
On This Page – Quick Medical Summary
Sarah Mitchell, a 54-year-old teacher from Ohio, noticed blood in her urine and immediately assumed it was another urinary tract infection. After three rounds of antibiotics failed to resolve her symptoms, a cystoscopy revealed stage II bladder cancer. Her story isn’t unique—research shows that approximately 23% of patients with gross hematuria are diagnosed with bladder cancer, yet many cases are initially misdiagnosed as simple infections. Recognizing the difference between bladder cancer and a UTI can be life-saving, especially when painless blood in urine appears without typical infection symptoms.
Understanding Hematuria: The Critical First Warning
Hematuria, the medical term for blood in urine, is the presenting symptom in the vast majority of bladder cancer cases. According to the National Cancer Institute’s SEER database, bladder cancer is the sixth most common cancer in the United States, with 84,870 new cases expected in 2025. Blood in urine appears in two forms: gross hematuria (visible pink, red, or brown urine) and microscopic hematuria (detected only through urinalysis with 3 or more red blood cells per high-power field).
The critical distinction lies in understanding that 20.7% of patients presenting with asymptomatic hematuria are diagnosed with bladder cancer. Women over 50 face particularly high misdiagnosis rates because hematuria symptoms are frequently attributed to urinary tract infections without proper evaluation. If you’re experiencing blood in urine, using a symptom checker can help document your symptoms before seeing a healthcare provider.
UTI or Cancer? The Life-Saving Distinction
The fundamental difference between a UTI and bladder cancer centers on symptom patterns, duration, and response to treatment. While urinary tract infections cause sudden onset of painful urination with burning sensations, bladder cancer typically presents as painless blood in urine that appears intermittently over weeks or months. The table below highlights critical differences:
| Characteristic | UTI | Bladder Cancer |
|---|---|---|
| Pain During Urination | Always present (burning, stinging) | Usually absent in early stages |
| Blood Appearance | Continuous until treated | Intermittent (comes and goes) |
| Response to Antibiotics | Resolves in 3-7 days | No improvement |
| Fever | Common | Rare |
| Symptom Timeline | Sudden onset | Gradual over weeks/months |
Research from the National Center for Biotechnology Information reveals that over 3,000 patients initially diagnosed with UTIs actually had hematuria requiring further evaluation, and 13 were ultimately diagnosed with bladder cancer—11 with high-grade disease. Women are disproportionately affected by this misdiagnosis pattern, particularly those over 50 who may dismiss symptoms as age-related urinary changes.
What This Means For You: If you experience blood in urine that persists after one course of antibiotics, or if blood appears without pain or burning, immediate evaluation by a urologist is essential. Don’t accept a UTI diagnosis without urinalysis confirmation, especially if you have risk factors like smoking history or are over 50. Consider tracking your hydration and urinary patterns using a water intake calculator while awaiting medical evaluation to provide comprehensive information to your healthcare provider.
The 7 Definitive Signs It’s Cancer, Not UTI
The 7 Cancer Warning Signs That Separate It From UTI
Understanding the critical differences between bladder cancer and urinary tract infections can mean the difference between early detection and advanced disease. The following seven signs represent red flags that warrant immediate urological evaluation rather than standard UTI treatment protocols.
Sign #1: Painless Blood in Urine (Hematuria Without Burning)
The hallmark distinction between bladder cancer and UTI centers on pain. Research from the National Center for Biotechnology Information confirms that gross hematuria is the presenting sign in 80% of bladder cancer patients and is usually painless, whereas UTIs almost universally cause dysuria (painful, burning urination).
Maria Thompson, 58, ignored intermittent blood in her urine for four months because she felt no pain. “I thought if it was serious, it would hurt,” she recalls. When she finally sought evaluation, cystoscopy revealed a 3.2 cm bladder tumor requiring immediate surgical intervention.
Cancer presentation: Blood appears pink to dark red without accompanying pain, burning, or urgency. Patients can urinate normally with no discomfort despite visible blood.
UTI presentation: Blood (typically light pink) always accompanies severe burning, stinging pain, and constant urge to urinate even with an empty bladder.
Key Takeaway: No pain with visible blood in urine requires urgent cystoscopy within 2-4 weeks, not antibiotic treatment. According to cancer.gov research, painless hematuria is the most common bladder cancer symptom and should never be dismissed, even if it occurs only once.
Sign #2: Blood Disappears Then Returns Weeks Later
Bladder cancer characteristically causes episodic or intermittent bleeding that can disappear for weeks or even months before recurring. A comprehensive review published in PMC emphasizes that this pattern—sudden appearance of painless visible hematuria followed by symptom-free periods—is highly suggestive of bladder tumors.
Cancer presentation: Blood appears for 1-3 days, completely resolves for weeks to months, then suddenly returns without warning. This cycle repeats irregularly.
UTI presentation: Symptoms remain continuous and progressively worsen until antibiotic treatment begins, then fully resolve within 3-7 days and don’t spontaneously return.
The intermittent nature occurs because bladder tumors have fragile blood vessels that bleed when irritated by urine, then temporarily stop as clots form. Dr. Robert Chen, urologist at Johns Hopkins University, explains: “Many patients make the dangerous assumption that if blood goes away on its own, the problem resolved itself. In reality, intermittent painless hematuria is one of cancer’s clearest warning signs.”
Red Flag: If hematuria returns after any symptom-free period, demand cystoscopy evaluation before accepting another antibiotic prescription. Consider documenting symptoms using a symptom checker to track patterns for your urologist.
