
On This Page – Quick Medical Summary
What Is Multiple Myeloma? Understanding This Blood Cancer in 2026
Multiple myeloma is a blood cancer affecting plasma cells in the bone marrow, with 62.4% of patients now surviving five years or longer thanks to breakthrough treatments approved in 2026.
James Martinez, a 67-year-old retired teacher from Phoenix, noticed persistent back pain and fatigue in early 2025. After months of assuming it was age-related, his doctor discovered abnormal proteins in his blood. The diagnosis: multiple myeloma. “I thought it was a death sentence,” James recalls. “But my oncologist explained how treatment has transformed in just the past few years.”
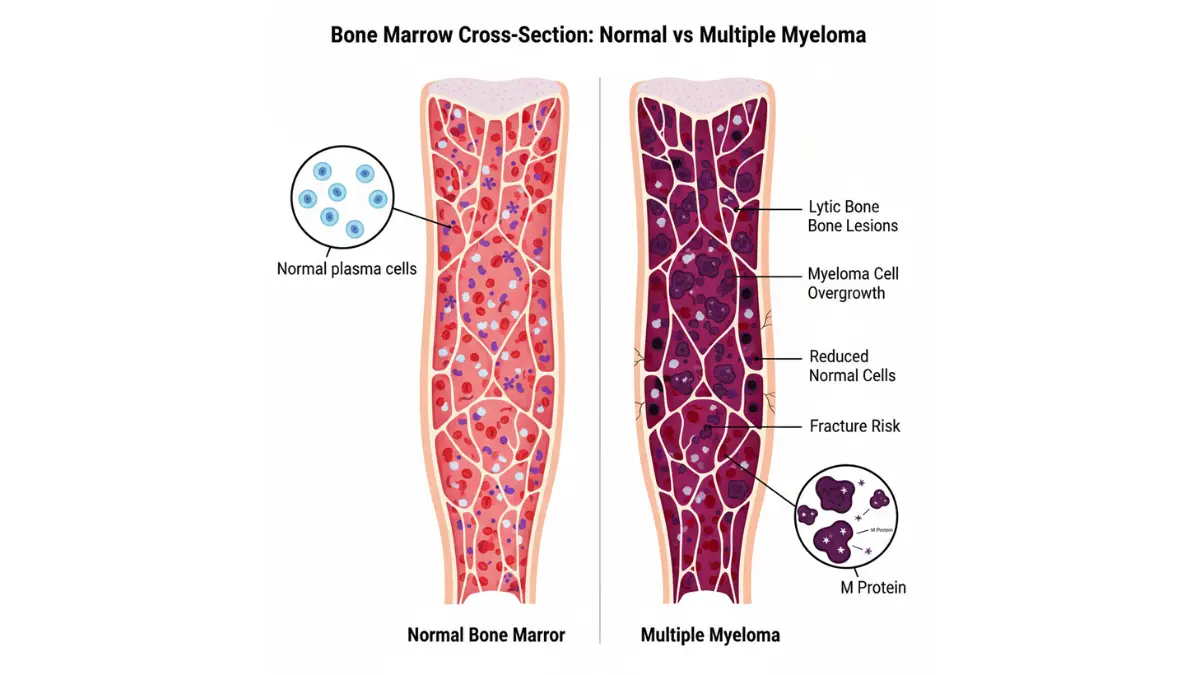
Multiple myeloma occurs when plasma cells—white blood cells that produce antibodies—become cancerous and multiply uncontrollably in the bone marrow. These malignant cells crowd out healthy blood cells and produce abnormal M proteins that damage kidneys and weaken bones.
Quick Facts About Multiple Myeloma:
- New cases in 2026: Approximately 36,110 Americans will be diagnosed this year
- 5-year survival rate: 62.4% (up from 35% in the 1990s)
- Median age at diagnosis: 69 years old
- Gender disparity: More common in men than women
- Racial factors: Black Americans diagnosed at twice the rate of white Americans
The disease typically manifests through bone pain (especially in the back and ribs), frequent infections, fatigue, and kidney problems. Many patients also experience the CRAB symptoms—high Calcium levels, Renal impairment, Anemia, and Bone damage.
