment, ask specifically: “Has my tumor been tested for EGFR, ALK, ROS1, KRAS G12C, PD-L1 expression, and MET amplification using a comprehensive NGS panel?” If not, request this testing — it is required before eligibility can be assessed for most currently enrolling precision oncology trials.
🩺 Physician Note: In my clinical experience, the most common reason a patient believes they are ineligible for a trial is incomplete biomarker testing — not an actual exclusion criterion. Patients whose biopsy was taken more than 12 months ago may need a fresh tissue sample or a liquid biopsy to qualify for a current protocol. Do not assume you have been ruled out until your oncologist has reviewed your complete 2026 pathology and molecular profile against the specific inclusion criteria of the trial in question. — Dr. Nathaniel J. Hargrove, MD, Oncology
Step-by-step: how to find and enroll in a lung cancer trial
Finding and enrolling in a lung cancer clinical trial begins with four steps. Most patients can begin Step 1 today — no appointment required.
Step 1: Get your biomarker and staging results in writing
Request a printed copy of your complete molecular pathology report and your most recent staging imaging report from your oncologist’s office. These two documents are required for every pre-screening conversation with a trial coordinator. Without them, no eligibility determination can be made.
Step 2: Search ClinicalTrials.gov using lung cancer filters
Go to ClinicalTrials.gov, the federally mandated registry where every IRB-approved lung cancer study in the United States must be registered before enrolling a single patient. Use these filters:
- Condition: Lung Neoplasms (or type “lung cancer”)
- Status: Recruiting
- Age: Adult
- Phase: Phase 2 or Phase 3
For a more patient-friendly starting point, the NCI’s lung cancer clinical trial search tool provides the same filtering capability with plain-language trial descriptions and a less technical interface.
Reviewing your available lung cancer treatment options alongside open trials helps you and your oncologist evaluate whether a specific trial protocol offers a meaningful advantage over the current standard of care.
Step 3: Contact the trial coordinator and complete pre-screening
Once you identify a trial of interest, call the contact number listed on the ClinicalTrials.gov entry. This is the trial coordinator at the enrolling site. That call typically involves:
- Coordinator reviews your pathology report and molecular biomarker results
- Coordinator confirms whether your ECOG status and current staging meet the protocol’s inclusion criteria
- Coordinator explains the randomization arms and the probabilities of assignment
- If initial criteria are met, a baseline visit is scheduled for formal eligibility screening
This call is not an enrollment commitment. It is an eligibility assessment conversation.

.
Step 4: Review the protocol and sign informed consent
The informed consent document is an IRB-approved legal and ethical document that must contain, by federal law: the study’s purpose, all foreseeable risks and benefits, alternative treatments available outside the trial, confidentiality protections, and an explicit statement that participation is entirely voluntary.
Signing the informed consent form is not a commitment to complete the trial. It is authorization to proceed to baseline eligibility screening. You may withdraw at any point, for any reason, without affecting your access to standard care.
Understanding how EGFR and ALK targeted therapies work for lung cancer helps you evaluate whether a biomarker-driven trial may offer a precision advantage over your current protocol.
✅ Patient Action: Ask your board-certified oncologist to provide a printed copy of your complete molecular pathology report and most recent staging imaging before contacting any trial site. These documents are required for pre-screening. Without them, no coordinator can confirm your eligibility against the protocol.
📊 Clinical Data Point: ClinicalTrials.gov lists thousands of registered lung cancer studies at any given time. Filtering to Recruiting status and Phase 2 or 3 narrows results to the trials most likely to be actively enrolling patients and offering a structured comparative treatment design. — Source: ClinicalTrials.gov, National Library of Medicine (2026)
Does insurance or Medicare cover lung cancer clinical trial costs?
The financial question stops many eligible patients before they ever reach a coordinator. The answer is more favorable than most patients expect — and it is grounded in federal law, not insurer discretion.
What Medicare covers for clinical trial participants
Under the Medicare Clinical Trial Policy, Medicare Part A and Part B cover routine care costs incurred during participation in a qualifying clinical trial. Covered routine costs include office visits, laboratory tests, diagnostic imaging, and hospitalizations related to the study treatment.
The investigational drug or device itself is provided by the trial sponsor — the pharmaceutical company or institution running the study — at no cost to the patient. You do not pay for the experimental treatment.