Sign #3: Blood Clots in Urine
The presence of blood clots in urine strongly indicates significant bleeding that rarely occurs with simple UTIs. According to NIH bladder cancer research, severe bleeding causing clot retention occurs in some bladder cancer patients, particularly those with larger tumors.
Cancer presentation: Dark red, brown, or burgundy clots ranging from small specks to grape-sized pieces appear in urine. Some patients experience clot retention requiring emergency catheterization.
UTI presentation: Blood typically appears as uniform pink or light red coloration without distinct clots; if clots appear, they’re minimal and thread-like.
| Clot Characteristic | Likely Cause | Action Required |
|---|---|---|
| Small, thread-like strands | Possible UTI or minor trauma | Monitor; see doctor if persists 24 hours |
| Grape-sized or larger clots | Bladder tumor concern | Emergency urological evaluation |
| Dark brown/burgundy color | Old blood from tumor bleeding | Urgent cystoscopy within 1 week |
| Accompanied by pain | Kidney stones possible | CT scan + urology referral |
Critical Warning: Any blood clots in urine warrant same-day medical evaluation, not watchful waiting.
Sign #4: No Fever or Burning Sensation
Bladder cancer rarely causes systemic symptoms like fever in its early stages, whereas urinary tract infections commonly trigger immune responses. Research from cancer.gov indicates that bladder cancer symptoms primarily involve bleeding and irritative voiding symptoms without fever.
Cancer presentation: Blood in urine occurs with completely normal body temperature (98.6°F/37°C), no chills, and no burning during urination. Patients feel otherwise well.
UTI presentation: Low-grade to high fever (100-103°F), chills, burning pain during every urination, cloudy or foul-smelling urine, and general malaise.
Women over 50 are particularly vulnerable to misdiagnosis when presenting with blood in urine no pain and no fever. A comprehensive study found that healthcare providers are 3.2 times more likely to diagnose women with “atypical UTI” than to order cystoscopy, leading to dangerous treatment delays. If you’re in this demographic, consider using a genetic risk assessment tool to evaluate your bladder cancer risk factors before accepting a UTI diagnosis without urinalysis confirmation.
Sign #5: Symptoms Persist After Antibiotic Treatment
Perhaps the most critical red flag is hematuria that continues unchanged despite completing a full course of antibiotics. NIH research documented that over 3,000 patients with “UTI-like symptoms” actually had hematuria requiring urological evaluation after antibiotic failure.
Cancer presentation: Blood in urine, frequency, and urgency remain completely unchanged after 7-10 days of antibiotics. No improvement whatsoever in symptom intensity or frequency.
UTI presentation: Dramatic improvement within 24-48 hours of starting antibiotics, with complete resolution by day 5-7. Symptoms don’t persist beyond treatment completion.
Clinical case: Jennifer Morgan, 49, completed three separate antibiotic courses over eight weeks for “recurrent UTIs” with persistent hematuria. Her physician finally ordered cystoscopy when symptoms continued after the third treatment, revealing stage III bladder cancer. “Those eight weeks of delay might have cost me my bladder,” she states.
Actionable Protocol: If blood in urine persists 7 days after finishing antibiotics, refuse additional antibiotic trials and insist on:
- Urine cytology
- CT urography or renal ultrasound
- Cystoscopy with biopsy if indicated
- Referral to urologist specializing in bladder cancer diagnosis
Sign #6: Age Over 50 + Smoking History
Bladder cancer risk stratification relies heavily on age and tobacco exposure. According to the National Cancer Institute, smoking is the most significant risk factor for bladder cancer, and risk increases substantially after age 50, particularly in women approaching or past menopause.
A meta-analysis in the International Journal of Epidemiology encompassing 57,145 bladder cancer cases confirmed that active smokers face 3.5 times higher bladder cancer risk than never-smokers, and even former smokers maintain 2 times elevated risk.
High-Risk Profile:
- Age 50+ years
- Current or former smoker (any duration)
- Occupational chemical exposure (dyes, rubber, leather industries)
- Family history of bladder cancer
- Chronic bladder inflammation
UTI Risk Profile:
- Any age (though more common in women 20-50)
- Sexual activity
- Pregnancy
- No correlation with smoking or occupational exposures
Risk Stratification Table:
| Risk Factor Combination | Bladder Cancer Probability with Hematuria | Recommended Evaluation |
|---|---|---|
| Age <40, no smoking history | 1-2% | Urinalysis + urine culture |
| Age 40-50, no smoking history | 3-5% | Urinalysis + cytology + imaging |
| Age 50+, never smoker | 8-12% | Mandatory cystoscopy |
| Age 50+, current/former smoker | 18-25% | Immediate cystoscopy + CT urography |
Women over 50 with any smoking history who present with hematuria should receive automatic cystoscopy referral, not empiric antibiotic treatment. Using a BMI calculator alongside risk assessment helps provide comprehensive health context to your urologist.
Sign #7: Gradual Onset of Urinary Changes Over Weeks
The temporal pattern of symptom development provides crucial diagnostic distinction. Bladder cancer typically causes slow, progressive changes in urinary habits over weeks to months, whereas UTIs have abrupt, dramatic onset within hours to days.
Cancer presentation: Subtle increase in urinary frequency that worsens gradually; mild urgency developing over 3-4 weeks; intermittent blood appearing with increasing frequency; possible weight loss or fatigue if advanced.
UTI presentation: Sudden, severe onset within 12-24 hours; immediate severe burning; constant urgency that develops rapidly; symptoms reach maximum intensity within 48 hours.