Unlike many cancers, multiple myeloma is currently considered treatable but not curable. However, the genetic factors that influence individual prognosis are better understood than ever before, allowing for increasingly personalized treatment approaches.
2026 Treatment Breakthroughs: Why Survival Rates Are Climbing
FDA-Approved Quadruplet Regimen (January 2026)
On January 27, 2026, the FDA approved a game-changing combination therapy that’s already reshaping frontline myeloma treatment. The new quadruplet regimen combines daratumumab with bortezomib, lenalidomide, and dexamethasone—four drugs working synergistically to attack cancer cells through multiple pathways.
Dr. Rajesh Patel, a hemato-oncologist at Cleveland Clinic, explains: “This approval represents the most significant advancement in first-line myeloma therapy since 2015. Patients receiving this combination achieve deeper remissions faster, with median progression-free survival extending beyond five years in many cases.”
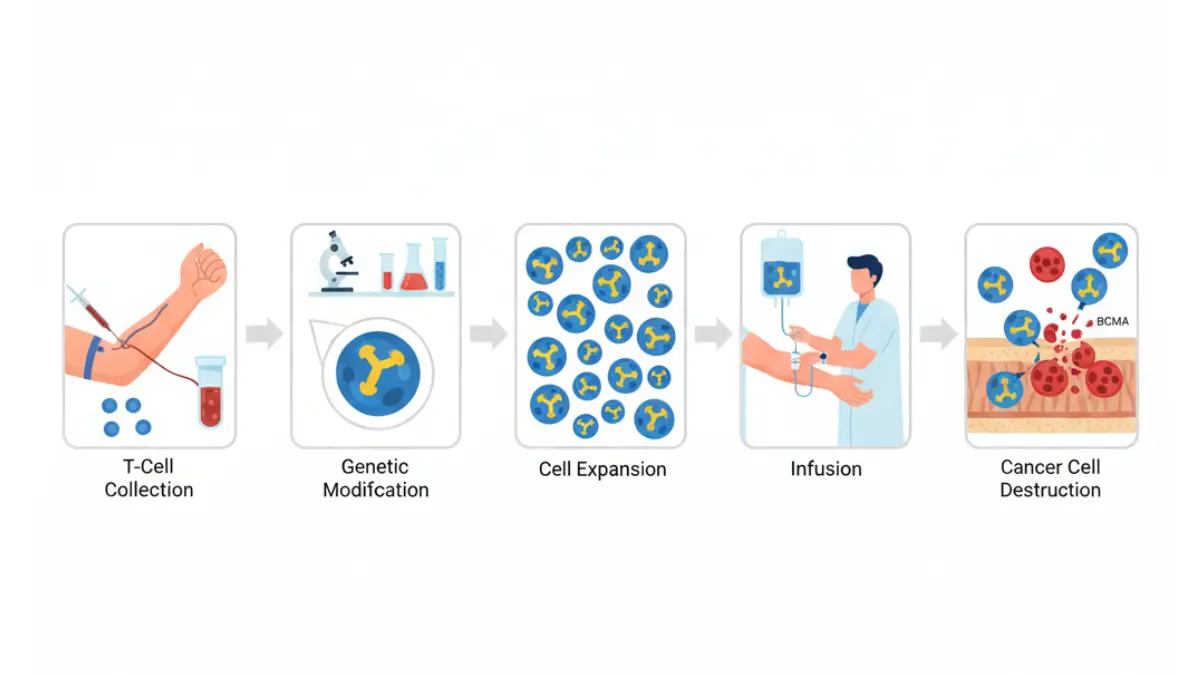
CAR-T Cell Therapy Advances
CAR-T cell therapy—which genetically engineers a patient’s own immune cells to recognize and destroy myeloma cells—has evolved dramatically. Approved CAR-T therapies like Abecma (idecabtagene vicleucel) and Carvykti (ciltacabtagene autoleucel) are now producing complete remissions lasting four to five years in patients with relapsed/refractory disease.