📊 Clinical Data Point: Medicare’s coverage of routine care costs in qualifying clinical trials is established under the Medicare Clinical Trial Policy. Routine care is defined as items and services that would typically be covered by Medicare if you were not participating in a clinical trial. — Source: Medicare’s clinical trial coverage policy, Centers for Medicare and Medicaid Services (CMS), 2026
Private insurance requirements under federal law
Under ACA Section 2709, most private health insurance plans sold in the United States are required to cover routine care costs for patients enrolled in approved clinical trials. Plans sold before the ACA’s effective date — known as grandfathered plans — may be exempt from this requirement. Verify your specific plan’s trial coverage terms with your insurer before enrollment.
Out-of-pocket costs patients should plan for
Federal law mandates routine care coverage. It does not cover:
- Travel to and from the trial site, which may be at an NCI-designated cancer center some distance away
- Lodging during multi-day treatment visits
- Time away from work or lost wages
- Experimental devices or procedures outside the formal trial scope
For a current overview of FDA-approved agents that frequently anchor the control arm of active trials, see our guide to FDA-approved lung cancer drugs and treatments in 2026.
✅ Patient Action: Before enrollment, contact your cancer center’s clinical trial navigator or patient financial advocate to verify your specific insurance plan’s trial coverage and identify any non-covered costs you should budget for. Many NCI-designated cancer centers have financial counselors dedicated to this conversation.
Benefits, real risks, and what caregivers need to know
Every eligible patient — and every caregiver — deserves an honest account of what lung cancer clinical trial participation involves. Not a promotional answer. An honest one.
What patients gain by enrolling in a Phase II or Phase III trial
In a Phase III trial, every participant receives treatment. The experimental arm receives the new agent. The control arm receives the current best available standard therapy — the same treatment your oncologist would prescribe outside the trial. There is no scenario in a Phase III lung cancer trial where you receive inferior care.
Beyond the treatment itself, enrolled patients typically receive more frequent monitoring, more thorough imaging intervals, and closer clinical attention than patients receiving standard care outside a trial setting.
For patients and caregivers weighing the potential benefit of enrollment, our breakdown of lung cancer survival statistics and prognosis by stage provides important clinical context for this decision.
.
Risks specific to early-phase (Phase I) trials
Phase I trials carry a meaningfully different risk profile than Phase III. In a Phase I dose-escalation study:
- The maximum tolerated dose has not yet been established
- Side effects may be unfamiliar or unpredictable based on preclinical data alone
- The primary goal is safety assessment, not treatment benefit for participants
- Serious or unexpected toxicities can occur at higher dose levels
If you are considering a Phase I trial, ask your oncologist for the full preclinical toxicity profile and the dose-escalation stopping rules before signing the consent form.
How caregivers can support the enrollment process
Caregivers play a specific and valuable role. At the pre-screening call, accompany the patient and take notes on randomization arm probabilities, the crossover policy, and the site visit frequency. Between visits, maintain a symptom log — trial coordinators require this data at each protocol visit. Ask about remote monitoring options if distance to the trial site is a concern.
For caregivers managing the emotional weight of this process alongside the patient, our guide to lung cancer and mental health support addresses what patients and families commonly experience during treatment decision-making.
✅ Patient Action: Ask your oncologist these three specific questions before enrollment: Which arm am I most likely to be randomized to? What does the control arm receive? What is the crossover policy if the experimental arm underperforms? These three answers give you the complete picture.
📊 Clinical Data Point: NCI guidance confirms that every enrolled clinical trial participant holds the unconditional right to withdraw from a study at any point, for any reason, without penalty and without loss of access to standard care. — Source: NCI guidance on patient protections in clinical trials, National Cancer Institute (2026)
What your oncologist may not be telling you about clinical trials
The single most persistent misconception I encounter in oncology practice is this: patients believe a clinical trial is something you pursue only after everything else has failed.
That belief costs people real options.
The most common misconception oncologists hear about clinical trials
NCCN guidelines for non-small cell lung cancer explicitly recommend that oncologists discuss clinical trial eligibility at initial staging — not only at disease progression. For certain EGFR-mutated NSCLC subtypes, the most promising active trials are specifically designed for treatment-naive patients. This means the trial is most appropriate at diagnosis, before any systemic therapy has been initiated.
Phase III trials guarantee every participant access to the current best-available standard therapy in the control arm. Participation is not a gamble. It is a structured scientific comparison with mandatory standard-of-care protection built into the protocol by federal regulatory requirement.
The question you should ask your oncologist at every appointment
At your next appointment, ask this exact question: “Based on my current subtype, stage, and biomarker profile, is there an open clinical trial you would recommend I consider?”
That phrasing prompts a protocol-level answer. “Have you thought about clinical trials?” prompts a generic response.