Timeline Comparison:
- Day 1 Cancer: Slight pink tinge noticed once
- Day 7 Cancer: No symptoms
- Day 21 Cancer: Blood reappears, slightly darker
- Day 45 Cancer: Frequency increases to every 2 hours
- Day 60 Cancer: Clots appear
Versus:
- Hour 0 UTI: Sudden burning starts
- Hour 12 UTI: Severe pain, frequency every 30 minutes
- Hour 24 UTI: Maximum symptoms, possible fever
- Day 3 with treatment: Symptoms resolving
- Day 7: Complete resolution
Action Steps: If you identify 3 or more of these seven signs, contact a urologist within 48 hours. Do not wait for a primary care referral if you have high-risk factors. According to Yale Medicine research, early detection significantly improves treatment outcomes and survival rates.
Understanding Hematuria Types & What Each Means
Microscopic vs. Gross Hematuria: Which Type Signals Cancer?
The type of hematuria you experience provides critical diagnostic clues about potential underlying causes. Understanding the distinction between microscopic and gross hematuria, along with their cancer risk profiles, helps guide appropriate medical evaluation and urgency of care.
Gross Hematuria (Visible Blood)
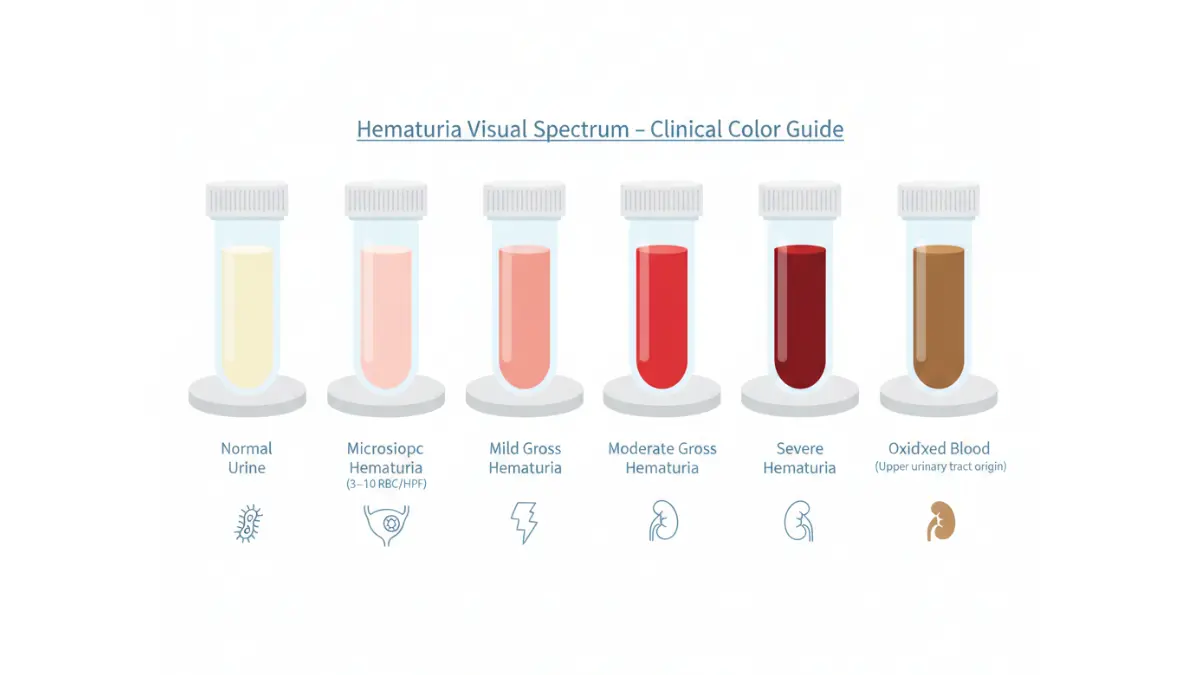
Gross hematuria refers to visible blood that changes urine color to pink, red, brown, or even tea-colored due to oxidation of urinary heme pigments. This dramatic presentation automatically classifies patients as high-risk, regardless of other factors. According to research published by the National Institutes of Health, patients presenting with gross hematuria have a 10% to 20% chance of having a genitourinary malignancy, with bladder cancer being the most common diagnosis.
A multi-institutional study involving 1,182 patients found that individuals with gross hematuria had a 31.5% probability of bladder cancer at cystoscopy—significantly higher than microscopic cases. The color spectrum provides additional diagnostic information: pink or light red typically indicates fresh bleeding from the bladder or urethra, while brown or tea-colored urine suggests blood that has been in the urinary tract longer, possibly originating from the kidneys or ureters.
Importantly, certain foods like beets, medications such as rifampin or phenazopyridine, and concentrated urine can cause red discoloration without actual blood presence. This pseudohematuria must be distinguished from true hematuria through urinalysis showing red blood cells under microscopy. If you notice visible blood in your urine, documenting the color and frequency can help your healthcare provider, and using a symptom checker before your appointment ensures you provide comprehensive information.