2026 CAR-T Success Metrics:
| Outcome Measure | Percentage |
|---|---|
| Overall response rate | 97% |
| Complete response rate | 83% |
| 4-year remission | 61% |
| Treatment-related mortality | <2% |
Bispecific Antibodies: The New Frontier
Bispecific antibodies represent a new class of immunotherapy that simultaneously binds to myeloma cells and T cells, forcing direct cancer cell destruction. Talvey (talquetamab) and Teclistamab, both approved in recent years, are showing remarkable efficacy in heavily pre-treated patients.
What This Means For You: If you’re newly diagnosed with multiple myeloma in 2026, you have access to treatment options that didn’t exist just 18 months ago. These therapies are not only more effective but often better tolerated than older chemotherapy regimens—meaning better quality of life during treatment.
MajesTEC-3 Trial Results
Published just this week, the MajesTEC-3 clinical trial demonstrated that teclistamab combined with daratumumab achieved an 89.5% overall response rate in relapsed/refractory patients. These results are prompting experts to reconsider when stem cell transplantation should be recommended, as newer therapies may delay or even eliminate the need for this intensive procedure.
Understanding how treatment affects overall health remains crucial for maintaining nutritional status during therapy.
Recognizing Multiple Myeloma: Symptoms and Diagnosis
CRAB Symptoms Explained
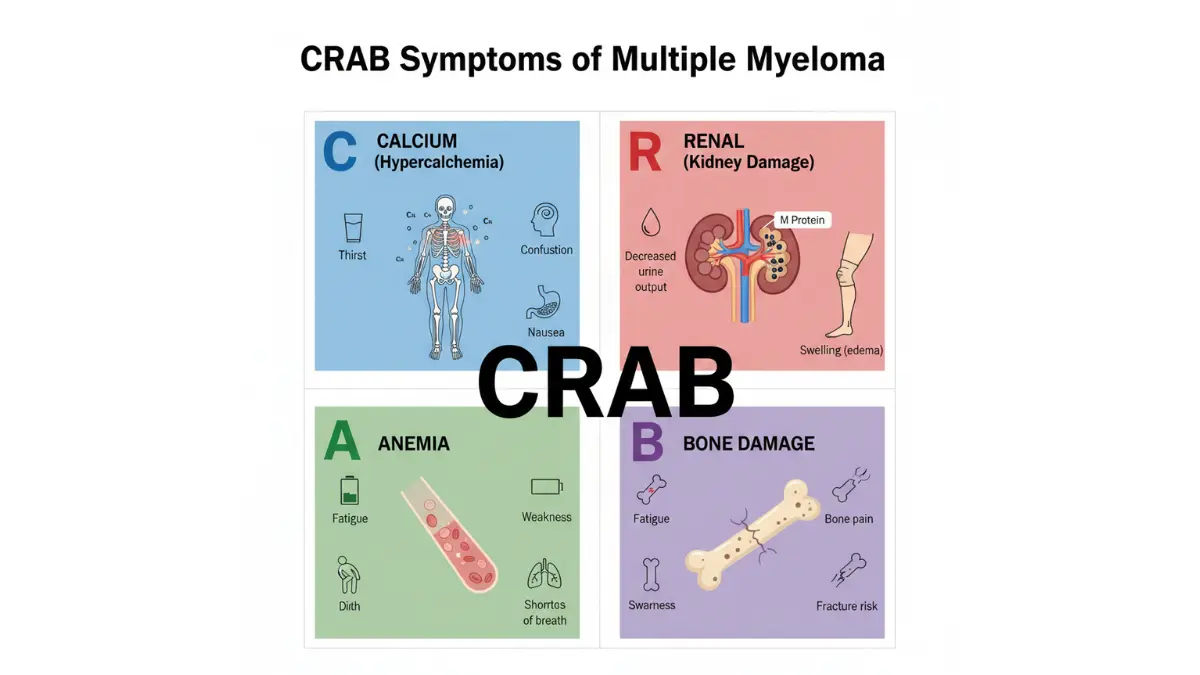
Multiple myeloma symptoms often develop gradually, making early detection challenging. Medical professionals use the CRAB acronym to identify the disease’s hallmark features:
C – Calcium (Hypercalcemia)
- Excessive thirst and frequent urination
- Nausea, constipation, and confusion
- Occurs in approximately 30% of newly diagnosed patients
R – Renal Impairment (Kidney Damage)
- Caused by M protein accumulation
- Present in 50% of patients at diagnosis
- May require dialysis in severe cases
A – Anemia (Low Red Blood Cells)
- Persistent fatigue and weakness
- Shortness of breath with minimal exertion
- Affects 70% of myeloma patients
B – Bone Lesions
- Severe bone pain, especially in back, ribs, and hips
- Pathological fractures from weakened bones
- Present in more than 80% of cases
If you experience these symptoms, use our symptom checker to assess whether medical evaluation is warranted.