I’ve had patients tell me their oncologist never mentioned a trial that was actively enrolling at a center 40 miles away. The reason is often logistical — the oncologist assumed the patient wouldn’t travel — not clinical. You have to ask the question directly. A competent specialist will welcome it.
Patients who receive care at NCI-designated cancer centers have access to a substantially broader portfolio of active trials than patients at community hospitals. If your oncologist practices at a community hospital, ask whether they have a referral relationship with the nearest NCI-designated center. This is not a criticism of their care — it is a standard component of advanced cancer management.
To understand the current landscape of immunotherapy options for lung cancer — which anchor the experimental arms of many active Phase III trials — see our detailed clinical guide.
🩺 Physician Note: When a patient asks me “Is there a trial for my case?” by name and subtype, I give them a different and more useful answer than when they ask “What are my options?” The specific question unlocks a protocol-level conversation. Ask it at every appointment — at initial staging, during treatment, and at progression. — Dr. Nathaniel J. Hargrove, MD, Oncology
Lung cancer clinical trials: answers to the questions patients ask most
1. What is a clinical trial for lung cancer?
A lung cancer clinical trial is a federally regulated research study that tests a new treatment, drug combination, or diagnostic approach in patients before it becomes widely available as standard therapy. Each trial follows an IRB-approved protocol with defined eligibility criteria, treatment arms, and a specific primary endpoint — such as progression-free survival or overall response rate — that the study is designed to measure.
2. How do I find a lung cancer clinical trial near me?
Search ClinicalTrials.gov using the Condition field (Lung Neoplasms), Status (Recruiting), Age (Adult), and Phase (2 or 3). This targets actively enrolling lung cancer clinical trial studies most likely to offer a structured comparative design. NCI’s lung cancer search tool offers the same function with a patient-friendly interface. Contact the listed trial coordinator directly to discuss eligibility before your next appointment. Consult your board-certified oncologist before contacting any trial site.
3. Who qualifies for a lung cancer clinical trial?
Most lung cancer clinical trial protocols require a histologically confirmed diagnosis, completed biomarker testing (EGFR, ALK, ROS1, KRAS G12C, and PD-L1 expression), an ECOG performance status of 0, 1, or 2, and adequate organ function on recent labs. Exclusion criteria vary by protocol and often include prior treatment with the specific drug class being studied. Consult your board-certified oncologist to review your eligibility against a specific trial’s protocol before assuming inclusion or exclusion.
4. What are the four phases of a clinical trial?
Phase I tests safety and optimal dosing in a small group of 15–30 patients. Phase II evaluates whether the treatment produces a measurable response in a larger group. Phase III is the gold standard — a randomized trial comparing the experimental treatment directly to the current best standard of care. Phase IV monitors long-term safety after FDA approval. Most lung cancer clinical trial enrollment opportunities are in Phase II or Phase III.
5. Can patients with stage 4 lung cancer enroll in clinical trials?
Stage 4 lung cancer patients are among the most actively recruited populations in clinical trial research. Standard treatment options at Stage IV are limited, and many Phase III trials for advanced or metastatic NSCLC specifically require Stage IV diagnosis for enrollment eligibility. Your biomarker profile determines which specific trials match your case. Consult your board-certified oncologist to identify actively enrolling trials matched to your molecular subtype.
6. Does Medicare cover lung cancer clinical trial participation?
Under the Medicare Clinical Trial Policy, Medicare Part A and Part B cover routine care costs — including office visits, laboratory tests, and imaging — during participation in a qualifying lung cancer clinical trial. The investigational drug itself is provided by the trial sponsor at no cost. Travel, lodging, and time away from work are not covered. Consult your cancer center’s patient financial advocate to verify which costs your specific plan covers before enrollment.
7. What is ClinicalTrials.gov and how do I use it?
ClinicalTrials.gov is the federally mandated registry, maintained by the National Library of Medicine, where every IRB-approved lung cancer clinical trial in the United States must be registered before enrolling patients. To search: enter “lung cancer” in the condition field, set Status to Recruiting, set Age to Adult, and set Phase to Phase 2 or Phase 3. Each listing includes eligibility criteria, treatment arms, and the contact number for the enrolling trial coordinator.
8. What is informed consent in a clinical trial?
Informed consent is an IRB-approved process in which the trial team explains the clinical trial‘s purpose, all foreseeable risks and benefits, alternative treatments available outside the study, and your right to withdraw at any time. Signing the consent document authorizes the trial site to begin your eligibility screening — it does not commit you to completing the trial. Consult your board-certified oncologist about any section of the consent form you do not fully understand before signing.