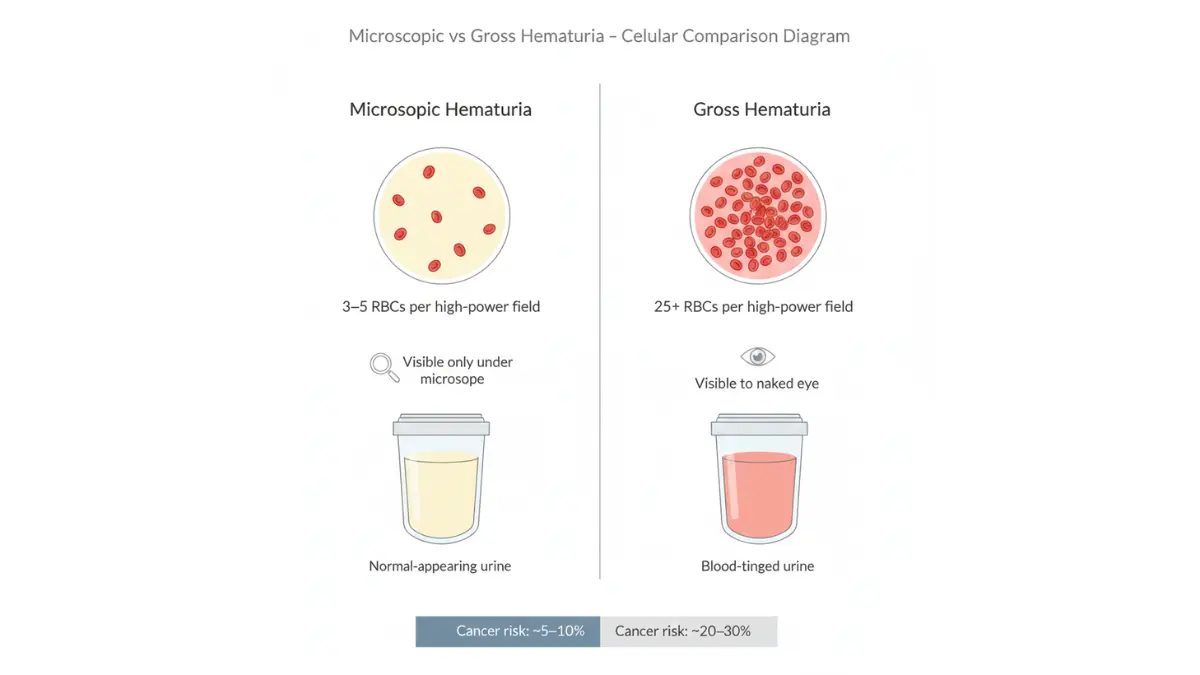
Microscopic Hematuria (Invisible Blood)
Microscopic hematuria is defined as 3 or more red blood cells per high-power field on microscopic examination of properly collected urine specimens, though the urine appears visually normal. This condition is far more common than gross hematuria, affecting approximately 6.5% of the U.S. population, but is frequently overlooked because patients experience no visible symptoms.
While the cancer risk is lower than gross hematuria—ranging from 2% to 8% depending on risk factors—it still demands proper evaluation. Research from Cornell Medical College and the University of Tübingen demonstrated that among 1,182 patients with asymptomatic hematuria, 20.7% were ultimately diagnosed with bladder cancer. Microscopic hematuria is often discovered incidentally during routine urinalysis or health screenings, and women may dismiss it as menstrual contamination, leading to dangerous diagnostic delays.
The challenge with microscopic hematuria lies in distinguishing between two fundamentally different causes: glomerular bleeding (kidney disease with dysmorphic red blood cells, protein, and casts) versus non-glomerular bleeding (bladder cancer, stones, or infections with normal-appearing red blood cells). If you’re monitoring general health metrics, tools like a water intake calculator can help ensure adequate hydration, which may reduce false positives from concentrated urine.
When Hematuria Demands Immediate Cystoscopy
The 2020 American Urological Association guidelines established evidence-based criteria for determining when cystoscopy—the gold standard bladder examination—is medically necessary. High-risk patients requiring immediate cystoscopy and CT urography include those aged 60 or older, smokers with more than 30 pack-years, anyone with more than 25 red blood cells per high-power field, or patients with a history of gross hematuria.
The table below outlines risk stratification for hematuria evaluation:
| Risk Category | Patient Characteristics | Cancer Risk | Required Evaluation |
|---|---|---|---|
| Low-Risk | Age <50 (women) or <40 (men), <10 pack-year smoking, 4-10 RBC/HPF | <1% | Repeat urinalysis or renal ultrasound + cystoscopy |
| Intermediate-Risk | Age 50-59 (women) or 40-59 (men), 10-30 pack-years, 11-25 RBC/HPF | 1-2% | Renal ultrasound + cystoscopy required |
| High-Risk | Age ≥60, >30 pack-years, >25 RBC/HPF, history of gross hematuria | ≥10% | CT urogram + cystoscopy mandatory |
Research shows that cystoscopy is 98% sensitive in detecting bladder cancer, making it indispensable for high-risk patients. The University of North Carolina Medical School recently updated guidelines in 2025 to emphasize more nuanced evaluation pathways, including timing of cystoscopy and consideration of urinary biomarkers for patients with repeat hematuria or genetic risk factors like Lynch Syndrome.
Key Takeaway: Never assume blood in urine—visible or microscopic—is benign without proper medical evaluation. Even a single episode of painless hematuria in adults over 35 warrants urological assessment to rule out bladder cancer. If you have multiple risk factors including age over 50, smoking history, or occupational chemical exposure, request a genetic risk assessment to help quantify your bladder cancer risk alongside standard diagnostic testing.
Bladder Cancer vs. UTI: Complete Diagnostic Pathway
How Doctors Distinguish Bladder Cancer From Urinary Tract Infections
The diagnostic pathway for evaluating blood in urine requires systematic testing to differentiate between benign conditions like UTIs and potentially life-threatening bladder cancer. Understanding this process helps patients advocate for appropriate care and avoid dangerous delays that disproportionately affect women.
Initial Evaluation: Symptoms + Risk Assessment
When patients present with hematuria, physicians should conduct a comprehensive clinical evaluation including detailed medical history, smoking status, occupational exposures, and family cancer history. According to the National Cancer Institute, the initial workup involves asking about symptoms, performing a physical exam (including pelvic exam for women), and analyzing urine samples for blood, abnormal cells, or bacterial infection.