Diagnostic Tests and Procedures
Confirming multiple myeloma requires comprehensive testing coordinated by a hematologist. The diagnostic pathway typically includes:
Blood Tests:
- Complete blood count (CBC)
- Serum protein electrophoresis (M-protein detection)
- Free light chain analysis
- Beta-2 microglobulin levels
- Lactate dehydrogenase (LDH)
Bone Marrow Biopsy: The gold standard for diagnosis, where a needle extracts marrow from the hip bone to examine plasma cell percentage and genetic abnormalities.
Imaging Studies:
- Skeletal bone survey (X-rays of all bones)
- MRI for spinal involvement
- PET-CT scan to detect active disease sites
ISS and R-ISS Staging Systems
The Revised International Staging System (R-ISS) stratifies patients into three risk categories based on beta-2 microglobulin, albumin levels, LDH, and cytogenetic abnormalities. This staging directly influences treatment selection and prognosis estimation.
Survival by R-ISS Stage:
| Stage | 5-Year Survival Rate |
|---|---|
| Stage I (Low Risk) | 82% |
| Stage II (Intermediate) | 62% |
| Stage III (High Risk) | 40% |
When to See a Doctor
Seek immediate medical attention if you experience unexplained bone pain, recurrent infections, or severe fatigue that interferes with daily activities. Early diagnosis significantly improves treatment outcomes.
Multiple Myeloma Survival Rates: 2026 Data and What Affects Your Outlook
Current 5-Year Survival Statistics
The latest SEER database statistics reveal that 62.4% of multiple myeloma patients diagnosed between 2015-2021 survived at least five years. This represents a dramatic improvement from historical survival rates and continues an upward trend driven by novel therapeutics.
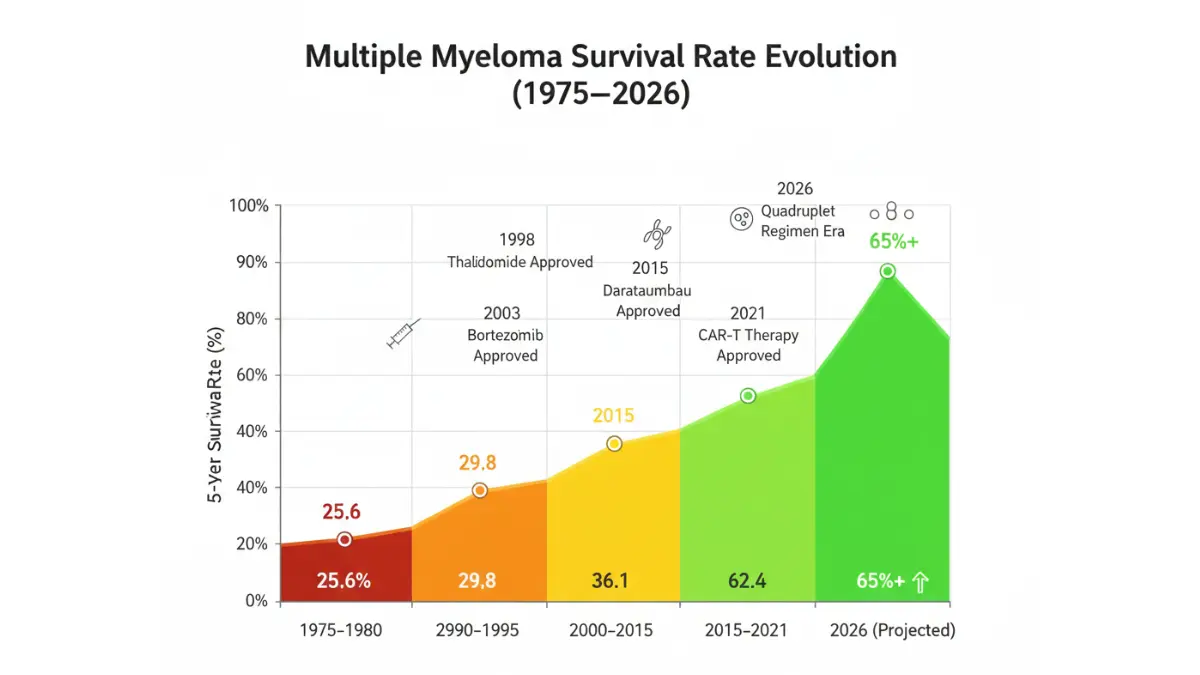
Survival Rate Evolution:
- 1975-1980: 25.6% five-year survival
- 2000-2005: 36.1% five-year survival
- 2015-2021: 62.4% five-year survival
- 2026 projection: >65% five-year survival
Survival by Stage
| Stage at Diagnosis | % of Patients | 5-Year Survival |
|---|---|---|