9. Can I leave a clinical trial after I’ve enrolled?
Every enrolled clinical trial participant holds the unconditional right to withdraw from the study at any point, for any reason, without penalty. Leaving does not affect your access to standard care outside the trial. Your oncologist is obligated to continue managing your treatment regardless of your withdrawal decision. There is no minimum participation requirement once informed consent has been signed — withdrawal is always your unconditional right.
10. Will I receive a placebo in a lung cancer clinical trial?
In most lung cancer clinical trial protocols, placebo-only arms do not exist. The control arm of a Phase III trial receives the current best available standard therapy — an approved chemotherapy regimen, immunotherapy, or targeted agent depending on biomarker status. Placebo-controlled arms are used only when no effective standard treatment exists for the enrolled patient population. Consult your board-certified oncologist to confirm what the control arm receives before signing your consent form.
11. Are lung cancer clinical trials free for patients?
The investigational treatment itself is always provided free by the trial sponsor. Federal law requires Medicare and most private insurers to cover routine care costs — office visits, labs, and imaging — during participation in a qualifying lung cancer clinical trial. Costs not covered by federal mandate include travel to the trial site, lodging, and time away from work. Ask your cancer center’s patient financial advocate for a full cost breakdown specific to your trial and insurance plan.
12. How long does a lung cancer clinical trial last?
Duration varies significantly by design. Phase I and Phase II lung cancer clinical trial participation typically runs 6–24 months, though the trial’s enrollment period may span several years. Phase III trials often require 2–4 years of follow-up to collect sufficient survival data. Your participation continues until disease progression, unacceptable toxicity, or voluntary withdrawal — whichever comes first. Ask the trial coordinator for the estimated duration specific to the protocol you are considering.
13. What happens to my care if the clinical trial ends early?
If a lung cancer clinical trial closes early — due to a safety finding, funding loss, or a compelling efficacy result — your access to standard care is not affected. Your oncologist assumes immediate responsibility for your treatment. If the trial showed compelling efficacy, the sponsor may offer expanded access or compassionate use of the investigational drug while seeking FDA approval. Consult your board-certified oncologist about your treatment options if your trial site informs you of early closure.
14. What are the risks of joining an early-phase lung cancer trial?
In a Phase I lung cancer clinical trial, the maximum tolerated dose is not yet established, and side effects may be unpredictable from preclinical data alone. The primary goal is safety assessment, not treatment benefit for participants. Serious or unexpected toxicities can occur at higher dose levels. Phase I trials are generally appropriate for patients who have exhausted standard treatment options. Consult your board-certified oncologist and request the preclinical toxicity profile before consenting to a Phase I study.
15. What questions should I ask before enrolling in a clinical trial?
Before enrolling in a lung cancer clinical trial, ask: Which arm am I most likely to be randomized to? What does the control arm receive? How often are site visits required? What are the protocol-defined discontinuation criteria? What costs are not covered by my insurance? Is crossover available if the experimental arm underperforms? These questions give you a complete picture of what participation involves. Consult your board-certified oncologist before signing any trial consent document.
16. How is a clinical trial different from standard lung cancer treatment?
Standard lung cancer treatment follows FDA-approved, NCCN-recommended protocols based on proven effectiveness. A clinical trial tests whether a new approach outperforms the current standard in a structured, closely monitored setting. Trial participants typically receive more frequent imaging and closer clinical oversight than patients receiving standard care outside a trial. Participation does not replace standard care — it competes directly against it in the control arm. Consult your board-certified oncologist to evaluate whether a trial or standard therapy better matches your current disease profile.
17. What is a biomarker and why does it determine my trial eligibility?
A biomarker is a measurable biological characteristic — a genetic mutation, protein expression level, or chromosomal rearrangement — that predicts treatment response. In lung cancer clinical trial enrollment, biomarkers including EGFR mutation, ALK rearrangement, KRAS G12C, and PD-L1 expression percentage determine which trials you qualify for. Most targeted therapy trials require a specific biomarker for inclusion. Consult your board-certified oncologist about completing a comprehensive NGS panel if your molecular profile is incomplete.
Your next step toward a lung cancer clinical trial
You do not need to wait for your next appointment to begin.
Gather your molecular pathology report and your most recent staging imaging today. Then visit ClinicalTrials.gov and search using the filters from Section 4 above. Every result you see represents a federally registered study currently seeking patients with your diagnosis.
Asking your oncologist about clinical trial eligibility is always appropriate — at diagnosis, during active treatment, and at disease progression. It is not a sign of desperation. It is an informed, reasonable, and often overdue part of managing a serious illness.
Return to our comprehensive guide to lung cancer types, stages, and treatment pathways for the full clinical foundation supporting every decision ahead of you.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.