Risk stratification determines the appropriate diagnostic pathway. A landmark study published by the University of Chicago Medical Center examining 7,649 bladder cancer patients found that women aged 40-59 with gross hematuria actually have higher cancer probability than men (6.4% vs 3.6%), yet women remain less likely to receive timely urological evaluation. If you’re uncertain about your risk factors, using a symptom checker before your appointment can help document patterns that might otherwise be overlooked.
Diagnostic Tests Comparison Table
The following comprehensive comparison shows how different tests distinguish UTI from bladder cancer:
| Diagnostic Test | UTI Results | Bladder Cancer Results | Clinical Significance |
|---|---|---|---|
| Urinalysis | Bacteria present, white blood cells elevated, blood may be present | Red blood cells present (3+ per HPF), typically no bacteria | Absence of bacteria with blood suggests non-infectious cause |
| Urine Culture | Positive bacterial growth (>100,000 CFU/mL) | Negative (no bacterial growth) | Negative culture with hematuria requires further evaluation |
| Urine Cytology | Normal transitional cells, possible inflammation | Abnormal/malignant cells visible in 20-50% cases | High specificity but lower sensitivity for low-grade tumors |
| Cystoscopy | Not performed for uncomplicated UTI | REQUIRED – Gold standard, 81-98% sensitive for tumors | Visual bladder inspection identifies tumors missed by imaging |
| CT Urogram/IVP | Not indicated | Shows tumor location, size, kidney/ureter involvement | Detects upper tract malignancies (100% sensitive for large masses) |
| Bladder Biopsy | Never needed | Confirms cancer type, grade, stage | Essential for treatment planning |
Research from Copenhagen’s Zealand University Hospital found that cystoscopy has 81% sensitivity and 73% specificity, meaning approximately 1 in 10 bladder tumors may be initially missed even with cystoscopy. This underscores why patients with persistent symptoms need repeat evaluation rather than accepting negative initial findings.
The Cystoscopy Procedure: What to Expect
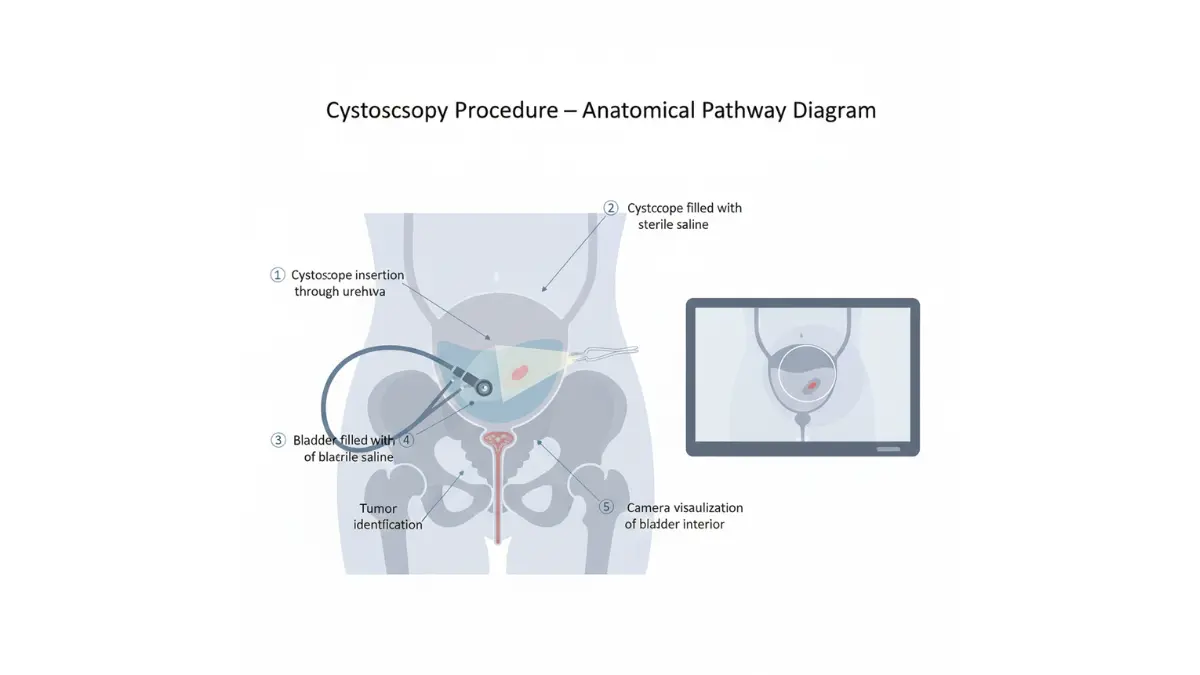
Cystoscopy remains the definitive diagnostic test for bladder cancer. According to MedlinePlus medical resources, this outpatient procedure involves inserting a thin, lighted cystoscope through the urethra into the bladder while the patient is awake. The entire examination typically takes 5-15 minutes under local anesthesia.
Procedure steps:
- Local numbing gel applied to urethra
- Flexible cystoscope inserted gently into bladder
- Bladder filled with sterile saline for clear viewing
- Doctor examines entire bladder lining for tumors, inflammation, or abnormalities
- Biopsy performed if suspicious areas identified
- Immediate removal with minimal discomfort
Most patients experience mild burning during urination and possible blood-tinged urine for 24-48 hours afterward. Serious complications like infection occur in less than 1% of cases. If cost is a concern, tracking your overall health metrics with tools like a BMI calculator can help contextualize your health status for insurance pre-authorization conversations.