| Localized (Single Plasmacytoma) | 3.4% | 80.7% |
| Distant (Multiple Sites) | 96.4% | 61.7% |
| Unknown/Unstaged | 0.2% | 66.8% |
The vast majority of patients (96%) present with distant disease at diagnosis, as multiple myeloma typically affects multiple bone sites simultaneously.
Factors That Influence Prognosis
Favorable Prognostic Factors:
- Age under 65 years
- Normal albumin levels (≥3.5 g/dL)
- Low beta-2 microglobulin (<3.5 mg/L)
- Standard-risk cytogenetics
- Deep treatment response (MRD-negative)
Unfavorable Prognostic Factors:
- High-risk cytogenetic abnormalities (del17p, t(4;14), t(14;16))
- Elevated LDH levels
- Advanced ISS stage III disease
- Renal impairment requiring dialysis
- Extramedullary disease
Maintaining optimal nutrition during treatment can be supported with tools like the protein intake calculator to ensure adequate nourishment.
Long-Term Survivor Characteristics
Italian researchers recently published findings from 344 myeloma patients who survived 10+ years. Key characteristics included:
- Median age at diagnosis: 59 years
- Received stem cell transplantation: 78%
- Achieved complete remission after first-line therapy: 63%
- No high-risk cytogenetic features: 81%
Relapsed/Refractory Myeloma Outlook
Most patients eventually experience disease relapse, with median survival after first relapse ranging from 24-48 months depending on initial treatment response. However, 2026’s new CAR-T and bispecific antibody therapies are significantly extending survival in the relapsed setting.
Key Takeaway: Nearly two-thirds of patients diagnosed with multiple myeloma today will live at least five years, with many surviving a decade or longer. Continued therapeutic advances suggest these numbers will only improve.
Living with Multiple Myeloma: Treatment Side Effects and Quality of Life
Managing Treatment Side Effects
Modern myeloma therapy aims to balance disease control with quality of life. Understanding common side effects and management strategies empowers patients to maintain optimal functioning during treatment.
Chemotherapy-Related Effects:
- Peripheral Neuropathy – Tingling, numbness in hands/feet from bortezomib
- Management: Dose reduction, gabapentin, physical therapy
- Often improves after treatment completion
- Gastrointestinal Symptoms – Nausea, diarrhea, constipation
- Management: Anti-nausea medications, dietary modifications
- Maintain hydration with appropriate water intake
- Fatigue – Most common side effect affecting 70-90% of patients
- Management: Gentle exercise, adequate rest, nutrition optimization
- Consider using a calorie deficit calculator for weight management
Immunotherapy Side Effects:
- Blood count suppression (neutropenia, anemia, thrombocytopenia)
- Increased infection risk requiring prophylactic antibiotics
- Venous thromboembolism risk with lenalidomide
- Rash and skin reactions
CAR-T and Bispecific Antibody Toxicities:
- Cytokine Release Syndrome (CRS) – Fever, low blood pressure, difficulty breathing
- Treated with tocilizumab and corticosteroids
- Usually occurs within first 1-2 weeks
- Immune Effector Cell-Associated Neurotoxicity Syndrome (ICANS) – Confusion, difficulty speaking
- Requires immediate medical intervention
- Generally reversible with proper management
Nutrition and Lifestyle Modifications
Dietary Recommendations:
- High-protein intake: 1.2-1.5 grams per kg body weight daily
- Supports muscle mass during treatment
- Calculate needs with our macro calculator
- Bone-strengthening foods: Dairy, leafy greens, fortified foods
- Calcium (1200 mg daily) and Vitamin D (2000 IU daily)
- Supports bone health alongside bisphosphonate therapy
- Infection prevention diet:
- Avoid raw/undercooked meats, seafood, eggs
- Wash all fresh produce thoroughly
- Avoid unpasteurized dairy products
Exercise Guidelines:
Moderate physical activity reduces fatigue and improves bone density. The American Cancer Society recommends:
- 150 minutes weekly of moderate-intensity activity
- Resistance training 2-3 times weekly
- Balance exercises to prevent falls
- Avoid high-impact activities that stress bones
Bone Health and Fracture Prevention
Myeloma-related bone disease requires proactive management:
Pharmacological Interventions:
- Bisphosphonates (zoledronic acid, pamidronate)
- Denosumab (monoclonal antibody)
- Administered monthly intravenously or subcutaneously
Lifestyle Modifications:
- Fall-prevention strategies at home
- Assistive devices (canes, walkers) as needed
- Adequate pain management without opioid dependence
Infection Prevention Strategies
Myeloma and its treatments compromise immune function, making infection prevention critical:
Essential Precautions:
- Annual influenza vaccination
- Pneumococcal and COVID-19 vaccines (consult oncologist for timing)
- Hand hygiene before eating and after public spaces
- Avoid crowded areas during neutropenic periods
- Dental care to prevent oral infections
Warning Signs Requiring Immediate Attention:
- Fever >100.4°F (38°C)
- Chills or sweating
- Cough, shortness of breath
- Burning with urination
- New skin redness or swelling
Emotional and Mental Health Support
Cancer diagnosis profoundly affects mental well-being. Evidence-based support strategies include:
- Cognitive-behavioral therapy for anxiety/depression
- Support groups (International Myeloma Foundation, LLS)
- Mindfulness and meditation practices
- Open communication with healthcare team about distress
Patient Testimony: Maria Chen, a 62-year-old myeloma survivor from Seattle, emphasizes: “The physical treatments were challenging, but addressing my mental health through counseling and connecting with other patients made the biggest difference in my quality of life.”
Understanding the full picture of cancer symptoms beyond myeloma can help patients advocate comprehensively for their health.
The Future of Multiple Myeloma Treatment: What’s Coming in 2026 and Beyond
Next-Generation CAR-T Therapies
Researchers are developing “off-the-shelf” allogeneic CAR-T cells that don’t require patient-specific manufacturing, dramatically reducing production time from weeks to hours. These universal donor cells could make CAR-T therapy accessible to more patients at lower costs.
Additionally, dual-targeting CAR-T therapies attacking both BCMA and CD38 simultaneously are showing promise in early-phase trials, potentially preventing resistance development.
Minimal Residual Disease (MRD) Testing
MRD negativity—the absence of detectable myeloma cells at extremely sensitive levels (10⁻⁵ or 10⁻⁶)—has emerged as the most powerful prognostic indicator. Patients achieving sustained MRD negativity experience progression-free survival exceeding 5-10 years.
Flow cytometry and next-generation sequencing now detect one cancer cell among a million normal cells, allowing oncologists to tailor treatment intensity based on depth of response.