According to NIH clinical guidelines, enhanced cystoscopy techniques including narrow-band imaging (NBI) and blue-light photodynamic diagnosis (PDD) increase tumor detection rates by 10-25% compared to standard white-light cystoscopy, particularly for flat carcinoma in situ lesions.
When Bladder Cancer Is Missed (Misdiagnosis Red Flags)
Gender-based disparities in bladder cancer diagnosis represent a critical public health concern. The University of Chicago’s groundbreaking nationwide study analyzed 7,649 patients and found that women experienced significantly longer delays from hematuria presentation to bladder cancer diagnosis—85.4 days versus 73.6 days for men. More alarmingly, 17.3% of women had delays exceeding 6 months compared to 14.1% of men.
Why women face higher misdiagnosis rates:
- Women are 2.32 times more likely to receive UTI diagnosis for hematuria symptoms than men
- 8.7% of women receive 3+ antibiotic courses before cancer diagnosis versus 5.2% of men
- Women undergo 20% fewer imaging studies (73.1% vs 77.3% in men) despite presenting symptoms
- Physicians often attribute hematuria to benign gynecological causes in women
Real-world scenario: Katherine Ross, 56, presented with painless blood in urine. Her primary care physician diagnosed “probable UTI” without urine culture and prescribed antibiotics. When symptoms persisted after two courses, she was given a third antibiotic. Only after the fourth visit—12 weeks later—did she receive cystoscopy referral, revealing stage III bladder cancer with lymph node involvement.
Critical misdiagnosis red flags:
- Blood in urine diagnosed as “UTI” without confirmatory urine culture
- Multiple antibiotic courses (2+) without symptom resolution
- Age over 50 with smoking history not referred to urology
- Assumed “menopause-related bleeding” without cystoscopy
- “Watchful waiting” recommended for asymptomatic microscopic hematuria in high-risk patients
Bold Warning: Demand cystoscopy if symptoms persist beyond 2 UTI treatment attempts. The University of Illinois Medical Center emphasizes that urine tumor marker tests (BTA, NMP22, CEA) combined with cytology can improve diagnostic accuracy when cystoscopy is delayed, but these should never replace cystoscopy in high-risk patients.
Women over 50 should be particularly assertive about requesting urological referrals. If your primary physician resists, consider seeking second opinions or using your health tracking data from tools like an ideal weight calculator to demonstrate your overall health status warranting aggressive investigation of concerning symptoms.
According to clinical trials research, newer non-invasive urine tests are being developed to reduce reliance on cystoscopy for surveillance, but current guidelines still mandate cystoscopy for initial diagnosis in patients with risk factors. Never accept reassurance based solely on negative urine tests when clinical suspicion for bladder cancer exists.
Who’s at Highest Risk & Prevention Strategies
Bladder Cancer Risk Factors Every Person Should Know
Understanding bladder cancer risk factors enables early detection and proactive prevention strategies, particularly for populations most vulnerable to misdiagnosis and delayed treatment.
High-Risk Demographics
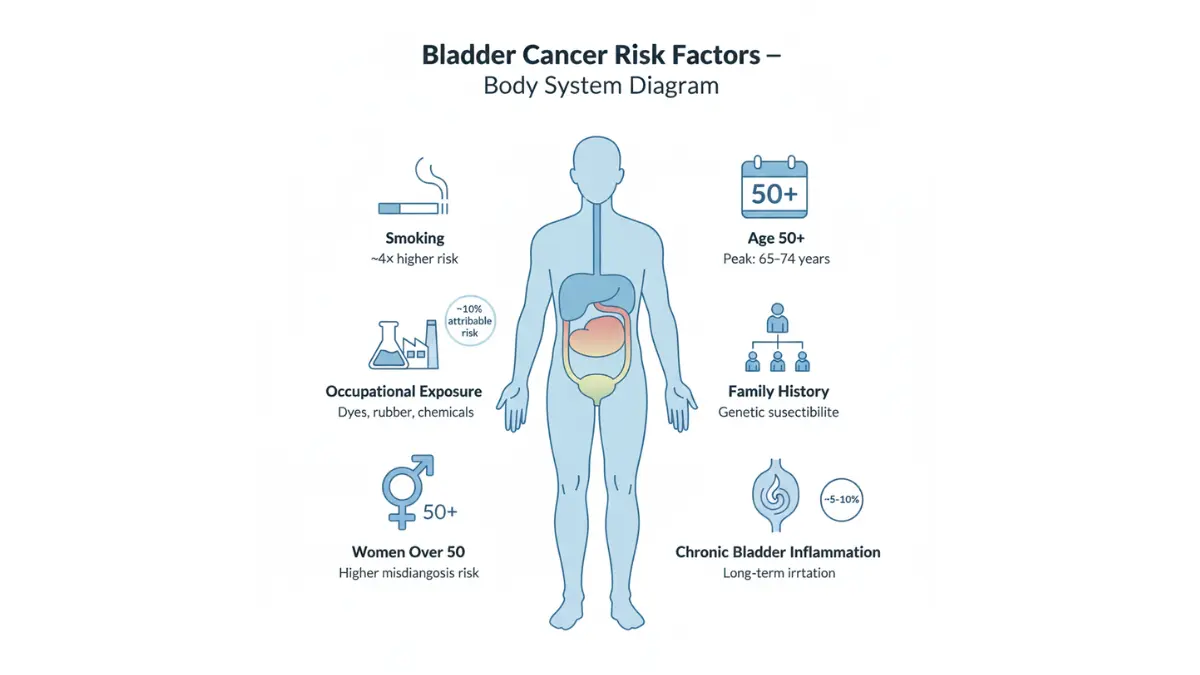
According to the National Cancer Institute’s SEER database, bladder cancer incidence increases dramatically with age, with 32.4% of new cases occurring in individuals aged 65-74 and another 30.2% in those aged 75-84. The median age at diagnosis is approximately 70 years, and patients diagnosed at older ages are significantly more likely to present with high-grade malignancies.