Personalized Medicine and Genomics
Comprehensive genomic profiling identifies specific mutations driving each patient’s myeloma, enabling precision therapy selection. For example:
- t(11;14) translocation: Responds preferentially to venetoclax
- Gain 1q/amp1q21: Requires intensive therapy with CAR-T consideration
- TP53 deletion: Benefits from bispecific antibodies early in treatment
Clinical Trials to Watch
MajesTEC-7 Trial: Comparing teclistamab combinations versus standard VRd in newly diagnosed patients ineligible for transplant. Results expected Q4 2026.
CARTITUDE-6: Evaluating earlier CAR-T therapy (after just 1-2 prior lines) versus standard treatment sequences.
Bispecific Antibody Combinations: Multiple trials exploring bispecific antibodies combined with immunomodulators or proteasome inhibitors.
Key Takeaway: The myeloma treatment landscape continues evolving rapidly. Patients diagnosed today benefit from therapies unavailable just 18-24 months ago, with even more promising options approaching FDA review.
Understanding how various cancer treatments compare across different malignancies helps contextualize myeloma therapeutic advances.
Frequently Asked Questions About Multiple Myeloma
1. Can multiple myeloma be cured in 2026?
While not yet curable, multiple myeloma is increasingly manageable as a chronic condition. Some patients achieve such deep, sustained remissions with CAR-T therapy that they remain disease-free for 5+ years off treatment—approaching functional cure status.
2. What triggers multiple myeloma?
The exact cause remains unknown. Risk factors include age over 65, Black race, family history, obesity, and prior MGUS diagnosis. Most cases arise from spontaneous genetic mutations in plasma cells rather than hereditary transmission.
3. How long can you live with multiple myeloma without treatment?
Untreated symptomatic myeloma progresses rapidly, with median survival of 6-12 months. Smoldering myeloma (asymptomatic) may remain stable for years before requiring treatment, with 10% annual progression risk to active disease.
4. Is multiple myeloma painful?
Bone pain affects 80% of patients, typically in the back, ribs, and long bones. Pain results from lytic bone lesions, pathological fractures, and tumor expansion within bone marrow. Effective pain management with analgesics, radiation, and disease-directed therapy is essential.
5. What foods should you avoid with multiple myeloma?
Avoid raw/undercooked meats, unpasteurized dairy, raw eggs, unwashed produce, and deli meats due to infection risk. Limit alcohol consumption as it can worsen neuropathy and interact with medications. Stay hydrated and maintain adequate protein intake.
6. Does multiple myeloma run in families?
Multiple myeloma is not typically hereditary, though first-degree relatives have 2-4 times higher risk than the general population. Genetic testing through services like our genetic risk assessment tool can clarify inherited cancer susceptibilities.
7. What is the difference between MGUS and multiple myeloma?
MGUS (monoclonal gammopathy of undetermined significance) is a precursor condition with <10% plasma cells in bone marrow and no organ damage. It progresses to myeloma at approximately 1% per year. MGUS requires monitoring but not active treatment.
8. How often does multiple myeloma come back?
Multiple myeloma typically relapses, though newer treatments are extending first remission durations. With modern therapy, median time to first relapse is 3-5 years, with subsequent remissions generally shorter unless salvage therapy includes CAR-T or bispecific antibodies.
9. Can you work with multiple myeloma?
Many patients continue working during treatment, especially with targeted therapies that cause fewer side effects than traditional chemotherapy. Accommodations may include flexible schedules during infusion days and short-term disability during stem cell transplantation.
10. What is the most common age for multiple myeloma?
Median age at diagnosis is 69 years, with peak incidence between 65-74 years. Only 2-3% of cases occur in patients under age 40. Younger patients generally have better prognosis due to tolerating aggressive therapies better.
11. Are there any new drugs for multiple myeloma in 2026?
Yes—the FDA approved daratumumab plus VRd quadruplet therapy in January 2026 for newly diagnosed patients. Additionally, next-generation bispecific antibodies targeting GPRC5D and FcRH5 are under accelerated review following breakthrough designation.
About the Author: This article was researched and compiled by the medical content team at MyMedicineAdvisor.com, which includes 21 internationally credentialed medical experts specializing in hematology-oncology, internal medicine, and patient education. All content undergoes peer review for accuracy and adherence to current clinical guidelines.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.