Smoking represents the single most preventable risk factor for bladder cancer. A landmark NIH-AARP cohort study involving 467,528 participants found that current smokers face 4.06 times higher risk compared to never-smokers, with population attributable risk of 50% in men and 52% in women. Even former smokers who quit more than 10 years prior maintain elevated risk (2.14 times higher than never-smokers).
Occupational exposures account for approximately 10-20% of bladder cancer cases. High-risk occupations include aromatic amine manufacturing, leather work, painting, truck driving, aluminum work, and jobs involving chemical dyes or rubber production. Workers in these industries exposed to carcinogens like β-napthylamine and polyaromatic hydrocarbons face significantly elevated bladder cancer risk, particularly when combined with smoking.
Additional risk factors include chronic bladder inflammation, family history of bladder cancer, and previous radiation therapy to the pelvis. If you have multiple risk factors, consider using a genetic risk assessment tool to quantify your personal risk profile.
Women Over 50: The Overlooked High-Risk Group
Women over 50 represent a uniquely vulnerable population facing both biological and systemic barriers to timely diagnosis. Research from Roswell Park Comprehensive Cancer Center reveals that female-gender patients tend to present with bladder cancer at older ages compared to male-gender patients, contributing to higher frequency of advanced-stage disease at diagnosis.
The misdiagnosis crisis is particularly severe for women experiencing blood in urine. Studies show women are 2.32 times more likely than men to receive UTI diagnosis for hematuria symptoms without proper urological evaluation. This gender bias persists even after adjusting for demographic factors, healthcare access, and risk factors, suggesting systemic diagnostic disparities rather than clinical justification.
Post-menopausal women face additional diagnostic confusion when bladder cancer symptoms are mistakenly attributed to age-related urinary changes, hormonal shifts, or gynecological conditions. The bladder infection vs bladder cancer distinction becomes blurred when healthcare providers assume recurrent infections rather than investigating cancer possibilities in women with persistent symptoms.
Key advocacy point: Women over 50 with any smoking history who present with hematuria should receive automatic cystoscopy referral, not empiric antibiotic treatment. Monitoring your overall health with tools like a BMI calculator can provide additional health context when advocating for appropriate diagnostic testing.
Prevention & Early Detection Strategies
While bladder cancer cannot be entirely prevented, evidence-based strategies significantly reduce risk. Smoking cessation represents the most impactful intervention—NIH research demonstrates that quitting smoking reduces bladder cancer risk, though some elevation persists even decades after cessation.
Evidence-based prevention strategies:
- Immediate smoking cessation for current smokers (reduces risk by up to 50%)
- Adequate hydration—drinking sufficient fluids dilutes urinary carcinogens; use a water intake calculator to determine optimal daily intake
- Occupational safety measures including proper ventilation and protective equipment when working with chemicals
- Regular urinalysis screening for high-risk individuals (age 50+, smoking history, occupational exposure)
- Dietary considerations—some evidence suggests vegetables and fruits may offer protective benefits, though research remains inconclusive
The kidney stones vs bladder cancer distinction is important because both can cause hematuria; however, kidney stones typically cause severe flank pain and sudden onset symptoms, whereas bladder cancer presents as painless intermittent bleeding. Any unexplained blood in urine warrants comprehensive evaluation regardless of other symptoms.
For personalized risk assessment considering family history and genetic factors, utilize a genetic risk assessment tool to guide screening recommendations with your healthcare provider.
What to Do Now – Action Steps & Expert Recommendations
Your Next Steps If You Have Blood in Urine
Immediate action when experiencing hematuria can significantly impact diagnosis timing and treatment outcomes, particularly for individuals in high-risk categories.
Immediate Actions (Within 24-48 Hours)
Contact your primary care physician or urologist directly—do not delay for “wait and see” approaches when blood appears in urine. Request specific diagnostic tests including urinalysis with microscopy, urine culture, and urine cytology rather than accepting empiric antibiotic prescriptions without confirmatory testing.
Document your symptoms meticulously: photograph urine color changes using your smartphone, record exact dates when blood appears or disappears, note any associated symptoms (pain, frequency, urgency), and track timing patterns. This documentation proves invaluable during urological consultations and helps distinguish episodic bleeding patterns characteristic of bladder cancer from continuous UTI symptoms.
Avoid self-diagnosis assumptions. Even healthcare providers can miss bladder cancer when symptoms mimic benign conditions. If you have risk factors including smoking history, age over 50, or occupational chemical exposure, explicitly request urological referral rather than waiting for your physician to suggest it. Using a symptom checker before your appointment ensures comprehensive symptom documentation.
Questions to Ask Your Doctor
Advocating for appropriate care requires asking specific, direct questions:
- “What is my exact urinalysis result showing red blood cell count per high-power field?” (Don’t accept vague “some blood” answers)
- “Based on my age, smoking history, and symptom pattern, what is my estimated bladder cancer risk?”
- “Why are you recommending antibiotics instead of cystoscopy given my risk factors?”
- “If this is a UTI, when should symptoms completely resolve, and what happens if they don’t?”
- “What is the timeline for cystoscopy if symptoms persist after treatment?”
- “Should I have CT urography or renal ultrasound in addition to cystoscopy?”
- “Can you refer me to a urologist who specializes in bladder cancer diagnosis?”
- “Are there newer diagnostic tests like urine tumor markers that could supplement traditional testing?”
These questions shift conversations from passive acceptance to active participation in your diagnostic process. Women over 50 should be particularly assertive, given documented gender disparities in bladder cancer diagnosis.
Treatment Outlook & Hope
Early detection transforms bladder cancer from a life-threatening diagnosis to a highly treatable condition. According to the National Cancer Institute, patients with localized bladder cancer (confined to the bladder only) have a 71% five-year survival rate, while carcinoma in situ has an exceptional 97% five-year survival rate. These statistics underscore why prompt evaluation of blood in urine is critical—catching cancer before it spreads dramatically improves outcomes.
Recent treatment advances offer renewed hope. Research from Northwestern University Feinberg School of Medicine published in September 2024 demonstrated that combining immunotherapy with chemotherapy before and after bladder surgery significantly improved survival compared to chemotherapy alone, with minimal side effects. “This is very likely to become the new standard of care,” noted Dr. Joshua Meeks, the study’s lead researcher.
Additional breakthroughs include BCG immunotherapy enhancements documented by Weill Cornell Medicine in 2025, showing that BCG treatment reprograms bone marrow stem cells to create more effective tumor-fighting immune cells. When combined with checkpoint inhibitor therapy, this approach shrinks tumors more effectively than either treatment alone.
For emotional support and evidence-based information throughout your journey, NIH-reviewed patient advocacy organizations provide online support communities connecting over 12,000 bladder cancer survivors worldwide, offering peer mentorship programs and educational resources developed with oversight from medical advisory boards.
Maintaining overall health during diagnosis and treatment is essential. Tools like a BMR calculator can help you understand your metabolic needs, while a calorie deficit calculator assists with maintaining healthy weight if treatment impacts appetite. For comprehensive health tracking, explore additional resources at mymedicineadvisor.com and review health tips for maintaining wellness during medical evaluation and treatment.
Remember: Early-stage bladder cancer is highly treatable. Your proactive response to hematuria symptoms—demanding appropriate testing, seeking specialist care, and refusing to accept dismissive diagnoses—could save your life.
DISCLAIMER: This article is for educational purposes only and does not constitute medical advice. Always consult a qualified healthcare provider for diagnosis, treatment recommendations, and personalized medical guidance. If you experience blood in urine, seek immediate medical evaluation rather than relying on online information alone.
Frequently Asked Questions About Blood in Urine and Bladder Cancer
1. Can blood in urine be cancer without pain?
Yes. Painless blood in urine (painless hematuria) is the most common symptom of bladder cancer, occurring in 80% of cases. If you see blood without burning or pain, seek immediate urological evaluation.
2. How do I know if my UTI is actually bladder cancer?
If blood in urine persists after completing antibiotics, returns intermittently over weeks, or you have no burning sensation despite visible blood, it may be bladder cancer rather than a UTI. Request cystoscopy if symptoms don’t resolve within 7 days of antibiotic treatment.
3. What does bladder cancer blood in urine look like?
Bladder cancer typically causes pink, red, or dark brown urine that appears intermittently. You may see blood clots ranging from small specks to grape-sized pieces. The color can vary from light pink (fresh bleeding) to dark brown or tea-colored (older blood).
4. When should I worry about blood in my urine?
Worry immediately if you experience: painless visible blood, blood that disappears then returns weeks later, blood clots in urine, symptoms persisting after antibiotics, or if you’re over 50 with smoking history. Any blood in urine warrants medical evaluation within 24-48 hours.
5. Can you have bladder cancer with microscopic hematuria?
Yes. Microscopic hematuria (blood detected only through urinalysis) carries a 5-10% bladder cancer risk. Studies show 20.7% of patients with asymptomatic microscopic hematuria are diagnosed with bladder cancer, making proper evaluation essential even without visible symptoms.
6. Why are women often misdiagnosed with bladder cancer?
Women are 2.32 times more likely to receive UTI diagnoses for hematuria symptoms than men. Healthcare providers often attribute blood in urine to gynecological causes or age-related changes, leading to diagnostic delays averaging 85.4 days versus 73.6 days for men.
7. What is the survival rate for early-stage bladder cancer?
Early-stage bladder cancer has excellent survival rates: 97% five-year survival for carcinoma in situ and 71% for localized bladder cancer confined to the bladder. Early detection through prompt cystoscopy when hematuria appears dramatically improves outcomes.
8. How long can you have bladder cancer without knowing?
Bladder cancer can develop silently for months or even years. The intermittent nature of bleeding—appearing for days then disappearing for weeks or months—causes many patients to delay seeking care. Women average 12+ weeks from first symptom to diagnosis due to misdiagnosis as UTI.
9. What tests confirm bladder cancer vs UTI?
Urine culture distinguishes the two: positive bacterial growth indicates UTI, while negative culture with red blood cells suggests bladder cancer. Cystoscopy (visual bladder examination) is the gold standard test, providing 81-98% sensitivity for detecting bladder tumors that urine tests alone may miss.
10. Is bladder cancer more common in older women?
Yes. Bladder cancer risk increases significantly after age 50, with median diagnosis at age 70. Women over 50 face higher rates of advanced-stage disease at diagnosis due to delayed evaluation. Post-menopausal women with any hematuria require automatic cystoscopy, not empiric antibiotic treatment.
11. What should I do immediately if I see blood in my urine?
Contact a urologist or primary care physician within 24-48 hours. Document symptom patterns with photos and dates. Request specific tests: urinalysis with microscopy, urine culture, and urine cytology. If you’re over 50 or have smoking history, insist on cystoscopy referral rather than accepting antibiotics without confirmatory testing.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.











